
Abstract
Purpose
Prevention of cough during emergence after nasal surgery is important for avoiding surgical site bleeding. We investigated the remifentanil effect-site concentration in 50% (EC50) of the elderly patients undergoing nasal surgery for smooth emergence without cough and compared it with that of adult patients.
Methods
Twenty-two elderly (aged 65–80 years) and 25 adult patients (aged 20–60 years) with an American Society of Anesthesiologists physical status I/II undergoing nasal surgery were enrolled. Anesthesia was maintained with sevoflurane and remifentanil. Remifentanil EC50 and EC95 for preventing cough were determined using the modified Dixon’s up-and-down method and isotonic regression with bootstrapping approach. Recovery profiles were also recorded.
Results
With Dixon’s up-and-down method, the EC50 of remifentanil in elderly patients (2.40±0.25 ng/mL) was not significantly different from that of adults (2.33±0.30 ng/mL) (P=0.687). With isotonic regression, the EC95 of remifentanil in elderly patients (3.32 [95% confidence interval: 3.06–3.38] ng/mL) was not significantly different from that of adults (3.30 [95% confidence interval: 2.96–3.37] ng/mL). However, eye opening time (14.1±3.8 vs 12.0±2.9 seconds), extubation time (17.2±4.1 vs 14.0±3.0 seconds), and postanesthesia care unit duration (44.5±7.6 vs 38.7±3.4 minutes) in elderly patients were significantly longer than those in adults (P<0.05).
Conclusion
Remifentanil EC50 for preventing cough after nasal surgery with sevoflurane anesthesia did not differ between elderly and adult patients. However, delayed awakening and respiratory adverse events may warrant attention in elderly patients.
Introduction
Cough suppression during emergence and tracheal extubation after general anesthesia has become an important issue in patient safety. Cough due to mechanical irritation of the endotracheal tube and cuff can be accompanied by various adverse effects such as laryngospasm, hypertension, tachycardia, arrhythmia, and an increase in intracranial, intraocular, or intra-abdominal pressure.Citation1 Consequently, this can lead to myocardial ischemia, disruption of wound, and bleeding at the surgical site. Alongside medical development, an increasing number of elderly patients undergo surgery and exhibit a greater prevalence of cardiovascular disease than younger patients.Citation2,Citation3 Therefore, the application of agents for cough suppression during emergence should be investigated further.
Remifentanil is a selective μ-receptor opioid agonist with a very rapid onset time. Its extrahepatic metabolism by nonspecific esterase results in rapid clearance.Citation4,Citation5 Maintenance of remifentanil infusion during emergence has been reported to be an effective method for reducing cough and cardiovascular change without delay of recovery.Citation6,Citation7 In previous studies, the effective effect-site concentration for 95% of adults (EC95) for preventing cough has been shown to vary according to anesthetic agent, type of surgery, and patient sex, and is ranging from 2.14 to 2.94 ng/mL.Citation8–Citation10
The aging process may alter not only the pharmacokinetics and pharmacodynamics,Citation11,Citation12 resulting in potentially variable responses to anesthetic drugs (likely increase in sensitivity), but also cough reflex.Citation13 The hypothesis of this study is that altered pharmacokinetics and cough sensitivity in elderly patients may require the titration of remifentanil target controlled infusion (TCI) for cough suppression during emergence. To the best of our knowledge, no studies to date have confirmed the effect of remifentanil TCI on cough suppression in the elderly. Therefore, the purpose of this study is to determine the effect-site concentration of remifentanil in 50% (EC50) of elderly patients undergoing nasal surgery for cough suppression during emergence after balanced anesthesia with sevoflurane and remifentanil. In addition, we have compared the difference in effect-site concentration of remifentanil and recovery profiles between elderly and adult patients.
Patients and methods
Patients
Approval was obtained from the Institutional Review Board of Ajou University Hospital (Suwon, Korea), and the study was registered with ClinicalTrials.gov (NCT No: 02334046). All patients provided informed written consent. Twenty-two elderly patients (aged 65–80 years) and 25 adult patients (aged 20–60 years) with an American Society of Anesthesiologists physical status I or II undergoing nasal surgery (endoscopic sinus surgery or septoplasty) were enrolled in this study. The following patients were excluded from the study: those with predicted difficult airway, body mass index >30 kg/m2, history of obstructive sleep apnea, chronic respiratory disease or coughing, current smokers, and angiotensin-converting enzyme inhibitor users.
Anesthesia
Patients were not administered with any premedication. Upon arrival in the operating theater, all patients were monitored via electrocardiography, pulse oximetry, automated noninvasive blood pressure measurement, and bispectral index (BIS) using the BIS™ Quatro Sensor (Covidien, Boulder, CO, USA) applied to the forehead of each patient. After preoxygenation with 100% oxygen for 1 minute, anesthesia was induced with a bolus injection of 1.5–2.0 mg/kg propofol and 2.0–3.0 ng/mL effect-site concentration of remifentanil via a TCI system (Orchestra®, Fresenius Vial, France) using Minto’s model.Citation14 After loss of consciousness, 0.6 mg/kg rocuronium was injected and then intubation was performed with a cuffed endotracheal tube (internal diameter 7.5 mm for males and 7.0 mm for females). The intracuff pressure was adjusted to 20–25 mmHg using a pressure gauge (Hi-Lo Hand Pressure Gauge, VBM Medizintechnik, GmbH, Germany). Anesthesia was maintained with 1.5–2.5 vol% sevoflurane and 2.0–4.0 ng/mL of remifentanil to target a BIS between 40 and 60, and a mean blood pressure and heart rate within 20% of baseline values. Mechanical ventilation was adjusted to maintain an end-tidal CO2 between 35 and 40 mmHg using 0.5 fraction of inspired oxygen. Corticosteroids which could affect the results were not administered during surgery. Approximately 15 minutes before the end of surgery, sevoflurane was adjusted to 1–1.2 vol% to achieve a BIS of ~60, and remifentanil was set at the predetermined effect-site concentration for obtaining equilibrium between plasma and effect-site at the time of surgery completion. After surgery, sevoflurane was discontinued and 0.004 mg/kg glycopyrrolate and 0.02 mg/kg neostigmine were injected for reversal of residual muscle relaxation after achieving a train-of-four ratio of 0.9. Oropharyngeal suction was gently performed before injection of reversal agents. Mechanical ventilation was switched to manual ventilation to maintain an end-tidal CO2 between 40 and 45 mmHg. Extubation was performed when patients were able to open their eyes on command and following the recovery of adequate spontaneous ventilation. Immediately after extubation, remifentanil infusion was stopped and 100% oxygen was administered via a face mask for 5 minutes. The presence of cough was recorded by the investigator who was unaware of the concentration of remifentanil. After confirmation of consciousness and adequate respiration, patients were transferred to the post-anesthetic care unit (PACU). In the PACU, fentanyl 1 μg/kg was administered when the pain score exceeded 5 points on the numerical rating scale. Patients were discharged from the PACU when Aldrete score was ≥9.Citation15
Determination of effect-site concentration and recovery profiles
The Dixon’s up-and-down method was used to determine the effect-site concentration of remifentanil for cough suppression during the emergence period (in the presence of endotracheal tube, during tracheal extubation, and 5 minutes after extubation).Citation16 If coughing occurred during the emergence period, it was considered a failure of cough suppression. The initial effect-site concentration of remifentanil was 1.8 ng/mL. In the next patient, the effect-site concentration of remifentanil was determined by the success or failure of cough suppression of the previous patient. If cough suppression was a success, then the effect-site concentration of remifentanil was reduced by 0.4 ng/mL, while in case of failure it was increased by 0.4 ng/mL. The remifentanil EC50 of patients, which enabled successful cough suppression, was determined by calculating the mean of the midpoint effect-site concentration of all independent pairs after six crossover points were obtained (ie, success to failure).
Hemodynamic data and respiratory profiles were recorded before anesthesia induction (baseline), at the end of surgery, at eye opening, immediately after extubation, and 5 minutes after extubation. The eye opening and extubation times were also measured and events of hypoventilation <8 breaths/min or oxygen saturation (SaO2) below 95% were recorded.
Statistical analysis
The sample size was decided based on prior literature about the modified Dixon’s up-and-down method. To minimize the inaccuracy of the individual study, more than the minimum six crossover points are required in this method.Citation17
Statistical analyses were performed using the Statistical Package for Social Sciences (version 20.0 for Windows; IBM Corporation, Armonk, NY, USA) and R for Windows (version 3.0.1; The R Foundation for Statistical Computing; https://www.r-project.org). The EC50 calculated from the modified Dixon’s up-and-down method was compared between the two patient groups using a t-test. For backup analysis, the data were analyzed using the isotonic regression method to estimate EC50 and EC95 along with 95% confidence intervals (CIs). The isotonic regression is a variant of restricted least squares regression to constrain the point estimates to either increase or decrease monotonically, which has favorable statistical properties.Citation18 The CI was estimated using the bootstrapping approach.Citation18 All other variables were compared between groups using an independent t-test, chi-square test, Fisher’s exact test, or Mann–Whitney U statistic, where appropriate. Hemodynamic data were analyzed with repeated measures of analysis of variance. Data were presented as the mean ± standard deviation or the number of patients. Statistical significance was accepted when the P-value was <0.05.
Results
In total, 47 patients completed the study (). The elderly patient group comprised 22 patients with a mean age of 69 (range: 65–80 years) and the adult patient group comprised 25 patients with a mean age of 35 (range: 20–60 years). Patient characteristics are presented in . There were significantly more patients in the elderly groups with an American Society of Anesthesiologists physical status of II than in the adult group (P<0.001). During mask ventilation and intubation, there was no unpredicted difficult airway.
Table 1 Patient characteristics
Figure 1 Consort flow diagram.
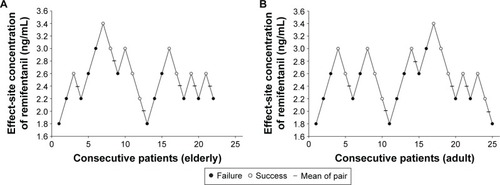
The sequence of dose–response data for each patient is shown in . Using the modified Dixon’s up-and-down method, the EC50 of remifentanil was not significantly different between the elderly and adult groups (2.40±0.25 vs 2.33±0.30 ng/mL, respectively, P=0.687). With isotonic regression and the bootstrapping approach, the EC50 of remifentanil was similar between the elderly and adult groups (2.50 [95% CI: 2.38–2.75] ng/mL and 2.52 [95% CI: 2.29–2.78] ng/mL, respectively). The EC95 of remifentanil was also similar between the elderly and adult groups (3.32 [95% CI: 3.06–3.38] ng/mL and 3.30 [95% CI: 2.96–3.37] ng/mL, respectively).
Figure 2 Sequences of effect-site concentration of remifentanil for preventing cough during emergence.
Recovery profiles are presented in . While the number of patients presenting cough and the effect-site concentration of remifentanil for cough suppression were similar between patient groups, eye opening time (14.1±3.8 vs 12.0±2.9 seconds), extubation time (17.2±4.1 vs 14.0±3.0 seconds), and PACU duration (44.5±7.6 vs 38.7±3.4 minutes) in the elderly group were significantly longer than those in the adult group (all P<0.05). There were no significant differences in pain score and additional analgesic requirement in the PACU between groups.
Table 2 Recovery profiles
There were no significant differences in hemodynamic data between elderly and adult patient groups (data not shown). In the present study, the highest concentration of remifentanil used was 3.4 ng/mL and the lowest concentration was 1.8 ng/mL. Hypoventilation (<8 breaths/min, respiratory rate) occurred in 8/22 (36%) patients in the elderly group and 6/25 (24%) patients in the adult group. Oxygen desaturation (SaO2 <95%) occurred in one patient in the elderly group, but did not occur in the adult patient group. While these adverse events occurred more frequently in the elderly group, there were no significant intergroup differences.
Discussion
Our results showed that maintaining remifentanil during emergence was an effective method for smooth emergence and the required effect-site concentration of remifentanil in elderly patients was not different from that of the adult patients.
Previous studies have investigated the EC50 and EC95 of remifentanil TCI for cough prevention in various surgeries.Citation8,Citation9 Choi et alCitation8 reported the EC50 and EC95 of remifentanil at 2.17 and 2.94 ng/mL, respectively, in males aged 18–60 years (median age 35 years) undergoing nasal surgery after balanced anesthesia with sevoflurane. These results are comparable to the present findings. Our study demonstrated that the EC50 of remifentanil in adult and elderly patients was 2.33 and 2.40 ng/mL, respectively, without significant intergroup differences. In another study,Citation9 the EC95 of remifentanil TCI was 2.51 ng/mL in patients (aged 20–65 years; mean: 43 years) undergoing transsphenoidal surgery during propofol and remifentanil anesthesia, using biased coin up-and-down sequential allocation and the isotonic regression method.
The effect of aging on cough reflex remains controversial.Citation13,Citation19,Citation20 A previous study demonstrated that the sensitivity of cough reflex significantly decreased in the elderly patients compared with that in the young patients,Citation13 whereas other studies failed to detect this association.Citation19,Citation20 The aging process may also alter pharmacokinetics and pharmacodynamics,Citation11,Citation12 and can affect clinical responses to drugs. In general, the elderly are expected to be more sensitive to many drugs, especially opioids. Sensitivity to remifentanil has been reported to be high in elderly patients.Citation14,Citation21 The TCI of remifentanil is age variable-adjusted because Minto’s model was based on the electroencephalogram (EEG) effect of remifentanil using a three-compartment model with height, weight, and age as covariates.Citation14
The present study demonstrated that there was no age-related difference in the effect-site concentration of remifentanil for cough suppression during emergence. This suggests that remifentanil TCI using Minto’s model is appropriate to predict the clinical performance on cough suppression; therefore, there is no need to reduce the effect-site concentration of remifentanil in the elderly. The antitussive effect of narcotics appears to be via opioid receptors such as μ- and κ-receptorsCitation22,Citation23 and, at the subtype level, the antitussive effect of μ-receptors is depressed via μ2 -receptors.Citation24 However, the opioid receptors involved in the EEG effect in Minto’s model may be different from those involved with antitussive action. Therefore, the explanation for the good clinical performance is unclear.
In contrast, recovery profiles such as eye opening time, extubation time, and PACU duration differed between elderly and adult patients in the present study. Although the clinical significance of the prolongation of recovery in the elderly group was relatively minor, it should be treated with caution to some extent. This difference between the elderly and adult patients may be due to several reasons. First, the reduced predictive clinical performance of Minto’s model of remifentanil TCI on recovery profiles. As mentioned earlier, Minto’s model is based on the EEG effect of remifentanil;Citation14 therefore, the influence of age on other clinical variables such as respiration and analgesia may be different. Second, the interpatient variability of remifentanil was larger in the elderly patient group than in the adult group.Citation14 Third, sevoflurane may have affected the results because the elimination rate of sevoflurane can be influenced by variations in the respiratory effect of remifentanil according to age or because the minimal alveolar concentration of sevoflurane for awakening also decreases with age.Citation25 Therefore, further studies are required to establish a definite conclusion on the influence of age on the clinical performance of remifentanil TCI with regard to recovery profiles.
Hypoventilation <8 breaths/min occurred in one-third of patients and desaturation below 95% in one patient in the elderly group. These adverse events were more frequent in the elderly group, although this difference lacked statistical significance. Remifentanil produces respiratory depression in a dose-dependent manner.Citation26 Chang et alCitation27 demonstrated that 2 ng/mL remifentanil is associated with a significant increase in hypoventilation episodes and delayed emergence. The EC95 of remifentanil for cough suppression during emergence would be more susceptible to respiratory depression. Therefore, when a remifentanil EC95 is administered, caution is required with regard to potential hypoventilation and desaturation.
This study has a few limitations. First, patient sex differences at the enrollment stage were not accounted for; the proportion of males in this study was 72%. According to the results of Soh et al,Citation28 the effect-site concentration of remifentanil TCI for antitussive effect is higher in males than in females. Therefore, variations in the dose–response according to sex may have affected this sequential data. Second, the type of surgery was limited to nasal surgery (endoscopic sinus surgery or septoplasty). Based on the differences in the effect-site concentration of remifentanil in previous studies of a similar design,Citation10,Citation27 surgery type is likely to influence the effect-site concentration of remifentanil. Therefore, the application of the current findings to other types of surgery should be considered carefully.
Conclusion
The effect-site concentration of remifentanil for preventing cough after nasal surgery (endoscopic sinus surgery or septoplasty) with sevoflurane anesthesia in elderly patients did not differ from that in adult patients. However, delayed awakening and respiratory adverse events may warrant special attention in elderly patients.
Disclosure
The authors report no conflicts of interest in this work.
References
- IrwinRSOwnbeyRCaglePTBakerSFraireAEInterpreting the histopathology of chronic cough: a prospective, controlled, comparative studyChest2006130236237016899833
- JacksonCFWengerNKCardiovascular disease in the elderlyRev Esp Cardiol201164869771221723657
- Lloyd-JonesDAdamsRCarnethonMHeart disease and stroke statistics – 2009 update: a report from the American Heart Association Statistics Committee and Stroke Statistics SubcommitteeCirculation20091193e21e18119075105
- EganTDRemifentanil pharmacokinetics and pharmacodynamics. A preliminary appraisalClin Pharmacokinet199529280947586903
- GlassPSGanTJHowellSA review of the pharmacokinetics and pharmacodynamics of remifentanilAnesth Analg1999894 SupplS7S1410511072
- AouadMTAl-AlamiAANasrVGSoukiFGZbeidyRASiddik-SayyidSMThe effect of low-dose remifentanil on responses to the endotracheal tube during emergence from general anesthesiaAnesth Analg200910841157116019299779
- NhoJSLeeSYKangJMEffects of maintaining a remifentanil infusion on the recovery profiles during emergence from anaesthesia and tracheal extubationBr J Anaesth2009103681782119864308
- ChoiEMParkWKChoiSHSohSLeeJRSmooth emergence in men undergoing nasal surgery: the effect site concentration of remifentanil for preventing cough after sevoflurane-balanced anaesthesiaActa Anaesthesiol Scand201256449850322220983
- ChoiSHMinKTLeeJRDetermination of EC95 of remifentanil for smooth emergence from propofol anesthesia in patients undergoing transsphenoidal surgeryJ Neurosurg Anesthesiol201527216016625105828
- LeeBLeeJRNaSTargeting smooth emergence: the effect site concentration of remifentanil for preventing cough during emergence during propofol-remifentanil anaesthesia for thyroid surgeryBr J Anaesth2009102677577819411668
- RiveraRAntogniniJFPerioperative drug therapy in elderly patientsAnesthesiology200911051176118119352149
- ShaferSLThe pharmacology of anesthetic drugs in elderly patientsAnesthesiol Clin North America200018112910934997
- NewnhamDMHamiltonSJSensitivity of the cough reflex in young and elderly subjectsAge Ageing19972631851889223713
- MintoCFSchniderTWShaferSLPharmacokinetics and pharmacodynamics of remifentanil. II. Model applicationAnesthesiology199786124339009936
- AldreteJAThe post-anesthesia recovery score revisitedJ Clin Anesth19957189917772368
- DixonWJStaircase bioassay: the up-and-down methodNeurosci Biobehav Rev199115147502052197
- PaulMFisherDMAre estimates of MAC reliable?Anesthesiology20019561362137011748393
- PaceNLStylianouMPAdvances in and limitations of up-and-down methodology: a précis of clinical use, study design, and dose estimation in anesthesia researchAnesthesiology2007107114415217585226
- EbiharaSEbiharaTKanezakiMAging deteriorated perception of urge-to-cough without changing cough reflex threshold to citric acid in female never-smokersCough201171321711545
- KatsumataUSekizawaKEbiharaTSasakiHAging effects on cough reflexChest199510712902917813298
- MintoCFSchniderTWEganTDInfluence of age and gender on the pharmacokinetics and pharmacodynamics of remifentanil. I. Model developmentAnesthesiology199786110239009935
- KameiJTaniharaHKasuyaYAntitussive effects of two specific kappa-opioid agonists, U-50,488H and U-62,066E, in ratsEur J Pharmacol199018722812862272363
- KameiJTaniharaHKasuyaYModulation of mu-mediated anti-tussive activity in rats by a delta agonistEur J Pharmacol199120311531561665789
- KameiJSaitohAMoritaKNagaseHAntagonistic effect of buprenorphine on the antitussive effect of morphine is mediated via the activation of mu 1-opioid receptorsLife Sci19955716PL231PL2357564887
- KatohTSuguroYKimuraTIkedaKCerebral awakening concentration of sevoflurane and isoflurane predicted during slow and fast alveolar washoutAnesth Analg1993775101210178214700
- MitsisGDGovernoRJRogersRPattinsonKTThe effect of remifentanil on respiratory variability, evaluated with dynamic modelingJ Appl Physiol200910641038104919196914
- ChangCHLeeJWChoiJRShimYHEffect-site concentration of remifentanil to prevent cough after laryngomicrosurgeryLaryngoscope2013123123105310923686891
- SohSParkWKKangSWLeeBRLeeJRSex differences in remifentanil requirements for preventing cough during anesthetic emergenceYonsei Med J201455380781424719152