
Abstract
Background
Older adults are at risk of multiple chronic diseases, most of which could be prevented by engaging in regular physical activity. Frailty is a state of increased vulnerability to diseases. Worsening symptoms of frailty, such as decrease in physical functionality, can compromise health-related quality of life (HR-QOL). Previous findings suggest that frailty moderates the relationship between physical activity and HR-QOL, yet intervention findings are limited, particularly in dose–response analyses. Hence, this study was conducted to test if lower-dose physical activity (120 minutes/week) would provide the same benefits in health outcomes (physical functionality and HR-QOL) as higher-dose physical activity (180 minutes/week).
Methods
Participants (n=110) were older adults comprising higher-dose, lower-dose, and control groups who were combined from recent randomized controlled trials. Experimental groups participated in a multimodal exercise program in a supervised laboratory setting for 12 weeks.
Results
The higher-dose group showed a significant improvement in physical functionality (β=0.23, P=0.03) and in overall HR-QOL (β=0.44, P=0.001) including its subcategories over the control group. A group × frailty interaction revealed that frail individuals significantly improved in capacity HR-QOL when they exercised at a higher dose (F (1, 49)=4.57, P=0.038).
Conclusion
This study identifies a positive, predictive relationship between exercise duration and health outcomes (HR-QOL dimensions and frailty) among older adults. Frail individuals in the higher-dose group demonstrated significant recovery of capacity HR-QOL, thus reflecting improvement in their daily activities.
Background
Older adults (age 65+) carry the highest risk for several chronic illnesses and conditions such as cancer, heart disease, cognitive impairments, and dementia.Citation1 Although health can be improved via a variety of behavior modifications, exercising regularly is considered to be one of the most effective preventive measures. Engaging in regular exercise functions as a robust primary and secondary preventive measure against multiple chronic illnesses including cardiovascular disease, cancer, and diabetes.Citation2,Citation3 Exercising regularly has also demonstrated various improvement in health outcomes among older adults such as cognitive function, symptoms of depression, and reduction in anxiety.Citation4
Health outcomes: health-related quality of life, physical functionality, and frailty
In addition to the cumulative benefits of exercise in reducing the risk of chronic diseases and improving psychological outcomes in older adults, research has also demonstrated that exercising regularly enhances psychological well-being and health-related quality of life (HR-QOL).Citation5 HR-QOL is the perceived physical and mental health perceptions such as energy level and mood.Citation6 Changes in this construct could signify improvement or worsening of illness and illness-related debilitating symptoms. Exercise has been shown to be a positive predictor of HR-QOL in the general population,Citation7,Citation8 and specifically in older adults.Citation9,Citation10
Physical functionality, the capacity to perform physical tasks, is a relevant construct that should be assessed in older adults.Citation11 It is correlated with HR-QOL and has also been shown to be positively predicted by participation in regular exercise.Citation9 Although widely assessed as an independent outcome, physical functionality has also been included as a proxy measure to assess frailty.Citation12–Citation14 Frailty is a clinically recognizable state of increased vulnerability to illnesses or disability caused by an age-associated decline in bodily reserve and functionality.Citation15 Relevant criteria to assess frailty have been widely debated in the literature as there is a lack of consensus on its specific components.Citation16,Citation17 Frailty is a predictor of HR-QOL,Citation18 and the literature on exercise has shown that frail individuals demonstrate improved symptoms of diseases and scores of HR-QOL when exercising regularly.Citation19
Dose–response findings
Investigating dose effects of exercise on HR-QOL and physical functionality in older adults is considered important to identify minimum levels of exercise required for effective interventions and may provide evidence to inform exercise guidelines in this population. While differences in dose could imply variation in the level of intensity or duration, national guidelines recommend exercise for a duration of 150 minutes/week at a moderate-to-vigorous level for healthy older adults.Citation2,Citation20 Using these guidelines as the recommended dose, we propose that a higher and lower dose could be compared at 20% of time (30 minutes) above and below the mark of 150 minutes/week, thus resulting in 120 minutes and 180 minutes/week at the same moderate-to-vigorous intensity as lower and higher doses, respectively. The purpose of this comparison cutoff was to test if falling below the recommended dose would still yield significant benefits compared with a control condition and if the extra efforts to go beyond the recommended dose would provide greater benefits. Reviews support evidence that physical functionality improves with regular participation in physical activity, with participation in a multicomponent training program (eg, aerobics combined with weight training workouts) providing the best results.Citation19,Citation21 However, research on the dose effect of exercise on functioning has not yielded conclusive results. Recent systematic reviews have shown some efficacy for low-dose interventions, while other studies have found no effect on improving physical functionality.Citation19,Citation21 Similarly, while there are consistent findings showing improvement in HR-QOL when exercising as per national guidelines,Citation22,Citation23 there is limited research testing the effects on HR-QOL at higher dosesCitation23,Citation24 and very little research on the effects at lower doses.
There currently appears to be some support for exercising 300 minutes/week both for physical functionality outcomesCitation25 and HR-QOL.Citation23 This level of exercise equates to nearly double the recommended level of physical activity for older adults according to national guidelines.Citation2 Albeit there are observed health benefits, prescribing 300 minutes/week is significantly demanding for older adults, even in a clinically prescribed protocol. Since reviews demonstrate improvements in frailty and HR-QOL at lower levels of exercise,Citation18 by comparison, an exploration of the minimum level of exercise required to produce meaningful changes in these outcomes is warranted. To date, no studies have tested the change in these constructs with levels of exercise that are slightly above and below the guideline levels. Identifying effects on adaptive outcomes at lower levels of exercise could serve as an incentive for older adults as it represents a more realistic exercise goal. Two recent randomized controlled trials (RCTs) primarily designed to determine the effects of 12-week exercise interventions on cognitive functioning in older adults administered the same battery of assessments including physical functionality and HR-QOL scales.Citation24,Citation26 Langlois et alCitation24 found a significant improvement in HR-QOL components in favor of the experimental group, which was prescribed to exercise 180 minutes/week, over the control group. The exercise-only arm from Desjardins-Crépeau et alCitation26 mirrored that of Langlois et al,Citation24 but participants exercised for 120 minutes/week; however, this trial did not evaluate between-group differences in physical functionality and did not analyze HR-QOL data. The exercise arms of the two trials along with a control arm were combined in the present study with the aim of comparing the levels of prescribed exercise doses (0, 120, and 180 minutes) and their effects on HR-QOL and physical functionality.
The purpose of this study was to investigate the dose effects of exercise on HR-QOL and physical functionality in a sample of older adults. The primary objective was to test the relative change in the older adults’ HR-QOL at different levels of prescribed exercise duration. We hypothesized that participants prescribed to a higher exercise dose (180 minutes/week) would report significantly higher HR-QOL over the control group and the lower-dose group (prescribed 120 minutes/ week) would not show significant improvement over indi viduals who did not receive any exercise prescription (control arm). The secondary objective was to test if higher and lower doses would differ in yielding improvements in physical functionality compared with the control condition. It was also hypothesized that improvements in physical functionality would correspond with the dose shown to improve HR-QOL. The final objective was to test if frailty would moderate the relationship between exercise dose and HR-QOL outcomes. Based on the previous findings, it was hypothesized that those who are frail would significantly benefit from greater exercise dose, which in turn would improve their HR-QOL.
Methods
Study design and participants
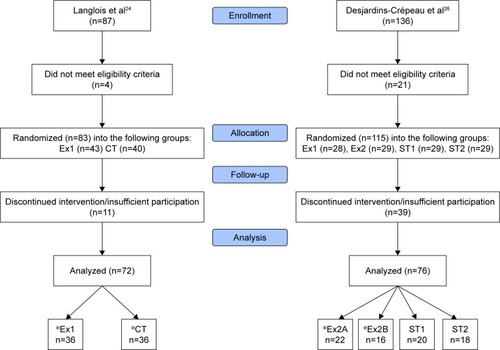
This study reports the secondary analysis of data from two recently published RCTs.Citation24,Citation26 The recruitment criteria for both studies were identical. Sedentary, community-dwelling healthy older adults (age 65+) from a large metropolitan city were recruited via public advertisements (flyers and newspapers). Participants were screened for signs of dementia (score <25 on the Mini-Mental State Examination)Citation27 or depression (score >10 on the Geriatric Depression Scale),Citation28 in addition to demonstrating any physical limitations of exercising. Finally, all potential participants were required to clear the Physical Activity and Readiness Questionnaire.Citation29 The control group (n=36), which was taken from Langlois et al’s study,Citation12 was instructed to only complete the baseline and follow-up measures. The intervention group from Langlois et al’s studyCitation12 (n=36) was instructed to engage in an exercise program for 180 minutes/week (1-hour session for 3 days). Desjardins-Crépeau et alCitation26 performed a multiple-arm trial in which two of the arms (total: n=38) undertook a multi-component exercise program identical to Langlois et al’sCitation12 intervention group with the exception that participants exercised for 120 minutes/week. Combining these samples yielded a total of 110 participants for analyses. The flowchart of both the RCTs, which identifies the groups selected for the present study, is shown in . Both intervention groups exercised in the same laboratory setting and were supervised by a kinesiologist to ensure safety and control for objective measurement of exercise time. The intervention groups undertook a multicomponent exercise session, which included aerobics (treadmill) and resistance/strength training (resistance cables). The lower- and higher-dose groups were prescribed with two and three exercise sessions/week, respectively. The protocol was built on recommendations from the literature for older adults, which included administering a multicomponent interventionCitation19,Citation21 that is delivered at an individual level.Citation18 Both studies were conducted in accordance with the Declaration of Helsinki and were ethically approved by the Research Center of the Institut Universitaire de Geriatrie de Montreal. Written informed consent was obtained from all individual participants included in the study.
Figure 1 CONSORT flow diagram of group selection.
Measures
Participants completed all of the following measures at baseline. Physical functionality and HR-QOL were also assessed at week 12.
Physical functionality
The modified Physical Performance TestCitation30 was used to assess the level of physical functionality.Citation30 This test is used for comprehensive fitness assessment that includes nine tasks rated from 0 to 4 points, with a maximum score of 36. Some of these tasks include 15-minute speed walk, picking up a coin from the floor, and standing up from a chair (five times). This test also included non-timed tasks such as performing a 360° turn and climbing up and down four flights of stairs.
Frailty
Frailty has been proposed with multiple definitions, and there is a lack of agreement on how this construct should be assessed.Citation16,Citation17 Hence, to maximize the content validity of the measures in the current study, multiple assessments were employed based on previous definitions to identify a participant as frail. This included: 1) administering Fried et al’s criteria,Citation31 which define frail as possessing any three of five frailty symptoms (muscular weakness, slow walking speed, fatigability, sedentary lifestyle, and unintentional weight loss); 2) having a score #28/36 on the modified Physical Performance Test;Citation30 and 3) assessing frailty index.Citation32 Participants were categorized as frail if they met at least two of the three criteria at the time of enrollment.
Health-related quality of life
The Quality of Life Systemic Inventory is a validated measure that assesses 28 dimensions of QOL.Citation33 Assessment procedure required participants to identify their current perceived level of each HR-QOL component followed by their ideal score on a 1–10 scale. The score discrepancy was recorded for each component. The scale possess strong test–retest reli ability of 0.88, and its subscales demonstrated convergent validity with their counterpart measuresCitation33 such as the Beck Depression Inventory,Citation34 the State-Trait Anxiety Inventory,Citation35 and the Self-efficacy Scale by Sherer et al.Citation36 However, only the HR-QOL subscale was used for the present study, which comprised leisure, physical capacity, and physical health components. The leisure component represented the ability to engage in a hobby or recreation activity without the interference of health-related symptoms. Physical capacity was defined as the ability of an individual to perform everyday tasks, and physical health reflected the experience of illness/disease symptoms in a resting state. Since all HR-QOL components were assessed and calculated on the same evaluation scale (out of 10 points), the total for each component was averaged to create an aggregated HR-QOL score.
Statistical methods
A power analysis using G Power 3.1 revealed that 99 participants would be necessary to detect a small effect size (FCitation2 of 0.15) as significant for the primary outcome in a linear multiple regression model with three groups/predictors with the alpha error probability set at 0.05 and power (1 − β error probability) adjusted to 0.90. Thus, the present study was sufficiently powered to conduct the analyses. SPSS 24.0 was used to conduct the analyses.Citation37 Although the participant sample as whole was homogenous based on screening for physical limitation and mild cognitive impairment, between-group analyses were performed to check for significant differences in demographic variables. Despite employing the same measures to assess the dependent variables in both studies, the measurement metrics, particularly in HR-QOL, used different ratio scores. Hence, comparing baseline data would provide an inaccurate comparison, which also aligns with the CONSORT statement and supporting evidence.Citation38 Rather, any discrepancies in baseline measures were controlled by calculating change score for each dependent variable by computing z-score residuals, which is a well-documented approach.Citation39–Citation41 Raw data of the samples can be found in previous papers.Citation24,Citation26 Associations between intervention group, demographic variables, and change scores of HR-QOL dimensions were first assessed by descriptive statistics and correlations (). The primary hypothesis was tested by investigating if group type would predict change in each HR-QOL component. This was performed by a series of ordinary least squares regression models by setting group type as the independent variable and group variables were dummy coded prior to analysis. The models included comparative tests between higher dose and control, lower dose and control, and higher dose and lower dose. The secondary hypothesis tested if each intervention group would predict change in physical functionality compared with the control. This was performed with separate regression models by regressing physical functionality on higher-dose and lower-dose groups.
Table 1 Bivariate correlations
We also tested our hypothesis that frailty would interact with intervention group type in the prediction of HR-QOL using hierarchical linear regression. Separate regression analyses were conducted with each HR-QOL construct at Week 12 (leisure, physical capacity, and physical health) as the dependent variable. In step 1 of the analysis, baseline HR-QOL, group (lower vs control; higher vs control), and frailty were included as independent predictors. In step 2, we included a mean-centered group × frailty interaction term as an additional predictor. Significant interaction effects were further investigated using simple slope analyses by segregating the sample into separate groups on the frailty variable (frail and non-frail) and calculating slopes representing the effect of exercise group on HR-QOL in each. Since the raw scores and z-score have been previously published for each group,Citation24,Citation26 the present study reports only effect sizes and standardized residuals.
Results
Participant characteristics
All groups were homogenous in age (F (2, 102)=0.14, P=0.871), sex (χ2=1.43, df =2, P=0.488), and frailty (χ2=1.75, df =2, P=0.418) at baseline. The age of the sample ranged from 65 to 91 years, and the mean age (SD) of the control, lower-dose, and higher-dose groups was 73.06 (SD=5.57), 71.11 (SD=6.95), and 71.44 (SD=6.81) years, respectively. Bivariate matrix () showed that all HR-QOL variables correlated with their corresponding construct at Week 12. Each HR-QOL construct also correlated with other subcomponents at the same measurement time.
Hypothesis testing
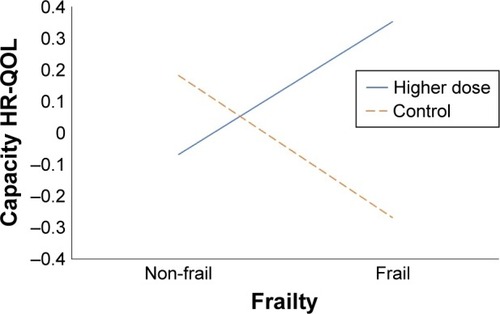
Hierarchical linear regression analyses revealed that exercise group type predicted HR-QOL dimensions (). The lower dose vs control group variable was not found to significantly predict leisure (β=0.11, P=0.371), capacity (β=0.13, P=0.265), physical health (β=0.21, P=0.077), and overall HR-QOL (β=0.23, P=0.058), with R2 values of 0.01, 0.02, 0.05, and 0.05, respectively. However, the higher dose vs control contrast found group type to show significant positive effects favoring higher doses on capacity (β=0.34, P=0.004), leisure (β=0.29. P=0.013), physical health (β=0.25, P=0.040), and overall HR-QOL (β=0.44, P=0.001) with R2 values of 0.11, 0.09, 0.06, and 0.20, respectively (). A group construct that compared both intervention groups predicted significant increase in capacity HR-QOL (β=0.25, P=0.038) with an R2 of 0.06 in favor of the higher-dose condition. The test for the secondary hypothesis found the higher dose vs control contrast to show improvement in physical functionality (β=0.31, P=0.011) with an R2 of 0.10 over the control condition; however, the lower dose did not show significant improvement over the control condition (P>0.05). Finally, the frailty interaction was tested in a hierarchical multiple regression model (). The frailty interaction model predicted change in HR-QOL capacity (F (1, 33)=4.74, P=0.037). In particular, the interaction increased the R2 from 0.06 to 0.19. Simple slope analyses revealed that group was a significant predictor in change of capacity HR-QOL among participants who were frail (β=0.53, standard error [SE] =0.37, P=0.014), but not for those who were non-frail (β=0.17, SE =0.46, P=0.497). Hence, frail individuals in the higher exercise dose condition demonstrated significant improvement in capacity HR-QOL over their non-frail counterparts.
Table 2 Results of multiple linear regression models
Figure 2 Relationship between exercise dose and change in HR-QOL.
Note: Effect size changes of HR-QOL outcomes when each exercise dose was compared with the control group.
Abbreviation: HR-QOL, health-related quality of life.
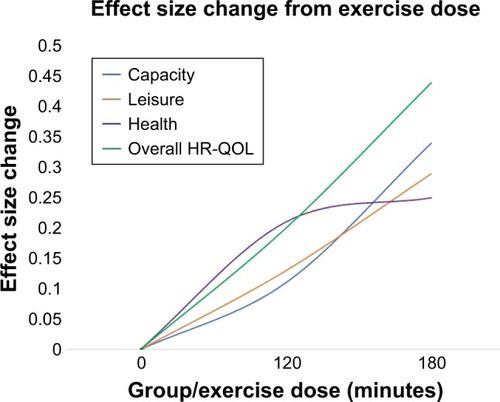
Figure 3 Exercise dose and frailty interaction.
Abbreviation: HR-QOL, health-related quality of life.
Discussion
The primary objective of this study was to test the dose– response relationship between exercise and HR-QOL, while the secondary objective was to test if exercise dose was associated with changes in a symptom of frailty (physical functionality). Finally, the tertiary objective was to test if frailty would interact between exercise dose and HR-QOL. Participating in a higher-dose exercise program was expected to be related to improvements in HR-QOL outcomes relative to lower-dose exercise programs and no exercise. Conforming to the hypothesis, the lower-dose group showed a nonsignificant improvement in HR-QOL constructs compared to the control group. However, participants in the higher-dose group demonstrated a significant improvement in each HR-QOL dimension with the change in effect size in the range of medium in magnitude.Citation42 Previous studies have distinguished prescribed doses as variability in intensity levels, showing improvement in HR-QOL in favor of greater-intensity group,Citation30,Citation43,Citation44 but the manipulation of total weekly exercise time has not been compared.
A review of exercise intervention and changes of HR-QOL concluded that evidence testing the dose–response relationship is limited, and has not identified any trials that have compared changes across different durations while controlling for the same type of exercise training.Citation18 Hence, the present findings mark as one of the first to show a continual improvement of HR-QOL components with increased exercise dose. Converting the results into a graph provided additional novel insight that showed unique patterns of each HR-QOL subcomponent. For instance, with the exception of physical health, the remaining components did not appear to show a ceiling effect at a higher exercise dose. Overall HR-QOL and the capacity subcomponent showed a positive slope with the latter demonstrating significant improvement compared to the lower-dose group. Given that HR-QOL is a distal health outcome that is predicted from the change in physical and cognitive performance,Citation45 these results suggest that participants in the higher-dose group may have benefited from improvement in various health symptoms across 12 weeks. This theorizing was further supported when testing the secondary hypothesis. The findings revealed physical functionality to show improvement corresponding to exercise dose (180 minutes/week) that predicted change in HR-QOL outcomes, though a review has identified a cluster of studies that showed significant improvement in functionality at lower exercise doses (35–120 minutes/week).Citation1 However, most of these interventions employed older-old adults (age 70+) and administered training programs that ranged from 6 to 12 months. The discrepancy in protocol designs creates some challenges when comparing changes in outcomes as the current findings reflect a 3-month training program for individuals over 60 years of age.
Finally, the third hypothesis investigated if frailty would moderate the effects of exercise dose on capacity HR-QOL. The results revealed that frail individuals showed significant improvement in capacity HR-QOL when they exercised at a higher dose. Specifically, the interaction was able to increase the variance from a small to a medium effect size.Citation46 While previous research supports frail individuals to exercise regularly,Citation19,Citation21,Citation47,Citation48 this is the first study to demonstrate that the improvements from multimodal exercise training translate to everyday activities as reflected from the capacity HR-QOL construct. While some support exists in the literature, the variability of sample (eg, nursing home, specific clinical populations) in addition to unclear details on prescribed exercise sessions in previous RCTs makes it a challenge to provide parallel comparisons. Overall, the present study addresses a call to investigate and test an optimal exercise program regarding frequency, type of exercise, and duration.Citation49 These findings are also one of the first to demonstrate that frailty interacts between exercise dose and HR-QOL with empirical data.
Strengths and limitations
A significant amount of methodological variability exists in exercise interventions for older adults, thus making it a challenge to directly compare some of our findings. The RCT groups analyzed in the present study carefully incorporated previous recommendations for conducting a robust trial for older adults, which includes the administration of multimodal exercise training for the interventionCitation19,Citation21 and employing a kinesiologist to deliver the exercise sessions.Citation19 However, the findings should not be used as outcome markers of exercising above and below the recommended guidelines.Citation20 For instance, the guidelines recommend 150 minutes of aerobic physical activity performed at a moderate-to-vigorous level in addition to resistance/weight training exercises, which would amount to a higher total recommended physical activity time/week.Citation20 The assessment of frailty is a well-documented challenge as it requires a careful multidimensional measurement approach to ensure a compressive reflection of this term.Citation15 The present study addressed this by employing a geriatrician to conduct a multi-measure assessment of this construct. Despite these strengths, the study has room for refinement. For instance, a follow-up frailty assessment at Week 12 would have allowed us to conduct predictive and change analysis with this construct. Evidence has demonstrated that exercise can reverse frailty,Citation25 and it would have been exciting to test if the higher-dose group produced a significant change in this construct, given the changes found in physical functionality. Finally, since this is one of the first studies to test exercise dose–response in HR-QOL variables among a sample of older adults, further empirical tests dedicated for dose–response analyses are warranted. Although a kinesiologist supervised the participants in the present study, Chin A Paw et alCitation19 suggested that exercising at home could be an attractive option for frail adults. Supporting this suggestion, a previous systematic review identified how exercising at home could be beneficial across all ages.Citation50 However, successfully transitioning older adults from exercising regularly in a laboratory to their home also requires further investigation.
Conclusion
Older adults who engaged in multimodal exercising training for 180 minutes/week demonstrated significant improvement in all HR-QOL outcomes compared with the control group and the capacity dimension compared with those exercising at 120 minutes/week. While numerous independent psychological and performance laboratory-based measures could be used, HR-QOL is a distal health outcome that reflects daily well-being, which provides a meaningful interpretation when dimensions of this construct are enhanced. Hence, the recovery in capacity HR-QOL among frail individuals reflects their improved experience when performing daily activities. In conjunction with the literature, engaging in any amount of exercise safely is beneficial for frail individuals. Overall, the results are encouraging to further investigate in a dedicated RCT that also includes the guideline dose as a reference arm to advance these findings.
Acknowledgments
The authors would like to thank all participants who took part in this study.
Disclosure
The authors report no conflicts of interest in this work.
References
- LangaKMLevineDAThe diagnosis and management of mild cognitive impairment: a clinical reviewJAMA2014312232551256125514304
- American College of Sports MedicineACSM’s Guidelines for Exercise Testing and Prescription10 edIndianapolisWolters Kluwer2017
- GarberCEBlissmerBDeschenesMRAmerican College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exerciseMed Sci Sports Exerc20114371334135921694556
- BhererLEricksonKILiu-AmbroseTA review of the effects of physical activity and exercise on cognitive and brain functions in older adultsJ Aging Res2013201318
- PenedoFJDahnJRExercise and well-being: a review of mental and physical health benefits associated with physical activityCurr Opin Psychiatry200518218919316639173
- CDCHealth-related quality of life2016 Available from: https://www.cdc.gov/hrqol/Accessed August 1, 2018
- KlavestrandJVingårdEThe relationship between physical activity and health-related quality of life: a systematic review of current evidenceScand J Med Sci Sports200919330019895380
- KallingsLVLeijonMHelléniusMLStåhleAPhysical activity on prescription in primary health care: a follow-up of physical activity level and quality of lifeScand J Med Sci Sports200818215416117555539
- VagettiGCBarbosa FilhoVCMoreiraNBOliveiraVMazzardoOCamposWAssociation between physical activity and quality of life in the elderly: a systematic review, 2000–2012Braz J Psychiatr20143617688
- VallanceJKEurichDTLavalleeCMJohnsonSTPhysical activity and health-related quality of life among older men: an examination of current physical activity recommendationsPrev Med2012543–423423622285441
- Chodzko-ZajkoWJProctorDNFiatarone SinghMAExercise and physical activity for older adultsMedicine and Science in Sports & Exercise20094171510153019516148
- LangloisFVuTTKergoatMJChasséKDupuisGBhererLThe multiple dimensions of frailty: physical capacity, cognition, and quality of lifeInt Psychogeriatr20122491429143622717010
- BagshawSMStelfoxHTJohnsonJALong-term association between frailty and health-related quality of life among survivors of critical illness: a prospective multicenter cohort studyCrit Care Med201543597398225668751
- ChangYWChenWLLinFGFrailty and its impact on health-related quality of life: a cross-sectional study on elder community- dwelling preventive health service usersPLoS One201275e3807922662268
- XueQLThe frailty syndrome: definition and natural historyClin Geriatr Med201127111521093718
- Rodríguez-MañasLFéartCMannGSearching for an operational definition of frailty: a Delphi method based consensus statement: the frailty operative definition-consensus conference projectJ Gerontol A Biol Sci Med Sci2013681626722511289
- BergmanHFerrucciLGuralnikJFrailty: an emerging research and clinical paradigm-issues and controversiesJ Gerontol A Biol Sci Med Sci200762773173717634320
- de VriesNMvan RavensbergCDHobbelenJSOlde RikkertMGStaalJBNijhuis-van der SandenMWEffects of physical exercise therapy on mobility, physical functioning, physical activity and quality of life in community-dwelling older adults with impaired mobility, physical disability and/or multi-morbidity: a meta-analysisAgeing Res Rev201211113614922101330
- ChinAPawMJvan UffelenJGRiphagenIvan MechelenWThe functional effects of physical exercise training in frail older people: a systematic reviewSports Med200838978179318712944
- CSEPCanadian Society for Exercise Physiology. Canadian Physical Activity GuidelinesOttawa, ONCanadian Society for Exercise Physiology2011
- TheouOStathokostasLRolandKPThe effectiveness of exercise interventions for the management of frailty: a systematic reviewJ Aging Res20112011119
- OlssonSJBörjessonMEkblom-BakEHemmingssonEHelléniusMLKallingsLVEffects of the Swedish physical activity on prescription model on health-related quality of life in overweight older adults: a randomised controlled trialBMC Public Health201515168726193882
- VallanceJEurichDGardinerPTaylorLJohnsonSAssociations of daily pedometer steps and self-reported physical activity with health-related quality of life: results from the alberta older adult health surveyJ Aging Health201628466167426486783
- LangloisFVuTTChasséKDupuisGKergoatMJBhererLBenefits of physical exercise training on cognition and quality of life in frail older adultsJ Gerontol B Psychol Sci Soc Sci201368340040422929394
- Tarazona-SantabalbinaFJGómez-CabreraMCPérez-RosPA multicomponent exercise intervention that reverses frailty and improves cognition, emotion, and social networking in the community-dwelling frail elderly: a randomized clinical trialJ Am Med Dir Assoc201617542643326947059
- Desjardins-CrépeauLBerrymanNFraserSAEffects of combined physical and cognitive training on fitness and neuropsychological outcomes in healthy older adultsClin Interv Aging2016111287129927698558
- FolsteinMFFolsteinSEMchughPR“Mini-mental state”. A practical method for grading the cognitive state of patients for the clinicianJ Psychiatr Res19751231891202204
- YesavageJABrinkTLRoseTLDevelopment and validation of a geriatric depression screening scale: a preliminary reportJ Psychiatr Res198217137497183759
- WarburtonDERBredinJamnikGGledhillNValidation of the PAR-Q+ and ePARmed-X+Health & Fitness Journal of Canada201143846
- BinderEFSchechtmanKBEhsaniAAEffects of exercise training on frailty in community-dwelling older adults: results of a randomized, controlled trialJ Am Geriatr Soc200250121921192812473001
- FriedLPTangenCMWalstonJCardiovascular Health Study Collaborative Research GroupFrailty in older adults: evidence for a phenotypeJ Gerontol A Biol Sci Med Sci2001563M146M15711253156
- RockwoodKSongXMacKnightCA global clinical measure of fitness and frailty in elderly peopleCMAJ2005173548949516129869
- DuquetteRLDupuisGPerraultJA new approach for quality of life assessment in cardiac patients: rationale and validation of the Quality of Life Systemic InventoryCan J Cardiol19941011061128111664
- BeckATWardCHMendelsonMMockJErbaughJAn inventory for measuring depressionArch Gen Psychiatry1961456157113688369
- SpielbergerCDGorsuchRLLusheneRVaggPRJacobsGAManual for the State-Trait Anxiety InventoryPalo AltoConsulting Psychologists Press1983
- ShererMMadduxJEMercandanteBPrentice-dunnSJacobsBRogersRWThe Self-efficacy Scale: Construction and validationPsychological Reports1982512663671
- IBMIBM SPSS Statistics for Windows, Version 24.0Armonk, NYIBM Corporporation2016
- de BoerMRWaterlanderWEKuijperLDSteenhuisIHTwiskJWTesting for baseline differences in randomized controlled trials: an unhealthy research behavior that is hard to eradicateInt J Behav Nutr Phys Act2015121425616598
- BuffartLMGalvãoDAChinapawMJMediators of the resistance and aerobic exercise intervention effect on physical and general health in men undergoing androgen deprivation therapy for prostate cancerCancer2014120229430124122296
- RogersLQFoglemanATrammellRInflammation and psychosocial factors mediate exercise effects on sleep quality in breast cancer survivors: pilot randomized controlled trialPsychooncology201524330231024916951
- KaushalNRhodesREMeldrumJTSpenceJCMediating mechanisms in a physical activity intervention: a test of habit formationJ Sport Exerc Psychol201840210111029945470
- CohenJA power primerPsychol Bull1992112115515919565683
- HelbostadJLSletvoldOMoe-NilssenREffects of home exercises and group training on functional abilities in home-dwelling older persons with mobility and balance problems. A randomized studyAging Clin Exp Res200416211312115195985
- HelbostadJLSletvoldOMoe-NilssenRHome training with and without additional group training in physically frail old people living at home: effect on health-related quality of life and ambulationClin Rehabil200418549850815293484
- KaushalNDesjardins-CrépeauLLangloisFBhererLThe effects of multi-component exercise training on cognitive functioning and health-related quality of life in older adultsInt J Behav Med2018617625
- FergusonCJAn effect size primer: a guide for clinicians and researchersProf Psychol2009405532538
- CadoreELRodríguez-MañasLSinclairAIzquierdoMEffects of different exercise interventions on risk of falls, gait ability, and balance in physically frail older adults: a systematic reviewRejuvenation Res201316210511423327448
- de VriesNMvan RavensbergCDHobbelenJSOlde RikkertMGStaalJBNijhuis-van der SandenMWEffects of physical exercise therapy on mobility, physical functioning, physical activity and quality of life in community-dwelling older adults with impaired mobility, physical disability and/or multi-morbidity: a meta-analysisAgeing Res Rev201211113614922101330
- FreibergerEKemmlerWSiegristMSieberCFrailty and exercise interventions: evidence and barriers for exercise programsZ Gerontol Geriatr201649760661127655437
- KaushalNRhodesREThe home physical environment and its relationship with physical activity and sedentary behavior: a systematic reviewPrev Med20146722123725084562