
Abstract
Purpose
Cough on anesthetic emergence should be prevented considering its dangerous complications. Target-controlled infusion (TCI) of remifentanil can reduce emergence cough effectively, and sex-related differences in effect-site concentration (Ce) of remifentanil have been evaluated in young patients. In this study, we determined the Ce of remifentanil for preventing emergence cough following extubation in male and female elderly patients and evaluated the sex-related difference.
Patients and methods
Twenty-three male and 22 female elderly patients aged between 60 and 75 years were enrolled. Anesthesia was maintained with sevoflurane and remifentanil TCI. The Ce of remifentanil for preventing emergence cough was determined for each sex using isotonic regression method with a bootstrapping approach, following Dixon’s up-and-down method.
Results
The Ce of remifentanil for preventing emergence cough in 50% (EC50) and 95% (EC95) of the population was significantly lower in females than in males. Isotonic regression revealed the EC50 (83% confidence interval [CI]) of remifentanil was 1.67 (1.55–1.83) ng/mL in females and 2.60 (2.29–2.91) ng/mL in males. The EC95 (95% CI) of remifentanil was 2.30 (2.02–2.62) ng/mL in females and 3.41 (3.27–3.58) ng/mL in males. Dixon’s up-and-down method indicated that the mean EC50 in females was lower than in males (1.56±0.26 ng/mL vs 2.56±0.37 ng/mL, P<0.001).
Conclusion
The remifentanil requirement for preventing emergence cough was lower in female than in male elderly patients, indicative of sex-related differences in Ce of remifentanil. Sex should be considered when using remifentanil TCI for preventing emergence cough in elderly patients.
Introduction
Coughing on emergence from general anesthesia is common,Citation1 particularly when an endotracheal tube is utilized. Coughing at extubation may result in serious complications including laryngospasm, negative-pressure pulmonary edema, arterial hypertension, arrhythmia, bleeding, and wound disruption. Based on the American Society of Anesthesiologists recommendation of preformulated strategy for extubation by the anesthesiologist,Citation2 a variety of techniques have been tried to reduce emergence cough including long-acting opioids, lidocaine, dexmedetomidine, and deep extubation.Citation3–Citation6 These may be beneficial, but can delay emergence.
Remifentanil is a potent ultrashort-acting opioid,Citation7 with rapid onset and offset of drug effect. Moreover, it is affected minimally by extremes of age or renal or hepatic dysfunction. Remifentanil allows rapid anesthetic emergence even after a prolonged infusion and decreases the at-risk time during extubation. In addition, cough suppression of remifentanil enables smooth extubation with reduced complications.Citation8,Citation9 Low-dose infusion than bolus dose of remifentanil was determined to decrease the emergence cough;Citation10,Citation11 hence, target-controlled infusion (TCI) has been used to customize infusion rate for individual patients, which maintains a desired target concentration by using pharmacokinetic model.Citation12 To date, several studies have examined the optimal effect-site concentration (Ce) of remifentanil for preventing emergence cough following extubation.Citation13–Citation21
Human studies have indicated that opioid has quantitative and qualitative differences in effect in male and female patients.Citation22–Citation25 Nevertheless, most studies regarding Ce of remifentanil for preventing emergence cough have neglected sex-related difference, except for one study.Citation20 Soh et al reported the occurrence of sex-related differences in the Ce of remifentanil for suppressing emergence cough among young patients aged 20–46 years.Citation20 Although there are little studies regarding differential effect of remifentanil based on sex,Citation26 it may be postulated that the difference is due to the higher mu-opioid receptor availability in females than in males. However, the elderly patient population shows a rapid rise, with 4 times higher surgery rates than young patients.Citation27 High comorbidities of elderly patients may lead to detrimental hemodynamic changes on emergence cough, despite age-related decline of cough reflex.Citation28 In addition, elderly patients have different opioid sensitivity, as compared to young patients.Citation25,Citation29 Thus, there is a need to determine the Ce of remifentanil for smooth extubation in each sex of elderly patients. We hypothesized that there may exist sex-related differences in the Ce of remifentanil for suppressing cough during anesthetic emergence among elderly patients and that male elderly patients may require higher Ce of remifentanil for emergence cough suppression than female elderly patients.
The purpose of this study was to investigate the Ce of remifentanil for preventing emergence cough following extubation during general anesthesia among elderly patients and to evaluate possible sex-based differences.
Patients and methods
This study was approved by Ajou University Hospital Institutional Review Board (protocol number: AJIRB-MED-CT4-15-55, April 16, 2015) and was registered at http://cris.nih.go.kr (registration number: KCT001910). All data were set and collected in Ajou University School of Medicine. The data collection was performed from September 2015 to June 2016. Twenty-three male and 22 female geriatric patients aged between 60 and 75 years with an ASA physical status I–II who underwent general anesthesia for laparoscopic cholecystectomy were included. Patients were excluded if any of the following criteria were present: Mallampati class 3 or 4, history of difficult intubation or respiratory disease, upper respiratory infection in previous 2 weeks, gastroesophageal reflux disease, uncontrolled hypertension and diabetes mellitus, smoking habit, and body mass index (BMI) >30 kg/m2. Female patients on hormone treatment were also excluded. Written informed consent was obtained from all patients.
All patients were not premedicated. On arrival at the operating room, electrocardiogram, pulse oxygen saturation, noninvasive arterial pressure, end-tidal carbon dioxide (EtCO2), and bispectral index (BIS™ Quatro Sensor; Covidien, Dublin, Ireland) were monitored. Anesthesia was induced with 4–5 mg/kg of thiopental sodium and 1–5 ng/mL target concentration of remifentanil (Ultiva; GlaxoSmithKline, Brentford, UK) using TCI for all patients. TCI of remifentanil was administered with a commercial total intravenous (IV) anesthesia pump (Orchestra® Base Primea; Fresenius Kabi, Bad Homburg, Germany) based on the pharmacokinetic model of Minto et al.Citation30 On absence of response to a verbal or eye stimulus, rocuronium 0.6 mg/kg was administered intravenously. Orotracheal intubation was performed in all patients using a 7.0 mm (internal diameter) tracheal tube for females and an 8.0 mm (internal diameter) tracheal tube for males. Cuff pressure was maintained at 20–25 cm H2O using a hand pressure gauge (Hi-Lo™ Hand Pressure Gauge; VBM Medizintechnik GmbH, Sulz am Neckar, Germany).
Anesthesia was maintained with 1.5–2.5 vol% sevoflurane and a remifentanil Ce of 1–5 ng/mL to maintain a BIS value of 40–55, mean arterial pressure (MAP), and heart rate (HR) within 20% of baseline. Mechanical ventilation was maintained with a tidal volume of 8 mL/kg, air/oxygen mixture (FiO2: 0.5, 3 L/min), and EtCO2 at 35–40 mmHg.
At the time of skin suture, sevoflurane was adjusted to an approximate BIS level of 60, and the Ce of remifentanil was titrated to a predetermined concentration. The Ce was maintained for at least 15 min throughout emergence. At the end of surgery, sevoflurane was discontinued, and fresh gas flow was increased up to 10 L/min. Postoperative analgesics and antiemetics included IV ketorolac 30 mg and ramosetron 0.3 mg, respectively, and IV Bridion® (sugammadex) 3 mg/kg was administered for reversal of neuromuscular block, which was reconfirmed as a train-of-4 ratio >90% using nerve stimulator. Manual ventilation was initiated with maintaining EtCO2 of 35–40 mmHg. During this phase, the patients were not stimulated, except for a verbal request to open their eyes. The tracheal tube was extubated on confirming that the patients showed opening of eyes and spontaneous respiration with an adequate tidal volume and respiratory rate. Subsequently, remifentanil infusion was stopped, and oxygen was supplemented via a facemask for at least 3 min. Extubation was performed by a single anesthesiologist with considerable experience with intubation.
Emergence cough was defined as the cough developed during the period of discontinuing sevoflurane and 3 min after extubation. Hemodynamic data, such as HR and MAP, were recorded at baseline (before induction, T0), end of operation (T1), just before extubation (T2), just after extubation (T3), and 3 min after extubation (T4). Bradycardia (HR <40 bpm) and hypotension (MAP <60 mmHg) were treated with IV atropine 0.5 mg and ephedrine at 4 mg, respectively. The sevoflurane concentration at the time of eye opening was recorded. Time to extubation was defined as the time from discontinuing sevoflurane until extubation. Complications such as bradypnea (respiratory rate <8 bpm), laryngospasm, and desaturation (SpO2 <95% despite oxygen supplementation) were evaluated throughout the emergence period. Sedation score was assessed for each patient on arrival at the recovery room. In addition, overall pain score was evaluated. Pain intensity was evaluated using an 11-point numerical rating scale (NRS; 0= no pain and 10= worst pain). Fentanyl 0.5 μg/kg was administered intravenously in patients who reported an NRS score ≥5.
For estimation of the remifentanil Ce, the up-and-down sequential allocation design was used. The initial Ce of remifentanil was 2 ng/mL for the first patient of each sex, and for the subsequent patient, the predetermined Ce of remifentanil was based on the cough response of the previous patient. If the patient did not cough throughout the peri-extubation period, it was considered as “success”, and the predetermined Ce of remifentanil for the subsequent patient was decreased by 0.5 ng/mL. If the patient coughed at any time before, during, or after extubation, it was considered as “failure”, and the predetermined Ce was increased by 0.5 ng/mL.
Statistics
The primary end point of this study was to investigate the effective concentration of remifentanil in 50% of the population (EC50) and 95% of population (EC95) for preventing emergence cough following extubation in patients aged 60–75 years in each sex. Since females show different sensitivity to opioid than males,Citation25 we hypothesized that there is a sex difference in the Ce of remifentanil for preventing emergence cough.
Based on previous studies in which the EC50 was estimated by the Dixon’s method,Citation20 the stopping rule requires at least 6 success/failure pairs in the same direction. Simulation studies for the up-and-down design suggest that at least 20 patients should be included to obtain stable estimates.Citation31 In our study, 23 and 22 patients were included in male and female groups, respectively, and so there were sufficient numbers to satisfy all requirements.
The EC50 of remifentanil by Dixon’s up-and-down method was defined as the mean value of mid-point dose of the independent crossover pairs for each sex (ie, success to failure), and the mean EC50 values of each sex were compared using independent t-test. To specify the precision of the target concentration, the isotonic regression method was also used to estimate the EC50 and the EC95 of remifentanil along with the confidence interval (CI). From the observed response rate, which presents the ratio of the number of successful patients to the number of subjects at each concentration, an adjusted response probability was calculated by a pooled-adjacent-violators algorithm (PAVA) in order to adhere to the assumption that the drug effect increases with increased dosage. The CI was estimated by a bootstrapping approach.Citation31 If the EC50 and EC95 values did not overlap at the level of the 83% and 95% CIs, respectively, the null hypothesis of equal effective concentrations was rejected at an α of 0.05.Citation31,Citation32
All values were expressed as the mean ± standard deviation (SD), the median (range), or the number of patients. The analysis between sexes was performed using an independent t-test (height, weight, BMI, anesthesia time, time to extubation), Mann–Whitney U test (age, operation time, sevoflurane vol% at eye opening, and NRS), Chi-squared test (ASA physical status and fentanyl administration), or Fisher’s exact test (respiratory complications and sedation score). Repeated-measures variables (MAP and HR) were analyzed using repeated-measures ANOVA with the Bonferroni correction. A P-value of <0.05 was considered statistically significant. Statistical analyses were performed using the Statistical Package for Social Sciences (version 23.0 for Windows; IBM Corporation, Armonk, NY, USA) and R for Windows (version 3.2.5; The R foundation for Statistical Computing).
Results
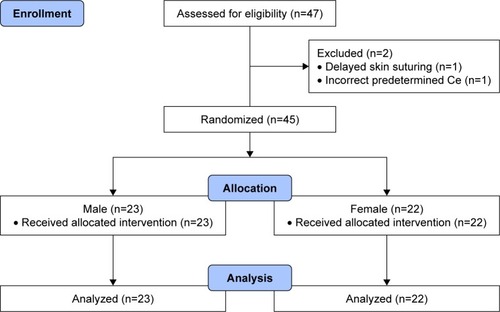
Among the enrolled 47 patients, 2 male patients were excluded due to delayed skin suturing and an incorrect predetermined Ce of remifentanil, and 23 male and 22 female patients were included in the final analysis (). Patient characteristics and operation details are summarized in . Due to sex-related differences, height and weight were significantly lower in females than in males, but BMI showed no significant difference.
Table 1 Patients characteristics and operation details
Figure 1 Consort diagram.
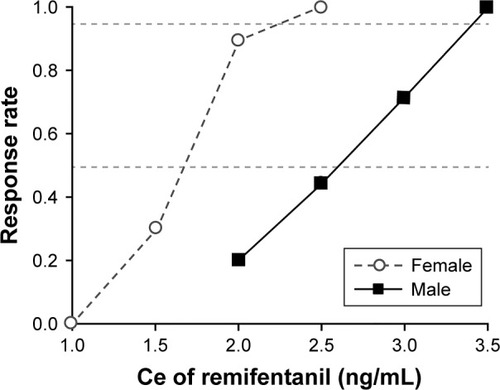
The sequence of successes and failures determined by Dixon’s up-and-down method is shown in , and the isotonic regression calculated using the PAVA is shown in . The EC50 and EC95 of remifentanil Ce for preventing emergence cough calculated by Dixon’s method or isotonic regression are presented in . The EC50 of remifentanil Ce estimated by Dixon’s method was lower in females than in males (mean ± SD 1.56±0.26 vs 2.56±0.37 ng/mL; P<0.001). The EC50 (83% CI) of remifentanil Ce estimated by isotonic regression was 1.67 (1.55–1.83) ng/mL in females and 2.60 (2.29–2.91) ng/mL in males. The EC95 (95% CI) of remifentanil Ce estimated by isotonic regression was 2.30 (2.02–2.62) ng/mL in females and 3.41 (3.27–3.58) ng/mL in males. As the EC50 and EC95 values did not overlap at the level of the 83% and 95% CIs, respectively, the Ce of remifentanil for preventing emergence cough was significantly lower in females than in males.
Table 2 Ce of remifentanil for preventing emergence cough following extubation
Figure 2 Assessment of success or failure at preventing emergence cough following extubation under the predetermined remifentanil Ce in consecutive patients determined by Dixon’s up-and-down methods.
Notes: The mean EC50 of remifentanil Ce for preventing emergence cough was calculated from crossover pairs of successes (filled circles) and failures (open circles) in (A) 23 male patients and (B) 22 female patients. The mean ± standard deviation EC50 values of remifentanil Ce values were 2.56±0.37 ng/mL in males and 1.56±0.26 ng/mL in females. EC50 is defined as effective concentration for preventing emergence cough following extubation in 50% of patients.
Abbreviation: Ce, effect-site concentration.
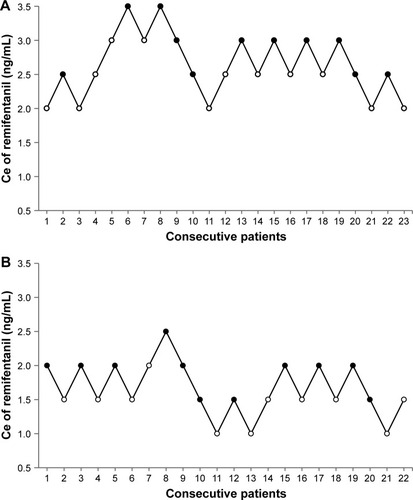
Figure 3 Pooled-adjacent-violators algorithm response rates in females (open circles) and in males (filled circles).
Abbreviations: Ce, effect-site concentration; CI, confidence interval.
Emergence and recovery profiles are summarized in . Among respiratory complications, bradypnea was observed in 4 female patients, of which remifentanil Ce was 1, 1.5, 2, and 2 ng/mL. Desaturation was developed in 1 female patient with remifentanil Ce of 1.5 ng/mL. Patients returned to a normal respiratory pattern immediately just by encouragement of deep breathing via facial mask without ventilatory support.
Table 3 Emergence and recovery profiles
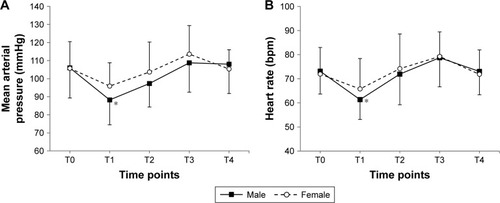
MAP and HR during anesthetic emergence and tracheal extubation are shown in . MAP showed no significant difference between sexes (, P=0.271), but MAP in males was significantly lower at the end of operation (T1), as compared with baseline (T0) value (P=0.001). Similarly, there were no significant differences between sexes in HR (, P=0.723), and HR in males was lower at the end of operation (T1), as compared with baseline (T0) value (P<0.001).
Figure 4 The (A) mean arterial pressure and (B) heart rate during emergence of anesthesia and tracheal extubation.
Discussion
In the present study, we implemented balanced anesthesia with sevoflurane and remifentanil TCI in elderly patients undergoing laparoscopic cholecystectomy in order to find the Ce of remifentanil in each sex for smooth extubation during anesthetic emergence. The results indicated that the remifentanil requirement for preventing emergence cough in elderly patients was lower in female subjects (EC50: 1.67 ng/mL) than in male subjects (EC50: 2.60 ng/mL), indicative of sex-related differences.
Cough reflex is mediated by dual-sensory neuron (nociceptor and mechanoreceptor) around trachea and brainstem processing of afferent information.Citation33 While anesthesia affects subcortical processing and regulates a voluntary cough, opioid acts at both brain stem and peripheral nociceptor and reduces a reflexive cough.Citation33 Among opioids for general anesthesia, remifentanil is commonly administered as infusion throughout the anesthesia. It is associated with deeper intraoperative analgesia and anesthesia, faster postoperative recovery, and less respiratory depression compared with short-acting opioids (fentanyl, alfentanil, or sufentanil).Citation34 In addition, remifentanil infusion on anesthetic emergence decreases the emergence cough following extubation.Citation7 Several previous studies, with differing types of surgery and combined anesthetics, have demonstrated reduced severity and incidence of anesthetic emergence cough,Citation14–Citation16,Citation19 or optimal Ce values of remifentanil for preventing emergence cough,Citation13,Citation18,Citation21 with the use of remifentanil TCI. However, most of these studies neglected sex-related differences regarding Ce of remifentanil. Recently, Soh et al reported the Ce of remifentanil for preventing emergence cough in male (EC50: 2.57 ng/mL) and in female (EC50: 1.30 ng/mL) young patients (aged 20–46 years) and existence of sex-related differences.Citation20 To our best knowledge, there has been no report showing sex-related difference in the Ce of remifentanil for preventing emergence cough in elderly patients.
The main result of our study was the sex-related difference in Ce of remifentanil for preventing emergence cough among elderly patients. The sex-related differences in opioid effect may not be restricted to the pain, but have a same direction with other effects such as emesis, respiratory depression, and cough suppression, since they stem from an inherent property of the endogenous opioid receptor system.Citation24 However, sex-related differences in opioid efficacy in elderly patients in prevention of emergence cough remain unclear.
Female elderly patients required lower Ce of remifentanil for preventing emergence cough compared to male elderly patients in the present study. Generally, gender is a significant factor influencing opioid requirement during postoperative period,Citation24,Citation25,Citation35 although the direction of sex-related differences in opioid efficacy is less clear in human studies because of many interacting variables.Citation23 First, sex-related differences in opioid efficacy may contribute to sex-related differences in basal pain perception. There is greater deactivation in pain-related brain regions among females.Citation36 Second, it could result from sex-related differences in sensitivity to opioid. Females differ from males in terms of distribution, expression, or sensitivity of opioid receptors in brain.Citation25 Third, it could be partially mediated by interaction between gonadal hormones and the opioid system.Citation25 Gonadectomy reduces analgesia in males but increases analgesia in females in vivo.Citation37 In a clinical study, Chia et al investigated the influence of age on the requirements for postoperative morphine in approximately 2,300 patients and revealed greater opioid consumption in males than in females.Citation35 This indicates a greater opioid efficacy in female patients.Citation37
The sex-related differences in opioid efficacy are confirmed in young patients, but conflicting in elderly patients.Citation25,Citation38 Clinically, Ce of remifentanil at loss of response to painful stimulus in elderly patients was similar to that in young patients during anesthetic induction.Citation39 In addition, young patients exhibited sex-related differences for postoperative pain and morphine requirement in postanesthesia care unit, but no differences were observed in elderly patients (aged ≥75 years).Citation40 These modulations by aging may be due to the influence of gonadal steroid hormone sensitivity to opioid analgesia.Citation41 In contrast, a meta-analysis concluded persistence of sex-related differences in opioid efficacy among elderly patients, suggesting that pain circuitry of humans is less regulated by sex hormones compared with animals.Citation24 In the present study, elderly patients exhibited sex-related differences in Ce of remifentanil for preventing emergence cough.
There was no great discrepancy in Ce value of remifentanil for preventing emergence cough between elderly patients in the present study and young patients in the previous study.Citation20 Although it is hard to compare between 2 studies because of different conditions including types of surgery, several possibilities may explain the phenomenon. First, elderly patients do not feel less pain than young patients, although the relationship between aging and postoperative pain has not yet been confirmed.Citation38 In Yang et al’s study, remifentanil requirement at loss of response for electrical stimulus using a peripheral nerve stimulator was similar between elderly and young patients.Citation39 Elderly patients tend to have lower pain score and demand less opioid than young patients, despite similar pain intensity.Citation42 Second, the patients in Gerbershagen et al’s and present studies underwent different types of surgery: thyroidectomy and laparoscopic cholecystectomy. Different conditions could require different doses of opioid for the desired effect, even though pain intensities of the surgeries are similar (NRS, 4 [3–6] vs 5 [3–6] in thyroidectomy and laparoscopic cholecystectomy).Citation43
There are some limitations in this study. First, all single cough were considered as “failure” regardless of the severity in this study. But minimal episode of single cough could have been considered as “success” because the single cough may have no clinical impact on practice or the patients. Second, TCI for remifentanil is performed using pharmacokinetic model of Minto et al, which takes into account co-variables such as age and lean body mass (using height and weight). In 1997, Minto et alCitation30 demonstrated that gender has no influence on the pharmacological model. However, the formula for lean body mass used different constants between genders. In addition, the sex-related differences in opioid effect have been raised after then, and there have been some trials about the different effect of remifentanil base on sex.Citation20,Citation26,Citation44
Conclusion
The Ce of remifentanil for preventing emergence cough following extubation was lower in female than in male patients, indicative of sex-related differences in optimal Ce of remifentanil in elderly patients. Sex should be considered when using remifentanil TCI for prevention of emergence cough in elderly patients.
Author contributions
SYL conceived and designed the experiments, performed the experiments, and wrote the paper. YYJ and BHL contributed to perform the experiments. JEK performed the experiments and wrote the paper. All authors contributed toward data analysis and drafting and critically revising the paper, and agree to be accountable for all aspects of the work.
Acknowledgments
This study was presented as a scientific poster at the 2017 Annual Meeting of Euroanesthesia on June 3, 2017, in Switzerland, Geneva.
Disclosure
The authors report no conflicts of interest in this work.
References
- KimESBishopMJCough during emergence from isoflurane anesthesiaAnesth Analg1998875117011749806703
- American Society of Anesthesiologists Task Force on Management of the Difficult AirwayPractice guidelines for management of the difficult airway: an updated report by the American Society of Anesthesiologists Task Force on Management of the Difficult AirwayAnesthesiology20039851269127712717151
- LeeJYLimBGParkHYKimNSSufentanil infusion before extubation suppresses coughing on emergence without delaying extubation time and reduces postoperative analgesic requirement without increasing nausea and vomiting after desflurane anesthesiaKorean J Anesthesiol201262651251722778885
- LeeJHKooBNJeongJJKimHSLeeJRDifferential effects of lidocaine and remifentanil on response to the tracheal tube during emergence from general anaesthesiaBr J Anaesth2011106341041521205628
- von Ungern-SternbergBSDaviesKHegartyMErbTOHabreWThe effect of deep vs. awake extubation on respiratory complications in high-risk children undergoing adenotonsillectomy: a randomised controlled trialEur J Anaesthesiol201330952953623344124
- LeeJSChoiSHKangYRKimYShimYHEfficacy of a single dose of dexmedetomidine for cough suppression during anesthetic emergence: a randomized controlled trialCan J Anaesth201562439239825523837
- BeersRCamporesiERemifentanil update: clinical science and utilityCNS Drugs200418151085110415581380
- TwerskyRSJamersonBWarnerDSFleisherLAHogueSHemodynamics and emergence profile of remifentanil versus fentanyl prospectively compared in a large population of surgical patientsJ Clin Anesth200113640741611578883
- MandelJEConsiderations for the use of short-acting opioids in general anesthesiaJ Clin Anesth2014261 SupplS1S724485553
- AouadMTAl-AlamiAANasrVGSoukiFGZbeidyRASiddik-SayyidSMThe effect of low-dose remifentanil on responses to the endotracheal tube during emergence from general anesthesiaAnesth Analg200910841157116019299779
- ShajarMAThompsonJPHallAPLeslieNAFoxAJEffect of a remifentanil bolus dose on the cardiovascular response to emergence from anaesthesia and tracheal extubationBr J Anaesth199983465465610673886
- AlbrechtSHeringWSchuttlerJSchwildenHNeue intravenöse Anästhetika Remifentanil, S(+)-Ketamin, Eltanolon und Target Controlled Infusion [New intravenous anesthetics. Remifentanil, S(+)-ketamine, eltanolone and target controlled infusion]Anaesthesist1996451211291141 German [with English abstract]9065246
- LeeBLeeJRNaSTargeting smooth emergence: the effect site concentration of remifentanil for preventing cough during emergence during propofol-remifentanil anaesthesia for thyroid surgeryBr J Anaesth2009102677577819411668
- ChenJLiWWangDHuXThe effect of remifentanil on cough suppression after endoscopic sinus surgery: a randomized studyActa Anaesthesiol Scand201054101197120321069899
- JunNHLeeJWSongJWKohJCParkWSShimYHOptimal effect-site concentration of remifentanil for preventing cough during emergence from sevoflurane-remifentanil anaesthesiaAnaesthesia201065993093520645945
- LimJHRyuSJLimYSThe incidence of cough induced by remifentanil during anesthetic induction was decreased by graded escalation of the remifentanil concentrationKorean J Anesthesiol201058211712120498788
- ChoiEMParkWKChoiSHSohSLeeJRSmooth emergence in men undergoing nasal surgery: the effect site concentration of remifentanil for preventing cough after sevoflurane-balanced anaesthesiaActa Anaesthesiol Scand201256449850322220983
- ChoHBKimJYKimDHKimDWChaeYJComparison of the optimal effect-site concentrations of remifentanil for preventing cough during emergence from desflurane or sevoflurane anaesthesiaJ Int Med Res201240117418322429357
- ChangCHLeeJWChoiJRShimYHEffect-site concentration of remifentanil to prevent cough after laryngomicrosurgeryLaryngoscope2013123123105310923686891
- SohSParkWKKangSWLeeBRLeeJRSex differences in remifentanil requirements for preventing cough during anesthetic emergenceYonsei Med J201455380781424719152
- YooJYKimJYKwakHJEffect-site concentration of remifentanil for preventing cough during emergence in elderly patients undergoing nasal surgery: a comparison with adult patientsClin Interv Aging2016111247125227672319
- CraftRMSex differences in opioid analgesia: “from mouse to man”Clin J Pain200319317518612792556
- DahanAKestBWaxmanARSartonESex-specific responses to opiates: animal and human studiesAnesth Analg20081071839518635471
- NiestersMDahanAKestBDo sex differences exist in opioid analgesia? A systematic review and meta-analysis of human experimental and clinical studiesPain20101511616820692097
- FillingimRBKingCDRibeiro-DasilvaMCRahim-WilliamsBRileyJL3rdSex, gender, and pain: a review of recent clinical and experimental findingsJ Pain200910544748519411059
- ParkSJParkHJChoiJYKangHSChoiHSThe influence of age and gender on remifentanil EC(50) for preventing rocuronium induced withdrawal movementsKorean J Anesthesiol201058324424820498772
- AubrunFMarmionFThe elderly patient and postoperative pain treatmentBest Pract Res Clin Anaesthesiol200721110912717489223
- EbiharaSEbiharaTKohzukiMEffect of aging on cough and swallowing reflexes: implications for preventing aspiration pneumoniaLung20121901293322033612
- BowieMWSlattumPWPharmacodynamics in older adults: a reviewAm J Geriatr Pharmacother20075326330317996666
- MintoCFSchniderTWEganTDInfluence of age and gender on the pharmacokinetics and pharmacodynamics of remifentanil. I. Model developmentAnesthesiology199786110239009935
- PaceNLStylianouMPAdvances in and limitations of up-and-down methodology: a precis of clinical use, study design, and dose estimation in anesthesia researchAnesthesiology2007107114415217585226
- PaytonMEGreenstoneMHSchenkerNOverlapping confidence intervals or standard error intervals: what do they mean in terms of statistical significance?J Insect Sci200333415841249
- CanningBJChangABBolserDCSmithJAMazzoneSBMcGarveyLCHEST Expert Cough PanelAnatomy and neurophysiology of cough: CHEST Guideline and Expert Panel reportChest201414661633164825188530
- KomatsuRTuranAMOrhan-SungurMMcGuireJRadkeOCApfelCCRemifentanil for general anaesthesia: a systematic reviewAnaesthesia200762121266128017991265
- ChiaYYChowLHHungCCLiuKGerLPWangPNGender and pain upon movement are associated with the requirements for postoperative patient-controlled iv analgesia: a prospective survey of 2,298 Chinese patientsCan J Anaesth200249324925511861342
- HendersonLAGandeviaSCMacefieldVGGender differences in brain activity evoked by muscle and cutaneous pain: a retrospective study of single-trial fMRI dataNeuroimage20083941867187618069004
- BodnarRJKestBSex differences in opioid analgesia, hyperalgesia, tolerance and withdrawal: central mechanisms of action and roles of gonadal hormonesHorm Behav2010581728119786031
- Wilder-SmithOHOpioid use in the elderlyEur J Pain20059213714015737802
- YangNZuoMZYueYWangYShiYZhangXNComparison of C50 for propofol-remifentanil target-controlled infusion and bispectral index at loss of consciousness and response to painful stimulus in elderly and young patientsChin Med J (Engl)2015128151994199926228208
- AubrunFSalviNCoriatPRiouBSex- and age-related differences in morphine requirements for postoperative pain reliefAnesthesiology2005103115616015983468
- AloisiAMGonadal hormones and sex differences in pain reactivityClin J Pain200319316817412792555
- GaglieseLWeizblitNEllisWChanVWThe measurement of postoperative pain: a comparison of intensity scales in younger and older surgical patientsPain2005117341242016153776
- GerbershagenHJAduckathilSvan WijckAJPeelenLMKalkmanCJMeissnerWPain intensity on the first day after surgery: a prospective cohort study comparing 179 surgical proceduresAnesthesiology2013118493494423392233
- KimSYSongMKKimMSKimEHHanDWSex-related differences in the effect-site concentration of remifentanil for preventing QTc interval prolongation following intubation in elderly patients with a normal QTc intervalDrugs Aging201431969570224989629