
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Neurological injuries such as stroke can lead to proprioceptive impairment. For an informed diagnosis, prognosis, and treatment planning, it is essential to be able to distinguish between healthy performance and deficits following the neurological injury. Since there is some evidence that proprioception declines with age and stroke occurs predominantly in the elderly population, it is important to create a healthy reference model in this specific age group. However, most studies investigate age effects by comparing young and elderly subjects and do not provide a model within a target age range. Moreover, despite the functional relevance of the hand in activities of daily living, age-based models of distal proprioception are scarce. Here, we present a proprioception model based on the assessment of the metacarpophalangeal joint angle difference threshold in 30 healthy elderly subjects, aged 55–80 years (median: 63, interquartile range: 58–66), using a robotic tool to apply passive flexion–extension movements to the index finger. A two-alternative forced-choice paradigm combined with an adaptive algorithm to define stimulus magnitude was used. The mixed-effects model analysis revealed that aging has a significant, increasing effect on the difference threshold at the metacarpophalangeal joint, whereas other predictors (eg, tested hand or sex) did not show a significant effect. The adaptive algorithm allowed reaching an average assessment duration <15 minutes, making its clinical applicability realistic. This study provides further evidence for an age-related decline in proprioception at the level of the hand. The established age-based model of proprioception in elderly may serve as a reference model for the proprioceptive performance of stroke patients, or of any other patient group with central or peripheral proprioceptive impairments. Furthermore, it demonstrates the potential of such automated robotic tools as a rapid and quantitative assessment to be used in research and clinical settings.
Introduction
Proprioception consists of limb position sense (sense of stationary position) and kinesthesia (sense of limb movement).Citation1 Proprioceptive information originates from muscle spindle afferents, mechanoreceptors in joint capsules and cutaneous tactile receptors.Citation2,Citation3 The perception and correct interpretation of proprioceptive inputs is an essential prerequisite for many activities of daily living (ADL),Citation4 such as haptic exploration of objectsCitation5 and grasping.Citation6 Proprioceptive function can be impaired, for example, as a result of peripheral or central neurological injuries, as in about half of stroke patients.Citation7,Citation8 There is some evidence that proprioceptive impairments reduce the probability of functional recovery,Citation9 which motivates an increased attention to assessing and treating proprioceptive deficits. To be able to quantify these impairments, normative data from the healthy population are required. There is some literature showing that proprioception in healthy subjects declines with increased age (also referred to as presbypropria,Citation10 for review, Goble et alCitation11). Although the effect of age-related proprioceptive changes in the lower limbs on postural control in the elderly has been studied widely, relatively few studies have focused on the upper limbs, despite their importance for ADL.Citation4–Citation6 The decline in proprioceptive performance in more proximal joints (ie, shoulder, elbow, and wrist) could be demonstrated in a set of different experimentsCitation12–Citation18 using mostly matching paradigms. For more distal joints (ie, in the hand) there exist some inconsistent results.Citation19–Citation22 The age-related effect on proprioception is usually investigated by comparing a young group of healthy subjects with an elderly group of healthy subjects. However, the incidence of neurological injuries may vary depending on the age, as it is the case for stroke, where incidence by age doubles each decade after the age of 55.Citation23 Thus, stroke predominantly affects the elderly population. Therefore, to differentiate, for example, between healthy aging and proprioceptive deficits following a stroke, it would be of higher clinical utility to have a detailed model of how proprioception is affected by age within the target age group. To create a valid and accurate reference model, it is essential to base it on outcome measures from reliable and quantitative assessments.
Proprioception is commonly assessed with clinical tests, such as the up-down test in which the finger or toe is moved passively and the patient has to report the direction of movement,Citation1,Citation24 or a recent extension to the latter, named dual joint position test, where two digits are simultaneously moved in the same or reverse direction, which was shown to be superior.Citation25 However, these tests are administered manually and suffer from poor inter-rater reliability and sensitivity.Citation26 Due to the use of ordinal scales, these tests do not provide a precise quantification of proprioceptive function, and the provided outcome measures cannot serve as a basis for a reference model.
With the development of novel methods combined with simple tools, it has become possible to create fine-graded scales.Citation21,Citation27,Citation28 Since with robotic technology it is possible to reduce or prevent manual intervention of the experimenter (eg, repositioning of the limb) and to take advantage of the control and sensing capabilities of robotic devices, stimuli can be presented in a more reproducible and well-controlled manner. This is suggested to increase reliability as well as sensitivityCitation29 or may reduce flooring and ceiling effects by using continuous outcome measures. As a result, many different studies quantifying proprioception with the help of robotic tools in combination with various assessment paradigms have emerged.Citation12,Citation22,Citation30–Citation38 These kinds of assessments would allow creating reference models of healthy performance as a function of age. However, so far there exists only a very limited number of models, namely, for arm position matchingCitation12 and grasp aperture discrimination using spherical objects.Citation21 Hence, since different assessment paradigms may target particular aspects of proprioception, it is necessary to create models, specific to the proprioceptive task, describing healthy performance of a target age group.
The purpose of this study was to create a model of proprioceptive function at the metacarpophalangeal (MCP) joint of the index finger in healthy elderly subjects to be used as a reference model for the prospective evaluation of proprioceptive deficits following peripheral and central neurological injuries, such as stroke. The index finger is essential for most grasp types used in ADL,Citation39–Citation41 and flexion of the MCP is a strong contributor to a major synergy for natural grasp patterns.Citation42 The MCP joint angle difference threshold or limen (DL) was assessed with an automated robotic tool using an adaptive procedure named Parameter Estimation by Sequential Testing (PEST)Citation43 in a two-alternative forced-choice (2AFC)Citation44 paradigm. The influence of age, sex, dominance of the tested hand, finger length, measurement order, and number of trials on the DL was examined. We hypothesized that the model would reveal a major influence of age on the DL, thus, demonstrating the sensitivity of the proposed assessment method and its suitability for research on proprioception as well as clinical settings for a more informed diagnosis, prognosis, and treatment planning after stroke or other neurological injuries.
Methods
Subjects
Thirty healthy elderly subjects (S01–S30, 62.8±6.4 years, range 55–80 years, 14 males and 16 females, 29 right and 1 left handed) completed the study. Average finger length (measured from the MCP joint to the tip of the index finger) was 97.3±7.2 mm (across both hands). Handedness was assessed with the Edinburgh Handedness Inventory.Citation45 Subjects were excluded from the study if they had somatosensory or motor deficits affecting hand function, or any history of neurological (central or peripheral) or hand injury. Before participating in the experiment, all subjects provided written informed consent. Ethical approval was obtained from the institutional ethics committee of ETH Zurich and the University of Konstanz.
Robotic apparatus
The assessment of MCP joint proprioception was performed with the Robotic Sensory Trainer () previously used in a pilot study.Citation36 This device can provide well-controlled and reproducible passive finger movements (flexion and extension) around the MCP joint through an actuated remote center of motion (RCM) mechanism.Citation32 The index finger is attached by means of two Velcro® straps to a sliding finger carriage mounted on the RCM mechanism. The hand and forearm supports can be adjusted with 6 degrees of freedom to allow for a comfortable posture. The tested hand of the subject is occluded from vision by a touchscreen to avoid visual cues on finger position. The subject can provide feedback on perceived stimuli directly on the touch-screen placed above the tested hand by using the nontested hand. Based on LabVIEW (National Instruments, Austin, TX, USA), the assessment runs autonomously and does not require intervention of the experimenter once initiated.
Figure 1 Side view on the RCM mechanism of the robotic device used to induce passive movements around the MCP joint.
Abbreviations: MCP, metacarpophalangeal; RCM, remote center of motion.

Experimental protocol
Subjects were seated in front of the assessment apparatus, and forearm, hand and index finger were strapped to the device after adjusting the supports. The MCP joint was carefully aligned with the RCM indicated by the extension of the black arrow mounted on the device (). The MCP joint position DL was assessed for the index fingers of both hands in randomized order within one experimental session.
Every trial consisted of two successive passive finger movements to different flexion angles of the MCP joint (two-interval design, ). Passive movements were induced by the robotic apparatus, always starting from the same resting position (with all finger segments aligned, indicated by the dashed line in ). Flexion movements and movements back to resting position lasted 1 s each, whereas the MCP flexion angle was maintained for 1.5 s. According to the 2AFC paradigm, subjects were asked after each trial to indicate on the touchscreen, using the nontested hand, which of the two presented angular displacements was larger. No feedback on correctness of the answer was provided. The difference between the two angles was defined as positive and centered around the flexion reference of 20°. The difference was adjusted from trial to trial using the adaptive PEST algorithmCitation43 in order to converge toward the DL. PEST is based on a set of heuristic rules taking the subject’s responses to past stimuli into account, leading to smaller stimulus differences in case of high proportion of correct responses, and larger difference in case of low proportion of correct responses. The range of angular differences was limited to (0°, 40°) due to the mechanical limitations of the device. The same starting parameters (first presented angular difference of 5.5°, and first decreasing or increasing step of 2°), termination conditions (minimum step of ±0.1°, or 20 consecutive trials at the same level), and logarithmic mapping as reported for the previous pilot studyCitation36 were used. A maximum of 120 trials was permitted in case of nonconvergence, in order to keep the assessment duration short. These parameter values were selected based on our prior experimental knowledge and experience.
Data analysis
In order to estimate the DL from the experimental data, the proportion of correct responses at stimulus levels x (ie, at differences between the consecutively presented angles) was fitted with the psychometric function ψ(x) in Equation(1)(1) using a Maximum Likelihood criterion:Citation46
F(x) corresponds to a cumulative normal function with the inflection point at α and the slope β at this point. The guessing rate γ was set to 0.5, according to the 2AFC paradigm, and the lapse rate λ (taking into account stimulus-independent errors, or “lapses”) was allowed to vary between 0 and 0.1, to reduce estimation bias.Citation47 The DL is defined at x = ψ−1 (0.75). The Weber fraction K (DL divided by the reference angle, here 20°) is reported together with the group average DL in degrees. Such a hybrid procedure combining adaptive sampling procedures and fitting of parametrized functions, as described by Hall,Citation48 allows estimating the DL even when the adaptive sequence (here PEST sequence) does not converge and terminate within a maximum number of trials.Citation36
A linear mixed-effects model analysis to describe the DL was performed. As fixed effects, age (in years), sex (male versus female), tested hand (dominant versus nondominant), index finger length (in millimeters), measurement order (first versus second assessment within the session), and number of trials were entered into the model. Furthermore, the interaction between the factors tested hand and measurement order was included. As random effects, intercepts for the subjects were added. Handedness (right versus left) was not included into the model, as the right and left handed groups were not balanced (29/1). A log10 transform was applied to the DL before fitting the model, since the DL is only supported in the positive, semi-infinite interval (0, ∞). Visual inspection of residual plots did not reveal any obvious deviations from homoscedasticity or normality when using the log10 transform. Furthermore, the predictors were tested for collinearity. In order to assess the significance of fixed effects, the P-values were obtained by simulated (n=1,000) likelihood ratio tests (LRTs, MATLAB function compare) of the full model HA with the effect in question against the model H0 without the effect in question. This method generates a reference distribution of the LRT statistic X2 under H0 and compares it to the observed X2. This is computationally more intensive, but could be more accurate than comparing the test statistic X2 to a χ2-distribution using an analysis of variance, which is not always a very good approximation and tends to be anticonservative. To test whether clinical utility could be improved by reducing the maximum number of trials (120 to 60) to shorten the assessment duration, the same mixed-effects model analysis was conducted with truncated PEST sequences.
Significance levels were set to α=0.05. Descriptive statistics are reported as mean ± standard deviation (SD). All statistical analyses were performed in MATLAB R2014a (MathWorks, Natick, MA, USA).
Results
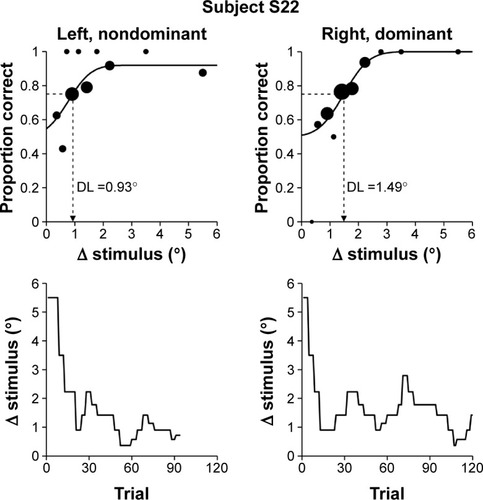
At group level (both hands), the MCP joint angle position DL averaged at 1.81°±0.96° (K=9.0%±4.8%). On average, 65.3±27.3 trials (ranging from 24 to 120) were required, resulting in an average duration of 14.3±6.0 min per assessment. In 5 out of the 60 assessments, the PEST algorithm did not converge, leading to a convergence rate of 91.7%. The psychometric functions fitted to the proportion of correct responses and the evolution of the corresponding PEST sequences for both hands are shown for a representative subject (S22) in . As visible in the top plots, stimulus levels are primarily sampled around the steeper part of the psychometric function, and the DL of the left, nondominant hand is smaller. In addition, only the assessment of the left, nondominant hand converged prior to 120 trials (bottom plots).
Figure 2 Resulting psychometric functions and PEST sequences of a representative subject.
Abbreviations: DL, difference threshold or limen; PEST, Parameter Estimation by Sequential Testing.
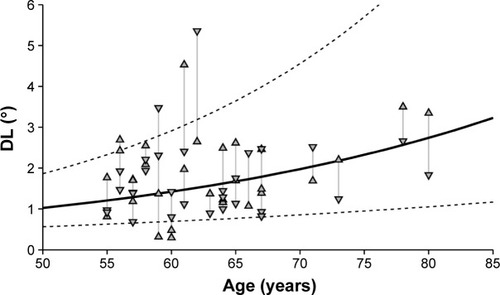
The mixed-effects model analysis revealed that age significantly affected the DL in increasing manner according to the simulated LRT (Page=0.029). The effect of age on the DL is illustrated in using averaged parameters of this sample multiplied by the estimates of the corresponding predictors not in question. Adding other fixed effects, that is, sex, finger length, handedness, tested hand, measurement, and number of trials as well as the interaction between tested hand and measurement, did not significantly improve the model for estimating the DL. Despite handedness not significantly improving the model, in 19 of 30 subjects, the DL of the nondominant hand was lower compared to the DL of the dominant hand. The simplest model for estimating the DL in healthy elderly (age range: 55–80 years) containing only the fixed effect age and a constant accounting for the other parameters was DL =10(0.014⋅age – 0.703) in degrees. The complete summary of the mixed-effects model is provided in . When truncating the assessment to a maximum of 60 trials, the number of trials was 51.5±11.9 on an average, with 33 of 60 assessments requiring all 60 trials. The changes in the model were minor (DL =10(0.015⋅age – 0.704), simulated LRT Page=0.032, all other P-values >0.05).
Table 1 Summary of the mixed-effects model analysis with the estimates and their SE predicting the log10DL
Figure 3 Age–DL relationship.
Abbreviations: DL, difference threshold or limen; SE, standard error.
Discussion
This study aimed to create a model of MCP joint proprioception in the healthy elderly population to serve as a reference for patients suffering from proprioceptive deficits. Proprioception was quantified by the joint angle DL and assessed with a robotic tool applying well-controlled flexion movements to the index finger. As hypothesized, the proposed assessment approach is sensitive enough to capture a declining effect of MCP joint proprioception with increasing age. According to the model, the index finger MCP joint angle DL increases by around 2° from age 55 to 80. Furthermore, age was the only fixed effect having a significant influence on the DL, and it is thus essential to include it in a model of proprioception.
Age-related decline of proprioception
The observed age effect is consistent with most of the literature on proprioception at more proximal jointsCitation12–Citation18 and distal joints.Citation20–Citation22 This decline in proprioception could be a consequence of increased proprioceptive attentional demand in older adultsCitation10 due to age-related centralCitation49 or peripheralCitation12 physiological changes (for review, Goble et alCitation11). However, there are also studies showing no age-related decline,Citation16,Citation19 or some showing age-related deficits depending on the task.Citation50 At the level of the hand, the assessment of proximal inter-phalangeal joint position sense through position matching using a robotic tool that induced velocities below the movement detection threshold, reported a significant deterioration from the young to the elderly group, as well as a moderate, but significant, positive correlation (r=0.466) between age and the magnitude of the matching error.Citation20 Similarly, comparisons between different age groups in two proprioceptive tasks (indicating overlap of fingers during passive crisscross movements and onset of passive finger movement) revealed larger errors in the elderly. In addition, an increase of 0.4 decision errors/decade for a total of 21 decisions was reported for an assessment where subjects had to indicate whether they perceived a comparison polystyrene ball to be larger, smaller, or equal to the volume of reference polystyrene ball.Citation21 In contrast, a study also assessing proprioception at the MCP joint, but by determining the detection threshold of sinusoidal movements, reported no major age-related decline in joint motion sensation.Citation19 However, it is difficult to compare the different findings on age-related changes in proprioception quantitatively due to the diversity of outcome measures arising from the different experimental paradigms. Models reported in the literature are based on matching paradigms and provide matching errors,Citation12,Citation20,Citation21 which cannot be directly related to different thresholds of proprioceptive perception.
One limitation of this study is the fact that the created model is limited to an age range of 55–80 years, and that the recruited subjects were not uniformly distributed across age. In particular, the number of subjects with age >70 years was small. However, additional verification of the model parameters showed that the model was robust to exclusion of the four most elderly subjects (>70 years), demonstrating that the effect of declining proprioception is supported by the entire data set. Furthermore, no comparison to a young group of healthy subjects was made. Yet, as expected, the group average of the DL in the elderly sample population of this study is slightly higher compared to the one reported for healthy young subjects (1.73°, K=8.6%) in the pilot study using the same apparatus and practically identical protocol.Citation36 Furthermore, although the incidence by age doubles each decade after the age of 55,Citation23 the age range of our study covers the major part of our target population. Although the comparison of young and elderly subjects can support the investigation of age-related changes, it has limited clinical value compared to an age-based reference model.
Influence of hand dominance and sex
Although the mixed-effects model did not show a significant effect of the tested hand (dominant versus nondominant) on the DL, about two-thirds of the subjects showed a better performance (ie, lower DL) with the nondominant limb. This trend is well in line with some literature, suggesting proprioceptive processing advantages of the nondominant limb in some conditions,Citation12,Citation16,Citation51–Citation55 while others suggest gain differences of sensory-motor loops as an explanation.Citation56 In contrast to those studies, other groups did not identify any difference between dominant and nondominant limb.Citation18,Citation22 There are also studies showing smaller matching errors with the dominant limb.Citation28 It has been suggested that long-term use-dependent superiority of the dominant hand may enhance proprioception.Citation57 As a conclusion, proprioception may be superior in the nondominant limb, although the dominant hand is generally more dexterous. However, as the results from the different studies show, this may strongly depend on the assessment paradigm used, as motor function may be a strong confound in some assessments, as for example in active matching tasks.
As in most previous studies, we did not find an effect of sex on proprioception.Citation16,Citation28,Citation51,Citation58 There was one study that identified sex-related differences, however, only in some of the outcome measures of a matching task including movements of the elbow and shoulder.Citation12
Robustness to fatigue and learning, number of trials, and clinical utility
Based on the results from this study, the DL is robust with respect to the measurement order (first versus second of two consecutive assessments, also if hand dominance is taken into account) and the number of trials. Whether the dominant/nondominant hand was assessed first or second within the session had no influence on the DL. This suggests that there is no learning effect of the task, which is essential for an assessment, as the goal is to measure the capacity of the subject and not the improvement due to increased level of familiarization with the task. Despite both hands being assessed consecutively, no fatigue effect could be observed. It could be, though, that learning and fatigue effects cancel each other. However, the fact that a larger number of trials does not have a significant influence on the DL either, provide further evidence that there is no important fatigue effect.
As previously shown in a pilot study with healthy young subjects, the adaptive sampling procedure PEST allows reducing the assessment time considerably compared to the widely used, but inefficient, method of constant stimuli,Citation36 resulting in an average assessment duration of ~15 min. Truncating PEST sequences to a maximum of 60 trials resulted in an average assessment duration of 11 min and only in minor changes of the mixed-effects model, demonstrating robustness of the assessment. This is crucial because shortening the assessment duration can significantly increase the assessment’s clinical utility, especially for patient groups, where assessment time is expensive, and where time constraints are perceived as a barrier.Citation59 Furthermore, reliability and validity of an assessment could benefit from short assessments, as the influence of confounding factors such as inattention and other cognitive factors would be decreased.Citation60
Advantages and limitations of the assessment paradigm
This paradigm assesses proprioception in an isolated way, in contrast to assessments using ipsilateral and contralateral matching tasks, which most often require the subject to move actively to reproduce a presented position. Thus, this assessment can be used to investigate somatosensory deficits independently of motor deficits. This allows investigating their contribution to functional impairments and effect on recovery after neurological injuries, such as stroke.
Besides potential confounding factors such as learning and fatigue, the 2AFC method could also be affected by short-term memory. Previous studies have shown that absolute errors in position matching tasks are significantly influenced by several factors such as the type of position matching task or reference position establishment (eg, reference joint angle and how the limb was displaced to present this angle).Citation61 A study with 10 healthy subjects demonstrated better proprioceptive performance in an ipsilateral matching task requiring short-term memory than in a contralateral (simultaneous) matching task requiring interhemispheric transfer, which in turn is better than in a contralateral remembered task requiring both, memory and interhemispheric transfer.Citation61 Similar results have been presented in another study for these three task types revealing mostly disproportionate increases in matching errors for the contralateral remembered task.Citation15 A parallel can be drawn to the assessments of difference thresholds using either two intervals (as was the case here) requiring short-term memory (the two stimuli have to be remembered and compared postpresentation) or two locations stimulated simultaneously (eg, on both index fingers) requiring interhemispheric transfer for comparison, inducing temporal or spatial errors, respectively. Hence, this suggests that the paradigm used in this study (two-interval 2AFC) should be less affected by factors besides healthy aging of proprioception and also be less error prone, as no interhemispheric transfer is required. Furthermore, many limb matching tests rely on the sensorimotor function of the ipsilesional “unimpaired” limb of the patient, which may also be affected by a cerebral lesion,Citation8,Citation62 and their outcomes might also be influenced by deficits in the central integration of proprioceptive information across the two limbs. These confounds are also fully addressed by the two-interval 2AFC approach. Moreover, compared to other psychophysical paradigms such as Yes–No, Remainder, and Same–Different, the 2AFC approach is more robust against decision criteria (ie, response bias), and thus more objective.Citation44,Citation63
Although in each trial of the 2AFC assessment paradigm movements with different amplitudes are presented, there is a trade-off between constant movement duration versus constant movement velocity. Thus, subjects could rely on one of these potential confounds besides the presented joint position angle. There have been approaches where a subthreshold movement velocity was used to resolve this trade-off.Citation20 However, this approach is only usable in research, as it leads to an increased trial duration resulting in overly long assessments, thus limiting their clinical applicability. For our assessment, a constant duration with varying velocity was chosen because perception of movement velocity (ie, kinesthesia) is a subpart of proprioception, and both position and velocity information is suggested to be incorporated within internal models.Citation64 In contrast, discriminating time intervals, apart from detection of movement onset and cessation following discharge of muscle spindles,Citation65 is not strictly part of the proprioceptive sense.
Conclusion
The results of this study demonstrate that taking age into account when creating a model of healthy performance of proprioception as a reference for neurological patients suffering from proprioceptive deficits is essential. All the more, as in some neurological injuries, such as stroke, the ipsilesional “unimpaired” limb of the patient can also be potentially affectedCitation8,Citation62 and should thus not be used as a reference to quantify the performance of the impaired limb.Citation66 Furthermore, this study supports the clinical utility of the objective and automated assessment approach using a robotic tool for quantifying the angular DL at the MCP joint through its sensitivity and rapid administration. This highlights its potential as an assessment tool to be used in combination with age-based reference models for an informed diagnosis, prognosis, and planning of clinical interventions.
Acknowledgments
The authors thank J-C Metzger and WL Popp for their valuable suggestions and thoughtful discussions, as well as the statistical consulting service at ETH Zurich for their advice. This research was supported by the National Center of Competence in Research on Neural Plasticity and Repair of the Swiss National Science Foundation, the Janggen-Pöhn Foundation, ETH Zurich and the Stiftung Schmieder für Wissenschaft und Forschung.
Disclosure
The authors report no conflicts of interest in this work.
References
- GilmanSJoint position sense and vibration sense: anatomical organisation and assessmentJ Neurol Neurosurg Psychiatry200273547347712397137
- GandeviaSCMcCloskeyDIJoint sense, muscle sense, and their combination as position sense, measured at the distal interphalangeal joint of the middle fingerJ Physiol19762602387407978533
- GardnerEMartinJThe bodily sensesKandelERJTPrinciples of Neural ScienceNew YorkMcGraw-Hill2000430450
- McPheeSDFunctional hand evaluations: a reviewAm J Occup Ther19874131581633318477
- OvervlietKESmeetsJBBrennerEThe use of proprioception and tactile information in haptic searchActa Psychol (Amst)20081291839018561891
- GentilucciMToniIChieffiSPavesiGThe role of proprioception in the control of prehension movements: a kinematic study in a peripherally deafferented patient and in normal subjectsExp Brain Res19949934835007957728
- ConnellLALincolnNBRadfordKASomatosensory impairment after stroke: frequency of different deficits and their recoveryClin Rehabil200822875876718678576
- CareyLMMatyasTAFrequency of discriminative sensory loss in the hand after stroke in a rehabilitation settingJ Rehabil Med201143325726321305243
- RedingMJPotesERehabilitation outcome following initial unilateral hemispheric stroke. Life table analysis approachStroke19881911135413583188120
- BoisgontierMPOlivierIChenuONougierVPresbypropria: the effects of physiological ageing on proprioceptive controlAge (Dordr)20123451179119421850402
- GobleDJCoxonJPWenderothNVan ImpeASwinnenSPProprioceptive sensibility in the elderly: degeneration, functional consequences and plastic-adaptive processesNeurosci Biobehav Rev200933327127818793668
- HerterTMScottSHDukelowSPSystematic changes in position sense accompany normal aging across adulthoodJ Neuroeng Rehabil2014114324666888
- StelmachGSiricaAAging and proprioceptionAGE19869499103
- Fry-WelchDCampbellJFoltzBMacekRAge-related changes in upper extremity kinesthesisPhys Occup Ther Geriatr2003203–4137154
- AdamoDEMartinBJBrownSHAge-related differences in upper limb proprioceptive acuityPercept Mot Skills20071043 Pt 21297130917879664
- SchmidtLDepperLKerkhoffGEffects of age, sex and arm on the precision of arm position sense-left-arm superiority in healthy right-handersFront Hum Neurosci2013791524399962
- AdamoDEAlexanderNBBrownSHThe influence of age and physical activity on upper limb proprioceptive abilityJ Aging Phys Act200917327229319799100
- WrightMLAdamoDEBrownSHAge-related declines in the detection of passive wrist movementNeurosci Lett2011500210811221704124
- KokmenEBossemeyerRWilliamsWJQuantitative evaluation of joint motion sensation in an aging populationJ Gerontol19783316267618968
- FerrellWRCrightonASturrockRDAge-dependent changes in position sense in human proximal interphalangeal jointsNeuroreport1992332592611515581
- KalischTKattenstrothJCKowalewskiRTegenthoffMDinseHRAge-related changes in the joint position sense of the human handClin Interv Aging2012749950723226011
- IngemansonMLRoweJBChanVWolbrechtETCramerSCReinkensmeyerDJUse of a robotic device to measure age-related decline in finger proprioceptionExp Brain Res20152341839326378004
- FeiginVLLawesCMBennettDAAndersonCSStroke epidemiology: a review of population-based studies of incidence, prevalence, and case-fatality in the late 20th centuryLancet Neurol200321435312849300
- EpsteinOPerkinGDCooksonJClinical ExaminationLondonElsevier Health Sciences2008
- BeckmannYYÇiftçiYErtekinCThe detection of sensitivity of proprioception by a new clinical test: the dual joint position testClin Neurol Neurosurg201311571023102723206894
- LincolnNBCrowJLJacksonJMWatersGRAdamsSAHodgsonPThe unreliability of sensory assessmentsClin Rehabil199154273282
- CareyLMOkeLEMatyasTAImpaired limb position sense after stroke: a quantitative test for clinical useArch Phys Med Rehabil19967712127112788976311
- WycherleyASHelliwellPSBirdHAA novel device for the measurement of proprioception in the handRheumatology (Oxford)200544563864115728416
- ScottSHDukelowSPPotential of robots as next-generation technology for clinical assessment of neurological disorders and upper-limb therapyJ Rehabil Res Dev201148433535321674387
- DukelowSPHerterTMMooreKDQuantitative assessment of limb position sense following strokeNeurorehabil Neural Repair201024217818719794134
- SqueriVZenzeriJMorassoPBasterisAIntegrating proprioceptive assessment with proprioceptive training of stroke patientsRehabilitation Robotics (ICORR), 2011 IEEE International Conference on (Zurich, Switzerland)162011
- LambercyOJuárez RoblesAKimYGassertRDesign of a robotic device for assessment and rehabilitation of hand sensory functionRehabilitation Robotics (ICORR), 2011 IEEE International Conference on (Zurich, Switzerland)162011
- DukelowSPHerterTMBaggSDScottSHThe independence of deficits in position sense and visually guided reaching following strokeJ Neuroeng Rehabil201297223035968
- SemrauJAHerterTMScottSHDukelowSPRobotic identification of kinesthetic deficits after strokeStroke201344123414342124193800
- SimoLBotzerLGhezCScheidtRAA robotic test of proprioception within the hemiparetic arm post-strokeJ Neuroeng Rehabil2014117724885197
- RinderknechtMDPoppWLLambercyOGassertRExperimental Validation of a Rapid, Adaptive Robotic Assessment of the MCP Joint Angle Difference ThresholdAuvrayMDuriezCHaptics: Neuroscience, Devices, Modeling, and Applications Lecture Notes in Computer ScienceBerlinHeidelberg Springer2014310
- CappelloLElangovanNContuSKhosravaniSKolchakJMaisaLRobot-aided assessment of wrist proprioceptionFront Hum Neurosci2015919825926785
- RinderknechtMDPoppWLLambercyOGassertRReliable and rapid robotic assessment of wrist proprioception using a gauge position matching paradigmFront Hum Neurosci20161031627445756
- ElliottJMConnollyKJA classification of manipulative hand movementsDev Med Child Neurol19842632832966734945
- FelixTRomeroJSchiedamHBDollarAMKragicDThe GRASP taxonomy of human grasp typesIEEE Trans Hum-Mach Syst20164616677
- KamakuraNMatsuoMIshiiHMitsuboshiFMiuraYPatterns of static prehension in normal handsAm J Occup Ther19803474374456446851
- SantelloMFlandersMSoechtingJFPostural hand synergies for tool useJ Neurosci1998182310105101159822764
- TaylorMMDouglas CreelmanCPEST: efficient estimates on probability functionsJ Acoust Soc Am1967414782
- MacmillanNADouglas CreelmanCDetection theory: a User’s GuideNew JerseyLawrence Erlbaum Associates2005
- OldfieldRCThe assessment and analysis of handedness: the Edinburgh inventoryNeuropsychologia197191971135146491
- PrinsNKingdomFAAPalamedes: Matlab routines for analyzing psychophysical data (version 1.8.2)2009
- WichmannFAHillNJThe psychometric function: I. Fitting, sampling, and goodness of fitPercept Psychophys20016381293131311800458
- HallJLHybrid adaptive procedure for estimation of psychometric functionsJ Acoust Soc Am1981696176317697240589
- GobleDJCoxonJPVan ImpeAThe neural basis of central proprioceptive processing in older versus younger adults: an important sensory role for right putamenHum Brain Mapp201233489590821432946
- BoisgontierMPSwinnenSPAge-related deficit in a bimanual joint position matching task is amplitude dependentFront Aging Neurosci2015716226347649
- GobleDJLewisCABrownSHUpper limb asymmetries in the utilization of proprioceptive feedbackExp Brain Res20061681–230731116311728
- GobleDJBrownSHThe biological and behavioral basis of upper limb asymmetries in sensorimotor performanceNeurosci Biobehav Rev200832359861018160103
- GobleDJBrownSHUpper limb asymmetries in the matching of proprioceptive versus visual targetsJ Neurophysiol20089963063307418436632
- GobleDJBrownSHDynamic proprioceptive target matching behavior in the upper limb: effects of speed, task difficulty and arm/hemisphere asymmetriesBehav Brain Res2009200171419073219
- GobleDJNobleBCBrownSHProprioceptive target matching asymmetries in left-handed individualsExp Brain Res2009197440340819572124
- AdamoDEMartinBJPosition sense asymmetryExp Brain Res20091921879518807022
- TeixeiraLACategories of manual asymmetry and their variation with advancing ageCortex200844670771618472040
- DjupsjöbackaMDomkinDCorrelation analysis of proprioceptive acuity in ipsilateral position-matching and velocity-discriminationSomatosens Mot Res2005221–2859316191761
- PumpaLUCahillLSCareyLMSomatosensory assessment and treatment after stroke: an evidence-practice gapAust Occup Ther J20156229310425615889
- GobleDJMousigianMABrownSHCompromised encoding of proprioceptively determined joint angles in older adults: the role of working memory and attentional loadExp Brain Res20122161354022006273
- GobleDJProprioceptive acuity assessment via joint position matching: from basic science to general practicePhys Ther20109081176118420522675
- SchaeferSYHaalandKYSainburgRLIpsilesional motor deficits following stroke reflect hemispheric specializations for movement controlBrain2007130Pt 82146215817626039
- GescheiderGPsychophysics: Method, Theory, and ApplicationsNew JerseyLawrence Erlbaum Associates1985
- KerrGKWorringhamCJVelocity perception and proprioceptionAdv Exp Med Biol2002508798612171154
- GrillSEHallettMVelocity sensitivity of human muscle spindle afferents and slowly adapting type II cutaneous mechanoreceptorsJ Physiol1995489Pt 25938847650
- DannenbaumRMJonesLAThe assessment and treatment of patients who have sensory loss following cortical lesionsJ Hand Ther1993621301388343879