
Abstract
Purpose
This study aimed to investigate the effects of resistance exercise (RE) on autonomic control and blood pressure (BP) reactivity during mental stress (MS) in treated older hypertensive women.
Methods
Ten older hypertensive women (age =71.1±5.5 years; body mass index =24.2±3.9; mean BP [MBP] =85.4±3.5) underwent a protocol consisting of BP and heart rate variability (HRV) output assessments at baseline and during MS, and these measurements were taken before and 60 minutes after two bouts of RE (traditional and circuit). MS was induced through a computerized 3-minute Stroop color–word test before and 1 hour after each exercise session; BP was measured every minute during MS, and HRV was monitored as a measure of cardiac autonomic control.
Results
A significant effect of time on systolic BP (Δpre =17.4±12.8 versus Δpost =12.5±9.6; P=0.01), diastolic BP (Δpre =13.7±7.1 versus Δpost =8.8±4.5; P=0.01), and MBP (Δpre =14.0±7.7 versus Δpost =9.3±5.4; P<0.01) after RE was observed, with no differences between the two sessions. In addition, a significant effect of time on log-normalized low-frequency component of HRV (ms2; 5.3±0.8 pre-exercise MS versus 4.8±1.0 baseline value; P=0.023) was also observed, showing a significant change from baseline to MS before RE, but not after RE sessions. These results may be related to a lessened RE-mediated cardiac sympathetic activity during MS.
Conclusion
RE is an effective tool to reduce BP reactivity to MS, which could therefore be associated with an acute reduction in cardiovascular risk. This result presents relevant clinical implications, combining previous evidence that recommends this exercise modality as an important component of an exercise program designed for the older and hypertensive subjects.
Introduction
Hypertension (HTN) is a growing health problem that plays an important role in the development of cardiovascular disease.Citation1 The prevalence of HTN increases with increasing age; currently, more than half of older individuals are affected.Citation2 Moreover, although blood pressure (BP) is typically lower in women, postmenopausal women have a higher prevalence of HTN when compared with age-matched men.Citation3 The management of HTN in older individuals is clearly relevant given that its prevalence and related complications are expected to increase with aging population, especially in older women. Various lifestyle modifications have been demonstrated to positively influence BP and thus is thought to be the first-line treatment.Citation1 In particular, physical exercise is an effective treatment strategy for individuals with HTN.Citation4
Hypertensive patients, as well as the general population, are exposed to mental and psychological stress in day-to-day life, imposing an increased load on the cardiovascular system.Citation5 Specifically, BP rise to a given stress stimulus in relation to baseline values has been referred to as BP reactivity. An augmented BP response to mental stress (MS) has been reported to be associated with future HTN developmentCitation6 and to predict carotid atherosclerosis in women.Citation7 Moreover, during MS, individuals with HTN have higher BP values when compared with their age-matched normotensive counterpartsCitation8,Citation9 and have impaired endothelial-dependent vasodilation.Citation10 These findings indicate that hypertensive subjects are at an increased risk of cardiovascular events and have greater susceptibility to vascular damage when exposed to frequent stressful situations.
Importantly, several reports have shown that the BP response to MS is attenuated after a single session of aerobic exerciseCitation11–Citation13 (the rhythmical contraction and relaxation of large muscle groups over a prolonged time) in healthy subjects. Furthermore, these findings have been extended to individuals with metabolic syndromeCitation14 and to patients with HTN,Citation15,Citation16 which has important clinical implications. In addition, it has been demonstrated that exercise promotes a reduction in vascular reactivity among individuals with a family history of HTN.Citation17 Few studies have been conducted to elucidate mechanisms associated with the acute reduction in BP reactivity after exercise. In this regard, Brownley et alCitation12 suggested that reduced BP reactivity to MS after an aerobic exercise session is associated with a decrease in sympathetic drive, whereas Ebbesen et alCitation18 observed the maintenance of catecholamine levels in response to MS. The mechanisms underlying attenuated BP responses to MS following a single bout of exercise require further exploration.
In fact, most physical activity guidelines for hypertensive individuals traditionally recommend aerobic activities such as cycling, walking, and jogging.Citation4 However, in addition to the well-documented positive effects of resistance training on muscle mass, strength, and function, more recent studies support many benefits of this training modality on cardiovascular health, such as positive changes in cardiovascular system structure and function and reduction in resting BP.Citation19 In addition, a single session of resistance exercise (RE) may be effective in reducing BP levels below resting levels.Citation20 Thus, RE has been used as an important component of physical activity programs for BP control.Citation4 However, little is known regarding the effect of a single bout of RE on BP reactivity to MS. In studies on RE among hypertensive subjects, exercise sessions are typically implemented using either a traditional (TR) multiple-set or a circuit-based (CI) regimen.Citation21,Citation22 Thus, in addition to examining the effects of RE on BP reactivity to MS, it would be informative to compare both the TR and CI approaches. Therefore, the aim of the present study was to investigate the acute effects of TR and CI RE sessions on BP reactivity to MS in treated older hypertensive women. Autonomic control was also examined in an effort to elucidate potential mechanisms. Based on the literature,Citation23 the hypothesis that both these RE arrangements would acutely attenuate BP reactivity to MS and thus provide additional support for exercise recommendation was raised.
Methods
Study design
In order to examine the acute effects of different RE modes on BP reactivity and autonomic modulation in older hypertensive women, each volunteer underwent six visits to the laboratory. During the first visit, the subjects completed face-to-face questionnaires addressing their medical history and lifestyle habits. Resting BP was measured by using an oscillometric device (Microlife BP 3AC1-1; Microlife USA Inc., Dunedin, FL, USA) at least two times, after 5 minutes of seated rest and with an interval of 5 minutes between readings. If a difference >5 mmHg was noted between readings, a third measurement was taken with the mean value considered for subsequent analyses. Then, the subjects proceeded to anthropometric measures and familiarization to RE sessions. During the second laboratory visit, resting BP measurements were repeated, and the subjects were further familiarized to the RE sessions. Load determinations were conducted and adjusted up to fourth laboratory visit. Visits 5 and 6 consisted of the TR or CI RE sessions, which were performed in a randomized order. BP and heart rate variability (HRV) responses to MS were evaluated before and after 60 minutes of the RE sessions. illustrates the schematic overview from the experimental sessions.
Figure 1 Schematic diagram of the experimental sessions.
Subjects
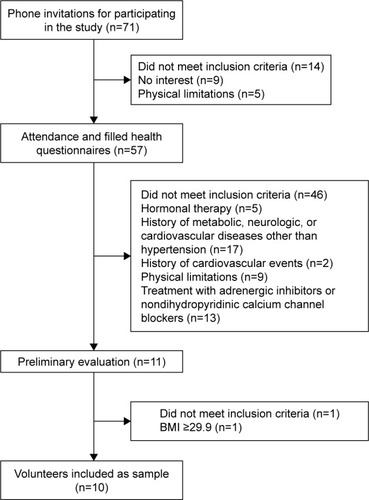
Volunteers were older hypertensive women recruited through flyers, banners, phone calls, and visits to centers of leisure for older adults, hospitals, and churches. In total, 71 subjects were eligible to participate in the present study. The exclusion criteria were as follows: subjects taking hormonal therapy; those with a history of metabolic, neurologic, or cardiovascular diseases other than HTN; those with a history of cardiovascular events; subjects with physical limitations; those with nontreated HTN (ie, systolic BP [SBP] and diastolic BP [DBP] <140/90 mmHg, respectively); subjects with obesity (body mass index ≥30.0); and subjects taking adrenergic inhibitors or nondihydropyridinic calcium channel blockers. After exclusion ten subjects (age =71±5.5 years; height =1.5±0.1 m; weight =56.1±9.8 kg) participated in this study (six subjects were taking dihydropyridinic calcium channel blockers, six subjects were taking diuretics, and seven subjects were taking angiotensin II receptor blockers). Experimental procedures were in line with the Declaration of Helsinki principles and were approved by the Institutional Review Board at the University of Brasília. All the participants signed an informed consent containing the objectives and procedures as well as possible risks and benefits related to the study. presents the subject characteristics, and presents a volunteer recruitment flowchart.
Table 1 Subject characteristics
Figure 2 Flowchart of sample recruitment and selection.
RE load assessment and familiarization
Exercise loads were assessed over seven REs (ie, seated leg press, seated row, leg extension, seated chest press, leg curl, shoulder abduction, and seated calf raises) by using the perceived effort Omnibus Resistance Exercise Scale (OMNI-RES), according to the procedures described elsewhere.Citation24 The rationale of this approach to set the appropriate load used in exercises is that it is an easy, effective, and time-saving procedure supported by a previous research on RE for older adults.Citation25–Citation27 In addition, it also has a practical application for professionals prescribing RE for older adults, as this may be used instead of one repetition maximum or other strength tests.Citation25
Except for shoulder abduction that was implemented using dumbbells, all REs were conducted using machines (Rotech Fitness Equipment, Goiania, Brazil). The subjects performed one repetition on each exercise and rated on the scale whether the perceived load was “somewhat easy.” If so, the volunteers proceeded to the next exercise; otherwise, the load was adjusted and another repetition was performed after 1 minute of rest, repeating this procedure until the subjects rated the perceived effort as “somewhat easy” for one repetition. It has been demonstrated that one repetition rated “somewhat easy” in OMNI-RES is ~60% of one maximum repetition.Citation28 This load was selected in order to follow RE recommendations for older and hypertensive individualsCitation4,Citation19 and thereby induce positive neuromuscular and cardiovascular adaptations.Citation19 A print copy of the OMNI-RES was fixed on each exercise machine and was visible to the subjects all the time. As anchoring procedures, the subjects were instructed to create a cognitive visual link using the scale and their memory of muscular efforts.Citation25 The load values of the RE machines were covered in order to avoid their influence on the perception of subjects.
After exercise load assessment, the volunteers were familiarized to TR or CI RE sessions. They performed one set of 12 repetitions at 50% of the estimated exercise load at Session 1; two sets of 12 repetitions at 60% of the estimated exercise load at Session 2; two sets of 12 repetitions at 70% of the estimated exercise load at Session 3; and three sets of 12 repetitions at 80% of the estimated exercise load at Session 4. Familiarization TR and CI sessions were separated by 48–72 hours and were performed in a randomized order determined by a statistical software (Decision Analyst STATS™ 2.0, Arlington, VA, USA).
It was previously demonstrated that memory anchoring was equal to exercise anchoring alone or exercise–memory anchoring on reliability ratings of perceived exertion after RE.Citation25 Moreover, OMNI-RES applicability was demonstrated in previous studies on older individuals (concurrent and construct validity values in comparison with Borg Scale ranging from 0.79 to 0.91 and 0.94 to 0.97, respectively),Citation26 was recently validated to CI RE arrangement (significant correlation with blood lactate; r=0.56), and has been shown to be an adequate instrument to manipulate and quantify effort intensity on RE in older women.Citation27,Citation29
RE sessions
In the TR session, the volunteers performed three sets of 12 repetitions for each of the aforementioned exercises, with 1-minute intervals between the sets and exercises. The CI session was performed in 3 laps, consisting of the same exercises, with one set being conducted for each lap, 30-second intervals between exercises and 1 minute between laps. Exercise order and loads were identical for both the arrangements. Immediately after each session, 200 mL of water was given to the subjects. Thirty minutes after completing the RE sessions, the subjects were presented with an adapted scale of perceived exertion used to quantitate the intensity of RE sessions, following the procedures described elsewhere.Citation30 The volunteers were instructed to avoid alcohol and caffeine and not to perform vigorous physical activity during the 24 hours before the experimental sessions. They were also asked to have a light meal 2 hours before each RE session and to maintain their habitual antihypertensive medication routine.
The REs were performed in the following order: seated leg press, seated row, leg extension, chest press, leg curl, shoulder abduction, and seated calf raises. Both the TR and CI sessions were performed in a randomized order at the same time of the morning (between 8 and 11 am) and were separated by 48–72 hours.
MS
MS tasks were induced by using a computerized version of the Stroop color–word test and was administrated individually to each participant over a 3-minute period.Citation31 Briefly, the study procedure included a slide presentation on a monitor placed in front of the participants. Each slide lasted ~1 second with the names of colors (ie, “blue,” “yellow,” and “red”) being displayed in different colors from that denoted by the name. The volunteers were instructed to report the color of the letters of the word, as fast as possible, and not the written word. Continuous auditory conflict (a taped voice saying different color names in a headphone) was provided during the test to ensure stress induction, and the recordings were obtained in a temperature-controlled, noise-free room.
The BP was measured by using a mercury-column sphygmomanometer immediately before and at the end of each minute during the test. All of the BP measures were taken by a single trained professional. Within-subjects coefficient of variation for the used device was 6.0% and 5.7% for SBP and DBP, respectively. The standard auscultatory method was tested against the automated and previously validated oscillometric method (Microlife BP 3AC1-1). Another sample of 30 independent individuals of both genders rested for 10 minutes, and their BPs were randomly measured by using both the auscultatory and oscillometric methods, the latter conducted by another blinded evaluator. Correlations between the methods were r=0.90 (P<0.001) for SBP and r=0.92 (P<0.001) for DBP. Furthermore, agreement between these methods was evaluated by using the Bland–Altman method. Mean differences were 3.9 mmHg (20.2–12.4 mmHg) and -3.4 mmHg (10.5–17.3 mmHg) for SBP and DBP, respectively.
Immediately after the slide presentation, the individuals were asked to report their perceived stress using the following scores: 0= not stressful; 1= slightly stressful; 2= stressful; 3= very stressful; and 4= extremely stressful.Citation11
HRV
HRV was used to assess autonomic control and was measured by using a cardiac monitor (RS800CX model; Polar Electro Oy, Kempele, Finland), according to the specifications published previously.Citation32 Briefly, the subjects wore a heart rate sensor attached to a strap and remained resting in the seated position for 10 minutes with spontaneous breathing prior to pre- and postexercise stress induction. A 5-minute reading was taken before exercise, with the last 3 minutes used for subsequent analyses. HRV was measured during MS both before and after RE sessions. Linear frequency-and time-domain analyses, as well as nonlinear measures of sample entropy (SampEn) were performed by using Kubios HRV 2.2 software (Biosignal Analysis and Medical Imaging Group, Joensuu, Finland). Time-domain HRV was expressed as the square root of the mean-squared differences of successive R-R intervals (RMSSD), whereas frequency-domain HRV was assessed by using autoregressive spectral analysis (model order =16), with HRV decomposed in a low-frequency (LF) band (0.04–0.15 Hz) and a high-frequency (HF) band (0.15–0.4 Hz). The LF/HF ratio of HRV was used as an indicator of sympathovagal balance. Spectral power bands are presented in both absolute (msCitation2) and normalized units (nu).
Statistical analyses
Reliability of loads determined with OMNI-RES was measured by intraclass correlation coefficient (Cronbach’s α, 95% confidence interval [CI]). Baseline hemodynamic and autonomic variables prior to RE sessions were compared using repeated measures analysis of variance (ANOVA) with a 2 (session: TR, CI) ×2 (time: pre-RE, post-RE) design for BP response to MS and a 2 (session: TR, CI) ×3 (time: baseline, during MS pre-RE, during MS post-RE) design for HRV. In addition, the repeated measures ANOVA was performed also to verify BP responses to MS before exercise (2 [session: TR, CI] ×2 [BP immediately before MS, BP peak during MS]) and individual perceived stress before and after exercise (2 [session: TR, CI] ×2 [time: pre-RE, post-RE]). All the data were presented as mean ± standard deviation (SD), otherwise noted. Statistical analyses were performed by using Statistical Package for the Social Sciences (version 20.0), with a significance level at P<0.05.
Results
Intraclass correlation coefficients (Cronbach’s α, 95% CI) for loads determined by OMNI-RES demonstrated r values of 0.92 (seated leg press), 0.93 (seated row), 0.98 (leg extension), 0.97 (chest press), 0.87 (leg curl), 0.93 (shoulder abduction), and 0.98 (plantar flexion). No differences in hemodynamic or autonomic variables were observed between RE sessions at baseline or 60 minutes after exercise ().
Table 2 Pre- and postexercise hemodynamic and autonomic variables in experimental session days (mean ± SD)
Perceived stress induced by Stroop color–word test did not differ within or between experimental sessions at any time (1.7±0.9 and 1.9±0.9 pre- and post-TR sessions, respectively; and 1.8±0.8 and 1.7±0.8 pre- and post-CI sessions, respectively; session: P=0.726; time: P=0.726; interaction: P=0.081). Repeated measures ANOVA showed a significant raise in SBP, DBP, and mean BP (MBP; all P<0.01) during MS before both the RE sessions, showing that the Stroop color–word test as an appropriate stressful tool, with no differences between the sessions.
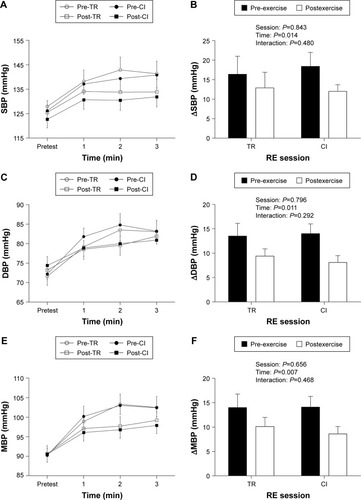
presents BP responses immediately before and at each minute of MS (Panels A, C, and E) as well as peak stress-induced BP increases (Panels B, D, and F) both pre- and post-RE sessions. A significant effect of time on SBP (17.4±12.8 Δpre versus 12.5±9.6 Δpost; P=0.01), DBP (13.7±7.1 Δpre versus 8.8±4.5 Δpost; P=0.01), and MBP (14.0±7.7 Δpre versus 9.3±5.4 Δpost; P<0.01) was observed. However, no significant interaction was observed, indicating that the RE approaches equally attenuated BP responses to MS. It was noted that BP readings immediately before the Stroop task did not differ when comparing pre- and post-RE conditions combined, nor between the experimental sessions (ie, TR versus CI).
Figure 3 Time course for SBP, DBP, and MBP responses and their changes (SBP, Panels A and B; DBP, Panels C and D; and MBP, Panels E and F) during MS before and 60 min after TR and CI RE sessions.
Abbreviations: CI, circuit-based; DBP, diastolic blood pressure; MBP, mean blood pressure; MS, mental stress; RE, resistance exercise; SBP, systolic blood pressure; SD, standard deviation; TR, traditional.
A significant effect of time on LF (nu; 76.8±15.0 pre-exercise MS versus 61.4±19.7 baseline value; P=0.032; and 79.1±9.5 postexercise MS versus 61.4±19.7 baseline value; P=0.011), HF (nu; 22.9±15.1 pre-exercise MS versus 38.5±19.7 baseline value; P=0.032; and 20.8±9.4 postexercise MS versus 38.5±19.7 baseline value; P=0.011), LF/HF ratio (1.4±0.2 pre-exercise MS versus 1.1±0.3 baseline value; P=0.025; and 1.4±0.2 postexercise MS versus 1.1±0.3 baseline value; P=0.010), and SampEn (1.28±0.20 pre-exercise MS versus 1.58±0.21 baseline value; P=0.015; and 1.19±0.23 postexercise MS versus 1.58±0.21 baseline value; P=0.004) was observed, showing significant changes from baseline to MS pre-RE and also from baseline to MS post-RE (). Interestingly, a significant effect of time on log-normalized low-frequency (ln LF; msCitation2; 5.3±0.8 pre-exercise MS versus 4.8±1.0 baseline value; P=0.023) was also observed, showing a significant change only from baseline to MS pre-RE, but not from baseline to MS post-RE sessions. The comparison of ln LF (msCitation2) postexercise with baseline values did not show significant differences. A time effect was absent for ln HF (msCitation2) and RMSSD. Session and interaction effects were not observed for any of the HRV variables.
Table 3 Mean ± SD of HRV components at baseline and during MS by Stroop task performed pre- and post-TR RE session and pre-and post-CI RE session
Discussion
The acute effects of aerobic exercise on BP reactivity to MS have been extensively studied.Citation13 However, although RE has been recommended for older hypertensive individuals, it is unknown whether this mode of exercise can provide similar benefits on the response to MS. The responses of different RE methods to BP reactivity would also be of interest, as TR and CI methods have been commonly used in RE studies for hypertensive individuals.Citation21,Citation22 The main findings of the present study provide the novel insight that both TR and CI RE sessions attenuate BP reactivity to MS in older hypertensive women, with no different effects between the sessions. These observations were followed by a reduction in sympathetic neural activity as evaluated by using HRV during MS, which might in part explain the attenuated BP response. These results have potential relevant clinical significance and extend previous evidence that recommends RE as an important component of physical activity programs designed for older hypertensive subjects.Citation19
The results from the present study corroborate previous studies that demonstrated that a single session of aerobic exercise attenuates BP responses to MS.Citation11,Citation12 It was observed that reductions in BP reactivity were similar to those reported in a meta-analysis by Hamer et al.Citation13 These authors reported mean reductions of 3.0 and 3.9 mmHg for SBP and DBP, respectively, following aerobic exercise sessions. The present results similarly indicated reductions of 3.5 (SBP) and 4.0 mmHg (DBP) following TR RE sessions and 6.4 (SBP) and 5.9 mmHg (DBP) after CI RE sessions, but with no significant differences between them. To the authors’ knowledge, only one study by Moreira et alCitation23 that included RE as part of a concurrent session designed in a CI manner reported an attenuated BP response to a cold pressor test following exercise; however, the BP rise in vascular tests in response to cold pressor testing occurred by different mechanisms from that elicited by Stroop color–word test, and these results may not occur if other stressors were employed. The present observations expand previous findings and suggest that RE per se could diminish the BP response to MS in older hypertensive women.
No differences in postexercise BP responses were observed between TR and CI even though these two approaches had equivalent loads and volume. In addition, the ratings of perceived exertion did not differ between the two approaches to RE (3.7±1.1 for TR and 3.4±1.2 for CI; P=0.193). CI RE has become a popular method for older adults and has been suggested to be advantageous, given its dynamic and time-saving nature. In fact, the CI session was accomplished in approximately two-thirds of the time required for the TR session (29.9±0.8 minutes for TR and 20.2±0.8 minutes for CI). Therefore, it can be argued that the CI approach is an equally effective and more efficient RE method for older hypertensive women as it promotes similar attenuation in BP reactivity when compared with TR, but it is completed in a shorter duration. In addition to the potential advantages when considering adherence, faster completion of CI might help to facilitate other modes such as aerobic and flexibility exercises in a typical exercise session.
In the present study, attenuation in BP reactivity might partially be explained by an acute RE-induced lessening in sympathetic activity during MS. This was supported by an absence of response from LF spectral band (msCitation2) during MS post-RE relative to baseline, while a significant rise in this frequency band was evident during MS before exercise. The results from the present study were in agreement with the observations of Brownley et al,Citation12 who showed that diminished sympathetic reactivity (reductions in norepinephrine and a rise in pre-ejection period) was responsible for up to 64% of the attenuation found in MBP during MS after a bout of aerobic exercise. However, previous reports regarding catecholamine levels and BP reactivity after dynamic exercise are controversial. Péronnet et alCitation33 reported a reduction in epinephrine levels after exercise during an MS test that was not accompanied by reductions in BP reactivity; Ebbesen et alCitation18 found the opposite results, showing a reduction in BP reactivity to MS and a maintenance of circulating catecholamines.
It is possible that the attenuated BP response observed during MS post-RE could also be mediated, in part, by a vasodilator response. This is supported by the findings of West et al,Citation16 who demonstrated a reduction in peripheral vascular resistance following a bout of exercise together with a reduction in BP reactivity to stress. In addition, the results of Brownley et alCitation12 corroborate this hypothesis. They reported a significant rise in β-2 adrenergic responsiveness after performing an exercise bout, which is demonstrated by a reduction in isoproterenol vasodilator dose necessary to diminish peripheral vascular resistance by 50%, suggesting that an adrenergic-mediated (β-2) vasodilation is one of the mechanisms responsible for BP attenuation during stress after exercise. Nonetheless, this concept is challenged by previous studies reporting that reductions in stroke volume and cardiac output but not peripheral vascular resistance are responsible for a diminished BP response to MS following exercise.Citation11,Citation34 The present results extend the previous studies supporting cardiovascular benefits of RE.Citation4,Citation19 It was observed that RE may reduce the sympathetic response to stress, limiting individual exposure to high levels of sympathetic activity. It was noted that high levels of sympathetic activity reflected by HRV are associated with a variety of adverse cardiovascular conditions including myocardial infarction, transient myocardial ischemia, congestive heart failure, and mortality.Citation35 In addition, as stated by Hamer et alCitation13 repeated, cumulative bouts of exercise are associated with cardiovascular health benefits, in part through its effect on lowering BP response to MS. This is important given that individuals who exhibit high BP responses to MS may be at a risk of developing diseases such as HTN,Citation6 silent cerebrovascular disease,Citation36 stroke,Citation37 cardiovascular mortality,Citation38 and transient endothelial dysfunction.Citation39
Volunteers enrolled in this investigation were older women who had HTN, two conditions associated with a high cardiovascular risk. Older adults, for example, showed a high SBP reactivity to stress when compared to young.Citation40 As demonstrated by Everson et al,Citation37 each 1 mmHg rise in SBP during a stressful situation corresponded to an 1% rise in stroke risk in an 11-year prospective study. Similarly, Carroll et alCitation38 observed that every 1-SD rise in SBP reactivity during stress was associated with a 3% elevation in cardiovascular mortality among 431 individuals followed up for 16 years. The present results may also have clinical significance for hypertensive individuals, as their conditions already represent an elevated cardiovascular risk that could be minimized by regular REs. Thus, the results of the present study supported guidelines from professional organizations regarding RE for older adultsCitation41 and for the management of HTN.Citation4
Pre-exercise BP levels were not diminished after 60 minutes of exercise in the present study, indicating the absence of postexercise hypotension. Despite evidence regarding the occurrence of post-RE hypotension in olderCitation42,Citation43 and hypertensive individuals,Citation44,Citation45 it is important to consider that the magnitude of BP changes in the postexercise period may directly be associated with higher pre-exercise BP levels,Citation46 which was not the case in the present sample. Moreover, as suggested by West et alCitation16 and observed in previous reports,Citation47,Citation48 anticipation of the upcoming stress test may prevent any significant BP reductions after exercise. The present results showed that even in the absence of postexercise hypotension, performing a single bout of RE may reduce cardiovascular risk by minimizing BP and sympathetic responses to stressful situations.
A lack of information exists concerning the effects of RE on BP response to a MS. The present study reported for the first time that RE can be used as a coping strategy to attenuate BP response to an MS test. Significant reductions in SBP, DBP, and MBP were shown after performing TR and CI sessions of RE, with no difference between the methods. The sessions were prescribed with volume and intensity commonly used in RE programs designed for older subjects (three sets with an intensity corresponding to a “somewhat easy” load on the OMNI-RES, a time-saving, efficient, and safe strategy on load determination). These findings were relevant considering the health risks associated with a hyperreactive BP response,Citation36,Citation37 showing that RE should be performed even in the absence of postexercise hypotension. This is important for hypertensive individuals, who present an elevated cardiovascular risk compared with their normotensive counterparts.Citation1
Limitations
The present study has several limitations. For example, HRV is an indirect measure of autonomic nervous activity that may not be sensitive enough to reflect changes in autonomic modulation during MS.Citation49,Citation50 However, a series of previous studies employed HRV as a measure of cardiac autonomic control during MS,Citation51–Citation53 and the results from the present study suggested a well-characterized response of sympathetic activation during stress. Furthermore, the volunteers were women with well-controlled HTN, and thus, the present observations cannot necessarily be extrapolated to those with uncontrolled HTN and to men. Future studies should be conducted in this regard.
Conclusion
The findings from the present study suggested that both TR and CI RE sessions acutely attenuate BP responses to MS in older hypertensive women, with no differences between the two approaches. These responses may partially be explained by the reduced sympathetic response during MS after exercise. These results have clinical implications in that they reinforce previous evidence that recommends RE as an important component of physical activity programs designed for older hypertensive subjects.
Acknowledgments
The authors thank the study participants. This work was supported by National Council for Scientific and Technological Development (grants 487622/2012-0 and 307630/2013-7) and by University of Brasília. The authors thank the Federal District Research Support Foundation (FAPDF) for funding the publication fee. Preliminary results of this work were published as an abstract in “ISAN 2015: First International Joint Meeting ISAN – AAS – EFAS – JSNR 2015,” held in Stresa, Italy. The abstract is referenced as Autonomic Neuroscience: basic and clinic, 2015. v. 192. p. 111. The text is available online and can be found in http://www.autonomicneuroscience.com/article/S1566-0702(15)00246-5/abstract.
Disclosure
The authors report no conflicts of interest in this work.
References
- AronowWSFlegJLPepineCJACCF/AHA 2011 expert consensus document on hypertension in the elderly: a report of the American College of Cardiology Foundation Task Force on clinical expert consensus documents developed in collaboration with the American Academy of Neurology, American Geriatrics Society, American Society for Preventive Cardiology, American Society of Hypertension, American Society of Nephrology, Association of Black Cardiologists, and European Society of HypertensionJ Am Coll Cardiol201157202037211421524875
- ChobanianAVBakrisGLBlackHRThe Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 reportJAMA2003289192560257112748199
- LimaRWoffordMReckelhoffJFHypertension in postmenopausal womenCurr Hypertens Rep201214325426022427070
- PescatelloLSFranklinBAFagardRAmerican College of Sports Medicine position stand. Exercise and hypertensionMed Sci Sports Exerc200436353355315076798
- PickeringTGMental stress as a causal factor in the development of hypertension and cardiovascular diseaseCurr Hypertens Rep20013324925411353576
- ChidaYSteptoeAGreater cardiovascular responses to laboratory mental stress are associated with poor subsequent cardiovascular risk status a meta-analysis of prospective evidenceHypertension20105541026103220194301
- MatthewsKAOwensJFKullerLHSutton-TyrrellKLassilaHCWolfsonSKStress-induced pulse pressure change predicts women’s carotid atherosclerosisStroke1998298152515309707187
- LindvallKKahanTde FaireUOstergrenJHjemdahlPStress-induced changes in blood pressure and left ventricular function in mild hypertensionClin Cardiol19911421251321646089
- TsaiPSYuchaCBNicholsWWYarandiHHemodynamics and arterial properties in response to mental stress in individuals with mild hypertensionPsychosom Med200365461361912883112
- CardilloCKilcoyneCMCannonROPanzaJAImpairment of the nitric oxide–mediated vasodilator response to mental stress in hypertensive but not in hypercholesterolemic patientsJ Am Coll Cardiol1998325120712139809927
- ViannaLCSilvaBMNóbregaACLSex differences in blood pressure responses to mental stress are abolished after a single bout of exercise: underlying hemodynamic mechanismsJ Physiol Sci201464321321924497232
- BrownleyKAHinderliterALWestSGGirdlerSSSherwoodALightKCSympathoadrenergic mechanisms in reduced hemodynamic stress responses after exerciseMed Sci Sports Exerc200335697898612783046
- HamerMTaylorASteptoeAThe effect of acute aerobic exercise on stress related blood pressure responses: a systematic review and meta-analysisBiol Psychol200671218319015979232
- SalesARFernandesIARochaNGAerobic exercise acutely prevents the endothelial dysfunction induced by mental stress among subjects with metabolic syndrome: the role of shear rateAm J Physiol Heart Circ Physiol20143067H963H97124531810
- BooneJBJrProbstMMRogersMWBergerRPostexercise hypotension reduces cardiovascular responses to stressJ Hypertens19931144494538390514
- WestSGBrownleyKALightKCPostexercise vasodilatation reduces diastolic blood pressure responses to stressAnn Behav Med199820277839989312
- HamerMJonesJBoutcherSHAcute exercise reduces vascular reactivity to mental challenge in offspring of hypertensive familiesJ Hypertens200624231532016508578
- EbbesenBLPrkachinKMMillsDEGreenHJEffects of acute exercise on cardiovascular reactivityJ Behav Med19921554895071447759
- WilliamsMAHaskellWLAdesPAResistance exercise in individuals with and without cardiovascular disease: 2007 update a scientific statement from the american heart association council on clinical cardiology and council on nutrition, physical activity, and metabolismCirculation2007116557258417638929
- TeixeiraLRitti-DiasRMTinucciTJúniorDMForjazCLMPost-concurrent exercise hemodynamics and cardiac autonomic modulationEur J Appl Physiol201111192069207821259026
- HarrisKAHollyRGPhysiological response to circuit weight training in borderline hypertensive subjectsMed Sci Sports Exerc19871932462523600238
- MoraesMRBacurauRFSimoesHGEffect of 12 weeks of resistance exercise on post-exercise hypotension in stage 1 hypertensive individualsJ Hum Hypertens201226953353921734721
- MoreiraSRLimaRMSilvaKESimoesHGCombined exercise circuit session acutely attenuates stress-induced blood pressure reactivity in healthy adultsBraz J Phys Ther2014181384624675911
- RobertsonRJGossFLRutkowskiJConcurrent validation of the OMNI perceived exertion scale for resistance exerciseMed Sci Sports Exerc200335233334112569225
- LagallyKMCostiganEMAnchoring procedures in reliability of ratings of perceived exertion during resistance exercisePercept Mot Skills2004983 Pt 21285129515291217
- GearhartRFJrLagallyKMRiechmanSEAndrewsRDRobertsonRJStrength tracking using the OMNI resistance exercise scale in older men and womenJ Strength Cond Res20092331011101519387373
- FerreiraSSKrinskiKAlvesRCThe use of session RPE to monitor the intensity of weight training in older women: acute responses to eccentric, concentric, and dynamic exercisesJ Aging Res2014201474931724834354
- LagallyKMRobertsonRJConstruct validity of the OMNI resistance exercise scaleJ Strength Cond Res200620225225616686549
- AnicetoRRRitti-DiasRMDos PrazeresTMFarahBQde LimaFFdo PradoWLRating of perceived exertion during circuit weight training: a concurrent validation studyJ Strength Cond Res201529123336334226595128
- SweetTWFosterCMcGuiganMRBriceGQuantitation of resistance training using the session rating of perceived exertion methodJ Strength Cond Res200418479680215574104
- StroopJRStudies of interference in serial verbal reactionsJ Exp Psychol1935186643662
- Task Force of the European Society of Cardiology and the North American Society of Pacing and ElectrophysiologyHeart rate variability. Standards of measurement, physiological interpretation, and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and ElectrophysiologyEur Heart J19961733543818737210
- PéronnetFMassicotteDPaquetJEBrissonGde ChamplainJBlood pressure and plasma catecholamine responses to various challenges during exercise-recovery in manEur J Appl Physiol Occup Physiol19895855515552759082
- NevesFJCarvalhoACRochaNGHemodynamic mechanisms of the attenuated blood pressure response to mental stress after a single bout of maximal dynamic exercise in healthy subjectsBraz J Med Biol Res201245761061622584644
- MontanoNPortaACogliatiCHeart rate variability explored in the frequency domain: a tool to investigate the link between heart and behaviorNeurosci Biobehav Rev2009332718018706440
- WaldsteinSRSiegelELLefkowitzDStress-induced blood pressure reactivity and silent cerebrovascular diseaseStroke20043561294129815087554
- EversonSALynchJWKaplanGALakkaTASiveniusJSalonenJTStress-induced blood pressure reactivity and incident stroke in middle-aged menStroke20013261263127011387485
- CarrollDGintyATDerGHuntKBenzevalMPhillipsACIncreased blood pressure reactions to acute mental stress are associated with 16-year cardiovascular disease mortalityPsychophysiology201249101444144822958235
- GhiadoniLDonaldAECropleyMMental stress induces transient endothelial dysfunction in humansCirculation2000102202473247811076819
- UchinoBNBirminghamWBergCAAre older adults less or more physiologically reactive? A meta-analysis of age-related differences in cardiovascular reactivity to laboratory tasksJ Gerontol B Psychol Sci Soc Sci2010652154162
- American College of Sports MedicineChodzko-ZajkoWJProctorDNAmerican College of Sports Medicine position stand. Exercise and physical activity for older adultsMed Sci Sports Exerc20094171510153019516148
- MotaMRde OliveiraRJDutraMTAcute and chronic effects of resistive exercise on blood pressure in hypertensive elderly womenJ Strength Cond Res201327123475348023478476
- QueirozACKanegusukuHChehuenMRCardiac work remains high after strength exercise in elderlyInt J Sports Med201334539139723175179
- Brito AdeFde OliveiraCVBrasileiro-Santos MdoSSantos AdaCResistance exercise with different volumes: blood pressure response and forearm blood flow in the hypertensive elderlyClin Interv Aging201492151215825540580
- ScherLMFerriolliEMorigutiJCScherRLimaNKThe effect of different volumes of acute resistance exercise on elderly individuals with treated hypertensionJ Strength Cond Res20112541016102320657311
- FisherMMThe effect of resistance exercise on recovery blood pressure in normotensive and borderline hypertensive womenJ Strength Cond Res200115221021611710406
- RejeskiWJGreggEThompsonABerryMThe effects of varying doses of acute aerobic exercise on psychophysiological stress responses in highly trained cyclistsJ Sport Exerc Psychol199113188199
- RejeskiWJThompsonABrubakerPHMillerHSAcute exercise: buffering psychosocial stress responses in womenHealth Psychol19921163553621286654
- SloanRKortenJMyersMMComponents of heart rate reactivity during mental arithmetic with and without speakingPhysiol Behav1991505103910451805266
- SloanRPShapiroPBagiellaEBiggerJLoEGormanJRelationships between circulating catecholamines and low frequency heart period variability as indices of cardiac sympathetic activity during mental stressPsychosom Med199658125318677285
- UchinoBNUnoDHolt-LunstadJFlindersJBAge-related differences in cardiovascular reactivity during acute psychological stress in men and womenJ Gerontol B Psychol Sci Soc Sci1999546P339P34610625961
- LangewitzWRüddelHSchächingerHChanges in sympathetic and parasympathetic cardiac activation during mental load: an assessment by spectral analysis of heart rate variabilityHomeost Health Dis1990331–22333
- BernardiLWdowczyk-SzulcJValentiCEffects of controlled breathing, mental activity and mental stress with or without verbalization on heart rate variabilityJ Am Coll Cardiol20003561462146910807448