
Abstract
Background
A number of studies have explored the issue of sex differences in stroke from biomedical perspective; however, there are still large gaps in the existing knowledge. The purpose of this study was to assess whether the differences in socioeconomic status and living conditions between men and women may explain the part of the sex differences in incidence and outcomes of stroke.
Methods
All stroke participants aged ≥60 years admitted in Vaseie Hospital in Sabzevar, Iran, from March 21, 2013, until March 20, 2014, were included in this study. Computerized tomography and magnetic resonance imaging were used to confirm stroke. A series of χ2 tests were performed and Statistical Program for Social Sciences, Version 21.0, was used to investigate the potential differences between older men and women in stroke incidence and outcomes.
Results
A total of 159 incident stroke cases were documented during 1 year. The annual rate of stroke was statistically significantly higher in elderly women than in elderly men (401 vs 357 per 100,000; P<0.001). Female elderly participants had significantly lower socioeconomic status, poorer living conditions, and higher lifetime history of depression, hypertension, and diabetes mellitus than their male counterparts.
Conclusion
The findings from this study showed that elderly women are more adversely affected by stroke in terms of incidence and outcomes of stroke than elderly men. The most noticeable result is that sex differences in socioeconomic status and living conditions may result in increased incidence of stroke and poorer outcomes in elderly women. Therefore, it is imperative to identify vulnerable elderly women and provide them appropriate treatment and services.
Introduction
Currently, stroke is an emerging major public health problem and the cause of 9% of overall mortality.Citation1 It is estimated that by 2020 stroke will be the second leading cause of death.Citation2 The results from several studies show that incidence and burden of stroke are mostly different for women and men,Citation3–Citation5 and elderly women are more likely affected by stroke than men. Some studies show an increased incidence of stroke and poorer outcomes, such as disability and quality of life, in elderly women than in elderly men.Citation1,Citation4,Citation6–Citation9 Although sex differences in stroke have increasingly been explored from biomedical perspectives, and several explanations such as pregnancy complications, genetic factors, clinical presentation, steroid hormones, hemoglobin levels, oral contraceptives, and menopause have been provided to explain the observed sex differences in stroke,Citation4,Citation10–Citation12 there are still large gaps in the existing knowledge.Citation4,Citation7,Citation13 It seems that the reasons for sex disparities in stroke are multifactorial, and the mechanisms that increase the risk of stroke in elderly women are not well understood.Citation4,Citation14 Therefore, a greater understanding of the differences in stroke between men and women may enhance the development of effective prevention and treatment strategies to improve stroke care and quality of life in the rapidly aging populations. As mentioned earlier, some studies reported sex differences in stroke from physiological perspectives and found that intrinsic sex differences may explain some of the differences in stroke between men and women, but there are still considerable gaps in our understanding of sex differences in stroke.Citation4
Some studies have found that socioeconomic status contributes to stroke;Citation2,Citation15,Citation16 however, only limited studies that investigated the differences in stroke between elderly men and women from a socioeconomic perspective are available. There are significant differences in socioeconomic status and living conditions between elderly men and women, wherein older women have lower socioeconomic status and living conditions.Citation11,Citation17–Citation19 A growing body of literature indicates that lower socioeconomic status and living conditions contribute to some risk factors for stroke such as hypertension, diabetes mellitus, and depression.Citation20–Citation24 Participants with low socioeconomic status are less likely to receive specific processes of care after stroke compared with participants with high socioeconomic status.Citation22,Citation25 Some studies have found that older adults living alone, being unmarried, and living in deprived areas are less likely to receive stroke care.Citation26,Citation27 Some other studies have found that access to health care may affect both incidence and recovery from stroke. Low access to health care for various prevention and therapeutic services is related to higher rates of stroke incidence and mortality.Citation2,Citation21 In addition, low socioeconomic status and poor living conditions decrease the willingness to seek medical care among older adults.Citation28–Citation30 presents the model of hypothesized relationships. Elderly women, compared to elderly men, have lower socioeconomic status and living conditions before stroke, which result in differences in risk factor distribution, availability of stroke prevention interventions, and provision of care that consequently increase the incidence of stroke and result in poorer outcomes of stroke.
Figure 1 Socioeconomic mechanism underlying sex differences in stroke.
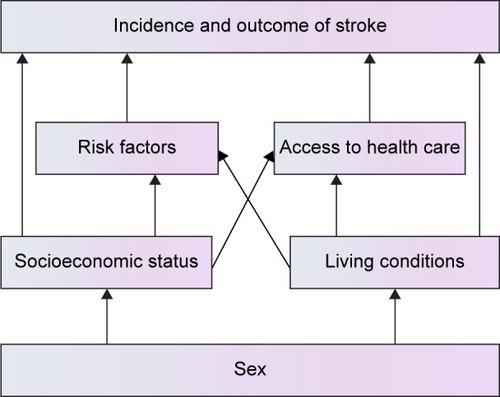
According to the aforementioned possible underlying mechanism, the present study aimed to assess whether the differences in socioeconomic status and living conditions between men and women may explain part of the sex differences in incidence and outcomes of stroke.
Methodology
This hospital-based study was conducted in Sabzevar (a region in the northeast of Iran, with a population of ~500,000) from March 21, 2013, until March 20, 2014. All the participants aged ≥60 years admitted in Vaseie Hospital in Sabzevar, Iran, were included in this study. Computerized tomography scan and magnetic resonance imaging were used to confirm stroke. All participants were followed up until a definite outcome was determined. Permission was obtained from hospital administration and Ethical Committee, and then, data such as sociodemographic characteristics and prestroke risk factors were collected.
Ethical approval
This study was conducted in accordance with the 1964 Declaration of Helsinki and its later amendments and was approved by the Ethics Committee of the Sabzevar University of Medical Sciences, Iran. Written informed consent was obtained from all participants or from their relatives; the objectives of this study were explained, and confidentiality of information was assured to them.
Statistical Program for Social Sciences for Windows, Version 21.0 (IBM Corporation, Armonk, NY, USA), was used for data analysis. Descriptive statistics including percentages, measures of central tendency, and measures of variability were used to present the sample. A series of χ2 tests were conducted to investigate the potential differences between older men and women in stroke incidence and outcomes. A two-tailed P-value ≤0.05 was used to determine the statistical significance.
Results
A total of 159 incident strokes among participants aged ≥60 years were observed during a period of 12 months from January 2013 to January 2014. The mean age of the participants was 76.38 years (standard deviation =8.50; range 60–95 years), 52.2% were female, 69.2% were unemployed, and 77.4% reported not having formal education. The annual rate of stroke was 378 cases per 100, 000 persons. There was a significantly higher incidence of stroke in elderly women than in elderly men (401 vs 357 per 100,000; P<0.001); ~41% of stroke victims were in young-old (60–74) group. As shown in , ~16% of participants reported a history of depression, 26.4% diabetes, and 79.2% hypertension. The mean of hospital arrival time after the onset of stroke was 22.31 hours (standard deviation =29.16).
Table 1 Descriptive characteristics of the sample
presents the sociodemographic and health characteristics of the sample with respect to sex. There was a strong association between marital status and sex (χ2[1] =17.05; P<0.001), with 88.2% of elderly male participants with stroke compared to 59.0% of elderly female participants with stroke being married. Slightly more than one-fourth of elderly women were living alone, whereas only a minority of the men (7.9%) were living alone. This sex difference was highly significant (χ2[2] =17.22; P<0.001). Majority (77.3%) of stroke participants in this sample had no formal education. Male stroke participants had significantly higher level of education than their female counterparts (χ2[2] =13.8; P<0.001).
Table 2 Sociodemographic and health characteristics of the sample with respect to sex
As shown in , statistically significant differences were observed in risk factors for stroke between men and women. Significantly more number of women reported lifetime history of depression (χ2[1] =4.66; P≤0.05), hypertension (χ2[1] =4.19; P≤0.05), and diabetes mellitus (χ2[1] =4.79; P≤0.05) than men. In addition, hospital arrival time after the onset of stroke was longer in women (χ2[1] =7.22; P≤0.05) than in men. Women were more likely to be unemployed than men (χ2[1] =10.85; P≤0.05). Although no significant association was observed between sex and mortality rate, elderly women had higher mortality rate after stroke than men. In female participants, in-hospital mortality rate was 7.2%, while in male participants it was 2.6%. No significant difference in age was observed between elderly male and female survivors with stroke.
Discussion
In order to identify sex differences in stroke and to explore sex disparities in terms of incidence and outcome of stroke in later life, the present study was conducted from a socioeconomic perspective. Although some epidemiological studies show that stroke is more common among men,Citation31,Citation32 our finding that is in line with some studies showing increased incidence of stroke among postmenopausal womenCitation1,Citation7,Citation33 revealed a significantly higher rate of stroke in older women than in their age-matched male counterparts. Although age as a nonmodifiable risk factor may explain higher rate of stroke in older women,Citation31,Citation34 the finding from the current study showed no significant difference between elderly men and women in age.
In-hospital mortality rate among elderly women was three times more than that among men, which supports a growing body of evidence showing a greater in-hospital mortality in women than in men after stroke.Citation4,Citation35 It seems that elderly women are not evaluated as elderly men and possibly not treated appropriately. The findings from a Swedish registry showed that older women were less likely to be treated with antithrombotic drugs and less likely to receive anticoagulation.Citation36 Similarly, another study showed that older women were less likely to have echocardiography or any carotid investigation after adjusting for other confounding factors such as age and initial stroke severity.Citation37
Since the main aim of the present study was to investigate sex disparities in stroke, we explored these differences from a socioeconomic perspective. The findings from the current study showed that older women, compared to older men, had lower socioeconomic status and were more likely being unmarried and living alone. These findings are consistent with the results of previous studies showing sex differences in socioeconomic statusCitation38,Citation39 and living conditions.Citation11,Citation17,Citation40 Multiple studies have found that people in low socioeconomic status and poor living conditions are more susceptible to acquiring chronic medical conditions and poorer health status.Citation18,Citation41 In parallel with previous studies,Citation23,Citation27 older women reported higher rates of past history of hypertension, diabetes mellitus, and depression, which might be associated with increased incidence of stroke.Citation42–Citation44 Older women are more vulnerable to social risk factors for depression than men.Citation45 Some studies show that low socioeconomic status is more closely associated with diabetes in women than in men.Citation46 The prevalence of hypertension is greater in women after menopause than in men, especially those with a history of hypertension during pregnancy. In addition, socioeconomic determinants of hypertension are more prevalent among women.Citation47,Citation48
Other findings from the current study showed a sex disparity in delayed hospital arrival, that is, elderly women had longer prehospital delay. This finding is consistent with the results of previous studies that have demonstrated elderly women, compared to men, are less likely to be admitted to the acute stroke care unit within the eligible time that may potentially delay treatment and results in poor stroke outcomes.Citation4,Citation27,Citation49,Citation50 In addition, some elderly female stroke participants might be managed at home by traditional techniquesCitation9 that may lead to poor stroke outcomes.
In sum, in line with some previous studies demonstrating that low socioeconomic status and poor living conditions are associated with increased incidence and mortality from stroke,Citation25,Citation41,Citation51 this study hypothesized that differences in socioeconomic status and living conditions between elderly men and women may explain part of sex disparities in sex differences in stroke in terms of incidence rate and outcomes. Our findings showing lower socioeconomic status and poorer living conditions for older female participants with stroke may account for part of sex disparities in stroke.
Although, to our knowledge, this study is one of the first studies exploring sex differences in stroke from a socioeconomic perspective and found interesting results, it has some limitations. First, no data on household income status of participants were available. However, it is noteworthy to mention that level of education and employment status can reflect income effect.Citation52 Second, the cross-sectional nature of the study precludes any definitive conclusion; therefore, a longitudinal study with a large sample size is required to confirm the proposed mechanism. The third limitation of the current study is that a multivariate analysis was not feasible, which may affect the results.
Conclusion
The findings from the current study supported some previous research studies showing that elderly women are more adversely affected by stroke in terms of incidence and in-hospital mortality of stroke than elderly men. The most noticeable result of our study was that sex differences in socioeconomic status and living conditions might result in higher rate of stroke incidence and poorer outcomes in elderly women. Therefore, it is imperative to identify vulnerable elderly women with stroke and provide them appropriate treatment and services.
Acknowledgments
This study was supported by Sabzevar University of Medical Sciences, Iran. The authors would like to thank Associate Professor Dr Robab Sahaf and anonymous reviewers for their helpful comments and suggestions for the revision and improvement in this manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
- HaastRAGustafsonDRKiliaanAJSex differences in strokeJ Cereb Blood Flow Metab201232122100210723032484
- CoxAMMcKevittCRuddAGWolfeCDSocioeconomic status and strokeLancet Neurol20065218118816426994
- PetreaREBeiserASSeshadriSKelly-HayesMKaseCSWolfPAGender differences in stroke incidence and poststroke disability in the Framingham Heart StudyStroke20094041032103719211484
- TurtzoLCMcCulloughLDSex differences in strokeCerebrovasc Dis200826546247418810232
- MorvicSRundekTDemarinVGender differences in strokePeriod Biol20121143267268
- AhangarAAAshraf VaghefiSBRamaezaniMEpidemiological evaluation of stroke in Babol, northern Iran (2001–2003)Eur Neurol2005542939716195668
- RothDLHaleyWEClayOJRace and gender differences in 1-year outcomes for community-dwelling stroke survivors with family caregiversStroke201142362663121257820
- GarganoJWReevesMJSex differences in stroke recovery and stroke-specific quality of life: results from a Statewide Stroke RegistryStroke20073892541254817673706
- FoerchCGhandehariKXuGKaulSExploring gender distribution in patients with acute stroke: a multi-national approachJ Res Med Sci2013181101623901335
- KimberlyWTLimaFOO’ConnorSFurieKLSex differences and hemoglobin levels in relation to stroke outcomesNeurology201380871972423365064
- ReevesMJBushnellCDHowardGSex differences in stroke: epidemiology, clinical presentation, medical care, and outcomesLancet Neurol200871091592618722812
- BushnellCDHurnPColtonCAdvancing the study of stroke in women: summary and recommendations for future research from an NINDS-Sponsored Multidisciplinary Working GroupStroke20063792387239916857945
- ReidJMDaiDGubitzGJKapralMKChristianCPhillipsSJGender differences in stroke examined in a 10-Year cohort of patients admitted to a Canadian teaching hospitalStroke20083941090109518292386
- TsaiKLLinCLHsuCIs gender-specific therapy necessary for patients of hemorrhagic stroke?J Exp Clin Med201246309312
- AddoJAyerbeLMohanKMSocioeconomic status and stroke an updated reviewStroke20124341186119122363052
- MarshallIJWangYCrichtonSMcKevittCRuddAGWolfeCDThe effects of socioeconomic status on stroke risk and outcomesLancet Neurol201514121206121826581971
- YahayaNAbdullahSSMomtazYAHamidTAQuality of life of older Malaysians living aloneEduc Gerontol20103610–11893906
- MomtazYAIbrahimRHamidTAYahayaNSociodemographic predictors of elderly’s psychological well-being in MalaysiaAging Ment Health201115443744521500010
- HamidTAMomtazYAAbdul RashidSNSOlder women and lower self-rated healthEduc Gerontol2010366521528
- WinklebyMAJatulisDEFrankEFortmannSPSocioeconomic status and health: how education, income, and occupation contribute to risk factors for cardiovascular diseaseAm J Public Health19928268168201585961
- KapralMKWangHMamdaniMTuJVEffect of socioeconomic status on treatment and mortality after strokeStroke200233126827511779921
- ArrichJMüllnerMLalouschekWGreiseneggerSCrevennaRHerknerHInfluence of socioeconomic status and gender on stroke treatment and diagnosticsStroke20083972066207218436881
- MomtazYAHamidTAYahayaNIbrahimREffects of chronic comorbidity on psychological well-being among older persons in Northern Peninsular MalaysiaAppl Res Qual Life201052133146
- Kautzky-WillerADornerTJensbyARiederAWomen show a closer association between educational level and hypertension or diabetes mellitus than males: a secondary analysis from the Austrian HISBMC Public Health20121239222646095
- LangagergaardVPalnumKHMehnertFSocioeconomic differences in quality of care and clinical outcome after stroke: a nationwide population-based studyStroke201142102896290221817140
- LazzarinoAIPalmerWBottleAAylinPInequalities in stroke patients’ management in English public hospitals: a survey on 200,000 patientsPLoS One201163e1721921399683
- BushnellCMcCulloughLDAwadIAGuidelines for the prevention of stroke in women: a statement for healthcare professionals from the American Heart Association/American Stroke AssociationStroke20144551545158824503673
- MomtazYAHamidTAIbrahimRYahayaNAbdullahSSModerating effect of Islamic religiosity on the relationship between chronic medical conditions and psychological well-being among elderly MalaysPsychogeriatrics2012121435322416828
- WiltshireJCRobertsVBrownRSartoGEThe effects of socioeconomic status on participation in care among middle-aged and older adultsJ Aging Health200921231433519091692
- AhmedSMTomsonGPetzoldMKabirZNSocioeconomic status overrides age and gender in determining health-seeking behaviour in rural BangladeshBull World Health Organ200583210911715744403
- Lloyd-JonesDAdamsRCarnethonMHeart disease and stroke statistics – 2009 update a report from the American Heart Association Statistics Committee and Stroke Statistics SubcommitteeCirculation20091193e21e18119075105
- AppelrosPStegmayrBTeréntASex differences in stroke epidemiology: a systematic reviewStroke20094041082109019211488
- DasSKBanerjeeTKBiswasAA prospective community-based study of stroke in Kolkata, IndiaStroke200738390691017272773
- CasoVPaciaroniMAgnelliGGender differences in patients with acute ischemic strokeWomens Health (Lond)201061515720088729
- PerskyRWTurtzoLCMcCulloughLDStroke in women: disparities and outcomesCurr Cardiol Rep201012161320425178
- GladerE-LStegmayrBNorrvingBSex differences in management and outcome after stroke a Swedish national perspectiveStroke20033481970197512855818
- WilliamsJEChimowitzMICotsonisGALynnMJWaddySPWASID InvestigatorsGender differences in outcomes among patients with symptomatic intracranial arterial stenosisStroke20073872055206217540969
- HamidTAMomtazYAIbrahimRPredictors and prevalence of successful aging among older MalaysiansGerontology201158436637022179496
- MomtazYAHamidTAYusoffSLoneliness as a risk factor for hypertension in later lifeJ Aging Health201224469671022422758
- MomtazYAHaronSAIbrahimRHamidTASocial embeddedness as a mechanism for linking social cohesion to well-being among older adults: moderating effect of genderClin Interv Aging2014986324904206
- ArrichJLalouschekWMüllnerMInfluence of socioeconomic status on mortality after stroke retrospective cohort studyStroke200536231031415625296
- O’DonnellMJXavierDLiuLRisk factors for ischaemic and intracerebral haemorrhagic stroke in 22 countries (the INTERSTROKE study): a case-control studyLancet2010376973511212320561675
- YongHFoodyJALinongJA systematic literature review of risk factors for Stroke in ChinaCardiol Rev2013212779322990372
- DelbariASalman RoghaniRTabatabaeiSSRahgozarMLokkJStroke epidemiology and one-month fatality among an urban population in IranInt J Stroke20116319520021557803
- CarayanniVStylianopoulouCKoulierakisGBabatsikouFKoutisCSex differences in depression among older adults: are older women more vulnerable than men in social risk factors? The case of open care centers for older people in GreeceEur J Ageing201292177186
- RathmannWHaastertBIcksASex differences in the associations of socioeconomic status with undiagnosed diabetes mellitus and impaired glucose tolerance in the elderly population: the KORA Survey 2000Eur J Public Health200515662763316051657
- BybeeKADewMLLawhornSLStevensTLCardiovascular Disease in Women EssentialsKansas City, MOJones & Bartlett Learning2012
- WarrellDACoxTMFirthJDOxford Textbook of Medicine1Cambridge, UKOxford University Press2003
- SmithMALisabethLDBonikowskiFMorgensternLBThe role of ethnicity, sex, and language on delay to hospital arrival for acute ischemic strokeStroke201041590590920339124
- LutfiyyaMNNgLAsnerNLipskyMSDisparities in stroke symptomology knowledge among US midlife women: an analysis of population survey dataJ Stroke Cerebrovasc Dis200918215015719251192
- PutmanKDe WitLSchoonackerMEffect of socioeconomic status on functional and motor recovery after stroke: a European multicentre studyJ Neurol Neurosurg Psychiatry200778659359917158561
- LitwakEKulisSTechnology, proximity, and measures of kin supportJ Marriage Fam1987493649661