
Abstract
Purpose
Persons with mild cognitive impairment (PwMCI) are at a higher risk of developing dementia than those without cognitive impairment. This research study aims to evaluate the effectiveness of a holistic health group intervention, which is based on the holistic brain health approach as well as an Eastern approach to health care, on improving the cognitive ability of Chinese PwMCI.
Research methods
In a randomized controlled trial (RCT), 38 Chinese PwMCI were randomly assigned to either a 10-session holistic health intervention group or the control group. The holistic health treatment group attempted to promote the acceptance of their illness, enhance memory and coping skills, develop a positive lifestyle, maintain positive emotions, and facilitate emotional support among participants. The 10-session holistic health group intervention was structured, with each session conducted once per week and ~90 minutes in length. Control group patients and their family caregivers received standardized basic educational materials that provided basic information on cognitive decline for them to read at home. The Montreal Cognitive Assessment (MoCA) test was used to assess the cognitive ability of PwMCI in the pre- and posttreatment periods by a research assistant who was blind to the group assignment of the participants.
Results
The paired-samples t-test indicated that the treatment group (n=18) showed significant improvement in the MoCA score, whereas the control group (n=20) did not. Moreover, 2×2 (group × time) repeated-measures analysis of covariance (ANCOVA) demonstrated that the holistic health group treatment was significantly more effective than the control intervention in improving the MoCA score, with a moderate effect size, and improving the delayed recall (ie, short-term memory), with a strong effect size, after controlling for age, sex, education, and marital status.
Conclusion
This present RCT provides evidence to support the feasibility and effectiveness of the holistic health group intervention in improving the cognitive and short-term memory abilities of PwMCI.
Introduction
Mild cognitive impairment (MCI) is an intermediate stage of cognitive function between normal cognitive aging and dementia.Citation1 Specifically, persons with MCI (PwMCI) are those who have subjective cognitive complaints, show cognitive impairment in one or more domains, preserve functional independence, and present no dementia.Citation2 The prevalence rate of MCI ranges from 10% to 20% for people aged 65 years or more.Citation1,Citation3 PwMCI are at risk of the development of dementia at a rate of 5%–10%, which is higher than that of healthy older people without MCI.Citation1,Citation4 Thus, there is an urgent need to develop effective interventions to improve the cognitive ability of PwMCI to delay their progression to dementia.
At present, the effectiveness of pharmacological treatment for MCI remains uncertain.Citation2,Citation3,Citation5 Furthermore, several reviews of research evidence have suggested that nonpharmacological interventions can improve the cognitive ability of PwMCI.Citation4,Citation6–Citation9 In particular, cognitive training,Citation7 physical exercise,Citation1,Citation10,Citation11 and social activitiesCitation12,Citation13 have been shown to be effective in improving the cognitive ability of PwMCI.
Recently, multicomponent intervention, which combines various kinds of nonpharmacological interventions, such as cognitive training, physical exercise, relation skills, and social group activities, into one single intervention has been developed and shown to be effective in improving the cognitive ability of PwMCI.Citation11,Citation14–Citation20 Additionally, after completing treatment with the multicomponent intervention, improvements in cognitive ability can be maintained up to 2 years.Citation21
However, generalizations of these positive research results on multicomponent intervention have been limited due to various factors. First, there is great variety within multicomponent interventions. For example, different multicomponent interventions may have different intervention durations, ranging from 6 weeks to 7 weeksCitation17,Citation18 up to 9 months.Citation15 Second, different multicomponent interventions have different theoretical approaches with a different emphasis in their program elements. Some multicomponent interventions focus more on developing memory skills,Citation15,Citation16,Citation18,Citation19 whereas others promote healthy lifestyles for brain health.Citation17,Citation19 Third, the provision of multicomponent intervention should be culturally sensitive when it is applied to Chinese PwMCI. Differences in linguistic property, cultural, and educational levels may affect the effects of training.Citation22 For example, Chinese PwMCI may not understand the mnemonic strategies originally designed for Western patients. Additionally, Chinese PwMCI prefer to practice tai chi to aerobics. Thus, it is important to indigenize the content of PwMCI multicomponent interventions in order to make them suitable for the local culture and context. Fourth, due to cultural influences, Chinese persons with neurocognitive disorder have somewhat different concerns about their cognitive decline.Citation23 Under traditional Chinese values, especially Confucianism, persons with neurocognitive disorder are perceived as those who are not competent members of society, those who fail to comply with the five cardinal relations, and those who cause “loss of face” and “shame” within the family and social systems.Citation24,Citation25 Thus, as shown in a local survey, Chinese persons with neurocognitive disorder express the fear of being labeled as mentally ill and losing their status within the family, in addition to feeling guilty for being dependent, being a burden to their family, and feeling helplessness.Citation23 Therefore, it is important for advocates of multicomponent intervention to address these special concerns of Chinese individuals with neurocognitive disorder.
Eastern holistic health approach
A multicomponent holistic health group intervention, which is founded on an Eastern approach to health care,Citation26,Citation27 has recently been developed to meet the special needs of Chinese people with neurocognitive disorders,Citation28 with the following characteristics. First, this approach emphasizes holistic care needs (ie, the biopsychosocial–spiritual health of individuals) rather than only targeting the cognitive decline. Additionally, the biological/physical, psychological, social, and spiritual aspects of individuals are considered to be interactive, and thus strategies that promote physical health will enhance brain health and cognitive ability. Second, according to the Yin-Yang philosophy, strengths and weaknesses coexist within individuals even when they are suffering from a chronic illness,Citation29 and therefore, this approach helps individuals to recognize their own strengths and mobilize support systems in facing with cognitive impairment. Third, this approach enhances individual coping skills and memory skills in order to combat cognitive decline. Fourth, this approach facilitates the development of a healthy lifestyle, such as adhering to a proper diet, physical exercise and recreational activities, maintaining a positive mood, and appreciating the family caregiver. Finally, this approach promotes the acceptance and tolerance of life adversities brought upon by their illness. Previous research results supported the efficacy of this group intervention for people with neurocognitive disorder and found that it significantly reduced depressive mood and improved the health-related quality of life of participants with neurocognitive disorder.Citation25,Citation28
This present study is an extension of a previous study.Citation28 This present study adds to the previous work by 1) modifying the contents of the holistic health group intervention to suit the needs of PwMCI and 2) evaluating the effectiveness of this holistic health group intervention in improving the cognitive ability of Chinese PwMCI. In the present study, in order to adapt the holistic health group intervention for PwMCI in a local context, the holistic health group intervention attempts to promote the acceptance of illness, enhance memory and coping skills, develop a positive lifestyle, maintain positive emotions, recognize individual strengths, improve communication skills with family caregivers, and facilitate emotional support among participants. Additionally, this holistic health group intervention helps participants to develop cognitive strategies, including internal and external strategies.Citation30 External strategies include modifying the living environment, as well as using aids such as calendars, checklists, and reminders. Internal strategies include attention, categorization, association, visual imagery, and mnemonics. It is hypothesized that this holistic health group intervention is effective in improving the cognitive ability of Chinese PwMCI.
Research methods
By adopting a randomized controlled trial (RCT) approach, 38 Chinese PwMCI were randomly assigned to either a treatment group or the control group. These participants were living at home and were recruited from centers for the elderly operated by nongovernmental organizations. The group assignment process was performed by DK Young, who was not involved in any data collection process. A research assistant who was blind to the group assignment of the participants used standardized assessment tools to collect the study data of all participants within 4 weeks before treatment and within 4 weeks after completing treatment. All participants received HK$100 as an incentive payment after completing all assessments.
Ethical considerations
The ethical aspects of this study were evaluated and approved by the Research Committee of the Hong Kong Baptist University (reference number: FRG1/14-15/050). Written informed consent was obtained from all participants with MCI, as well as their family caregivers, on the day of pretreatment assessment.
Treatment and control groups
The holistic health group intervention was structured and consisted of 10 sessions. Each session was conducted once per week and was, on average, 90 minutes in length. The group size was 8–10 PwMCI. Family caregivers of the treatment group patients were encouraged to participate in two sessions focusing on caring and communication skills. Each group was led by a social worker who had more than 2 years of working experience with neurocognitive disorders. A standardized manual was produced by the author for use in the group intervention. provides an outline of the contents of the holistic health group interventions. The social worker received training on the standardized manual by DK Young. Additionally, the author attended some group sessions, acting as observer without changing any group intervention contents, and provided regular supervision to the social worker to ensure that the standardized manual was properly and fully implemented. Moreover, the social worker used group work skills to facilitate sharing and mutual support among group participants.
Table 1 Session outline of 10-week holistic health group intervention for persons with mild cognitive impairment
The control group participants with MCI, as well as their family caregivers, received three pages of written educational material providing basic information on neurocognitive disorders, which they were encouraged to read at home. This information was summarized from an educational leaflet on neurocognitive disorder produced by the public health care unit. Control group participants and their family caregivers were not required to attend any group sessions and were contacted only during the pre- and posttreatment periods for assessment purposes.
Subject inclusion criteria
In this study, the inclusion criteria were as follows 1) age of 60 years or more; 2) a diagnosis of MCI or mild neurocognitive disorder according to the criteria of the Diagnostic and Statistical Manual of Mental Disorders (Fifth Edition);Citation31 3) an awareness of memory loss and a history of memory complaints; and 4) the ability to participate independently in a group setting. Participants who did not have a diagnosis of MCI or mild neurocognitive disorder were assessed by the researcher by using a screening tool (ie, the Montreal Cognitive Assessment [MoCA]).Citation32 The cognitive ability of participants was also assessed by the Mini Mental State Examination (MMSE) (Chinese version), which has been found to have satisfactory validity, internal consistency (α=0.80–0.95), and test–retest reliability (r=0.72).Citation33
Outcome assessment tools
The MoCA tool (Chinese version),Citation32 which has been validated and widely used internationally, was used for outcome assessment.Citation1,Citation3,Citation34 The MoCA assesses various cognitive domains, including attention and concentration, executive functions, memory, language, visuoconstructional skills, conceptual thinking, calculations, and orientation. The reliability and validity of the Chinese version of MoCA have been tested to be satisfactory (Cronbach’s α=0.77).Citation32 The score is summed over the items. The whole scale has a maximum score of 30, with higher scores indicating better cognitive ability. According to the original scale,Citation34 a MoCA cutoff point <26 and >17 is indicative of MCI, which has been adopted in this study.
Data analyses
The analysis was carried out according to an intention-to-treat principle, using last observation carried forward (LOCF) analysis for missing data. The baseline demographic and clinical characteristics of the treatment and control groups were compared by using chi-square (χ2) tests for the categorical variables and independent samples t-test for continuous variables. A paired-samples t-test was used to analyze the significant changes in the pre- and posttreatment MoCA scores for both the treatment and the control groups. To investigate the magnitude of the treatment effect, the outcome measure was analyzed using the general linear model 2×2 repeated-measures analysis of covariance (ANCOVA), with the two groups (treatment and control groups) as between-subject factors and the two outcome assessments (pre- and posttreatment scores) as within-subject factors, adjusting for age, sex, education, and marital status. The effect sizes were calculated using the partial eta-square. For the partial eta-square, the values 0.01, 0.06, and 0.14 were considered small, moderate, and large effects, respectively.Citation35 For all analyses, two-tailed P-values <0.05 indicate statistical significance. Data analyses were performed using SPSS 22.0 (IBM Corporation, Armonk, NY, USA).
Results
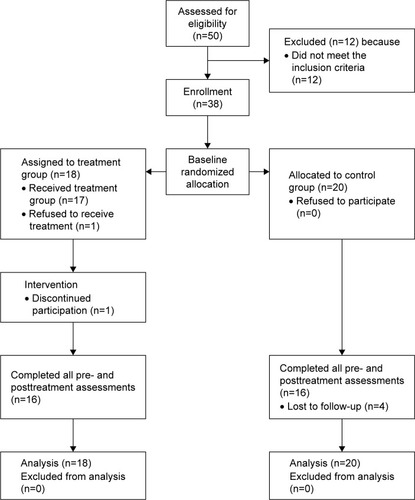
A total of 50 participants with MCI were recruited from the centers for the elderly. However, 12 did not meet the inclusion criteria and were hence excluded. The remaining 38 subjects were randomly assigned to a treatment group or the control group. Of these, 18 were placed in the treatment group and 20 were assigned to the control group. Two treatment groups and two control groups were formed. Each treatment group consisted of ~8–10 participants with MCI. illustrates the recruitment procedure. After the study was completed, 32 treatment group subjects finished all of the assessments. Two dropped out from the treatment group and four dropped out from the control group.
Figure 1 Flow of participants through each stage of the study.
Characteristics of the research sample
provides the baseline demographic data and measures of all the participants with MCI (n=38). The mean age of the participants was 75.0 (SD =6.0) years. The majority (86.8%, n=33) were female, had received a primary school or higher education (78.9%, n=30), and lived with their family members (65.8%, n=25). A little more than half (52.6%, n=20) were married, followed by widowed, divorced, or separated participants (44.7%, n=17). None of them received a diagnosis of MCI from their medical officers, and all of them were as assessed as having MCI as per the MoCA by the researcher. Two-thirds (63.2%, n=24) suffered from one or more physical illnesses, and they reported no change in medication during the pre- and posttreatment period.
Table 2 Baseline characteristics of all participants with mild cognitive impairment
Baseline assessment score
The independent t-test and chi-square analyses showed no significant difference between the treatment and control groups in terms of all baseline demographic variables, including the MoCA and MMSE scores ( shows the data analysis). Additionally, those participants who dropped out did not show any significant difference in any of their baseline demographic and clinical variables compared with the retained participants. Among all participants, a mean MoCA score of 21.5 (SD =2.2) and mean MMSE score of 24.8 (SD =1.6) were observed.
Treatment outcomes
summarizes the change in the MoCA score for both the treatment and the control groups. The results of a paired-samples t-test demonstrate that after completing the group intervention, the treatment group showed significant improvement in the MoCA score from 21.00 (SD =2.81) to 23.56 (SD =2.90) (t=4.25, P<0.01). Additionally, the treatment group showed significant improvement in the adjusted MoCA score from 21.61 (SD =2.50) to 24.17 (SD =2.88) (t=4.25, P<0.01), alternative trail making score from 0.56 (SD =0.51) to 0.83 (SD =0.38) (t=2.56, P<0.05), naming score from 2.39 (SD =0.78) to 2.61 (SD =0.50) (t=2.20, P<0.05), and delayed recall score from 1.00 (SD =1.41) to 2.11 (SD =1.57) (t=2.56, P<0.05).
Table 3 Pretest, posttest, and comparison of score change between the intervention and control groups on assessment
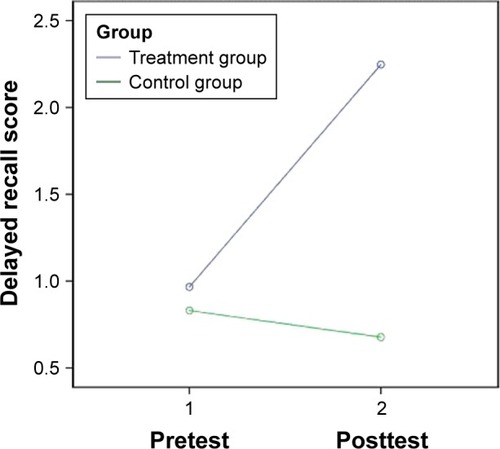
The 2 (group) ×2 (time) repeated-measures ANCOVA demonstrates that the holistic health treatment was significantly more effective than the control intervention in improving the MoCA score, controlling for age, sex, education, and marital status (F=4.45, P<0.05), with a moderate-to-strong effect size (partial eta-square =0.13). Additionally, the holistic health intervention was significantly more effective than the control intervention at improving the adjusted MoCA score (F=4.28, P<0.05), with a moderate-to-strong effect size (partial eta-square =0.12), and improving the delayed recall score (F=5.04, P<0.05), with a strong effect size (partial eta-square =0.14), after controlling for age, sex, education, and marital status ( and ).
Figure 2 Change in adjusted MoCA score of the treatment and the control groups.
Note: Covariates appearing in the model are evaluated at the following values: age =74.97, sex =0.13, education =2.18, marital status =3.26.
Abbreviation: MoCA, Montreal Cognitive Assessment (Hong Kong version).
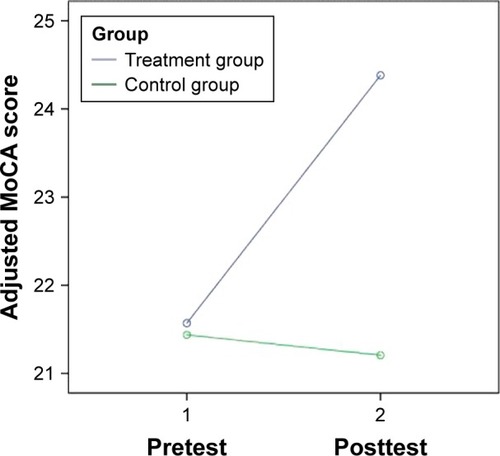
Figure 3 Change in delayed recall score of the treatment and the control groups.
Discussion
This present study shows that the multicomponent holistic health group intervention significantly improves the cognitive ability of participants with MCI, supporting the feasibility and effectiveness of the multicomponent intervention in the local context. In particular, ANCOVA and paired-samples t-test demonstrate that the holistic health group intervention was more effective than the control intervention at improving the overall cognitive ability and delayed recall (ie, short-term memory) of PwMCI even after controlling for the differences between holistic health group treatment and control groups in terms of various demographic variables such as age, sex, educational level, and marital status.
Two theoretical approaches of multicomponent intervention have been developed in Western countries. The first approach focuses more on evidence-based cognitive interventions.Citation15,Citation16,Citation18,Citation20 There are three types of cognitive interventions: cognitive stimulation, cognitive training, and cognitive rehabilitation.Citation36,Citation37 Cognitive stimulation emphasizes the activities conducted in a group format to increase cognitive and social functioning in a nonspecific manner. Cognitive training involves teaching strategies and skills to improve specific aspects of cognitive functioning. Cognitive rehabilitation entails individually tailored programs targeting specific activities of daily living. Research suggests that cognitive training,Citation7,Citation9 cognitive stimulation,Citation38 and cognitive rehabilitationCitation39 are effective in improving cognitive functioning for PwMCI. Accordingly, a number of specific training activities (eg, visual imagery, mnemonics, and so on) have been developedCitation14,Citation16,Citation40 and are included – in addition to physical exercise as well as social and recreational activities – in multicomponent interventions.Citation14,Citation18,Citation20 However, there are great variations among interventions based on this approach, including differences in duration, focus, and training activities. More research studies are needed to investigate the appropriate duration, focus, and training activities for PwMCI across cultures and societies.
A second approach, named the holistic brain health approach, has recently been developed.Citation17,Citation19 In this method, a holistic approach to brain health is employed with a combination of diet, exercise, socialization, stress reduction, and mental stimulation and this method can delay the onset of neurocognitive disorder.Citation17 Research supports the effectiveness of short-term structured interventions based on this holistic brain health approach in terms of improving the cognitive functioning of PwMCI.Citation17,Citation19 For example, a 10-session multicomponent intervention that emphasized establishing a healthy lifestyle through learning memory skills, stress reduction, recreation, nutrition, and community resources was found to enhance memory strategies in the daily life of PwMCI.Citation19 However, because previous research studies did not report a change in the objective cognitive ability of research subjects after intervention,Citation17,Citation19 it remains unclear whether the holistic brain health approach is effective at improving the cognitive ability of PwMCI.
As discussed previously, due to cultural influence, Chinese individuals with neurocognitive disorder have some-what different concerns about their cognitive decline.Citation23,Citation25 Chinese persons with neurocognitive disorder express fear of being labeled as mentally ill and losing their status within the family, in addition to feeling guilty for being dependent, being a burden to their family, and feeling helplessness.Citation23 Therefore, it is important for advocates of a multicomponent intervention to address these special concerns of Chinese PwMCI.
The holistic health group intervention, which is founded on the Eastern health care approach, is a unique application and adaptation of the holistic brain health approach in Chinese cultures and societies. This present study shows that the short-term structured holistic health group intervention, which aims to meet the special concerns of Chinese PwMCI, significantly improves the cognitive ability of participants with MCI, supporting the feasibility and effectiveness of the short-term structured multicomponent intervention for PwMCI in the local context. More important, the present RCT is one of the few studies demonstrating the effectiveness of the short-term structured holistic brain health intervention to improve the objective cognitive ability and short-term memory of PwMCI.
The identification of the essential group elements contributing to the effectiveness of this holistic health group intervention certainly needs further investigation. Some observations on the effective group elements of this holistic health group intervention are highlighted herein. First, it is feasible, appropriate, and useful for this holistic health group intervention to promote the acceptance of illness, develop a positive lifestyle, maintain positive emotions, recognize individual strengths, and improve communication and relationships with family caregivers among PwMCI. Second, it is also important for the holistic health group intervention to enhance various internal and external cognitive strategies for participants,Citation30 such as attention, categorization, association, visual imagery, and mnemonics. Third, it is important for the holistic health group intervention to facilitate emotional support among the participants who share similar difficulties that are encountered in daily living. By receiving emotional support from others, participants can reduce their anxiety and helplessness, which are typical characteristics of MCI.
Several methodological limitations of this RCT require attention. First, the generalizability of the research results is limited by the small sample size. In the future, a larger-scale RCT should be conducted to further validate the effectiveness and benefits of the holistic health group model for PwMCI across cultures and societies. Second, the studied group was dominated by female participants, which may limit the generalization of research results to male participants. Third, this studied group lacked proper control in drug treatment between the treatment and the control groups, although all participants reported no change in medication during the pre- and posttreatment period. The change in cognitive functioning might be due to the change in medications, which might also limit generalization of the research result. Finally, in this study, promoting the acceptance of illness, enhancing learning and memory skills, developing a positive lifestyle, maintaining positive emotions, recognizing individual strengths, improving relationships with family caregivers, and facilitating emotional support among participants are thought to be essential elements of this holistic health group intervention. However, no standardized tools have been adopted to assess these elements in this study. Therefore, further research studies should be conducted to identify the essential elements of holistic health group interventions for PwMCI.
This present study shows that a holistic health group intervention significantly improves the cognitive and memory ability of participants with MCI, supporting the feasibility and effectiveness of holistic health group interventions.
Acknowledgments
This research work was financially supported by the Faculty of Social Sciences, Hong Kong Baptist University (FRG1/14-15/050).
Disclosure
The authors report no conflicts of interest in this work.
References
- PetersenRCMild cognitive impairmentN Engl J Med2011364232227223421651394
- PetersenRCCaraccioloBBrayneCGauthierSJelicVFratiglioniLMild cognitive impairment: a concept in evolutionJ Intern Med2014275321422824605806
- GordonCMartinDJMild cognitive impairmentExpert Rev Neurother201313111247126124175723
- TeixeiraCVLGobbiLTBCorazzaDIStellaFCostaJLRGobbiSNon-pharmacological interventions on cognitive functions in older people with mild cognitive impairmentArch Gerontol Geriatr201254117518021397960
- CooperCLiRLyketsosCLivingstonGTreatment for mild cognitive impairment: systematic reviewBr J Psychiatry2013203325526424085737
- HorrTMessinger-RapportBPillaiJASystematic review of strengths and limitations of randomized controlled trials for non-pharmacological interventions in mild cognitive impairment: focus on Alzheimer’s diseaseJ Nutr Health Aging201519214115325651439
- LiHLiJLiNLiBWangPZhouTCognitive Intervention for persons with mild cognitive impairment: a meta-analysisAgeing Res Rev201110228529621130185
- ReijndersJHeugtenCVBoxtelMVCognitive interventions in healthy older adults and people with cognitive impairment: a systematic reviewAgeing Res Rev201312126327522841936
- ScottJSpectorAA review of the effectiveness of memory interventions in mild cognitive impairmentInt Psychogeriatr201123452653820946704
- BakerLDFrankLLFoster-SchubertKEffects of aerobic exercise on mild cognitive impairmentArch Neurol2010671717920065132
- SuzukiTShimadaHMakizakoHEffects of multicomponent exercise on cognitive function in older adults with amnestic mild cognitive impairment: a randomized controlled trialBMC Neurol201212112823113898
- HughesTFFlattJDFuBChangCCHGanguliMEngagement in social activities and progression from mild to severe cognitive impairment: the MYHAT studyInt Psychogeriatr201325458759523257280
- PitkalaKHRoutasaloPKautiainenHSintonenHTelvisRSEffects of socially simulating group intervention on lonely, older people’s cognition: a randomized controlled trialAm J Geriatr Psychiatry201119765466321709611
- BuschertVCFrieseUTeipelSJEffects of a newly develop cognitive intervention in amnestic mild cognitive impairment and mild Alzheimer’s Disease: a pilot studyJ Alzheimers Dis201125467969421483095
- DannhauserTMCleverleyMWhitfieldTJFlectcherBStevensTA complex multimodal activity intervention to reduce the risk of dementia in mild cognitive impairment – ThinkingFit: pilot and feasibility study for a randomized controlled trialBMC Psychiatry201414112924886353
- HwangHRChoiSHYoonDHThe effect of cognitive training in patients with mild cognitive impairment and early Alzheimer’s Disease: a preliminary studyJ Clin Neurol20128319019723091528
- HyerLScottCKylesJDhabliwalaJMcKenzieLMemory intervention: the value of a clinical holistic program for older adults with memory impairmentAging Ment Health201418216917823889364
- RappSBrenesGMarshAPMemory enhancement training for older with mild cognitive impairment: a preliminary studyAging Ment Health20026151111827617
- TroyerAKMurphyKJAndersonNDMoscovitchMCraikFIMChanging everyday memory behavior in amnestic mild cognitive impairment: a randomized controlled trialNeuropsychol Rehabil2008181658817943615
- TsolakiMKountiFAgogiatouCEffectiveness of nonpharmacological approaches in patients with mild cognitive impairmentNeurodegener Dis20118313814521135531
- BuschertVCGieglingITeipelSJLong-term observation of a multicomponent cognitive intervention in mild cognitive impairmentJ Clin Psychiatry20127312e1492e149823290333
- KwokTWongAChanGEffectiveness of cognitive training for Chinese elderly in Hong KongClin Interv Aging2013821321923440076
- MokELaiKYWongLFWanPLiving with early-stage dementia: the perspective of older Chinese peopleJ Adv Nurs200759659160017727403
- LamCSTsangHWHCorriganPWChinese lay theory and mental illness stigma: implications for research and practicesJ Rehabil20107613540
- YoungKWKwokTNgPSingle blind randomized control trial on support group for Chinese persons with mild dementiaClin Interv Aging20142014921052112
- ChanCLWAn Eastern Body-Mind-Spirit Approach – A Training Manual with One Second Techniques2nd edHong KongHong Kong University2006
- LeungPYChanLWNgSMLeeMYTowards Body–Mind–Spirit integration: East meets West in clinical social work practiceClin Soc Work J2009374303311
- YoungKWA randomized control study on psycho-education group on improving health-related quality of life of Chinese persons with major neurocognitive disorderClin Gerontol2016395449467
- NgPTsunASuSYoungKWCognitive behavioural therapy in the Chinese cultural context: a case reportAsia Pac Psychiatry20135320521123857732
- HutchensRLKinsellaGJOngBKnowledge and use of memory strategies in amnestic mild cognitive impairmentPsychol Aging201227376877722122606
- American Psychiatric AssociationDiagnostic and Statistical Manual of Mental Disorders5th edWashington, DCAmerican Psychiatric Association2013
- YeungPYWongLLChanCCLeungJLMYungCYA validation study of the Hong Kong version of Montreal Cognitive Assessment (HK-MoCA) in Chinese older adults in Hong KongHong Kong Med J201420650451025125421
- ChiuHFLeeHCChungWSKwongPKReliability and validity of the Cantonese version of mini-mental state examination – a preliminary studyJ Hong Kong Coll Psychiatr199442528
- NasreddineZSPhillipsNABedirianVThe Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairmentJ Am Geriatr Soc200553469569915817019
- CohenJStatistical Power Analysis for the Behavioral Sciences2nd edHillsdale, NJLawrence Erlbaum Associates1988
- BellevilleSCognitive training for persons with mild cognitive impairmentInt Psychogeriatr2008201576617958927
- FaucounauVWuYHBoulayMDe RotrouJRigaudASCognitive intervention programmes on patients affected by mild cognitive impairment: a promising intervention tool for MCIJ Nutr Health Aging2010141313520082051
- MoroVCondoleoMRSalaFPernigoSMorettoGGambinaGCognitive stimulation in a-MCI: an experimental studyAm J Alzheimers Dis Other Demen201227212113022495340
- KurzAPohlCRamsenthalerMSorgCCognitive rehabilitation in patients with mild cognitive impairmentInt J Geriatr Psychiatry200924216316818636436
- KinsellaGJMullalyERandEEarly intervention for mild cognitive impairment: a randomized controlled trialJ Neurol Neurosurg Psychiatry200980773073619332424