
Abstract
Purpose
The aim is to systematically assess the effectiveness and safety of Chinese herbal formula Erxian decoction (EXD) for treating osteoporosis.
Materials and methods
Six databases were searched from inception through September 17, 2016, without language restriction. All randomized controlled trials of EXD for osteoporosis were included. One or more outcome measures including fracture, change in bone mineral density (BMD), pain symptom improvement, bone biochemical markers, quality of life, adverse event or adverse drug reaction were evaluated. Study selection, data extraction, quality assessment, and data analyses were conducted according to Cochrane standards.
Results
Eight trials including 644 patients investigated the effects of EXD in the treatment of osteoporosis. The methodological quality of the included trials was generally low. The meta-analysis from two trials showed favorable effects of EXD in improving BMD of lumbar spine (mean difference [MD]: 0.05 [0.03, 0.06]; I2=0%; P<0.00001) and BMD of femoral great trochanter (MD: 0.06 [0.02, 0.10]; I2=59%; P=0.005) compared with caltrate tablets. The other meta-analysis from two trials showed beneficial effects of EXD plus caltrate tablets and calcitriol in improving BMD of femoral neck (MD: 0.04 [0.00, 0.09]; I2=56%; P=0.04), the level of calcium (MD: 0.20 [0.15, 0.24]; I2=0%; P<0.00001), and phosphorus (MD: −0.28 [−0.39, −0.17]; I2=68%; P<0.00001) compared with caltrate tablets and calcitriol alone. The adverse drug reactions of EXD were mainly slight gastrointestinal symptoms.
Conclusion
The study provides suggestive evidence of the superiority of EXD monotherapy or combination therapy over basic supplements for treating osteoporosis. However, the evidence remains weak. More rigorously designed and measured, randomized double-blind, placebo-controlled trials with larger sample size are needed to verify the current conclusions.
Introduction
Osteoporosis is a pathological condition that can lead to the reduction of bone mass and the impairment of the bone architecture, which increases the risk of falling and fracture.Citation1,Citation2 The disease affects a large amount of the population, especially the elderly and postmenopausal women, being considered a very important problem as a growing concern of aging.Citation3 In the last two decades, significant progress has been made in epidemiology studies and in understanding its complex pathogenesis. However, the pathogenesis of osteoporosis is still complex and multifactorial, which makes us put more emphasis on preventing and treating this “silent disease”.Citation4,Citation5 Furthermore, a growing body of research evidence has fostered the development of clinical practice guidelines to monitor and provide appropriate choices for osteoporosis intervention.
Reducing loss of bone mass, adequately treating clinical symptoms, and preventing osteoporotic fractures are the major therapeutic targets. Therefore, osteoporosis management usually includes pharmacological approaches, physiotherapy interventions, health education measures, and in rare cases, surgical treatment.Citation6 Among the treatment strategies, the application of drugs in the management of osteoporosis remains a clinical challenge as a result of patient selection, potential adverse effects or patient adherence.Citation7 Calcium (Ca), vitamin D, bisphosphonates, and calcitonin are the commonly used medications. However, an increasing number of studies demonstrated that using these conventional medicines increased the risk of cardiovascular events.Citation8,Citation9 A recent study revealed that 8.5% reported low adherence to osteoporosis medications and 21.6% of patients stopped their medication completely over the 2-year follow-up period.Citation10 Therefore, there is a need to seek alternative and effective treatment alternatives for osteoporosis. Clinical practice has shown a bright future for Chinese herbal medicine and Chinese herbal formulas in treating osteoporosis.Citation11,Citation12
Erxian decoction (EXD), a traditional Chinese herbal formula, has been widely used for treating many chronic diseases, such as osteoporosis, menopausal syndrome, and delayed puberty in the past 60 years.Citation13,Citation14 EXD is made up of six herbs, containing Epimedii Folium (Yinyanghuo), Curculiginis Rhizoma (Xianmao), Morindae Officinalis Radix (Bajitian), Anemarrhenae Rhizoma (Zhimu), Phellodendri Chinensis Cortex (Huangbai), and Angelicae Sinensis Radix (Danggui).Citation13 Twelve anti-osteoporotic constituents, such as icariin, anemarsaponin BII, and berberine were isolated through bioactivity-guided fractionation.Citation15 More and more fundamental researches revealed that EXD had a definite anti-osteoporotic effect similar to estrogen.Citation16–Citation18 EXD displayed inhibitory effects on osteoclastic bone resorption, including decreasing the formation of bone resorption pits, the number of multinucleated osteoclasts, and so on.Citation19 A recent experimental study further confirmed that EXD could increase bone mass, elevate osteocalcin protein levels in vivo, and promote the self-renewal and osteoblastic differentiation of bone mesenchymal stem cells ex vivo in ovariectomized mice.Citation20
A previous systematic review and randomized double-blind controlled trial has shown that EXD is effective in improving menopausal symptoms.Citation21,Citation22 Nevertheless, there is no critically appraised evidence such as systematic reviews or meta-analysis to justify the clinical use of EXD for osteoporosis. Thus, the aim of the current systematic review is to investigate the effectiveness and safety of EXD for the condition.
Materials and methods
Search strategy
Two authors (Mu XH and Ma S) independently performed the literature search using predetermined inclusion/exclusion criteria. A computer-based online search was conducted in the PubMed, Embase, Cochrane Library, Chinese National Knowledge Infrastructure (CNKI), Chinese Scientific Journal Database (VIP), and Wanfang databases. In addition, the reference lists of all obtained articles were examined for additional studies. All the articles were considered without language limitation. All of the searches ended on September 17, 2016. Search terms were Erxian decoction (Er-xian decoction) combined with osteoporosis. The strategy for searching PubMed was listed: ((osteoporosis [MeSH Terms]) AND Erxian decoction) OR Er-xian decoction.
Study selection
Randomized controlled trials (RCTs) were included, but crossover randomized trials and quasi-randomized trials were excluded. Diagnosis of osteoporosis was established by bone mineral density (BMD) examination. The following interventions were considered for inclusion: EXD versus no treatment or placebo, EXD versus routine anti-osteoporosis medications, EXD plus anti-osteoporosis medications versus anti-osteoporosis medications, EXD plus anti-osteoporosis medications versus placebo plus anti-osteoporosis medications. Modified EXD changes based on traditional Chinese medicine syndrome differentiations were acceptable. The outcome measures included fracture, change in BMD, pain symptom improvement, bone biochemical markers, quality of life, adverse event, or adverse drug reaction (ADR). Any differences in opinion regarding inclusion in the review were resolved by discussion or consulting a third party.
Data extraction and analysis
Two investigators (Jia YS and Chai LM) independently extracted details of each included study: the principal authors, year of publication, sample sizes, patients’ characteristics, details of intervention, details of control interventions, intervention durations, and outcomes for each study. When important data were not available, authors of the relevant study were contacted and requested to provide missing data.
Two authors (Li JY and Wei X) assessed the RCTs based on a 7-item quality checklist from the Cochrane Handbook, comprising: 1) random sequence generation; 2) allocation concealment; 3) blinding of participants and personnel; 4) blinding of outcome assessment; 5) incomplete outcome data; 6) selective reporting; and 7) other bias.Citation23 The quality of RCTs was categorized into three levels: low risk of bias (all the items were assessed as having low risk of bias), high risk of bias (at least one item was assessed as having high risk of bias), and unclear risk of bias (at least one item’s risk of bias was in unclear). Discrepancies were resolved by consensus through discussion between the two investigators, if needed, by consulting a third party (Xu L).
Data analysis was conducted using the Review Manager 5.2 software provided by the Cochrane Collaboration. The mean difference (MD) was applied for studies using the same scale, and the standardized MD was utilized when the reported scales differed, along with 95% confidence intervals. For the meta-analysis of the traditional Chinese medicine compound recipe, random-effects model was used to analyze the data.Citation24 I2 values ≤50% indicated acceptable heterogeneity among studies. The relative strength of treatment efficacy was illustrated by forest plots. When possible, sensitivity analyses were conducted for all outcomes.
Results
Literature search results
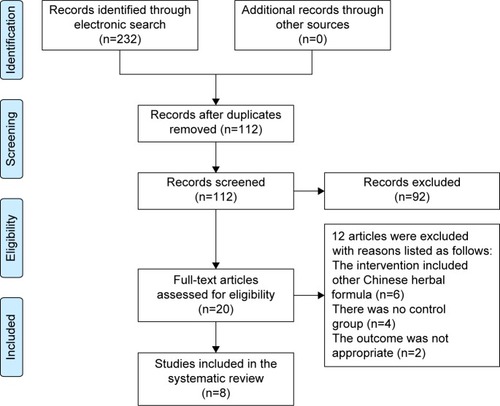
A flow chart depicted the search process and study selection (). A total of 232 articles were initially identified, all of which came from electronic databases. Full text papers of 20 studies were retrieved. Twelve articles were excluded with reasons listed as follows: the intervention included other Chinese herbal formula (n=6), there was no control group (n=4), and the outcome was not appropriate (n=2). Finally, a total of eight trials including EXD or modified EXD were included.Citation25–Citation32 All the papers were published in Chinese. Eight selected trials could be retrieved in the Chinese databases, including CNKI, VIP and Wanfang databases. The characteristics of included trials were listed in .
Table 1 Characteristics of included trials
Figure 1 Study selection process. Databases were PubMed, Embase, Cochrane Library, Chinese National Knowledge Infrastructure (CNKI), Chinese Scientific Journal Database (VIP), and Wanfang databases.
Study and participant characteristics
Eight trials involved a total of 644 patients diagnosed with osteoporosis. The variation in the mean age of participants was 40–70 years. Two trials enrolled middle- and old-aged people,Citation27,Citation30 five trials just enrolled postmenopausal women,Citation26,Citation28,Citation29,Citation31,Citation32 and one trial did not state the sex distribution of participants.Citation25 The different compositions of EXD or modified EXD were presented in . The controls were routine anti-osteoporosis medications which had six types of groups: 1) caltrate tablets, 2) salmon calcitonin, 3) hormonal treatment, including nilestriol or testosterone propionate, 4) caltrate tablets and calcitriol, 5) caltrate tablets and vitamin D plus alfacalcidol, and 6) elcatonin. The total treatment duration ranged from 2 months to 6 months. The outcome covered BMD, clinical symptoms score, bone metabolism markers, and ADRs.
Table 2 Composition of formula
Methodological quality of included trials
The methodological quality assessments were summarized in . All of the included trials were evaluated and deemed to be of generally poor methodological quality. Two trials stated that the method of random number table was used,Citation26,Citation29 one trial described the random allocation using SPSS software.Citation32 The others only mentioned that “subjects were randomized into two groups”, but did not report the detailed methods for sequence generation. None of the trials reported allocation concealment and used matched placebo to blind participants and practitioners. The number of dropout or withdrawal cases and intention-to-treat analysis were not mentioned, so the item “incomplete outcome data” was not identified. Selective reporting was unclear because the protocols of all the trials were not accessible. The baseline information on the age, sex, and the outcomes was not adequate in the four trials.Citation25,Citation28,Citation29,Citation31
Table 3 Methodological quality of the included trials
Fracture prevention and quality of life
None of the trials reported the fracture incidence and quality of life as the observed outcomes.
BMD
The trials that tested the BMD values in different parts of the body were analyzed.
Improvement of BMD in lumbar spine. Seven trials studied the benefits of improved BMD in lumbar spine and two meta-analyses could be performed.Citation25–Citation30,Citation32 Two studies including 128 participants compared the effect of EXD with caltrate tablets to measure the outcome.Citation25,Citation30 A meta-analysis showed a significant beneficial effect of EXD compared with caltrate tablets in improving BMD of lumbar spine (MD: 0.05 [0.03, 0.06]; I2=0%; P<0.00001) (). In addition, two studies including 208 participants compared the effect of EXD plus caltrate tablets and calcitriol with caltrate tablets and calcitriol.Citation28,Citation29 A pooled analysis indicated that there was no significant difference between the integrative therapy and routine treatment drugs in improving BMD of lumbar spine (MD: 0.08 [−0.03, 0.18]; I2=91%; P=0.15) ().
The other three trials were not included in meta-analyses.Citation26,Citation27,Citation32 One study by Zhu and Gu indicated EXD plus salmon calcitonin was better than the use of salmon calcitonin alone over a period of three months (P<0.05).Citation26 Anther study found a greater improvement in the EXD group compared to hormonal treatment over a period of two months (P<0.05).Citation27 Another study demonstrated that the result of the EXD plus elcatonin group was significantly better than elcatonin monotherapy in enhancing the BMD in lumbar spine L2 to L4 after three months (P<0.001).Citation32
Improvement of BMD in femoral neck. Five trials studied BMD in femoral neck, and one meta-analysis was conducted to evaluate the effect of the Chinese herbal formula.Citation27–Citation31 The meta-analysis from two trials demonstrated that EXD plus caltrate tablets and calcitriol was superior to caltrate tablets and calcitriol alone in improving BMD of femoral neck (MD: 0.04 [0.00, 0.09]; I2=56%; P=0.04) ().Citation28,Citation29
The other three trials were not included in meta-analyses.Citation27,Citation30,Citation31 Gao’s study showed EXD alone had a significant advantage compared to hormonal treatment in enhancing BMD of femoral neck (P<0.05).Citation27 Another study showed a significant treatment effect of modified EXD compared with caltrate tablets (P=0.009).Citation30 Xu et al confirmed the effect of combination therapy (modified EXD plus anti-osteoporosis medicine) was better than anti-osteoporosis medicine alone after three months of therapy (P<0.05).Citation31
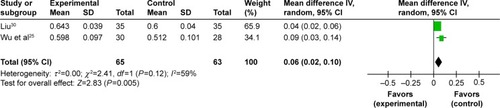
Improvement of BMD in femoral great trochanter. Three trials observed the effect of BMD in femoral great trochanter.Citation25,Citation27,Citation30 One meta-analysis could be performed.Citation25,Citation30 The meta-analysis showed there is significant beneficial effect in EXD group compared to caltrate tablets group (MD: 0.06 [0.02, 0.10]; I2=59%; P=0.005) (). The remaining trial reported that the EXD group experienced more benefits than the hormonal treatment group (P<0.05).Citation27
Improvement of BMD in Ward’s area. Two trials observed the effect of BMD in Ward’s area.Citation27,Citation30 One trial reported that EXD group experienced more benefits than the hormonal treatment group after two months (P<0.05).Citation27 The other trial also found modified EXD showed more improvement than caltrate tablets after two months of treatment (P<0.001).Citation30
Improvement of BMD in tibia. Only one trial assessed the effect of BMD in tibia.Citation32 The result revealed that the curative effect experienced by the EXD plus elcatonin group was better than the elcatonin group after three months (P<0.001).
Figure 2 Forest plot of comparison between EXD and caltrate tablets. The outcome was BMD in lumbar spine.
Abbreviations: EXD, Erxian decoction; BMD, bone mineral density; CI, confidence interval; SD, standard deviation; df, degrees of freedom.
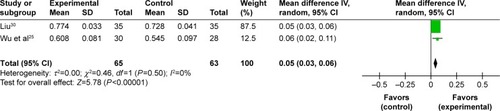
Figure 3 Forest plot of comparison between EXD plus caltrate tablets and calcitriol versus caltrate tablets and calcitriol. The outcome was BMD in lumbar spine.
Abbreviations: EXD, Erxian decoction; BMD, bone mineral density; CI, confidence interval; SD, standard deviation; df, degrees of freedom.
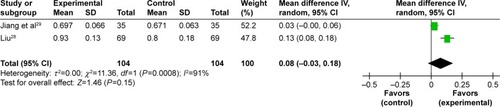
Figure 4 Forest plot of comparison between EXD plus caltrate tablets and calcitriol versus caltrate tablets and calcitriol. The outcome was BMD in femoral neck.
Abbreviations: EXD, Erxian decoction; BMD, bone mineral density; CI, confidence interval; SD, standard deviation; df, degrees of freedom.
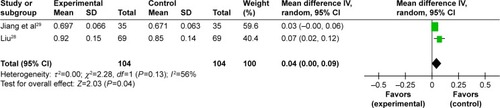
Figure 5 Forest plot of comparison between EXD and caltrate tablets. The outcome was BMD in femoral great trochanter.
Pain symptom
Two trials used the pain score as the outcome.Citation30,Citation32 One trial showed that the modified EXD was better than caltrate tablets in reducing pain (visual analog scale score) after two months (P<0.001). The other trial evaluated the pain-relieving effect of EXD plus elcatonin.Citation32 After three-month treatment, EXD plus elcatonin could significantly improve the pain symptom of osteoporosis compared with elcatonin alone (P<0.001).
Bone biochemical markers
The trials that measured the blood Ca, phosphorus (P), alkaline phosphatase (ALP), bone gla protein (BGP), calcitonin (CT), and estradiol (E2) were analyzed.
Improvement of Ca, P, ALP. Five trials analyzed the level of blood Ca and two meta-analyses were conducted.Citation25,Citation26,Citation28,Citation30 No statistical difference in blood Ca (MD: −0.13 [−0.28, 0.01]; I2=38%; P=0.06), blood P (MD: 0.13 [−0.19, 0.49]; I2=91%; P=0.39), and blood ALP (MD: −1.21 [−5.54, 3.12]; I2=0%; P=0.59) were found between the EXD group and caltrate tablets group. However, EXD plus caltrate tablets and calcitriol significantly increased the level of blood Ca (MD: 0.20 [0.15, 0.24]; I2=0%; P<0.00001) and lowered the level of blood P (MD: −0.28 [−0.39, −0.17]; I2=68%; P<0.00001) compared with caltrate tablets and calcitriol based on the meta-analysis. No statistical differences in blood ALP (MD: −1.87 [−7.58, 3.84]; I2=0%; P=0.52) were found between the integrative therapy group and routine treatment drugs group.
The other two trials were not analyzed in meta-analyses.Citation26,Citation31 One trial showed a statistically significant difference in favor of EXD plus salmon calcitonin in improving the level of ALP compared to salmon calcitonin (P<0.05) after three months.Citation26 The other showed a statistically significant difference in favor of the combination therapy in improving the level of ALP compared to caltrate tablets and vitamin D plus alfacalcidol (P<0.05) after three months.Citation31
Improvement of BGP, CT, E2. Two trials analyzed the level of blood BGP, CT, E2 and no meta-analysis could be conducted.Citation26,Citation31 The statistical data indicated that EXD plus salmon calcitonin was better than salmon calcitonin alone with regard to increasing the level of BGP (P<0.05), CT (P<0.05), E2 (P<0.01) after three months.Citation26 The other data also indicated that the combination therapy was better than caltrate tablets and vitamin D plus alfacalcidol with regard to increasing the level of E2 (P<0.05) after three months.Citation31
Adverse effects
Three trials (3/8) reported the ADRs.Citation28,Citation29,Citation32 One trial demonstrated 1 case with abdominal distension (1/69, 1.45%), 3 cases (2/69, 4.35%) with constipation and 2 cases (2/69, 2.90%) with stomach upset in the modified EXD plus caltrate tablets and calcitriol group.Citation28 However, the occurrence of ADRs was higher in the caltrate tablets and calcitriol group (P<0.05), including 5 cases with abdominal distension (5/69, 7.25%), 7 cases (7/69, 10.14%) with constipation, and 6 cases (6/69, 8.70%) with stomach upset. Another trial exhibited 1 case with diarrhea (1/40, 2.5%) in the EXD group, 1 case with facial flushing (1/40, 2.5%), and 1 case with nausea (1/40, 2.5%) in the elcatonin group.Citation32 And the adverse effects were not serious in the Chinese medicine group. No ADRs were found in another trial.Citation29 The remaining five trials did not mention whether the adverse events were monitored.
Publication bias
The funnel plots were not conducted due to the inadequate number of included osteoporosis studies.
Discussion
Plant-based therapies including traditional Chinese medicines have long been used to prevent and treat osteoporosis and have received extensive attention.Citation33–Citation35 According to the theory of Chinese medicine, Shen-Jing deficiency (Kidney essence) plays an important part in the development of osteoporosis and is better for diagnosing osteoporosis.Citation36 Therefore, kidney-tonifying herbs or herbal formula contribute to treating both the disease and the Chinese medicine syndromes.Citation36,Citation37 Among the several Chinese medicine prescriptions, EXD is one of the most representative formulas reflecting kidney-tonifying principle.Citation38 To our knowledge, this is the first systematic review on EXD for osteoporosis with regard to different outcomes.
A detailed analysis was performed based on the different interventions, controls, and outcomes. One aggregated result indicated that EXD was more effective for participants in increasing BMD of lumbar spine and femoral great trochanter than for those in the caltrate tablets group in only two studies. The other aggregated result showed that EXD plus caltrate tablets and calcitriol was more effective in increasing BMD of femoral neck and improving the level of blood Ca and P than caltrate tablets and calcitriol in only two studies. Additionally, two independent trials showed that modified EXD or EXD plus elcatonin significantly improved pain symptoms in patients with osteoporosis. The ADR of EXD might be abdominal distension, constipation, diarrhea, and stomach upset.
In our review, quality of life was not observed in the previous studies. Also, there was insufficient evidence to support or refute the value of EXD monotherapy or combination therapy compared with other active therapies alone because of the limited number of studies. A randomized double-blind, placebo-controlled trial was not found in the literature. Thus, the definite effect of Chinese medicine still needs to be proven by scientific research. Placebo control is of equal importance as active control in clinical trials of Chinese medicine.Citation39 Further studies should first compare EXD with placebo or no treatment. More standard therapies, such as bisphosphonate or exercise, need to be considered as a control. Our results indicated that a minimal valid duration of EXD for osteoporosis might be at least 2 months. Nevertheless, the longer duration may achieve better gains. Unlike diabetes and hypertension, conventional drugs for osteoporosis can bring persistent structural benefits.Citation40,Citation41 But so far the long-term effects and safety of EXD are still unknown.
Before accepting the above findings, the following limitations should be noted. First, in all the articles published in People’s Republic of China, there were no data about the effect of EXD for treating osteoporosis in other countries. Therefore, the potential selection bias could not be ruled out. Second, the majority of studies failed to report the random method, did not use blinding, did not describe the number and the reason of withdrawal, and did not register the study protocol. Similar to the several systematic reviews of alternative medicine for osteoporosis, the methodological quality of RCTs is the major problem affecting the efficacy evaluation.Citation42,Citation43 The researchers of Chinese medicine should attach more importance to improve reporting quality using the Consolidated Standards of Reporting Trials (CONSORT) statement.Citation44 Third, our results may be affected by the modified herbs, dosing parameters of EXD, and treatment duration. Fourth, the information on the adverse events or ADR is inadequate. The safety of EXD needs to be rigorously monitored in future clinical trials. Due to the poor quality of the previous studies, the results of our review are likely to be influenced by many factors.
Conclusion
The present meta-analysis proved that EXD monotherapy or EXD plus caltrate tablets and calcitriol for osteoporosis may have beneficial effects on the improvement of BMD at anatomical sites. EXD plus caltrate tablets and calcitriol can significantly improve the level of Ca and P. As a result of the methodological drawbacks in the previous studies, more rigorously designed and measured, randomized double-blind, placebo-controlled trials with larger sample size are needed to verify the current conclusions.
Acknowledgments
The authors are thankful for the financial support from National Natural Science Foundation of China (81503601) and Science and Technology Program of Beijing Administration of Traditional Chinese Medicine (JJ2015-57). The authors would like to thank Yukun Yin from Indiana University Purdue University Indianapolis for revising the English language of this paper.
Disclosure
The authors report no conflicts of interest in this work.
References
- HernlundESvedbomAIvergårdMOsteoporosis in the European Union: medical management, epidemiology and economic burden. A report prepared in collaboration with the International Osteoporosis Foundation (IOF) and the European Federation of Pharmaceutical Industry Associations (EFPIA)Arch Osteoporos2013813624113837
- LinXXiongDPengYQEpidemiology and management of osteoporosis in the People’s Republic of China: current perspectivesClin Interv Aging2015101017103326150706
- AbobuluiMBergheaFVladVEvaluation of adherence to anti-osteoporosis treatment from the socio-economic contextJ Med Life20158Spec Issue11912326361520
- RosenCJThe Epidemiology and Pathogenesis of OsteoporosisEndotext2014
- Mafi GolchinMHeidariLGhaderianSMAkhavan-NiakiHOsteoporosis: a silent disease with complex genetic contributionJ Genet Genomics2016432496126924688
- PaolucciTSaraceniVMPiccininiGManagement of chronic pain in osteoporosis: challenges and solutionsJ Pain Res2016917718627099529
- BollandMJGreyAAvenellAGambleGDReidIRCalcium supplements with or without vitamin D and risk of cardiovascular events: reanalysis of the Women’s Health Initiative limited access dataset and meta-analysisBMJ2011342d204021505219
- MarakaSKennelKABisphosphonates for the prevention and treatment of osteoporosisBMJ2015351h378326333528
- WangJCChienWCChungCHLiaoWITsaiSHAdverse cardiovascular effects of nitrogen-containing bisphosphonates in patients with osteoporosis: a nationwide population-based retrospective studyInt J Cardiol201621523223727128537
- ClarkEMGouldVCTobiasJHHomeRNatural history, reasons for, and impact of low/non-adherence to medications for osteoporosis in a cohort of community-dwelling older women already established on medication: a 2-year follow-up studyOsteoporos Int2016272579590
- WangLLiYGuoYHerba Epimedii: an ancient Chinese herbal medicine in the prevention and treatment of osteoporosisCurr Pharm Des201622332834926561074
- SiuWSWongHLLauCPThe effects of an antiosteoporosis herbal formula containing epimedii herba, ligustri lucidi fructus and psoraleae fructus on density and structure of rat long bones under tail-suspension, and its mechanisms of actionPhytother Res201327448449222628292
- LiJJLiJTFuJPErxian tang – introduction of a Chinese herbal formula, clinical practice, and experimental studiesChin J Integr Med2007131677317578324
- ZhuZLiLJinXFangJZhangDEr-Xian decoction, a traditional Chinese herbal formula, intervening early in hypothalamic-pituitary axis of male rats with delayed pubertyPharmacogn Mag2014104051752125422555
- QinLHanTZhangQAntiosteoporotic chemical constituents from Er-Xian decoction, a traditional Chinese herbal formulaJ Ethnopharmacol2008118227127918501540
- NianHQinLPZhangQYZhengHCYuYHuangBKAntiosteoporotic activity of Er-Xian decoction, a traditional Chinese herbal formula, in ovariectomized ratsJ Ethnopharmacol200610819610216765003
- XueLWangYJiangYComparative effects of Er-Xian decoction, epimedium herbs, and icariin with estrogen on bone and reproductive tissue in ovariectomized ratsEvid Based Complement Alternat Med2012201224141623227099
- WongKCLeeKSLukHKEr-xian Decoction exerts estrogen-like osteoprotective effects in vivo and in vitroAm J Chin Med201442240942624707871
- XueLJiaoLWangYEffects and interaction of icariin, curculigoside, and berberine in er-xian decoction, a traditional Chinese medicinal formula, on osteoclastic bone resorptionEvid Based Complement Alternat Med2012201249084323243450
- LiuSHuangJWangJEr-Xian Decoction stimulates osteoblastic differentiation of bone mesenchymal stem cells in ovariectomized mice and its gene profile analysisStem Cells Int20162016407921027064269
- ChenHYChoWCSzeSCTongYTreatment of menopausal symptoms with Er-xian decoction: a systematic reviewAm J Chin Med200836223324418457358
- ZhongLLTongYTangGWA randomized, double-blind, controlled trial of a Chinese herbal formula (Er-Xian decoction) for menopausal symptoms in Hong Kong perimenopausal womenMenopause201320776777623793167
- HigginsJPTGreenSCochrane Handbook for Systematic Reviews of Interventions, Version 5.1.0The Cochrane Collaboration2009
- ZhangWWangSZhangREvidence of Chinese herbal medicine Duhuo Jisheng decoction for knee osteoarthritis: a systematic review of randomised clinical trialsBMJ Open201661e008973
- WuJZZhouXMZhengCXThe clinical observation of Erxian decoction for primary osteoporosisXin Zhong Yi20104222526
- ZhuQAGuMQEfficacy of salmon calcitonin plus erxian decoction (EXD) for osteoporosis in postmenopausal women: a clinical observationZhong Hua Zhong Yi Yao Xue Kan201242228062809
- GaoCThe clinical observation of erxian decoction for primary osteoporosisHai Xia Yao Xue2012247103104
- LiuYNThe clinical observation of modified erxian decoction for postmenopausal osteoporosisZhong Guo Zhong Xi Yi Ji Chu Yi Xue Za Zhi2012188886899
- JiangHLeXLiuDLThirty-five cases efficacy observation of modified erxian decoction for postmenopausal osteoporosisZhong Guo Yao Fang2014251725692571
- LiuHThe efficacy observation of erxian decoction for primary osteoporosisDang Dai Yi Xue20141274445
- XuXLMaXSunJJThe clinical observation and influence on E2, ALP of modified erxian decoction in the treatment of postmenopausal osteoporosisZhong Guo Zhong Yi Yao Ke Ji20162316874
- YeBLLiSHLiSLClinical study on erxian decoction combined with elcatonin in the treatment of postmenopausal osteoporosisZhong Guo Zhong Yi Yao Xin Xi Za Zhi20162362326
- AnJYangHZhangQNatural products for treatment of osteoporosis: the effects and mechanisms on promoting osteoblast-mediated bone formationLife Sci2016147465826796578
- GuoYLiYXueLSalvia miltiorrhiza: an ancient Chinese herbal medicine as a source for anti-osteoporotic drugsJ Ethnopharmacol201415531401141625109459
- LiuYLiuJPXiaYChinese herbal medicines for treating osteoporosisCochrane Database Syst Rev20143CD005467
- ShuBShiQWangYJShen (Kidney)-tonifying principle for primary osteoporosis: to treat both the disease and the Chinese medicine syndromeChin J Integr Med201521965666126432789
- RenYBHuangJHCaiWJShenZYShen-Jing as a Chinese medicine concept might be a counterpart of stem cells in regenerative medicineChin J Integr Med Epub201574
- LinLWuSTangJClinical observation and experimental study of the treatment of aplastic anemia by warming and tonifying the spleen and kidneyZhong Xi Yi Jie He Za Zhi1990105272274259 Chinese2397541
- WuJPlacebo control and clinical trial of Chinese medicineZhong Xi Yi Jie He Xue Bao2010810906910 Chinese20939980
- IdolazziLFassioAGattiDDuration of treatment for osteoporosisReumatismo2013651223523550257
- AdlerRADuration of anti-resorptive therapy for osteoporosisEndocrine201651222222426433739
- WangZQLiJLSunYLChinese herbal medicine for osteoporosis: a systematic review of randomized controlled trailsEvid Based Complement Alternat Med2013201335626023431336
- WeiXXuAYinYZhangRThe potential effect of Wuqinxi exercise for primary osteoporosis: a systematic review and meta-analysisMaturitas201582434635426386831
- HeJDuLLiuGQuality assessment of reporting of randomization, allocation concealment, and blinding in traditional Chinese medicine RCTs: a review of 3159 RCTs identified from 260 systematic reviewsTrials20111212221569452