
Abstract
Background
Group-based psychosocial therapy, such as group Cognitive Stimulation Therapy, improves cognition and quality of life in people living with dementia. Neuropsychiatric symptoms and restricted mobility are common complications for people with Parkinson’s-related dementia (PRD) and may limit access to, and participation in, group activities. This study describes the development of a condition-specific, home-based psychosocial therapy for people with PRD ready to be trialled in a clinical population.
Methods
By means of a multistage process, a draft therapy manual was developed in an iterative manner through collaboration with medical experts, researchers and Patient and Public Involvement (PPI) representatives. In stage 1, an extensive literature search of psychosocial therapies for dementia with potential relevance for Parkinson’s disease (PD) was undertaken to select a candidate therapy for adaptation. In stage 2, qualitative feedback from stakeholders and intelligence regarding existing nonpharmacological therapies for cognitive impairment in PD was combined to produce a prototype therapy manual. In stage 3, the manual was field tested in: 1) a home-setting using a 25-item assessment tool; and 2) at a local PD support group with PPI representatives. Based on the feedback from this phase, final design modifications were implemented and a draft therapy manual produced.
Results
The manual was developed in an iterative manner. Interview and focus group transcripts identified three enduring themes: manual form and content, therapy acceptability by people with PRD, and companion guidance and support. Major adaptations included: removal of discrete levels of task complexity, removal of images that were potentially hallucinogenic or lacked clarity, and updating of the content.
Conclusion
We have successfully developed a Cognitive Stimulation Therapy-based psychosocial therapy specifically adapted for people with PRD. The therapy is ready to trial in a pilot randomized controlled study.
Introduction
England’s National Institute for Health and Clinical Excellence guidelinesCitation1 recommend that people with dementia have timely access to a psychosocial therapy, such as group Cognitive Stimulation Therapy (CST). Therapies such as CST may be appropriate for the less common types of dementia; however, they often do not meet the more complex needs (ie, restricted mobility, development of an inferiority complex within a group and neuropsychiatric symptoms) of people with dementia in the context of movement disorders.
Individuals with Parkinson’s disease (PD) can experience a wide range of motor and non-motor symptoms that present challenges in undertaking day-to-day activities.Citation2–Citation4 Approximately 30% of people with early, unmedicated PD report problems with attention and memory.Citation5 A quarter of people with PD will develop mild cognitive impairment (PD-MCI) and are at increased risk of developing dementia.Citation6 The likelihood is that over 80% of people with PD will develop dementia after 20 years.Citation7 People who have dementia with Lewy bodies (DLB) present with similar cognitive and motor symptoms to those with PD and dementia (PDD)Citation8 and face similar challenges in accessing currently available psychosocial treatment. Thus, there is a clinical need to develop and evaluate psychosocial support interventions for people with Parkinson’s-related dementia (PRD).
The Medical Research Council (MRC) guidelines for developing and evaluating complex interventionsCitation9 recommend that complex interventions are developed systematically using the best available evidence and supported by an appropriate theoretical framework. Despite these guidelines, early findings from an ongoing Cochrane review of trials of cognitive training (a technique focusing on the repetition of cognitive exercises that may strengthen impaired cognitive processes) for people with PD and cognitive impairment suggests that relatively few studies meet these criteria.Citation10 The guidelines also recommend that interventions be developed to the point where they can reasonably be expected to have a worthwhile effect. One approach to following these guidelines is to modify an intervention that already has a robust theoretical, empirical and clinical rationale and an emerging evidence base of efficacy. The added benefit of this approach is that the development time can be reduced and the intervention is more likely to be scalable and sustainable.
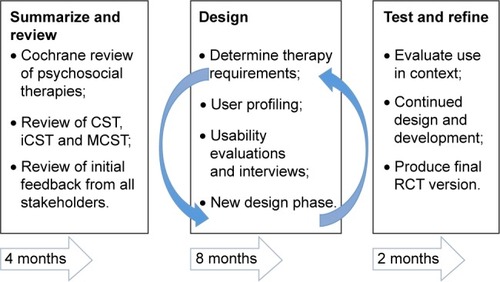
This paper describes the methods and outcomes relating to the adaptation of a psychosocial therapy for people with PRD and their companions. To meet the needs and challenges of this specific clinical population, we adopted a user-driven development framework including principles such as: active user involvement, iterative design, prototyping, evaluations with real users and usability considerations ().Citation11 Given the increased levels of caregiver burden in this population, the acceptability and tolerability of the therapy by companions (historically referred to as carers or caregivers) was also carefully considered. The effectiveness of the adapted therapy will be subsequently examined in an innovative feasibility and efficacy trial following the MRC’s clinical guidelines.Citation9
Figure 1 The user-driven development framework adopted during the development of CST adapted for people with Parkinson’s-related dementias (CST-PD).
Aims and objectives
The aim of this study was to develop a comprehensive psychosocial therapy specifically adapted for people with PRD and their companions. In this context, people with PRD comprise those who have PDD, PD-MCI or DLB. The specific objectives were:
To conduct an extensive literature search to: 1) summarize and review the existing evidence of psychosocial therapies for cognitive impairment and dementia related to PD; 2) develop a theoretical understanding of the likely processes of change; and 3) select a candidate therapy for adaptation (stage 1; summarize and review).
Identify aspects of the candidate therapy that need to be adapted for people with PRD: Combine feedback from consultations with Patient and Public Involvement (PPI) representatives, clinical experts and intelligence regarding existing nonpharmacological therapies for cognitive impairment in PD to identify an initial set of adaptations required to produce the prototype therapy manual prior to field testing (stage 2; design).
Evaluate the design against stakeholder requirements: Field test the prototype therapy manual to: 1) obtain feedback on the usability of the adapted therapy delivered by a companion in a home-setting and 2) obtain feedback from PPI representatives and clinical experts (stage 3; test and refine).
Stage 1 – summarize and review (existing research)
To summarize and review the existing evidence of psychosocial therapies for cognitive impairment and dementia related to PD, we conducted a scoping exercise followed by a systematic review of seven studies (the number of studies reviewed is an indication of the paucity of high-quality research in this area). Scoping exercises do not evaluate the quality of the evidence reviewed; however, they can provide a narrative integration of evidence when the research area is complex and has not been comprehensively reviewed before.Citation12 We considered studies that recruited people with PRD and: 1) reported a comparison between a psychosocial intervention (cognitive-related) and a control group; 2) reported a comparison between pre- and posttest; and 3) reported the experiences of people with dementia participating in a psychosocial intervention. To map rapidly the key concepts underpinning effective cognitive stimulation in this clinical population, we synthesized knowledge from an ongoing, larger systematic review study.Citation10 Throughout the review process, stakeholders (clinicians and PPI representatives) were consulted to provide insight on what the literature failed to highlight. The process was iterative, rather than linear, and involved cycling between early findings and new insights. The findings from the scoping and systematic review are now discussed.
Early psychosocial therapies for people with dementia, such as Reality OrientationCitation13 and Reminiscence Therapy,Citation14,Citation15 evolved in parallel with the aim of reducing disorientation and improving well-being. Reality Orientation involves the use of supporting aids to establish time, season, location and other current or basic personal information, but has been criticized for being rigid and confrontational, with doubts being raised about the therapy’s capability for demonstrating any clinically significant improvement.Citation16 Supported by the use of memory aids (photographs, books or objects), Reminiscence Therapy involves discussing past experiences and events, but has also been found to have considerable shortcomings. A recent randomized, controlled trial of Reminiscence Therapy with people with dementia demonstrated no clinical benefit compared to “treatment as usual”, and anxiety levels had increased in companions.Citation17 Continued use of both of these early psychosocial therapies has been cautioned by the American Psychiatric Association.Citation18
More recently, use of CST has gained momentum and is recommended by a large number of National Health Service trusts in the UK. The principle behind CST supports the engagement in cognitive and social activities to enhance cognitive functioning and quality of life of people with dementia. The therapy was developed by systematically selecting the aspects of the early psychosocial therapies that were beneficial and building on these techniques by incorporating the discussion of new ideas and thoughts into various cognitively stimulating activities and topics. A randomized, controlled trial of the CST demonstrated improvements in quality of life and cognitive functioning.Citation19 Economic analysis showed CST was cost-effectiveCitation20 and that the results for cognition compared favorably with trials of cholinesterase inhibitors for Alzheimer’s disease. Since these early studies, the evidence base supporting the use of CST to improve outcomes for people with dementia has continued to grow.Citation19
Following research on the effects of group CST, recent research has reported significant effects (quality of life and cognition) for people attending maintenance CST sessions (a follow-on therapy after group CST)Citation21,Citation22 and, to a lesser extent, individual CST (iCST).Citation19 iCST is delivered individually to a person with dementia by a friend or a family member. A recent randomized, controlled trial of iCST showed that iCST did not result in improved cognition or quality of life for the person living with dementia, however, participating in iCST did enhance the quality of the caregiving relationship and caregivers’ quality of life.Citation23,Citation24 These findings are relevant here, as companions of people with PRD are reported to experience burden and a lower quality of life due to the responsibility of supporting the complex physical and cognitive needs of people with PRD.Citation25 We are aware of only one exploratory studyCitation26 that has assessed the effectiveness of home-based CST in people with PRD using neuropsychological assessment and molecular analysis. The authors reported that scores on the Montreal Cognitive Assessment,Citation27 Parkinson’s Disease Questionnaire-39Citation28 and Quality of Life – Alzheimer’s DiseaseCitation29 significantly improved following a 7-week period of CST delivered by a family member. In addition, levels of serum brain-derived neurotrophic factor (BDNF; a neuroprotectant that colocalizes with dopaminergic neurons) significantly improved at posttest. The sample size in this study was small and there was no control group; however, the ability to demonstrate positive change in a highly objective biomarker is encouraging.
Given the benefits offered by CST, maintenance CST, iCST and a recent Cochrane Review recommending systematic evaluation of different modalities of CST, including real-life settings,Citation16 the home-based companion-delivered iCST was selected as the candidate therapy for adaptation. The modified version is henceforth referred to as CST-PD.
Process of change
In accordance with MRC guidance for developing and evaluating complex interventions,Citation9 a good theoretical understanding of how the intervention effects change is required in order to identify and strengthen areas of weakness within the intervention.Citation30 Prior to the design and prototyping stage, a literature scoping exercise was performed to identify the potential processes of change. At a fundamental level, for the people with PRD, the therapy may result in neurobiologic or psychosocial changes or a combination of the two. Recent evidence supports the idea that nonpharmacologic therapies exert action on neurobiologic processes within the brain.Citation26,Citation31,Citation32 For example, Angelucci et alCitation31 demonstrated that cognitive training elevates BDNF in individuals with PD. The mechanism by which BDNF improves cognition is not yet fully understood, nor is it likely to be the sole mechanism responsible for clinically significant change, but only one of the components of which we are currently aware. While cognitive stimulation differs from cognitive training, the former therapy involving discussion and activities as opposed to guided practice on a standard set of cognitive tasks,Citation33 an association between cognitive stimulation and serum BDNF has also been reported.Citation26 The latter study is of particular relevance to the current research as the CST was delivered by family members in the home environment. Collectively, these studies suggest that if cognitive stimulation has the potential to elevate BDNF, the growth factor could be considered for use as a biomarker in future large-scale clinical trials of CST and adapted versions.
In addition to neurobiological variables, it is important to consider psychological and social factors. Social stigma or other socially imposed barriers can be a significant source of distress and thus impact on outcome.Citation34 Examples of psychosocial issues include negative social interactions, unemployment or early retirement due to symptoms, physical disability that prevents access to certain environments and changes to family life, such as increased dependency on a companion or partner.Citation34–Citation37 Negative psychosocial factors can lead to a decrease in personal efficacy, psychological well-being, and relationship satisfaction and increased social isolation and depression.Citation35,Citation36,Citation38,Citation39 CST-PD will seek to address the negative psychosocial outcomes of PDD, PD-MCI and DLB by providing opportunities for companion-supported mastery experiences; having the therapy delivered by a known and significant other may allow people with PRD to feel more comfortable challenging themselves in cognitively stimulating activities. Improvements in perceived personal efficacy, through mastery experiences, could foster interest and (re)engagement in social or previously enjoyed activities, lower vulnerability to depression and improve relationship satisfaction.Citation40
It is also important to consider personal efficacy from the companions’ point of view: the change effected by the intervention may be influenced by the companions’ beliefs in their ability to deliver the therapy (instructional efficacyCitation39). Companions’ level of perceived efficacy to motivate the people with PRD and promote mental stimulation may affect the therapy environment, the level of adherence, the quality of therapy delivered and, ultimately, outcomes for people with PRD (eg, cognition and quality of life). In school-based studies, instructors with high levels of instructional efficacy are reported to devote more time to learning, offer the appropriate level of help and praise and encourage autonomy.Citation41 While CST-PD does not aim to create a school-based environment at home, there is potential for companions’ instructional efficacy to act as a change agent and influence therapy outcomes. Throughout the development of CST-PD, companions will be consulted to identify their needs and to develop the necessary recourses to support instructional efficacy.
Stage 2 – design (modeling and piloting phases)
In the initial meeting with stakeholders (clinical experts, researchers and a PPI advisory group), user consultations took place to identify issues related to the nature of tasks and the therapy environment. Three key factors were identified: 1) the potential impact of symptom-specific issues on the therapy, for example, physical limitations from motor impairments, fluctuating levels of alertness and motor function, hallucinations and/or delusions, person-specific cognitive impairment, high levels of apathy and ability to promote self-management; 2) companions’ confidence in delivering CST-PD; and 3) whether physical activity-based tasks would be appropriate as part of the therapy. To fully address these issues, perspectives from professionals, companions and people with PRD were sought.
Methods
Participants
PD professionals (n=5), patient participants (n=3) and companions (n=2) were recruited from neurology and geriatric psychiatry services in Greater Manchester. Patient participants had a diagnosis of PD-MCI, PDD or DLB according to the appropriate consensus criteria for each condition.Citation42–Citation46
Procedure
The study received ethical approval from Yorkshire and the Humber–Bradford Leeds Research Ethics Committee (Reference: 15/YH/0024). All participants provided written informed consent or had a nominated consultee who provided the appropriate declaration. Focus groups were conducted by a CST-trained cognitive neuropsychologist and a psychology research assistant at the University of Manchester. PD professionals, companions (in this case, spouses) and people with PRD were invited to attend separate focus groups. Based on the methods by Krueger and CaseyCitation47 and adapted for dementia by Bamford and Bruce,Citation48 the groups were intentionally small, with no more than eight participants plus facilitators. As some companions and people with PRD were unable to attend the focus groups due to unforeseen medical or caring responsibilities, a second focus group was held for companions and semi-structured interviews were conducted with a further companion and two people with PRD, in the home setting.
A semi-structured interview design probed opinions relating to a number of issues specific to people with PD and DLB, as well as those identified by our PPI advisory group, including the suitability of tasks to motor difficulties, psychiatric issues and cognitive difficulties. Digital voice recordings were made of all focus groups and interviews to enable transcription and analyses.
Focus groups
Professionals were split into two groups and asked to evaluate six activities, spanning three topics, plus evaluate the introduction section of the original iCST manual. The groups were then asked to describe their evaluation to the other party, before having an open discussion of the points identified by the PPI advisory group. Finally, opinion was sought for five new topics, devised by the research team, before concluding the focus group with a yes/no topic inclusion/exclusion checklist to determine which subject areas were deemed most appropriate for the adapted therapy.
In the focus group for companions, participants were invited to try several of the activities, in pairs, over a range of different topic areas. Open discussion took place after each topic, with focus on the issues identified by the PPI advisory group. The focus group concluded with a yes/no topic inclusion/exclusion checklist.
The focus group of people with PRD involved a short group CST session and preferences were observed from the conversations that resulted. This focus group also concluded with a yes/no topic inclusion/exclusion checklist.
Transcript analysis and reporting
To ensure an iterative development process, data analysis ran alongside data collection, that is, subsequent focus groups were adapted using information obtained from previous sessions. The process of analysis began with reading and re-reading each transcript. Salient comments were noted and grouped by commonality, within and across transcripts. Rereading, comparison and re-grouping of comments continued until the main themes and subthemes were identified. Data were reported in accordance with an abbreviated consolidated criteria for reporting qualitative research (COREQ) structure.Citation49
Results
Three main themes were identified and are presented in with subthemes and frequency of comments. The professionals provided comments on all but 3 of the 28 subthemes (89%). In contrast, companions and patients identified with a substantial proportion of the subthemes (64% and 61%, respectively), but tended to focus on specific issues that they considered most relevant to them.
Table 1 Summary of themes and subthemes identified from focus groups and interviews
To accurately represent the views of the participants, a single quote from each theme has been selected (agreed among authors), with five additional examples in .
Table 2 Additional examples of content within each major qualitative theme
Theme 1: manual form and content
All parties agreed that the content needed updating (eg, add topics on technology, computers, mobile phones) as well as making topics culturally inclusive. Professionals suggested that the topics should include: art, history, geography, pets, books, transport and sports (eg, golf and cycling), among others. People with PRD did not want to avoid sensitive topics, but rather viewed CST-PD as an opportunity to facilitate discussion that otherwise would not usually happen:
[…] would it be possible for people like myself to have a general discussion on “do you miss work?”, “what elements of work do you miss?”. I can’t see it will work for all but maybe for some, you know […] I miss work so much, I miss the hassle, I miss the estimating, I miss the hiring, the firing, doing wages and all sorts. If I hadn’t got ill, I don’t think I would have ever retired. [Person with PRD]
In the iCST manual, each topic is split into two levels of difficulty; however, professionals highlighted that this format may be demotivating for those with deteriorating level of cognitive function. Professionals also felt that color-coded sections would be of benefit to ease the selection of topics based on one’s interest. There was consensus that lengthy paragraphs should be avoided and more images should be included to keep topics from becoming dry and cluttered. Companions also suggested the use of good-quality and thin paper, as thicker paper can cause problems with page turning in people with tremor. Professionals and companions also pointed out that any speech impairment might make reading aloud difficult, so any instructions to read aloud should be optional.
Key recommendations
Encourage opinion-based questions.
Include more photography, limit paragraph length.
Modernize and extend the topic content, make it multicultural.
Remove the two discrete levels of complexity and gradually increase the complexity of the tasks within each topic.
Color code topic sections.
Include optional instructions to read information aloud.
Theme 2: therapy acceptability in PD
All parties expressed the desire for the CST-PD to improve cognition, and professionals suggested card games as a potential tool to help with strategy and memory. Companions felt that the inclusion of constructive activities might successfully distract people with PRD from the compulsive, repetitive and stereotyped behaviors known as punding. Companions and people with PRD expressed polarized views of apathy: companions were concerned about getting individuals started with the therapy, whereas people with PRD were more positive and felt that the therapy would be motivating, encouraging and would alleviate boredom:
I love things like this, I do. I enjoy it. It’s good fun as well and it gives you something to talk about. [Person with PRD]
Professionals and people with PRD commented on visual and perceptual issues and pointed out that in the original iCST manual, some images were too busy and confusing with many shapes and colors that may cause hallucinations. The professionals were keen for art topics to remain, but wanted art images to be less vivid, disturbing and chaotic. Professionals also thought that abstract questions relating to art (eg,“Do you think there is a message behind the painting?”) or superstition-based questions should be reconsidered and revised to avoid precipitating or perpetuating complications such as delusions.
With regards to motor impairment, all participants agreed that delivering CST-PD in the home was most acceptable, and might help reduce feelings of isolation or boredom. Professionals and some companions were concerned about the physical activity-based tasks in the existing therapy. Following a lengthy discussion, it was determined that without individual physiotherapist assessment, the potential risks of including physical exercise activities outweighed the potential gain, and therefore, it was recommended that dedicated physical exercise be excluded from the activities in CST-PD.
Key recommendations
Include card/strategy games and constructive activities.
Exclude physical activity tasks.
Avoid disturbing images and abstract questions.
Theme 3: companion considerations
All parties were cautious when discussing the acceptability of the therapy for companions with a caregiving role. Professionals and companions acknowledged that dyads engaging in constructive discussion might be of benefit, but exhaustion and feelings of pressure of companions and family members could not be disregarded. Involving other family members (eg, grandchildren) was suggested in all focus groups. Participants felt that involving family members would be a pleasurable experience and would limit any burden that a dyadic therapy might introduce:
We are together all the time. Sometimes the relationship gets strained because you are at the end of it. So, I think my daughter could get my husband to do a lot more than I could. She could sit down with him and talk to him about things that he just says to me “Oh you are not listening”. So I think it is imperative to involve your immediate family. (Companion)
Companions communicated concerns about self-doubt and uncertainty in delivering the therapy, and all participants agreed advice should be provided on what to do in situations of confrontation. With respect to the current iCST manual, all participants felt that the introduction was too long and overly complicated, and suggested reducing it to a single page with 10 key points including a summary of what is in the manual, what support there is and how to find it. The importance of appropriate training was of interest to professionals and people with PRD, with professionals suggesting that companions read through materials in advance of the therapy session.
Key recommendations
Involve others (family members, grandchildren, friends).
Streamline the introduction.
Provide advice on managing challenging behavior.
Include strategies to build instructional efficacy.
Stage 3: test and refine
At the end of the design stage, a final draft CST-PD therapy manual was produced. This was subsequently field tested by dyads ie, people with PRD and companions (Part A). The purpose was to evaluate the therapy manual (in context) against the user requirements defined in Stage 2. Additional opinion was also sought from PPI representatives at a local Parkinson’s UK branch meeting to better understand if the intervention and delivery processes could work in a real world (Part B).Citation50
Part A (companions and people with PRD)
Methods
Participants
Companions (n=3) and people with PRD (n=3) participated in the field testing. Participants were recruited from local neurology and geriatric psychiatry services in Greater Manchester and had a diagnosis of either PD-MCI, PDD or DLB according to the appropriate consensus criteria for each condition.Citation42–Citation46
Procedure
The study received favorable ethical opinion from Yorkshire and the Humber–Bradford Leeds Research Ethics Committee (Reference: 15/YH/0531). Dyads completed a portion (2 weeks; ~6 sessions) of the program with support from the research team. At the end of the 2-week period, dyads completed a usability assessment and provided detailed qualitative feedback. The usability assessment was based on the 10-item System Usability Scale,Citation51,Citation52 which was adapted to suit the needs of this study and population (ie, the term “system” was replaced with “therapy manual” and additional questions relating to formatting, layout and so on were included). The adapted assessment consisted of 24 statements (eg, “I found the manual unnecessarily complex” and “I would imagine that most companions would learn to use the manual very quickly”) to which the participants provided free answers. Items were categorized with relevance to themes from the focus groups and interviews, and are discussed accordingly.
Results
Of the 24 items, 11 statements were grouped under Theme 1, “Manual form and content”, 9 under Theme 2, “Therapy acceptability in PD”, and 4 under Theme 3, “Companion considerations”.
Theme 1: manual form and content
All participants found the manual layout was consistent, the pages were easy to navigate, the topics were well-integrated with plenty of choice, and the size and color of the print was good. Participants reported they would appreciate additional materials consisting of games, adult coloring and stationary.
Theme 2: therapy acceptability in PD
All participants with PRD agreed that they would feel confident using the manual and would likely use it three times per week. The task complexity was perceived differently depending on the level of cognitive impairment; the participant with PD-MCI found the level of complexity appropriate, and the participant with PDD found the tasks challenging. The person with DLB found the manual, images and tasks challenging. The participant with DLB and their companion agreed that the manual was not suitable, with the companion attributing this to the advanced level of cognitive impairment of the participant.
Theme 3: companion considerations
Both participants with dementia, but not the participant with PD-MCI, were definitive that they would need support to use the manual. All companions agreed that they would be able to learn to use the manual quickly, although they felt it beneficial to have some preparation time before commencing use of the manual.
Key recommendations
Companion-training package should include preparation time.
Additional support may be required depending on the level of cognitive impairment.
Part B (PPI representatives)
Methods
Participants
Thirty-three PPI representatives (companions and people with PRD) from a local Parkinson’s UK community group took part.
Procedure
PPI representatives piloted the therapy questions and topic guides in a single group session held at a Parkinson’s UK support group. Attendees were given the option of completing a feedback form to comment on the usability and acceptability of the therapy. Four topics were randomly selected from the manual for use on the day: herbs, newspapers, Blackpool and ball games. A modified version of the in-house usability assessment, using a five-point Likert response scale (1= “strongly disagree” to 5= “strongly agree”), with one question reverse-scored, was circulated to gather feedback.
This phase of the study was carried out as a PPI session and, as such, ethical approval was not obtained to record opinion from the PD UK community group. Feedback was gathered anonymously and no further information (identifiable or otherwise) was collected about the volunteers.
Results
Sixteen volunteers elected to complete the feedback form. Responders strongly agreed that it was easy to engage in the session (median =5), to stimulate conversation using the topic materials (median =5), and that the discussion was stimulating and interesting (median =5). Responders also agreed that the session content (median =4.5) and images (median =4) were clear and easy to understand, that there was opportunity to personalize the session (median =4) and that they would like to do a similar activity in the future (median =4). Volunteers were uncertain about whether the level of complexity was suitable for someone with memory problems (median =3, “neither agree nor disagree”).
Key recommendation
In future evaluations, assess topic acceptability in people with moderate–severe cognitive impairment.
Discussion
This research adapted and tested a psychosocial therapy for people with PRD and their companions. A user-centered design was employed, and professionals, people with PRD, companions and researchers worked collaboratively to modify an existing therapy to meet specific user needs. The first step was to identify and review the evidence base for psychosocial therapies for people with PRD and the potential mechanisms of change. Subsequently, a candidate therapy for adaptation was selected. A basic prototype manual (loose pages and sample topic ideas) was developed early in the second phase to allow the proposed therapy to be discussed in a more meaningful way with stakeholders. The final version of the therapy manual was developed iteratively through a series of focus groups, interviews, a group demonstration and field testing.
An advantage of co-developing the intervention with stakeholders is that it limits the risk of missing critical therapeutic requirements and provides a positive and satisfying experience for the individuals involved (ie, the therapy meets the goals of its users because its users have been actively involved in the iterative development of the therapy). This aspect was particularly important for CST-PD, as the target population is frail, the symptoms complex and a therapy companion is required. As the specific needs of this population are not well understood, the design of the therapy could not be informed through literature only. Hence, we involved people with PRD, companions and health professionals as partners throughout the design process. Testament to CST-PD meeting the needs of people with PRD and their companions is the positive feedback received from the Parkinson’s UK field testing session. The comments indicated that the members engaged with the session and enjoyed the activities. Although speculative at this stage, these findings suggest the therapy might address the neuropsychiatric symptoms (eg, apathy and anxiety) associated with increased caregiver distress in PRD.Citation50 The successful delivery of the session in a group format also highlights the versatility of the adapted therapy and indicates that it may be appropriate for people with PRD attending group-based sessions.
This study has some limitations. The number of participants is small, and focus group methodology proved challenging for this companion and patient population, given their complex and changeable needs. The obstacles faced in bringing participants together for a focus group demonstrate how difficult it might be for companions and people with PRD to attend group CST sessions, and reinforce the appropriateness of developing a home-based therapy that can be carried out at the convenience of the people involved.
Conclusion
There is an urgent need to expand the management options for people with PRD beyond standard pharmacologic approaches. Psychosocial therapies suitable for this group of people may, therefore, have a vital role. The development phase of CST-PD was extensive and involved an iterative process comprising theory-driven recommendations, evaluation of users’ needs, prototype manual development and field testing. This aspect of the trial resulted in the production of CST-PD, a therapy manual specifically tailored for people with PRD and their companions. Following the MRC guidelines,Citation9 a pilot randomized clinical trial is currently underway to examine the feasibility, acceptability and tolerability of CST-PD and to explore the outcome measures.Citation53 The pilot data will be used to inform a subsequent, definitive, multisite randomized controlled trial.
Authors’ contributions
SAM and KRM prepared the manuscript. KRM and SV recruited participants, facilitated focus groups, conducted individual interviews and conducted the analysis of the data gathered. IL, VO, KRM, SAM, SV, EP and SS were involved in the conception and design of the CST-PD approach, the critical appraisal of the intellectual content, manuscript revisions and final approval prior to publication.
Acknowledgments
This article presents independent research supported and funded by the National Institute for Health Research, under the Research for Patient Benefit (RfPB) Program (competition number 22; grant number PB-PG-0613-31058). The views expressed in this article are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.
The authors would like to acknowledge and thank the original CST and iCST development team for permitting the adaptation of their therapy, the R&D personnel involved in study set-up and maintenance, and the NHS clinicians and nursing teams involved in referral of participants to the study. The authors would also like to thank the PPI representatives for their helpful advice and continued support at various stages of the project. The authors kindly acknowledge the contribution of Professor Martin Orrell, Dr Monty Silverdale and Dr Bo Fu in the conception and design of CST-PD.
Disclosure
The authors report no conflicts of interest in this work.
References
- The British Psychological Society and The Royal College of PsychiatristsDementia: A NICE–SCIE Guideline on supporting people with dementia and their carers in health and social care1st edLondonAldren Press2007
- AarslandDLarsenJPLimNGRange of neuropsychiatric disturbances in patients with Parkinson’s diseaseJ Neurol Neurosurg Psychiatry199967449249610486397
- WitjasTKaphanEAzulayJPNonmotor fluctuations in Parkinson’s disease: frequent and disablingNeurology200259340841312177375
- CahnDASullivanEVShearPKPfefferbaumAHeitGSilverbergGDifferential contributions of cognitive and motor component processes to physical and instrumental activities of daily living in Parkinson’s diseaseArchClin Neuropsychol1998137575583
- Pont-SunyerCHotterAGaigCThe onset of nonmotor symptoms in Parkinson’s disease (The ONSET PD Study)Mov Disord201530222923725449044
- AarslandDBronnickKWilliams-GrayCMild cognitive impairment in Parkinson disease. A multicenter pooled analysisNeurology201075121062106920855849
- HelyMAReidWGAdenaMAHallidayGMMorrisJGThe sydney multicenter study of Parkinson’s disease: the inevitability of dementia at 20 yearsMov Disord200823683784418307261
- BallardCGAarslandDMcKeithIFluctuations in attention: PD dementia vs DLB with parkinsonismNeurology200259111714172012473758
- CraigPDieppePMacintyreSMichieSNazarethIPetticrewMMedical Research Council GuidanceDeveloping and evaluating complex interventions: the new Medical Research Council guidanceBMJ2008337a165518824488
- OrgetaVMcDonaldKRPoliakoffEHindleJClareLLeroiICognitive training interventions for dementia and mild cognitive impairment in Parkinson’s diseaseCochran Database Syst Rev201511 Art. No. CD011961
- GoranssonBThe re-design of a PDA-based system for supporting people with Parkinson’s diseaseFincherSPanosMMooreDRuddleRPeople and Computers XVIII – Design for Life: Proceedings of HCI 2004LondonSpringer2005181196
- MaysNRobertsEPopayJSynthesizing research evidenceFulopNAllenPClarkeABlackNStudying the Organization and Delivery of Health Services: Research MethodsLondonRoutledge2001188220
- TaulbeeLRFolsomJCReality orientation for geriatric patientsHosp Community Psychiatry19661751331355932198
- NorrisAReminiscence With Elderly PeopleBicesterWinslow Press1986
- ButlerRNThe life review: an interpretation of reminiscence in the agedPsychiatry1963261657614017386
- WoodsBAguirreESpectorAEOrrellMCognitive stimulation to improve cognitive functioning in people with dementiaCochrane Database Syst Rev20122CD005562
- WoodsRTOrrellMBruceEREMCARE: pragmatic multi-centerrandomizedtrial of reminiscence groups for people with dementia and their family carers: effectiveness and economic analysisPLoS One2016114e015284327093052
- GuidelinesAPAPractice guideline for the treatment of patients with alzheimer’s disease and other dementias of late life. American Psychiatric AssociationAm J Psychiatry19971545 Suppl139
- SpectorAThorgrimsenLWoodsBEfficacy of an evidence-based cognitive stimulation therapy program for people with dementiaBr J Psychiatry200318324825412948999
- KnappMThorgrimsenLPatelACognitive stimulation therapy for people with dementia: cost-effectiveness analysisBr J Psychiatry2006188657458016738349
- OrrellMAguirreESpectorAMaintenance cognitive stimulation therapy for dementia: single-blind, multicentre, pragmatic randomized controlled trialBr J Psychiatry2014204645446124676963
- OrrellMSpectorAThorgrimsenLWoodsBA pilot study examining the effectiveness of maintenance cognitive stimulation therapy (MCST) for people with dementiaInt J Geriatr Psychiatry200520544645115852436
- LeungPYatesLOrgetaVHamidiFOrrellMThe experiences of people with dementia and their carers participating in individual cognitive stimulation therapyInt J Geriatr Psychiatry Epub2017220
- OrrellMYatesLLeungPThe impact of individual cognitive stimulation therapy (iCST) on cognition, quality of life, caregiver health, and family relationships in dementia: a randomized controlled trialPLoS Med2017143e100226928350796
- LeroiIMcDonaldKPantulaHHarbishettarVCognitive impairment in Parkinson disease: impact on quality of life, disability, and caregiver burdenJ Geriatr Psychiatry Neurol201225420821423172765
- FarzanaFSreekanthVMohiuddinMKMohanVBalakrishnaNAhujaYRCan individual home-based cognitive stimulation therapy benefit Parkinson’s patients with mild to moderate cognitive impairment?Int J Geriatr Psychiatry201530443343525754020
- NasreddineZSPhillipsNABédirianVThe montreal cognitive assessment, MoCA: a brief screening tool for mild cognitive impairmentJ Am Geriatr Soc200553469569915817019
- JenkinsonCFitzpatrickRPetoVGreenhallRHymanNThe Parkinson’s diisease questionnaire (PDQ-39): development and validation of a Parkinson’s disease summary index scoreAge Ageing19972653533579351479
- ThorgrimsenLSelwoodASpectorAWhose quality of life is it anyway?: the validity and reliability of the quality of life-alzheimer’s disease (QoL-AD) scaleAlzheimer Dis Assoc Disord200317420120814657783
- CraigPDieppePMacintyreSMichieSNazarethIPetticrewMDeveloping and evaluating complex interventions: The new Medical Research Council guidanceInt J Nurs Stud201350558759223159157
- AngelucciFPeppeACarlesimoGAA pilot study on the effect of cognitive training on BDNF serum levels in individuals with Parkinson’s diseaseFront Hum Neurosci2015913025852518
- FarzanaFAhujaYRSreekanthVNon-pharmacological interventions for enhancing brain plasticity and promoting brain recovery: a reviewRes Neurosci2013233949
- ClareLWoodsRTCognitive training and cognitive rehabilitation for people with early-stage alzheimer’s disease: a reviewNeuropsychol Rehabil2004144385401
- SimpsonJMcMillanHReeveDReformulating psychological difficulties in people with Parkinson’s disease: the potential of a social relational approach to disablismParkinsons Dis2013201360856224000316
- ReeveDTowards a psychology of disability:the emotional effects of living in a disabled societyGoodleyDLawthornRDisability and Psychology: Critical Introductions and ReflectionsBasingstoke, UKMacmillan200694107
- SchragAHovrisAMorleyDQuinnNJahanshahiMYoung-versus older-onset Parkinson’s disease: impact of disease and psychosocial consequencesMov Disord200318111250125614639664
- JoachimGAcornSStigma of visible and invisible chronic conditionsJ Adv Nurs200032124324810886457
- SindhiALeroiINonpharmacological therapies for cognitive enhancement in Parkinson’s disease: applying old interventions in a new setting?Neurodegener Dis Manag201336539547
- BrownRJahanshahiMDepression in Parkinson’s disease: a psychosocial viewpointAdv Neurol19956561847872153
- BanduraAPerceived self-efficacy in cognitive development and functioningEduc Psychol1993282117148
- GibsonSDemboMHTeacher efficacy: a construct validationJ Educ Psychol1984764569
- HughesAJDanielSEKilfordLLeesAJAccuracy of clinical diagnosis of idiopathic Parkinson’s disease: a clinico-pathological study of 100 casesJ Neurol Neurosurg Psychiatry19925531811841564476
- EmreMAarslandDBrownRClinical diagnostic criteria for dementia associated with Parkinson’s diseaseMov Disord2007221216891707 quiz 183717542011
- DuboisBBurnDGoetzCDiagnostic procedures for Parkinson’s disease dementia: recommendations from the movement disorder society task forceMov Disord200722162314232418098298
- McKeithIGDicksonDWLoweJDiagnosis and management of dementia with lewy bodies – third report of the DLB consortiumNeurology200565121863187216237129
- LitvanIGoldmanJGTrosterAIDiagnostic criteria for mild cognitive impairment in Parkinson’s disease: Movement Disorder Society Task Force guidelinesMov Disord201227334935622275317
- KruegerRACaseyMAFocus Groups:A Practical Guide for Applied Research4th edLondonSAGE2009
- BamfordCBruceESuccesses and challenges in using focus groups with older people with dementiaWilkinsonHThe Perspectives of People With Dementia:Research Methods and MotivationsLondonJessica Kingsley2002139164
- TongASainsburyPCraigJConsolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groupsInt J Qual Health Care200719634935717872937
- O’CathainAThomasKJDrabbleSJRudolphAGoodeJHewisonJMaximizing the value of combining qualitative research and randomized controlled trials in health research: the QUAlitative Research in Trials (QUART) studya mixed methods studyHealth Technol Assess201418381197vvi
- SauroJMeasuring Usability With The System Usability Scale (SUS)2011 Available from: http://www.measuringu.com/sus.phpAccessed February 1, 2016
- BrookeJSUS-A quick and dirty usability scaleUsability Evaluation in Industry199618919447
- McCormickSAMcDonaldKRVatterSPsychosocial therapy for Parkinson’s-related dementia: study protocol for the INVEST randomised controlled trialBMJ Open201776e016801