
Abstract
Background/aims
The pathophysiology of delirium is poorly understood. Increasing evidence suggests that different pathways might be involved in the pathophysiology depending on the population studied. The aim of the present study was to investigate potential differences in mean plasma levels of neopterin, amino acids, amino acid ratios and homovanillic acid between two groups of patients with delirium.
Methods
Data from acutely ill medical patients aged 65 years and older, and patients aged 70 years and older undergoing elective cardiac surgery, were used. Differences in biomarker levels between the groups were investigated using univariate ANOVA with adjustments for age, sex, comorbidities, C-reactive protein (CRP) and the estimated glomerular filtration rate (eGFR), where appropriate. Linear regression analysis was used to identify potential determinants of the investigated biochemical markers.
Results
Eighty patients with delirium were included (23 acutely ill medical patients and 57 elective cardiac surgery patients). After adjustment, higher mean neopterin levels (93.1 vs 47.3 nmol/L, P=0.001) and higher phenylalanine/tyrosine ratios (1.39 vs 1.15, P=0.032) were found in acutely ill medical patients when compared to elective cardiac surgery patients. CRP levels were positively correlated with neopterin levels in acutely ill medical patients, explaining 28.4% of the variance in neopterin levels. eGFR was negatively correlated with neopterin in elective cardiac surgery patients, explaining 53.7% of the variance in neopterin levels.
Conclusion
In this study, we found differences in mean neopterin levels and phenylalanine/tyrosine ratios between acutely ill medical and elective cardiac surgery patients with delirium. Moreover, our findings may suggest that in acutely ill medical patients, neopterin levels are mainly determined by inflammation/oxidative stress whereas in elective cardiac surgery patients, neopterin levels are mainly driven by renal function/fluid status. These findings suggest that the markers and pathways that might be involved in the pathophysiology of delirium may differ between specific groups of patients.
Introduction
Delirium – an acute neuropsychiatric syndrome characterized by disturbances in attention, awareness and cognition – is a frequent disorder in older hospitalized patients.Citation1–Citation3 It is associated with poor clinical outcomes including prolonged hospital stay, loss of independence, increased risk of cognitive decline and mortality.Citation4 Although it is widely accepted that the cause of delirium is multifactorial with a complex interplay between predisposing factors (eg, advanced age and dementia) and precipitating factors (eg, acute medical illness and surgery), the pathophysiology of delirium is still poorly understood.Citation3
Increasing evidence suggests that delirium might have different pathophysiological mechanisms depending on the precipitating factor and the health status of the patient (acutely ill or relatively healthy).Citation5,Citation6 Several mechanisms may play a role and include, among others, activation of the immune system, oxidative stress and disturbances in serotonergic and dopaminergic neurotransmission.Citation7 During immune system activation, monocytes and macrophages are stimulated to produce neopterin.Citation8 The association between this novel potential biomarker, neopterin, and delirium has been investigated in three previous studies which included acutely ill medical patients,Citation9 elective patients undergoing cardiac surgeryCitation10 and acute hip fracture patients undergoing surgery.Citation11 In all three studies, neopterin levels were elevated in patients with delirium. However, when comparing the results of the studies, large differences are observed in mean neopterin levels between the different studies. Considerably lower mean neopterin levels were found in surgical patients with deliriumCitation10,Citation11 than in acutely ill medical patients with delirium.Citation9 Also interestingly, neopterin levels measured in patients with delirium after cardiac surgeryCitation10 were in the same order as neopterin levels measured in acutely ill medical patients without delirium.Citation9
Disturbances in serotonergic and dopaminergic neurotransmission may also contribute to delirium.Citation7 The synthesis of serotonin in the central nervous system is, among others, dependent on the availability of its precursor, the large neutral amino acid (LNAA) tryptophan. Tryptophan competes with the other LNAAs (phenylalanine, tyrosine, valine, leucine and isoleucine) for transport across the blood–brain barrier. The amount of tryptophan that eventually enters the brain is determined by the ratio of tryptophan to the sum of the other LNAAs.Citation12 Therefore, a reduced ratio may result in a decreased synthesis of serotonin. Several studies have found decreased levels of tryptophan and tryptophan/LNAAs ratios in patients with delirium,Citation10,Citation12–Citation15 whereas other studies did not report differences in these parameters between patients with and without delirium.Citation16–Citation18
It has also been suggested that an increased dopaminergic neurotransmission plays a role in delirium. The amino acids phenylalanine and tyrosine are the precursors of dopamine and the ratios of phenylalanine and tyrosine to the other LNAAs are suggestive of the amount of phenylalanine and tyrosine that enters the brain. In patients with delirium, increased ratios,Citation17 as well as increased plasma levels of dopamine’s metabolite homovanillic acid (HVA), have been found,Citation10,Citation16 but the results are inconclusive.Citation19
In addition, serotonin and dopamine are synthesized from tryptophan, phenylalanine and tyrosine in enzymatic reactions that use tetrahydrobiopterin (BH4) as an essential cofactor.Citation20 A change in the availability of BH4 may therefore affect the synthesis of these neurotransmitters. The ratio of phenylalanine to tyrosine (Phe/Tyr ratio) can be used as an indirect measure of BH4. This ratio reflects the activity of the peripherally located enzyme phenylalanine hydroxylase, an enzyme that requires BH4 to convert phenylalanine into tyrosine.Citation20,Citation21 An increased Phe/Tyr ratio suggests a reduced availability of BH4. In a previous study, an increased ratio was found in patients with delirium,Citation19 whereas another study reported no difference between patients with and without delirium.Citation10
These controversial findings can be caused by differences in analytical procedures but can also be suggestive of potential differences in biochemical profiles and pathophysiological pathways between patient groups with delirium. Adequate knowledge regarding possible differences in the pathophysiology is required to improve delirium prevention and treatment.
The aim of this exploratory study was to investigate potential differences in mean plasma levels of neopterin, amino acids, amino acid ratios and HVA between two specific groups of patients with delirium, ie, acutely ill medical patients with delirium and patients with a delirium after elective cardiac surgery.
Methods
Study populations
In this study, we used data from the Delirium In The Old (DITO) studyCitation9,Citation19 and the DElirium pathogenesis, Cognition and Outcome (DECO) study.Citation10 In both studies, mean levels of neopterin, several amino acids, amino acid ratios and HVA in patients with and without delirium were compared and the results can be found elsewhere.Citation9,Citation10,Citation19 Only patients with delirium were included in the present study. The most relevant procedures of the two studies will be described here; detailed information can be found in previous publications.Citation9,Citation10,Citation19
The DITO study was a cross-sectional study in patients aged 65 years and older who were acutely ill and admitted to the wards of Internal Medicine and Geriatrics of the Erasmus University Medical Center (Erasmus MC) and the ward of Geriatrics of the Harbour Hospital, Rotterdam, the Netherlands. Exclusion criteria were a diagnosis of Lewy body dementia, Parkinson’s disease, neuroleptic malignant syndrome, tardive dyskinesia, ongoing treatment with antipsychotics or other psychiatric medications except haloperidol and benzodiazepines, aphasia, insufficient understanding of the Dutch language and a Mini-Mental State Examination (MMSE) score <10 points out of 30.
The DECO study was a prospective cohort study in patients aged 70 years and older who underwent elective cardiac surgery (coronary artery bypass graft [CABG], valve surgery or both) at the Department of Cardiothoracic Surgery of the Erasmus MC. Exclusion criteria were surgery in which deep hypothermia circulatory arrest or an emergency procedure was required, insufficient understanding of the Dutch language, preoperative delirium and insufficient adherence to the protocol.
In both studies, written informed consent was obtained from all participants or their representatives. The study protocols were approved by the Medical Ethics Committee of the Erasmus MC. All methods were performed in accordance with the relevant guidelines and regulations.
Procedures
In both studies, participants were assessed daily for the presence of delirium by the nursing and medical staff and by members of the research teams until discharge or until 7 days after surgery.
In the DITO study, the 13-items Delirium Observation Screening scale was used to screen for a change in behavior.Citation22 The diagnosis of delirium was made by a geriatrician, according to the criteria of the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV),Citation1 and was based on psychiatric examination of the patient, the medical and nursing records, the Delirium Observation Screening scale scores and information given by the patient’s closest relative. Cognitive functioning was assessed in the absence of delirium, at a later moment during the hospital stay, using the MMSE.Citation23 When it was impossible to score the MMSE during admission because the patient was too ill, the cognitive functioning was discussed with a clinician or assessed with information from the available medical records. When the clinical opinion was that the patient would have a MMSE score ≥10, the patient was not excluded from the study.
In the DECO study, the diagnosis of delirium was made by a senior psychiatrist and/or a trained researcher in daily assessments between 10:00 and 12:00 hours using the Confusion Assessment Method for the Intensive Care Unit (which follows the criteria for delirium of the DSM-IV)Citation24 and was based on psychiatric examination of the patient and information in the medical and nursing records. Delirium lasting >1 day was considered clinically relevant. The first day after surgery was not taken into account because of possible residual effects of anesthesia. On the day before surgery, cognitive functioning was assessed using the MMSE.
In the DITO study, blood samples were collected within 48 hours after admission. When a patient developed delirium during the hospital stay, new blood samples were collected within 24 hours after the onset of delirium and were used instead of the first blood samples for the statistical analyses. In the DECO study, blood samples were collected on the day before surgery and the second day after surgery.
In the present study, we compared the biochemical data collected in the DITO study with the postoperative biochemical data from the DECO study.
Biochemical measurements
In both studies, non-fasting blood was collected preferably between 8 and 10 am in an 8-mL tube containing ethylene diamine tetra-acetic acid. After blood sampling, the tubes were protected from light to prevent oxidative loss of neopterinCitation25 and stored at room temperature to prevent changes in the transfer of amino acids between plasma and blood cells.Citation26 Within 3 hours, the blood was centrifuged for 20 minutes at 2,650 g and 20°C. The obtained plasma was stored at −80°C until analysis.
In both studies, neopterin, amino acids and HVA were determined by the same procedures and by the same analytical staff. Plasma neopterin levels were determined by HPLC after acid oxidation.Citation21 Plasma amino acid levels were measured using HPLC with automated pre-column derivatization with ortho-phthalaldehyde,Citation26 and plasma HVA levels were determined by reversed-phase HPLC and electrochemical detection, as previously described for the measurement of serotonin.Citation27
C-reactive protein (CRP) levels and the estimated glomerular filtration rate (eGFR) were taken from the medical records. In case of the DECO study, the 2-day postoperative levels were recorded. The eGFR was determined by the following Modification of Diet in Renal Disease formula: 175 × [serum creatinine (μmol/L) × 0.0113]−1.154 × age−0.203 × 0.742 (if female).
Statistical analysis
Differences in participant characteristics between acutely ill medical and elective cardiac surgery patients with delirium were evaluated using the chi-squared test or Fisher’s exact test for categorical variables and the Mann–Whitney U-test or the Student’s t-test for continuous variables, depending on the distribution of the data.
Univariate ANOVA was used to investigate potential differences in mean levels of biochemical parameters (dependent variable) between acutely ill medical and elective cardiac surgery patients. For this purpose, biochemical parameters that were not normally distributed were logarithmically transformed (neopterin, HVA, all amino acids and amino acid ratios). Analyses were adjusted for age, sex and Charlson Comorbidity Index (CCI). The model including neopterin was additionally adjusted for CRP and eGFR, since neopterin is an inflammatory marker which is mainly excreted by the kidneys.Citation8 In additional analyses, neopterin, HVA, all amino acids and amino acid ratios were also adjusted for MMSE score. All mean levels and corresponding 95% CIs presented in this manuscript are the back-transformed log10-values.
Unadjusted linear regression analysis was performed to identify potential determinants of biochemical parameters, which were statistically significantly different between the two groups. Second, variables with a P-value ≤0.10 were included in a multiple linear regression analysis and stratified for study, to determine the relative contribution of each variable to the total variance in the biochemical parameter. Semi-partial (part) correlation coefficients were squared to calculate the percentage of total variance that was explained by each variable.
Due to the exploratory nature of this study, no correction for multiple comparisons was applied. All statistical analyses were performed using SPSS, version 21.0 (IBM Co., Armonk, NY, USA). Results were considered statistically significant at a two-sided P<0.05. Figures were constructed using GraphPad Prism 5.01 for Windows (GraphPad Software, San Diego, CA, USA).
Results
Participant characteristics
Of the 211 patients enrolled in the two studies, 81 were diagnosed with delirium. One participant from the DECO study was excluded due to withdrawal of consent. In total, 80 patients with delirium were included, 23 acutely ill medical patients and 57 elective cardiac surgery patients. Of the 23 acutely ill medical patients with delirium, 21 had delirium on admission and 2 developed delirium during the hospital stay. presents the demographic and clinical characteristics of the participants. Acutely ill medical patients with delirium were older (mean 85.9 vs 76.8 years, P<0.001), had lower MMSE scores (median 20 vs 27, P<0.001) and lower CRP levels (median 36.0 vs 100.0 mg/L, P=0.013) than elective cardiac surgery patients with delirium.
Table 1 Characteristics of the study participants
Analyses of biochemical parameters
The adjusted mean levels and corresponding 95% CIs of the investigated biochemical parameters in acutely ill medical and elective cardiac surgery patients are presented in . After adjustment for age, sex, CCI, eGFR and CRP levels, mean neopterin levels were significantly higher in acutely ill medical patients (93.1 nmol/L, 95% CI: 69.3–125.3) than in elective cardiac surgery patients (47.3 nmol/L, 95% CI: 40.1–55.8) (P=0.001). Furthermore, mean Phe/Tyr ratios were significantly higher in acutely ill medical patients (1.39, 95% CI: 1.22–1.58) than in elective cardiac surgery patients (1.15, 95% CI: 1.07–1.24) (P=0.032). No statistically significant differences were found in the mean levels of the other biochemical parameters. Estimates remained unchanged after additional adjustment for MMSE scores (Table S1).
Table 2 Adjusted mean levels of biochemical parameters
Determinants of neopterin
Unadjusted linear regression analysis revealed that neopterin levels were positively correlated with CRP levels in acutely ill medical patients with delirium and negatively correlated with eGFR in elective cardiac surgery patients with delirium (, ). Trends toward lower neopterin levels were found for increasing age (r=−0.399, P=0.060) and increasing eGFR (r=−0.396, P=0.061) in acutely ill medical patients (, ). No correlation was found between neopterin, CCI and MMSE scores in both groups of patients (P>0.10) ().
Figure 1 Scatterplots showing the relation between neopterin and age (A), CRP (B), eGFR (C) and MMSE score (D) in acutely ill medical patients with delirium (DITO) and patients with delirium after elective cardiac surgery (DECO).
Table 3 Unadjusted linear regression analyses of potential determinants of neopterin and Phe/Tyr ratio
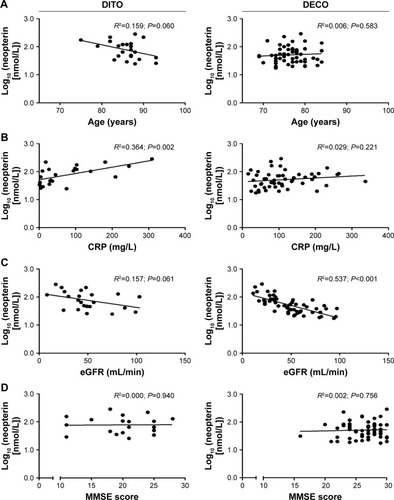
Multiple linear regression analysis revealed that a model based on age, CRP and eGFR could explain 53.2% of the variance in neopterin levels in acutely ill medical patients with delirium (). In this model, CRP levels remained positively correlated with neopterin levels and explained 28.4% of the variance in neopterin levels. Age and eGFR explained 8.53% and 3.96%, respectively of the variance in neopterin levels, but were not statistically significant determinants of neopterin. In elective cardiac surgery patients with delirium, the same model explained 56.7% of the variance in neopterin levels (). In this model, eGFR remained negatively correlated with neopterin levels and explained 53.7% of the variance in neopterin levels. Age and CRP explained 0.18% and 2.76% of the variance in neopterin levels, respectively, and were not statistically significant determinants of neopterin levels.
Table 4 Multiple linear regression analyses of potential determinants of neopterin
Determinants of Phe/Tyr ratio
Unadjusted linear regression analysis revealed that age, sex, CCI and MMSE scores were not statistically significantly correlated with Phe/Tyr ratios in both acutely ill medical and elective cardiac surgery patients with delirium (). Also no trends toward correlation were found.
Discussion
In this study, we found higher mean levels of neopterin and higher Phe/Tyr ratios in acutely ill medical patients with delirium than in patients who developed a delirium after elective cardiac surgery. These findings suggest that the markers and pathways that might be involved in the pathophysiology of delirium in acutely ill medical patients may differ from those in elective cardiac surgery patients.
Delirium frequently occurs in conditions in which the immune system is activated, and this suggests that inflammatory mediators may play a role in the pathophysiology. Several cytokines and inflammatory markers have already been found to be increased in acutely ill medicalCitation9,Citation28 and cardiac surgery patientsCitation29 with delirium. Neopterin can be considered as a marker of cell-mediated immune system activation and oxidative stress as it is primarily produced by activated monocytes and macrophages upon stimulation with the pro-inflammatory cytokine interferon-gamma (IFN-γ). Previous studies, including the DITO and DECO study, have found increased neopterin levels in plasma and cerebrospinal fluid prior to and during deliriumCitation9–Citation11 and this consistency in findings suggests that neopterin might indeed play a role in the pathophysiology of delirium. Nevertheless, in the present study we found a large difference in mean neopterin levels between acutely ill medical and elective cardiac surgery patients with delirium, where all neopterin measurements were performed in the same laboratory using identical procedures. This finding remained significant after adjustment for potential confounders.
Substantial differences in determinants of neopterin levels were found between the two groups of patients with delirium. CRP levels were the strongest determinant of neopterin levels in acutely ill medical patients with delirium, explaining 28.4% of the variance in neopterin levels, whereas the eGFR was the strongest determinant of neopterin levels, explaining 53.7% of the variance in neopterin levels, in elective cardiac surgery patients with delirium. These findings may suggest that, in acutely ill medical patients, neopterin levels are mainly determined by inflammation/oxidative stress, whereas in elective cardiac surgery patients, neopterin levels are mainly driven by renal function/fluid status. However, it should be noticed that the majority of the medical patients was admitted with an infection.
In both groups of patients with delirium, the model based on age, CRP and eGFR explained approximately half of the variance in neopterin levels and therefore the remaining variance might be determined by other factors, eg, the severity of delirium,Citation11 the presence of comorbid cognitive disorders, other medical conditionsCitation8 or the use of specific drugs, such as aspirinCitation30 and statins.Citation31 Several studies have shown that a decrease in cognitive performance is accompanied by an increase in neopterin levels.Citation32,Citation33 In the present study, we found that acutely ill medical patients with delirium had significantly lower MMSE scores than patients who developed a delirium after elective cardiac surgery, but it should be noted that in acutely ill medical patients MMSE scores were obtained after the delirium episode and therefore, the episode can have had residual effects on the MMSE score. Nevertheless, this finding might also suggest that acutely ill medical patients were cognitively more impaired than the elective cardiac surgery patients. However, when we added MMSE score as covariate to the analyses, estimates did not change and therefore, we are not able to confirm that the difference in mean neopterin levels is caused by a difference in cognitive performance between the two groups.
In the present study, we found no correlation between CRP and neopterin levels in elective cardiac surgery patients, although CRP levels were significantly higher in elective cardiac surgery patients than in acutely ill medical patients. A previous study, performed in patients who underwent CABG, showed that both CRP and neopterin levels increased after on-pump CABG, but the increase was significantly greater for CRP than for neopterin.Citation34 This finding suggests a poor correlation between CRP and neopterin after on-pump CABG, which is in line with our findings. Since CRP is produced by other cells than neopterin, it might be possible that CRP levels reflect the activity of several other components of the immune system in elective cardiac surgery patients than in acutely ill medical patients.
BH4 functions as an essential cofactor in several enzymatic reactions involved in the production of serotonin and dopamine,Citation20 two neurotransmitters that may play a role in delirium.Citation7 The Phe/Tyr ratio is an indirect measure of the BH4 status, as it reflects the activity of the enzyme phenylalanine hydroxylase, an enzyme that uses BH4 as an essential cofactor.Citation20,Citation21 An elevated ratio of phenylalanine to tyrosine might be suggestive of a decreased BH4 availability. To the best our knowledge, BH4 status in relation to delirium has only been investigated in the DITO and DECO studies. In the DITO study, an increased Phe/Tyr ratio was found in acutely ill patients with delirium compared to those without,Citation19 whereas in the DECO study, no differences were found in both the BH4 level and the Phe/Tyr ratio between patients who developed a delirium after elective cardiac surgery and those who did not.Citation10 In the present study, we found higher Phe/Tyr ratios in acutely ill medical patients with delirium than in patients who developed a delirium after elective cardiac surgery. This finding might suggest a decreased availability of the essential cofactor BH4 in the production of serotonin and dopamine in acutely ill medical patients with delirium. No determinants of the Phe/Tyr ratio could be identified.
Although we found differences in the mean levels of neopterin and Phe/Tyr ratios and in the determinants of neopterin between the two groups of patients, the potential role of these markers in the pathophysiology of delirium needs to be elucidated in future studies. It remains speculative why mean neopterin levels in surgical patients with delirium are 1) lower than mean neopterin levels in acutely ill medical patients with delirium and 2) comparable with mean neopterin levels measured in acutely ill medical patients without delirium.Citation9 This observation might suggest different threshold levels of neopterin in the development of delirium. Also, it cannot be excluded that factors other than the inflammatory response, eg, a low intraoperative perfusion pressure, hypoxia or changes in cerebral autoregulation,Citation35,Citation36 play a more dominant role in the pathogenesis of delirium after cardiac surgery. This hypothesis is in line with the results of a previous study in which the magnitude of the inflammatory response after cardiac surgery did not show a relationship with the development of postoperative cognitive dysfunction.Citation37
This study has some limitations. First, the two studies used in the present study were not developed to compare these with each other. Inclusion and exclusion criteria were different and this might have influenced the results. Although we have adjusted our analyses for several covariates, we cannot exclude residual confounding. Second, considering the relatively small groups of patients with delirium, the findings need to be confirmed in a larger study. Third, due to the exploratory nature of this study, we did not adjust for multiple comparisons; therefore, we cannot exclude the possibility that the findings were obtained by chance. Using a Bonferroni correction for multiple comparisons, a P-value <0.002 would be required to denote statistical significance. In this case, the difference in Phe/Tyr ratio would be no longer statistically significant. Fourth, it might be possible that the degree of cognitive functioning has influenced our results. Although MMSE scores were obtained after delirium in acutely ill medical patients, the delirium episode can have had residual effects on the MMSE score. However, we have adjusted our statistical analyses for the CCI; therefore, we believe that we have provided an indirect adjustment for dementia. Fifth, the blood samples in the DITO and DECO studies were not analyzed at the same time and therefore, one might speculate that this can have introduced some bias. However, we do not think that this has influenced our results. In each HPLC run, several samples of the former run were reanalyzed to check for precision. If the values were within a range of 5% of the results of the former analysis, the run was defined as good/accurate. Additionally, depending on the compound measured, all HPLC runs included external/internal standards and recovery measurements, as previously described.Citation21,Citation26,Citation27
Sixth, we used CRP as indirect marker of inflammation in the analyses performed to identify possible determinants of neopterin. However, CRP is an acute phase reactant and might be a poor marker of cell-mediated immune system activation. Therefore, it might be possible that cell-mediated immune system activation and oxidative stress have played a larger role in both patient groups. Adjustment for inflammation markers other than CRP (eg, IFN-γ) would probably have given more insights in the results.
The present study has several strengths. First, the investigated markers were determined in the same laboratory using identical procedures; therefore, potential differences in mean levels of the investigated markers due to differences in the assay are unlikely. Second, in the two studies, patients were intensively monitored for clinical symptoms of delirium and the diagnosis of delirium was made by a geriatrician or psychiatrist using DSM-IV criteria. This makes it less likely that delirium was missed or that symptoms were misdiagnosed.
Conclusion
In this study, we found that acutely ill medical patients with delirium had higher levels of neopterin and higher Phe/Tyr ratios than patients who developed delirium after elective cardiac surgery. Differences in determinants of neopterin levels were found between the two groups. Our findings may suggest that, in acutely ill medical patients, neopterin levels are mainly determined by inflammation/oxidative stress whereas in elective cardiac surgery patients, neopterin levels are mainly driven by renal function/fluid status. These findings could suggest that the markers and pathways that might be involved in the pathophysiology of delirium in acutely ill medical patients may differ from those in elective cardiac surgery patients. Longitudinal studies with repeated measurements over time are needed to investigate whether the pathophysiology of delirium is different among groups. A major step forward in delirium research would be a large study, including several health care settings (eg, surgical, medical and intensive care units), in which potential bio-markers and other factors are compared across different groups of patients.
Acknowledgments
The DITO study was supported by a research grant of Fund NutsOhra. The DECO study was funded by the Department of Psychiatry, Erasmus MC, University Medical Center Rotterdam, the Netherlands.
Disclosure
The authors report no conflicts of interests in this work.
Supplementary material
Table S1 Mean levels of biochemical parameters after additional adjustment for MMSE score
References
- American Psychiatric AssociationDiagnostic and Statistical Manual of Mental Disorders4th ed Text revisionWashington, DCAmerican Psychiatric Association2000
- American Psychiatric AssociationDiagnostic and Statistical Manual of Mental Disorders5th edArlington, VAAmerican Psychiatric Association2013
- InouyeSKWestendorpRGSaczynskiJSDelirium in elderly peopleLancet2014383992091192223992774
- WitloxJEurelingsLSde JongheJFKalisvaartKJEikelenboomPvan GoolWADelirium in elderly patients and the risk of postdischarge mortality, institutionalization, and dementia: a meta-analysisJAMA2010304444345120664045
- LagartoLCerejeiraJIdentification of sub-groups in acutely ill elderly patients with delirium: a cluster analysisInt Psychogeriatr20162881283129226972383
- van den BoogaardMKoxMQuinnKLBiomarkers associated with delirium in critically ill patients and their relation with long-term subjective cognitive dysfunction; indications for different pathways governing delirium in inflamed and noninflamed patientsCrit Care2011156R29722206727
- MaldonadoJRNeuropathogenesis of delirium: review of current etiologic theories and common pathwaysAm J Geriatr Psychiatry201321121190122224206937
- BerdowskaAZwirska-KorczalaKNeopterin measurement in clinical diagnosisJ Clin Pharm Ther200126531932911679022
- EgbertsAWijnbeldEHFekkesDNeopterin: a potential biomarker for delirium in elderly patientsDement Geriatr Cogn Disord2015391–211612425413160
- OsseRJFekkesDTulenJHHigh preoperative plasma neopterin predicts delirium after cardiac surgery in older adultsJ Am Geriatr Soc201260466166822316274
- HallRJWatneLOIdlandAVCerebrospinal fluid levels of neopterin are elevated in delirium after hip fractureJ Neuroinflammation201613117027357281
- van der MastRCvan den BroekWWFekkesDPepplinkhuizenLHabbemaJDIs delirium after cardiac surgery related to plasma amino acids and physical condition?J Neuropsychiatry Clin Neurosci2000121576310678514
- van der MastRCFekkesDMolemanPPepplinkhuizenLIs postoperative delirium related to reduced plasma tryptophan?Lancet199133887718518521681217
- PandharipandePPMorandiAAdamsJRPlasma tryptophan and tyrosine levels are independent risk factors for delirium in critically ill patientsIntensive Care Med200935111886189219588122
- RobinsonTNRaeburnCDAnglesEMMossMLow tryptophan levels are associated with postoperative delirium in the elderlyAm J Surg2008196567067418789427
- van der CammenTJTiemeierHEngelhartMJFekkesDAbnormal neurotransmitter metabolite levels in Alzheimer patients with a deliriumInt J Geriatr Psychiatry200621983884316955437
- FlackerJMLipsitzLALarge neutral amino acid changes and delirium in febrile elderly medical patientsJ Gerontol A Biol Sci Med Sci2000555B249B252 discussion B253–B24410819312
- de JongheAvan MunsterBCFekkesDvan OostenHEde RooijSEThe tryptophan depletion theory in delirium: not confirmed in elderly hip fracture patientsPsychosomatics201253323624322458995
- EgbertsAFekkesDWijnbeldEHDisturbed serotonergic neurotransmission and oxidative stress in elderly patients with deliriumDement Geriatr Cogn Dis Extra20155345045826955379
- WernerERBlauNThönyBTetrahydrobiopterin: biochemistry and pathophysiologyBiochem J2011438339741421867484
- van GoolARFekkesDKruitWHSerum amino acids, biopterin and neopterin during long-term immunotherapy with interferon-alpha in high-risk melanoma patientsPsychiatry Res20031191–212513212860366
- SchuurmansMJShortridge-BaggettLMDuursmaSAThe delirium observation screening scale: a screening instrument for deliriumRes Theory Nurs Pract2003171315012751884
- FolsteinMFFolsteinSEMcHughPR“Mini-mental state”. A practical method for grading the cognitive state of patients for the clinicianJ Psychiatr Res19751231891981202204
- ElyEWInouyeSKBernardGRDelirium in mechanically ventilated patients: validity and reliability of the confusion assessment method for the intensive care unit (CAM-ICU)JAMA2001286212703271011730446
- LaichANeurauterGWirleitnerBFuchsDDegradation of serum neopterin during daylight exposureClin Chim Acta20023221–217517812104098
- FekkesDAutomated analysis of primary amino acids in plasma by high-performance liquid chromatographyMethods Mol Biol201282818320022125146
- FekkesDTimmermanLPepplinkhuizenLEffects of clomipramine on plasma amino acids and serotonergic parameters in panic disorder and depressionEur Neuropsychopharmacol1997732352399213084
- de RooijSEvan MunsterBCKorevaarJCLeviMCytokines and acute phase response in deliriumJ Psychosom Res200762552152517467406
- KazmierskiJBanysALatekJBourkeJJaszewskiRRaised IL-2 and TNF-α concentrations are associated with postoperative delirium in patients undergoing coronary-artery bypass graft surgeryInt Psychogeriatr201426584585524345656
- EgbertsAFekkesDZiereGvan der CammenTMattace-RasoFPotential influence of aspirin on neopterin and tryptophan levels in patients with a deliriumGeriatrics20161210
- AvanzasPArroyo-EspligueroRQuilesJRoyDKaskiJCElevated serum neopterin predicts future adverse cardiac events in patients with chronic stable angina pectorisEur Heart J200526545746315684278
- ParkerDCMielkeMMYuQPlasma neopterin level as a marker of peripheral immune activation in amnestic mild cognitive impairment and Alzheimer’s diseaseInt J Geriatr Psychiatry201328214915422539447
- BlaskoIKnausGWeissECognitive deterioration in Alzheimer’s disease is accompanied by increase of plasma neopterinJ Psychiatr Res200741869470116542679
- AyazLUnluASucuNTamerLAtikUSungurMARole of neopterin, C-reactive protein and myeloperoxidase in patients undergoing cardiopulmonary bypassMed Princ Pract201019647948420881417
- SiepeMPfeifferTGieringerAIncreased systemic perfusion pressure during cardiopulmonary bypass is associated with less early postoperative cognitive dysfunction and deliriumEur J Cardiothorac Surg201140120020721168339
- HollingerASiegemundMGoettelNSteinerLAPostoperative delirium in cardiac surgery: an unavoidable menace?J Cardiothorac Vasc Anesth20152961677168726456271
- NemethEVigKRaczKInfluence of the postoperative inflammatory response on cognitive decline in elderly patients undergoing on-pump cardiac surgery: a controlled, prospective observational studyBMC Anesthesiol201717111328851286