
Abstract
Background
The objective of this review was to obtain an overview of the technologies that have been explored with older adults with mild cognitive impairment and dementia (MCI/D), current knowledge on the usability and acceptability of such technologies, and how people with MCI/D and their family carers (FCs) were involved in these studies.
Materials and methods
Primary studies published between 2007 and 2017 that explored the use of technologies for community-dwelling people with MCI/D were identified through five databases: MEDLINE, PsycINFO, Embase, AMED, and CINAHL. Twenty-nine out of 359 papers met the criteria for eligibility. We used the Mixed Methods Appraisal Tool for quality assessment.
Results
A wide range of technologies was presented in the 29 studies, sorted into four domains: 1) safe walking indoors and outdoors; 2) safe living; 3) independent living; and 4) entertainment and social communication. The current state of knowledge regarding usability and acceptability reveals that even if researchers are aware of these concepts and intend to measure usability and acceptability, they seem difficult to assess. Terms such as “user friendliness” and “acceptance” were used frequently. User participation in the 29 studies was high. Persons with MCI/D, FCs, and staff/other older adults were involved in focus groups, workshops, and interviews as part of the preimplementation process.
Conclusion
Research regarding technologies to support people with MCI/D seems optimistic, and a wide range of technologies has been evaluated in homes with people with MCI/D and their FCs. A major finding was the importance of including people with MCI/D and their FCs in research, in order to learn about required design features to enhance usability and acceptability. Surprisingly, very few studies reported on the consequences of technology use with regard to quality of life, occupational performance, or human dignity.
Introduction
The aging society is described as a grand societal challenge,Citation1 and access to technology is one important strategy in future health-care services.Citation2 Older people often have multiple and chronic diseases, often requiring extensive care services. The prevalence of Alzheimer’s disease or related dementias extends to nearly 44 million people worldwide and is most common in Western Europe.Citation3 Dementia is a neurodegenerative condition due to disease of the brain, of a chronic or progressive nature, that influences cognitive, psychological, behavioral, and motor skills, having consequences for quality of life (QoL) and everyday living competency.Citation4 The ICD-10 presents four criteria for dementia: 1) impaired memory; 2) clear consciousness; 3) impaired emotional control, motivation or social behavior; and 4) the condition must have lasted for at least 6 months. Dementia is divided into mild, moderate, and severe stages, depending on the extent to which the condition influences everyday living.Citation5
Mild cognitive impairment (MCI) encompasses attention, concentration, memory, comprehension, reasoning, and problem solving. According to Winblad et al (2004), MCI is a useful term as both a clinical and a research entityCitation6 and is usually perceived as the preclinical stage of dementia. However, MCI may be stable and occasionally reversible.Citation7 The risk of mortality seems to be high for all types. Hedman et al (2013) studied patterns of functioning in older adults with MCI and found that they exhibited different patterns: stable, fluctuating, descending, or ascending. The patterns may change over time, and thus individual support is needed.Citation8
Technologies, such as digital calendars, speaking watches, and Global Positioning System (GPS), have been shown to support time orientation, memory, and safety in people with mild cognitive impairment/dementia (MCI/D).Citation9–Citation12 Technology may have the potential to support a person’s occupational performance, meaning helping out “the actual execution or carrying out of an occupation” (p. 26),Citation13 and facilitate a good and dignified life, reducing the pressure on family carers (FCs) and the need for community care services. Dignified lives for older adults, defined by HeggestadCitation14 refers to Jacobson’s definition (2009) of human dignity as “the intrinsic dignity that belongs to every human being,”Citation14 are increasingly discussed in health-care services. Human dignity is closely related to human identity. Being a technology user has implications for identity.Citation15 If a person finds the technology ugly, not user friendly, or not compatible with his or her lifestyle, the device will hardly be accepted.
Access to technology that addresses a need is anticipated to have an impact on QoL, which may be defined as:
an individual’s perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, and standards and concerns.Citation16
However, it is a prerequisite that the technology matches the needs of the user and is accepted as an aid and incorporated into everyday living.
Eicher et al (2017) claimed that good usability and user acceptability encourage patients to engage in the training and coping with the new technology. Therefore, it is interesting to investigate usability and acceptability in technology studies.Citation17 “Usability” is defined as “the extent to which a product can be used by specified users to achieve specified goals with effectiveness, efficiency, and satisfaction in a specified context of use,”Citation18 while “acceptability” is defined as “the degree of primary users’ predisposition to carry out daily activities using the intended device” (p. 73).Citation19 Arthur (2009, p. 29) defined acceptability for technology as being a “means to fulfill a human purpose,”Citation20 and stated that technology may be a method, process, or device.
It has been argued that technology mainly has been provided to safeguard older people with MCI/D at home, with less attention given to technology for assisting people in living a good life.Citation21 Kenigsberg et al (2016) state that assistive technology such as information and communication technologies can provide useful information for assisting older adults with dementia, if tailored to the end users’ capacities. However, there is still a need to educate health staff to assess users’ capacities, preferences, and motivation for using technology and to evaluate the information and communication technologies to better inform technology developers as to user needs and performance styles.Citation22 In addition, an important factor concerns creating a supportive network for the user as part of the technology implementation.Citation23
The criteria for successfully matching technology to a person’s needs and capacities are various. They include health staff’s assessment skills in revealing the needs, resources, challenges, and capacities of the user, their ability to successfully individualize the technology to the user’s needs and context, and the user’s acceptance of technology. An additional issue is the usability of the chosen technology: its maturity, robustness, and predictability as a sustainable solution for the user. The organization of community services and access to proper technology support are also important.Citation24
Several pilot projects (Enable,Citation64 Safe@home,Citation65 ACTION,Citation66 COGKNOW,Citation67 Rosetta,Citation27 Casas,Citation68 and NOCTURNALCitation69) have focused on the usability of different types of technologies for older people with dementia and MCI in test laboratories or at home, and found that such technology may be of benefit for both the person with MCI/D and their FC. However, all of these projects concluded that further research is needed, in particular studies that include the users’ perspectives on usability and acceptability.
This systematic review aims to investigate primary studies that include people with MCI/D in technology trials. As recommended for systematic reviews, we outlined three research questions for our literature search:Citation25
What types of technologies have been explored with home-dwelling older adults with MCI/D?
What is the current knowledge about the usability and acceptability of such technologies with regard to occupational performance, QoL, and human dignity for independent living?
How are users involved in the reviewed technology studies?
Material and methods
This systematic review was prospectively registered in PROSPERO (reg 42017058789, May 7, 2017).
Data sources and search strategy
We searched PROSPERO (www.prospero.org) to check whether others had performed a recent literature review on this topic, before starting the literature search. However, we did not find any earlier or ongoing reviews on this topic.
Eligibility criteria
The review aimed to identify peer-reviewed primary studies concerning technologies that had been developed and/or explored with home-dwelling older adults with MCI/D above 65 years of age. The search included studies from January 2007 to June 2017. Papers in the English language were included.
Inclusion criteria
Primary studies on technology for older people with MCI/D.
The title and/or keywords included a type or types of technology; this could be the name of a device or technology mentioned as a system, eg, smart-home system, ambient assistive living (AAL), or artificial intelligence (AI).
The title and/or keywords included the population (mild) cognitive impairment, dementia, or early phase of dementia, or Alzheimer’s disease.
Exclusion criteria
Not target population (MCI/D)
Not primary study
Laboratory studies
Not technology for support of everyday living
Long-term care/nursing home
Conference paper, editorial, protocol
Review articles/meta-analyses
Books, book chapters.
Information sources
Five databases were searched for studies: MEDLINE, PsycINFO, Embase, AMED, and CINAHL (). A systematic literature search must make use of search words that are valid in the thesaurus of each database, eg, Medical Subject Headings terms.Citation25
Table 1 Databases and search words for identifying literature for review, June 20, 2016
Search strategy
The strategy was to use the Medical Subject Headings terms related to each database. shows an example of the search strategy from the CINAHL database.
Table 2 Example of search strategy
Study selection
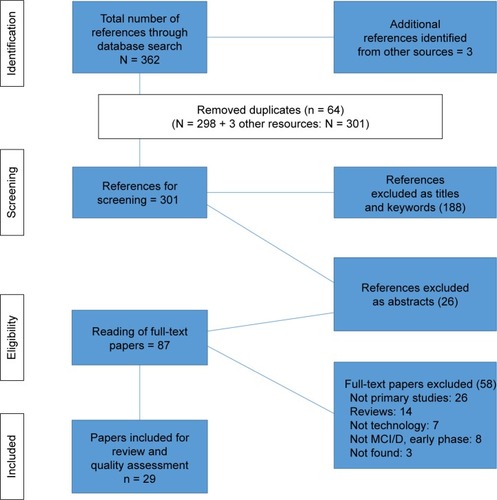
Altogether, 359 titles were identified in this literature search. After checking for duplicates, the number decreased to 298. Ovid Auto Updates were checked for relevant titles after the search date June 20, 2016 and until June 17, 2017. One more paper was of interest; however, the full text was not found. Another two papers were detected through other sources; one was sent to us from an earlier project colleagueCitation34 and the other was found in the first author’s personal archive of papers on technology and dementia.Citation32 Thus, the review consisted of 301 papers to be appraised by all five authors, three nurses, and two occupational therapists. Four of the authors completed Steps 1 and 2 in the review process before the fifth author (a nurse) took part from Step 3 onward.
Review process
The review process had four steps:
Step 1. Screening titles: The pile with 301 titles was divided into two piles. Two teams, each consisting of one nurse and one occupational therapist, screened titles and keywords for relevance separately. Then, the two authors from each team met and compared their screening results and agreed upon which titles to include and exclude. Thereafter, the two teams met and presented their screening results and elaborated an overview of which titles to include for the next step. In this first screening step, 188 titles were excluded.
Step 2. Reading abstracts: The two teams read the abstracts of the selected papers and excluded papers not relevant to the research questions. An additional 26 titles were excluded owing to being reviews, editorials, conference papers, nonintervention studies, studies not involving MCI/D, nursing home studies, or books and book chapters. At the end of this step, 87 titles remained.
Step 3. Reading full-text articles: The first author transferred the 87 titles eligible for full-text review into an Excel file, with columns for data about the aim of studies, number of participants and sample characteristics, study design, types of technologies, and findings regarding usability, effectiveness of technology, and acceptability reported by people with MCI/D and their FCs. The five authors individually read on-fifth of the articles and filled in the data abstraction Excel file. At this step, another 58 papers were excluded for reasons of: not being primary studies (26 studies), being reviews (14 studies), not focusing on technology usability and acceptance (seven studies), participants not having MCI/D (eight studies), and being unable to find the full text of a paper (three studies) (). The full-text review ended up with 29 papers.
Step 4. Out of the pool of five authors, two and two read the same half of the 29 papers. The first author read all the selected papers. We conducted a quality assessment of papers using the Mixed Methods Appraisal Tool (MMAT)Citation26 for systematic mixed methods review. Only papers that clearly stated having a mixed method design were sorted under mixed methods.
Figure 1 PRISMA flowchart for selection of papers.
Abbreviations: PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; MCI/D, mild cognitive impairment/dementia.
Quality assessment of papers
The MMAT for systematic mixed methods review was used to assess the quality of the papers selected for this review. The MMAT has five categories of study design: 1) qualitative; 2) quantitative randomized controlled trials; 3) quantitative nonrandomized; 4) quantitative descriptive; and 5) mixed methods. The MMAT permits the researcher to concomitantly appraise and describe the methodological quality for qualitative, quantitative, and mixed method studies, defined using specific methodological quality criteria.Citation26 Six of the 29 reviewed papers were rated as high-quality studies, meeting all the quality criteria (four stars); 11 were rated with three stars (meeting 75% of the quality criteria); seven with two stars (meeting half of the quality criteria); and five with one star (meeting 25% of the quality criteria) (). This allowed us to overview by the quality of the selected studies and provided the opportunity to exclude studies with the lowest quality from the review, or to contrast high-quality studies with low-quality studies. However, in our review, the aim was to obtain an overview of what technologies have been explored among people with MCI/D and their FCs. Therefore, no studies were excluded because of a lack of quality.
Table 3 Data abstraction sheet
Preparing data abstraction findings for presentation
The following data characteristics were recorded in the Excel files: author, year, country, MMAT score, title; type of technology, purpose of technology; number of participants (MCI/D + FCs/staff); design according to MMAT, duration of intervention, usability/acceptability; impact on QoL, occupational performance, and human dignity; and implications for clinical practice.
According to the template for this paper, data abstraction is presented in three steps: quantitative synthesis, qualitative synthesis, and study designs for user involvement in the 29 reviewed studies.
Results
The aim of this review was three-fold: to obtain an overview of the kind of technologies that were evaluated with people with MCI/D and FCs in the past decade (2007–2017), and how these users rated the usability and acceptability of such technologies. Further, we wanted to learn about how people with MCI/D and FCs had been involved in the studies reviewed.
Characteristics of included studies
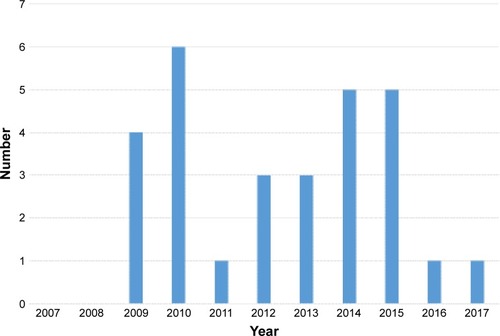
The number of papers published per year varied throughout the past decade and had a peak in 2010 with seven published papers ().
Figure 2 Number of papers per year.
The 29 included papers consisted of 17 qualitative studies, one quantitative randomized controlled trial, two quantitative nonrandomized studies, seven quantitative descriptive studies, and two mixed methods studies. The studies mostly took place in Western countries (), and three papers were connected to the COGKNOW and Rosetta projects.Citation27–Citation29 Another author had published more papers on the same technology.Citation30,Citation31
Figure 3 Overview of papers per country 2007–2017; for papers written in collaboration with authors from other countries, only the first author’s country is counted.
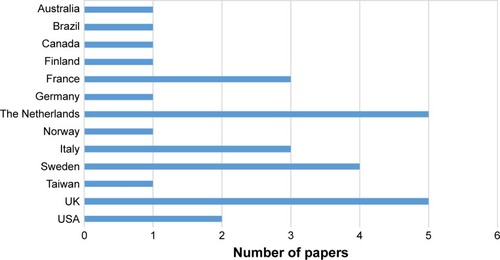
The reviewed papers explored several different technologies in conjunction with persons with MCI/D and their FCs. Most of the studies took place in Europe. However, Taiwan, Brazil, the USA, and Canada were also represented, and all these studies contributed to greater knowledge in the field.
Study participants
The participants in the 29 included papers were older people with MCI or dementia, above 65 years of age. Different terminologies described these participants: older adults with cognitive impairment, Alzheimer’s patients, persons with dementia, users, care recipients, etc. In this review, all primary participants in the target group, people with cognitive impairment due to dementia or MCI, are called “people/persons with MCI/D.” In total, 665 people with dementia and 83 people with MCI had been involved in the 29 technology studies.
The FCs were named informal carer, spouse, relative, significant other, etc. In this paper, we use the expression FC for all. In total, 248 FCs took part in the 29 studies.
Health workers were named formal carer, nurse, therapist, home-care worker, etc. We chose the term “staff” for all professional health personnel. In total, 55 staff members and 23 others (older adults, dementia experts, volunteers) had taken part in the 29 studies.
What types of technologies have been explored with older people with MCI/D?
The first research question was to establish an overview of the types of technologies that had been evaluated with older adults with MCI/D and their FCs in everyday life. After listing the technologies studied, we grouped them into four domains according to aims and purposes: 1) safe walking indoors and outdoors; 2) safe living; 3) independent living; and 4) entertainment and social communication.
Columns two and three of provide an overview of the types of technology and their purposes, and thus answer the first research question.
Domain 1 presents six papers on technology either for locating personsCitation32–Citation34 or for supporting navigation,Citation35,Citation36 or on how to involve users in the product design of devices for location and navigation.Citation37 Domain 2 presents 10 papers on technologies for enhancing safe living, with five studies focused on monitoring systems,Citation19,Citation29,Citation38–Citation40 including two papers particularly describing technology for nighttime security.Citation38,Citation39 Further, one paper investigated “stand-alone” technologies to enhance safe living,Citation40 and one study investigated user requirements prior to the development of a safety wristband.Citation41
Domain 3 presents six studies that explored possibly improved occupational performance with the help of technology.Citation30,Citation31,Citation42–Citation45
Domain 4 presents seven studies on technologies for entertainment and leisure. Four papers explored the use of touch-screen tablets (iPads).Citation21,Citation46–Citation48 One study explored using a camera to document personal events with the intention of reminding the person of (jogging the memory for) recent events,Citation49 and one study used a digital board with a touch screen for both cognitive stimulation and joy.Citation50
In general, some technologies were multifunctional and could therefore belong to more than one domain. Seven studies described user participation with MCI/D and their FC to identify user requirements, as recommendations for development of design of products (see “How users were involved in technology development,” later in this section). Only one study compared the user friendliness of two different strategies for indoor navigation for people with MCI/D; namely, a radio frequency identification navigation device (a device communicating with radio frequency signals) compared with an aerial map.Citation36 Suijkerbuijk et al (2015) asked users with MCI/D to evaluate their use of a dynamic lamp, which aimed to improve sleep/wake rhythms, by answering questions playing a personal evaluation game on an iPad (“Angenaam”) (eight couples) or answering a questionnaire using a tablet (four couples).Citation51
Current knowledge about the usability and acceptability of the explored technologies
Our second research question was about the usability and acceptability of the technologies with regard to occupational performance, QoL, and human dignity for independent living. Column seven in presents the knowledge on usability and acceptability in the reviewed studies, while column eight presents findings related to QoL, occupational performance, and human dignity.
Usability and acceptability in the reviewed studies
Many of the studies explicitly aimed to evaluate the usability of the technologies that were explored.Citation19,Citation28,Citation38,Citation40,Citation43,Citation47,Citation49,Citation51 Cavallo et al (2015) found that perceived usability could improve QoL for people with MCI/D and their FCs.Citation19 Cavallo et al (2015),Citation19 Leuty et al (2013),Citation47 and Lindqvist et al (2015)Citation43 used the same definition as this review regarding usability. Meiland et al (2012, p. 584) explained usability in terms of “user friendliness” (gratifying, easy to manage), “usefulness” (meeting the needs and desires of people with dementia), and “effectiveness” in promoting autonomy, coping, and QoL.Citation28 Lindqvist (2015, p. 138) operationalized the concept of usability to include three factors: the user’s desired goals, the hindering task according to the user, and the chosen assistive technology.Citation43 Some researchers used the term “user friendliness” instead of usability.Citation28,Citation42 Boman et al (2014, p. 170) stated that acceptance of technology has been associated with “the ability to maintain a certain desired self-image of being competent.”Citation42
None of the studies explicitly evaluated the acceptability of technologies. Some studies reported degrees of acceptance in people with MCI/D and FCs; for example, finding a device ugly could be interpreted as being not accepted,Citation32 while experiences of fewer worries for the person with MCI/D or spare time for the FCCitation33 could mean that the device is accepted.
Usability and acceptability of technology that aims to provide safe walking
Safe walking outdoors refer to the opportunity for people with MCI/D to go for walks alone. Safe walking involves many aspects: strategies for wayfinding, the ability to return to the starting point, physical strength/endurance, balance, judgment of one’s own physical capacity, vision, footwear, the surface of the outdoor area, and surrounding characteristics, such as woods, beaches, parks, or cities with heavy traffic, etc. Three papers included the GPS as the subject for technology evaluation.Citation32–Citation34 The studies from 2009 and 2011 included a GPS localization device, whereas the study from 2017 included a wearable arm–wrist mobile safety alarm with GPS and two-way communication, which can be used both indoors and outdoors, 24 hours a day. GPS is a technology mainly used for the localization of a person. One dyad case study found that the user agreed to carry the GPS only to reassure his wife, and he perceived the GPS as a limitation rather than an instrument of freedom, as his wife did. The couple stressed that the device should not be stigmatizing but rather unnoticeable and support autonomy.Citation32 FC users of GPS technology expressed fewer worries and reported that the technology was easy to use.Citation33 Røhne et al (2017) found that people with MCI/D who had a mobile safety alarm were able to stay longer at home.Citation34 Two other studies explored navigation technologies for indoor wayfinding.Citation35,Citation36 Chang et al (2010) tested a prototype of near-field radio frequency identification technology, having six people with MCI/D find their way from A to B in a hospital setting,Citation35 and Lanza et al (2014) compared the use of mobile navigation technology with photographs to ordinary aerial maps for autonomous outdoor wayfinding within a large hospital campus.Citation36 Both studies found that the participants with MCI/D managed wayfinding in approximately half of the attempts. Therefore, the evaluated technologies seemed promising, given that repeated training sessions are available.
Usability and acceptability of technology for safe living
Five studies explored integrated monitoring systems, also called AAL, that aim to support independent living and detect risks/events in the home to send alerts in case of accidents.Citation19,Citation27–Citation29,Citation38,Citation39 The purposes of these technologies varied somewhat, including to “support MCI/D at home,”Citation27 to create “safe environments and prevent injuries and avoid unattended exits at night,”Citation39 and to “monitor health status, safety, and activities of daily living”.Citation19 AAL could also imply a strategy to decrease the burden of care for FCsCitation40 and to postpone the need for transition to a nursing home.Citation39
The AAL systems could also offer multimodal assistive services, with cognitive stimulationCitation38 providing reminders to the person with dementia about events or tasks to carry out, and facilitating communication with family and friends.Citation28 The AAL systems normally required internet-based computers.Citation28 None of the papers presented perceptions of these AAL technologies from the perspective of those with MCI/D.
One paperCitation40 presented user experiences with different “stand-alone” technologies that are not a part of a system but that still aim to contribute to safety at home by preventing risks, detecting emergencies, and assisting the memory of persons with MCI/D. Riikonen et al (2010) found that such technologies contributed to decreased stress in FCs. People with MCI/D seemed to accept best passive devices that did not require active control or activation.Citation40
Usability and acceptability of technology for independent living
Some technologies aimed to promote independence and autonomy by compensating for lost cognitive skills, for example, by providing reminders via a sound, a light, and/or a written or spoken message. Because cognitive impairments affect occupational performance, compensatory technology can be useful for some. Lancioni et al (2010) tested verbal instruction technologies to remind persons with MCI/D about the steps in a given task, and this strategy seemed to help them recapture the performance.Citation31 One study presented occupational performances of self-chosen, everyday technologies,Citation45 and found that both intrapersonal capacities and environmental characteristics influenced the performance of handling the technology.
Usability and acceptability of technology for entertainment and social communication
Six studies tested computer tablets and iPads with people with MCI/D.Citation21,Citation46–Citation48,Citation50,Citation51 The purposes were mainly to provide meaningful engagementCitation21 and cognitive stimulation from photos, music, and games.Citation46,Citation48,Citation50 De Oliveira Assis et al (2010) found that 50 minutes of cognitive stimulation programs twice a week positively influenced cognitive functioning, as demonstrated with pre–post measures on the Mini-Mental State Examination.Citation50 Another study used tablet computers in art activities, which was appreciated by participants with MCI/D. They expressed excitement about the novelty of the device and satisfaction with the art they made.Citation47 The therapists, however, remained uncertain as to whether the MCI/D participants were truly satisfied with the tablet computers.Citation47
Astell et al (2010) evaluated tablets as social communication and reminiscence devices between staff and people with MCI/D. They compared the use of tablets to traditional reminiscence work, and found that the tablets increased the interaction between staff and residents, empowering people with MCI/D and redressing the status hierarchy during the course of the interaction, as well as leading to increased job satisfaction in staff members.Citation21
Tablets were also explored regarding entertainment and joy. Kerssens et al (2015) found that the majority of seven persons with MCI/D enjoyed the touch-screen shows, which brought back memories and helped with relaxation and joy. However, two of the six persons with MCI/D did not use the touch screen independently.Citation46 Lim et al (2013) found in their study of 21 people with MCI/D that almost 43% used the tablet independently for more than 10 minutes/day, which proved to be helpful for FCs. However, 18% of the people with MCI/D expressed a clear disinterest. The study concluded that user needs must be considered on a case-by-case basis, along with access to informal support.Citation48
How users were involved in technology development
This subsection answers the third research question: How are users involved in the reviewed technology studies?
One major finding, represented in all 29 papers, emphasizes user involvement in preimplementation technology design and development and feasibility testing. Several studies highlighted the need to identify and confirm user needs in older adults with MCI/D in order to develop useful technologies, as earlier studies had mainly asked proxy persons these questions. Potential users of the technology include persons with MCI/D, their FCs, and staff, and they took all part in the studies we reviewed (see column four in ).Citation28,Citation29,Citation37,Citation38,Citation41,Citation42,Citation52 Some studies showed prototypes or mock-ups of the technology in question, in order to facilitate users’ responses on perceptions and opinions.Citation29,Citation41 Involving people with dementia in the process of participatory design is feasible. This could lead to the development of devices that are more acceptable and relevant to their needs.Citation41 According to Cavallo et al (2015), the involvement of persons with MCI/D and FCs in the design of technologies was fundamental for participation in a trial.Citation19 Meiland et al (2014)Citation29 and Hattink et al (2016)Citation27 explicitly recommended user participation in the design of new technologies and evaluation of their user friendliness and usefulness.
The study designs for user involvement varied. The most frequent design was the focus group. Five studies carried out focus groups for MCI/D and four for FCs.Citation29,Citation37,Citation38,Citation42,Citation52 Two studies used workshops as the method for user engagement,Citation29,Citation41 and six studies used observation as method.Citation28,Citation40,Citation43–Citation45,Citation53 Most studies used more than one method for data collection (see column five, ).
Nine studies were experimental trials, which often started with a workshop or focus group with MCI/D participants and FCs/staff to identify user needs and requirements.Citation19,Citation29,Citation38 Thereafter, the same participants were invited to give their opinions on a mock-up or prototype device installed at home, in order to evaluate usability and acceptance. The primary aim was to hear the voice of the MCI/D participant and to learn about the usability of the device. Only three studies were randomized controlled trials, with a pre–posttest design and control group.Citation29,Citation36,Citation39
Some studies underlined the necessity of tailoring the technology to the user’s needs and preferences.Citation33,Citation43,Citation48 Pot et al (2012) stated that the specific problem for the person with MCI/D and FC must be defined, in order to identify the most appropriate solution.Citation33 During the user-needs assessment, it is thus important to assess the user’s ability to manage the everyday technology that they already possess and are familiar with before any new technology is introduced.Citation45 According to Malinowsky et al (2010), intrapersonal skills and environmental characteristics influence performance and management of technologies, but at the same time, the “person–environment fit” is dynamic, ie, it will change over time.Citation44 Adaptation of the social and physical environment can facilitate the management of everyday technologies by people with MCI/D.Citation44 Further, each user’s customization to the technology always depends upon the self-perception of his or her own goals.Citation43 If the technology was evaluated as positive, it proved successful in improving the social (care) network and reduced stress in FCs.Citation40
Discussion
This review aimed to obtain an overview of the types of technologies being explored with persons with MCI/D, identifying the usability and acceptability of such technologies with regard to occupational performance, QoL, and human dignity, as well as to learn how user involvement of those with MCI/D and FCs was achieved in these studies.
Types of technologies
The reviewed studies showed a wide range of technologies, such as GPS, monitoring systems, tablets, touch-screen computers with calendar, clock and task reminders, verbal instruction technology, and robot technology, which we categorized into four domains related to the purposes of everyday living: safe walking, safe living, independent living, and entertainment and social communication. However, the technologies within the domains may overlap. For example, a stove timer with the purpose of safety at home can be a “stand-alone” device or a part of AAL technologies, with the potential to send an emergency alarm. Likewise, a digital calendar for supporting a person’s memory may be a separate device, as well as part of a digital structure enhancing safety at home. Sometimes, technologies may benefit others than the person with dementia. Gibson et al (2016, p. 7) conducted a scoping review and found 171 types of assistive technologies, which they divided across three areas: “assistive technology used ‘by’, ‘with,’ and ‘on’ people with dementia.”Citation54 Another divide can be between “active” and “passive” technologies,Citation63 depending on the person with MCI/D’s role as a technology user. Lindqvist et al (2015) stated that the person with MCI/D’s perception of the extent to which their own goals have been achieved must be included to assess the usability of a product or solution.Citation43
Usability and acceptability
Technology that is simple to use and enables a person with reduced cognitive capacity to cope independently with daily tasks and obligations is classified as being usable and acceptable. The usability of technology was defined as user friendliness, usefulness, and effectiveness,Citation28 and by the extent to which a product can help a user to achieve a specific goal. User-friendly technologies are thus a means to enable older adults and people with reduced capacities to engage in activities and participate in society, equal to other citizens. McCreadie and Tinker (2005) found that a technical device must address a person’s “felt need” in order to be perceived as useful.Citation55 This is in line with Peek et al (2014, p. 242), who found that a perceived personal need for technology was the most frequent factor mentioned for technology use and acceptance.Citation56
Several authors referred to the International Organization for Standardization’s definition of usability.Citation19,Citation43,Citation47 However, it may be interesting to discuss usability related to utility and identity. Ravneberg and Söderström (2017) stated that usability is used synonymously with user friendliness and easy to use/learn, while utility is the functionality of the technology, and identity is connected to a user’s opinion of whether the device/aid matches the user’s personal character and reflects the person’s identity.Citation15 These aspects may be difficult to distinguish and will influence the acceptability of a device. The degree to which the technology was accepted depended upon the end users’ experiences of reliability and stability of the technical performance of the device.Citation28 Acceptability also considers whether the device matches the user’s identity.Citation15 This may explain why users may hesitate to wear a device (eg, GPS) in their belt or pocket. The device may make the user feel stigmatized and result in rejection of the device. Some older adults will perceive a technology as being more relevant for other elderly people with more extensive functional impairmentsCitation56 and be less motivated to use it themselves. One major consideration is the ability and motivation of the person with MCI/D to accept and incorporate such technologies in their everyday living.Citation24 A Swedish study that found that older adults with MCI strived to downsize their approaches toward everyday activities, owing to changing abilities. They achieved this by using familiar technologies in a new way, by replacing old technology with something simpler. Sometimes they chose to stop using technology, although they needed it, or they had a desire to update their technology use.Citation57 However, downsizing use of technologies will become a challenge when the health services seek to implement new technologies. Older adults may be reluctant to use new technology that they not yet are familiar with.Citation58
However, one finding was that usability of technology often was rated low at the beginning of the project,Citation19 which may be associated with late or nonadopters of technologies, or with skepticism toward new technologies. Also, it could be that FCs were unaware of the potential of the technologies and feared that they would not be appropriate for the person with MCI/D. Peek et al (2016, p. 4) revealed that older adults stated that such technologies were not necessarily intended for them, but rather “for others, less healthy older people.”Citation58
Engaging older adults in a preimplementation study thus risks obtaining a “prototypical result,” according to Peek et al (2014).Citation56 Posttrial evaluation of usability and acceptability was more positive as users had experienced the technologies’ potential to improve the quality of care.Citation19 A clinical trial allowing end users to try the technology at home, in real-life situations, seemed to be an eye-opener by giving older adults the opportunity to realize how technology may, or may not, be of benefit. Therefore, clinical trials with end users are needed to evaluate the usability and acceptability of technologies.
Surprisingly, less than half of the 22 reviewed studies on technology trials reported the perceptions of the participants with MCI/D on the usability and acceptability of the explored technologies. The proxy opinions of FCs and staff were mainly reported. This finding leads us to ask why the opinions of the participants with MCI/D were so scarcely reported.
User involvement in the studies
User involvement was included in all the reviewed studies, which involved both persons with MCI/D and their FCs or staff. User involvement requires a bottom–up approach: that developers and researchers assess persons’ experiences with technology tried at home and consider those opinions when furthering development work. The evaluation of a product or solution with potential end users is a way of ensuring that the device works sufficiently for the target group. Some of the studies highlighted that the technology must be tailored to the user in order to be useful and usable.Citation19,Citation43,Citation45,Citation52 The study by Robinson et al (2009) contained a three-stage user-centered design (UCD) process involving persons with MCI/D and FCsCitation41 (UCD was introduced by Rubin in 1994,Citation59 as a method to explore user needs and requirements and put the user at the center of the design process.). Robinson et al (2009) concluded that user engagement resulted in products that were more acceptable and relevant to the users’ needs.Citation41 Augusto et al (2014) implemented technology in accordance with UCD principles, to monitor the sleep/wake patterns in five households dealing with persons with dementia and their FCs. Thereafter, they developed an appropriate technological solution together. This exploration informed improved design of user interfaces.Citation38
Even if it is challenging to include people with MCI/D in a user-driven development process, it is worthwhile.Citation42 Meiland et al (2012) recommend a user participatory design with direct involvement of people with MCI/D and FCs, from the beginning of the project and through the whole process.Citation28 McCabe and Innes (2013) stated that user engagement in product development provided valuable inputs on how GPS might be designed and used.Citation37 They stated that successful devices are those that give consideration to real-life use and concerns from potential users.Citation37 In other words, developing user-friendly interfaces, which are found to be usable and acceptable by the end users, requires user involvement. However, the terms “user” or “end user” might include both persons with MCI/D and FCs in the reviewed trials. We found it difficult to distinguish between the opinions of the person with MCI/D and those of the FC or staff on the technologies tried at home. Further research should investigate and report possible discrepancies between these parts.
Finally, the duration of the intervention and the study design influenced results on assessing usability and acceptability, since MCI/D usually progresses over time. Five of the studies lasted for less than 2 months, and eight lasted 6 months or longer. In one study,Citation32 the person with dementia and his spouse left the trial after only 1 day. No information or training was provided prior to the trial, which in other studies seemed to be important. For how long should people with MCI/D try a product in order to be able to appraise it?
Attitudes toward MCI/D are changing, and nowadays people with MCI/D are more aware of their needs and rights. The European Dementia Working Group’s slogan, “Nothing about us without us,”Citation60 underscores their desire for user participation in all service planning and authorizes their expression of own needs and preferences for technological or human support. The findings of this review clearly underscore the value of user involvement in technology development and clinical trials. More research is needed on what happens when technology is introduced to people with MCI/D and their environments, and whether technology will accommodate the needs and wishes stated by people with MCI/D and their FCs in a just and ethical way.
Possible biases
First, our search strategy may contain biases. We had many search words, which were challenging to include in one search. The search stories became long and we had to put extra effort into screening more titles for relevance.
Most of the studies reviewed had small sample sizes, and 10 out of the 29 studies had 10 participants or fewer. This is often criticized as a possible bias because generalization of results is not possible. However, our aim was to explore the width and depth of technology interventions, and small sample sizes nevertheless provided rich data. Further, multiple publications from the same authors/projectsCitation24–Citation27,Citation38,Citation39 may also skew the impression of the extent of the research.
Another possible bias is the close and regular relation between the participants and the researchers over time, as mentioned by Browne et al (p. 719).Citation49 Since many of the experiments had a pre–post design, and follow-up after a period, many participant–researcher relations may have developed beyond a neutral and formal attitude, to a more informal and friendly relationship. However, this is difficult to avoid in a participatory action research approach, where the research process relies on collaboration between the researcher and participants.Citation61
One bias may be the use of the MMAT matrix for quality assessments of the 29 eligible papers. Five team members rated one-fifth of the papers individually, before comparing the assessment results with another team member. If discrepancies arose, a third team member was involved in the decision. Even though we chose not to exclude any of the papers owing to low quality, the quality assessment provided an overview of the quality of the papers included in our review.
Conclusion
The research about technologies to support people with MCI/D in everyday living seems optimistic, and a wide range of technologies has been evaluated at home with persons with MCI/D and their FCs. A major and representative finding was the importance of including those with MCI/D and their FCs in research, in order to learn about required design features to enhance usability and acceptability. Few studies reported findings on people with MCI/D’s perceptions of the acceptability and usability of the technologies or on the consequences of technology for QoL and occupational performance. None reported the consequences of technology use relating to human dignity.
Author contributions
TH, first author, PhD student, led the review, took part in the literature searches, screened half of the titles, and reviewed all abstracts before a full-text reading of all included papers. She prepared and wrote all versions of this paper for discussion with co-authors, and later completed the paper for submission. All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
LH, second author, mentor, took part in the literature searches, screened half of the titles, reviewed one-fifth in full text, and carried out the quality assessment according to MMAT. She judiciously contributed to the design of this paper, endorsing and commenting on the work during the entire process, as well as critically revising the article for final approval.
DK, third author, took part in the literature searches, screened half of the titles, reviewed one-fifth in full text, and performed a quality assessment according to MMAT. He contributed to the design of this paper and offered discerning appraisal during the writing process, critiquing and revising this paper for intellectual content.
K-AH, fourth author, entered the author group somewhat later. She read one-fifth of the titles in full text and assessed the quality of the papers according to MMAT. She read three versions of this paper and contributed with critical appraisal during the writing process.
AL, fifth author, took part in the literature searches, screened half of the titles, reviewed and quality-assessed one-fifth of the full-text papers, contributed to the design of the review, and contributed to the writing process. She revised this article for intellectual content and for final approval before it was submitted for publication.
Acknowledgments
We want to acknowledge the Norwegian Research Council, which funded the Assisted Living Project, librarian Bente Schjødt-Osmo, Cappelen Damm, for excellent supervision during the first literature search, and librarian Kristin Røijen, HIOA, for assisting the search of the CINAHL database. Further, we would like to thank the Assisted Living Project group and project leader Ellen-Marie Forsberg, AFI, HIOA (https://assistedlivingweb.wordpress.com/). Finally, we thank Oslo and Akershus University College, HIOA, for financing this Dove Press Open Access publication.
Disclosure
The authors report no conflicts of interest in this work.
References
- von SchombergRA vision of responsible research and innovationOwenRBessantJHeintzMResponsible Innovation: Managing the Responsible Emergence of Science and Innovation in SocietyLondonJohn Wiley & Sons20135174
- DamodaranLOlphertWForesight Evidence Review: How Are Attitudes and Behaviours to the Ageing Process Changing in Light of New Media and New Technology? How Might These Continue to Evolve by 2025 and 2040? GS/15/17LondonGovernment Office for Science201527
- Alzheimers.net [database on the Internet]2016Alzheimer’s statistics Available from: alzheimers.net/resources/alzheimers-statisticsAccessed September 13, 2017
- EngedalKHaugenPKDemens—Fakta og utfordringer. En lærebok [Dementia—Facts and Challenges. A Textbook]5th edTønsbergForlaget Aldring og helse2009
- WHOInternational Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10). F00: Dementia in Alzheimer Disease2016 Available from: http://apps.who.int/classifications/icd10/browse/2016/en#/F00Accessed May 15, 2017
- WinbladBPalmerKKivipeltoMMild cognitive impairment—beyond controversies, towards a consensus: report of the International Working Group on Mild Cognitive ImpairmentJ Intern Med200425624024615324367
- PetersenRCRobertsROKnopmanDSMild cognitive impairment: ten years laterArch Neurol200966121447145520008648
- HedmanANygårdLAlmkvistOKottorpAPatterns of functioning in older adults with mild cognitive impairment: a two-year study focusing on everyday technology useAging Ment Health201317667968823550598
- LindqvistENygårdLBorellLSignificant junctures on the way towards becoming a user of assistive technology in Alzheimer’s diseaseScand J Occup Ther201320538639623394183
- NygårdLStarkhammarSThe use of everyday technology by people with dementia living alone: mapping out the difficultiesAging Ment Health20071114415517453547
- ØderudTGrutLAketunSSamspill—GPS i Oslo. Pilotering av Trygghetspakke 3. Bruk av GPS for lokalisering av personer med demens [Interaction—GPS in Oslo. Piloting Safety Package 3. Using GPS to Locate People with Dementia]OsloSINTEF Teknologi og samfunn, avd. helse, SINTEF IKT8172015
- ØrjasæterNKistorpKVelferdsteknologi i Sentrum (VIS)Innføring av velferdsteknologi i sentrumsbydene i Oslo [Wellfare Technologies in Focus (WIF). Introduction of wellfare technologies in downtown districts of Oslo]2016 Available from: https://helsedirektoratet.no/Documents/Velferdsteknologi/Velferdsteksnologi%20i%20sen-trum_delleveranse%202%20av%202.pdfAccessed May 15, 2017
- TownsendEAPolatajkoHJEnabling Occupation II: Advancing an Occupational Therapy Vision for Health, Well-Being & Justice Through OccupationOttawaCanadian Association of Occupational Therapists2007
- HeggestadATo Be Taken Seriously as a Human Being [PhD dissertation]OsloUniversity of Oslo2014
- RavnebergBSöderströmSDisability, Society and Assistive TechnologyLondonRoutledge2017
- WHOQOL GroupThe World Health Organization Quality of Life assessment (WHOQOL): position paper from the World Health OrganizationSoc Sci Med19954110140314098560308
- EicherCHaesnerMSprangerMKuzmichevaOGräserASteinhagen-ThiessenEUsability and acceptability by a younger and older user group regarding a mobile robot-supported gait rehabilitation systemAssist Technol20171619
- International Organization for Standardization. ISO 9241-110:2006Ergonomics of Human-System InteractionGenevaISO2006
- CavalloFAquilanoMArvatiMAn ambient assisted living approach in designing domiciliary services combined with innovative technologies for patients with Alzheimer’s disease: a case studyAm J Alzheimers Dis Other Demen2015301697724951634
- ArthurWBThe Nature of Technology: What It Is and How It EvolvesLondonAllen Lane2009
- AstellAJEllisMPBernardiLUsing a touch screen computer to support relationships between people with dementia and caregiversInteract Comput2010224267275
- KenigsbergPAAquinoJPBérardADementia beyond 2025: knowledge and uncertaintiesDementia (London)201615162125740575
- RosenbergLKottorpANygårdLReadiness for technology use with people with dementia: the perspectives of significant othersJ Appl Gerontol2012314510530
- ArntzenCHoltheTJentoftRTracing the successful incorporation of assistive technology into everyday life for younger people with dementia and family carersDementia (London)201615464666224784941
- MoherDLiberatiATetzlaffJAltmanDGPRISMA GroupReprint—Preferred Reporting Items for Systematic Reviews and Meta-Analyses: the PRISMA statementPhys Ther200989987388019723669
- PluyePRobertECargoMProposal: A Mixed Methods Appraisal Tool for Systematic Mixed Studies ReviewsMontrealMcGill University2011 Available from: http://mixedmethodsappraisaltool-public.pbworks.comAccessed August 29, 2016
- HattinkBJMeilandFJOvermars-MarxTThe electronic, personalizable Rosetta system for dementia care: exploring the user-friendliness, usefulness and impactDisabil Rehabil Assist Technol2016111617124989993
- MeilandFJBoumanAISävenstedtSUsability of a new electronic assistive device for community-dwelling persons with mild dementiaAging Ment Health201216558459122360649
- MeilandFJHattinkBJOvermars-MarxTParticipation of end users in the design of assistive technology for people with mild to severe cognitive problems: the European Rosetta projectInt Psychogeriatr201426576977924507571
- LancioniGSinghNO’ReillyMPersons with mild and moderate Alzheimer’s disease use verbal-instruction technology to manage daily activities: effects on performance and moodDev Neurorehabil200912418119019842817
- LancioniGESinghNNO’ReillyMFTechnology-aided verbal instructions to help persons with mild or moderate Alzheimer’s disease perform daily activitiesRes Dev Disabil20103161240125020696547
- FaucounauVRiguetMOrvoenGElectronic tracking system and wandering in Alzheimer’s disease: a case studyAnn Phys Rehabil Med20095257958719744906
- PotAMWillemseBMHorjusSA pilot study on the use of tracking technology: feasibility, acceptability, and benefits for people in early stages of dementia and their informal caregiversAging Ment Health201216112713421780960
- RøhneMBoysenEAusenDWearable and mobile technology for safe and active livingpHealth 2017 Proceedings of the 14th International Conference on Wearable, Micro & Nano Technologies for Personalized Health14–16 May 2017Eindhoven, The NetherlandsAmsterdamIOS Press2017133139
- ChangYJPengSMWangTYChenSFChenYRChenHCAutonomous indoor wayfinding for individuals with cognitive impairmentsJ Neuroeng Rehabil201074520840786
- LanzaCKnörzerOWeberMRiepeMWAutonomous spatial orientation in patients with mild to moderate Alzheimer’s disease by using mobile assistive devices: a pilot studyJ Alzheimers Dis201442387988424958461
- McCabeLInnesASupporting safe walking for people with dementia: user participation in the development of new technologyGerontechnology2013121415
- AugustoJMulvennaMZhengHNight optimised care technology for users needing assisted lifestylesBehav Inf Technol2014331212611277
- RoweMAKellyAHorneCReducing dangerous nighttime events in persons with dementia by using a nighttime monitoring systemAlzheimers Dement20095541942619751921
- RiikonenMMäkeläKPeräläSSafety and monitoring technologies for the homes of people with dementiaGerontechnology2010913245
- RobinsonLBrittainKLindsaySJacksonDOlivierPKeeping In Touch Everyday (KITE) project: developing assistive technologies with people with dementia and their carers to promote independenceInt Psychogeriatr200921349450219193255
- BomanILNygårdLRosenbergLUsers’ and professionals’ contributions in the process of designing an easy-to-use videophone for people with dementiaDisabil Rehabil Assist Technol20149216417224512219
- LindqvistELarssonTJBorellLExperienced usability of assistive technology for cognitive support with respect to user goalsNeuroRehabilitation201536113514925547777
- MalinowskyCAlmkvistOKottorpANygårdLAbility to manage everyday technology: a comparison of persons with dementia or mild cognitive impairment and older adults without cognitive impairmentDisabil Rehabil Assist Technol20105646246920545577
- MalinowskyCAlmkvistONygårdLKottorpAIndividual variability and environmental characteristics influence older adults’ abilities to manage everyday technologyInt Psychogeriatr201224348449522067900
- KerssensCKumarRAdamsAEPersonalized technology to support older adults with and without cognitive impairment living at homeAm J Alzheimer Dis Other Demen20153018597
- LeutyVBogerJYoungLHoeyJMihailidisAEngaging older adults with dementia in creative occupations using artificially intelligent assistive technologyAssist Technol2013252727923923689
- LimFSWallaceTLuszczMAReynoldsKJUsability of tablet computers by people with early-stage dementiaGerontology201359217418223257664
- BrowneGBerryEKapurNSenseCam improves memory for recent events and quality of life in a patient with memory retrieval difficultiesMemory201119771372221942784
- de Oliveira AssisLTiradoMGde Melo PertenceAEPereiraLSManciniMCEvaluation of cognitive technologies in geriatric rehabilitation: a case study pilot projectOccup Ther Int2010172536320146197
- SuijkerbuijkSBrankaertRde KortYASnaphaanLJden OudenESeeing the first-person perspective in dementia: a qualitative personal evaluation game to evaluate assistive technology for people affected by dementia in the home contextInteract Comput20152714759
- WuYHCristancho-LacroixVFassertCFaucounauVde RotrouJRigaudASThe attitudes and perceptions of older adults with mild cognitive impairment toward an assistive robotJ Appl Gerontol201635131724652924
- MehrabianSExtraJWuYHPinoMTraykovLRigaudASThe perceptions of cognitively impaired patients and their caregivers of a home telecare systemMed Devices (Auckl)20158212925552909
- GibsonGNewtonLPritchardGFinchTBrittainKRobinsonLThe provision of assistive technology products and services for people with dementia in the United KingdomDementia (London)201615468170124803646
- McCreadieCTinkerAThe acceptability of assistive technology to older peopleAgeing Soc200525191110
- PeekSTMWoutersEJMvan HoofJLuijkxKGBoeijeHRVrijhoefHJMFactors influencing acceptance of technology for aging in place: a systematic reviewInt J Med Inform20148323524824529817
- HedmanALindqvistENygårdLHow older adults with mild cognitive impairment relate to technology as part of present and future everyday life: a qualitative studyBMC Geriatr2016167327036538
- PeekSTMAartsSWoutersEJMCan smart home technology deliver on the promise of independent living?van HoofJDenirisGWoutersEHandbook of Smart Homes, Health Care and Well-BeingChamSpringer2016203214
- RubinJHandbook of Usability: How to Plan, Design and Conduct Effective TestsNew YorkJohn Wiley & Sons1994
- European Working Group of People with DementiaNothing about us without us23rd Alzheimer Europe ConferenceSt Julian’s, MaltaOctober 2013 Available from: http://www.alzheimer-europe.org/Conferences/Previous-conferences/2013-St-Julian-s/Detailed-programme-abstracts-and-presentations/SS1.-Nothing-about-us-without-usAccessed January 9, 2018
- CreswellJWResearch Design Qualitative, Quantitative, and Mixed Method Approaches4th edThousand OaksSage2014
- DemersLWeiss-LambrouRSkaBThe Quebec User Evaluation of Satisfaction with Assistive Technology (QUEST 2.0): an overview and recent progressTechnol Disabil200214101105
- Swarthmore College Computer SocietyTechnology definitions www.sccs.swarthmore.edu/users/97/jahall/thesis/tech/actpassive.htmlAccessed January 9, 2018
- EU-project ENABLE QLK6-CT-2000-00653 (2001–2004) National reports from assessment studies in UK, Finland, Norway and Lithuania Available from: Enable. www.enableproject.orgAccessed May 22, 2017
- WoolhamJFrisbyBHow technology can help people feel safe at home Available from: https://www.researchgate.net/publication/292541867Accessed May 22, 2017
- MagnussonLBertholdHChambersMBritoLEmeryDDalyTUsing telematics with older people: the ACTION project. Assisting Carers using Telematics Interventions to meet Older persons’ NeedsNurs Stand19981353640
- MeilandFJReinersmannASävenstedtSUser-participatory development of assistive technology for people with dementia – from needs to functional requirements. First results of the COGKNOW projectNon-Pharmacological Therapies in Dementia2010117190
- AlberdiAWeakleyASchmitter-EdgecombeMSmart Homes predicting the Multi-Domain Symptoms of Alzheimer’s DiseaseIEEE J of biomedical and health informatics2018 Available from: http://eecs.wsu.edu/~cook/pubs/jbi18.pdfAccessed March 19, 2018
- AugustoJCZhengHMulvennaMWangHCarswellWJeffersPDesign and Modelling of the Nocturnal AAL Care SystemAmbient Intelligence – Software and Applications201192109116