Abstract
Background
Studies on the effect of a low intensity coordination exercise on the elderly with limited mobility are sparse. This prospective study attempted to compare the effectiveness of a customized coordination exercise and a strength exercise in improving the cognitive functioning and physical mobility on the elderly.
Methods
Participants from two centers for the elderly were allocated to practice either an 8-week coordination training (CT) program or an 8-week towel exercise (TE) program. The Chinese Mini-Mental State Examination and Chinese Dementia Rating Scale (CDRS) were used to measure cognitive functioning of participants, and Timed Up-and-Go test for physical mobility. These assessments were administered before and after the program.
Results
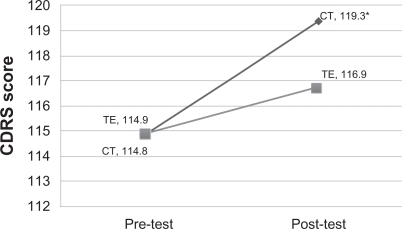
Paired t-tests showed that the CDRS scores of the CT group improved significantly from 114.8 at pre-test to 119.3 after training (P = 0.045). The CDRS scores of the TE group also improved from 114.9 at pre-test to 116.9 after training.
Conclusion
Findings from this prospective study demonstrated that low-intensity level mind-body exercise could be beneficial to the cognitive functioning of older adults.
Introduction
The benefits of physical exercise on cognitive function in the elderly have been demonstrated in many studies. Several large-scale longitudinal studies showed that older people who have a high level of physical activity, have a significantly lower risk of developing Alzheimer’s disease and cognitive impairment.Citation1–Citation7 The results of a meta-analysis of 18 studies investigating the effectiveness of aerobic exercise concluded that fitness training could enhance the cognitive functioning of the elderly.Citation8 This study also showed that a short duration, moderate-level training program could create an optimal effect on cognitive functions in the elderly. Another meta-analysis investigating the change of duration and intensity of physical activity conducted by van Gelder et al found that elderly people who participated in physical exercise for an average of 30 minutes per day or more could postpone their cognitive decline.Citation9
However, studies on the benefits of physical training have focused closely on aerobic exercise such as walking, and strength exercise, such as weight lifting.Citation4,Citation6,Citation7,Citation10–Citation12 These aerobic and strength exercises require the participants to be highly mobile. The elderly with low mobility, or who are hospitalized, might have difficulty enjoying the full benefit of the exercise because of their limited locomotive ability. Therefore exercise with reduced locomotion requirement, could provide the benefits of aerobic exercise to the elderly with restricted mobility. Recently, there has been growing research interest in the therapeutic effects of mind–body exercise.Citation13,Citation14 Tai Chi Chuan, commonly known as Tai Chi, is a typical example of mind–body exercise; it is characterized by slow motion and emphasizes the conscious control of body movements, ie, it requires less locomotive mobility and is deemed appropriate for most elderly people.Citation15 Research has shown that the cognitive functions of the elderly could be well preserved with the aid of such mind–body exercise, in a way similar to typical physical exercise.Citation3
Exercises with lower requirements of locomotive ability, such as coordination training (CT) and towel exercise (TE), are needed for the elderly with poor mobility. Both CT and TE require low locomotive ability, and thus are suitable for most elderly. The literature review showed that CT and TE may also be beneficial for the cognitive functioning of the elderly. The purpose of this study was to compare the effectiveness of CT and TE on the cognitive functioning and physical mobility of the elderly, with the aim of developing an exercise with a low mobility requirement, to benefit the cognitive functioning of the elderly. We hypothesized that the elderly in the CT group would show significant improvement in the cognitive measures compared with the elderly in the TE group.
Method
Subjects
Forty elderly (three male, 37 female) with normal cognition were recruited from two elderly centers of the Hong Kong Lutheran Social Service, aged 66–90 (mean = 79.0, SD = 5.8).
Targeted participants were asked to take the Chinese version of Mini-Mental State Examination (CMMSE) as one of the screening criteria, and those who scored ≥ 18 were eligible for this study.Citation16 Other than that, there was no other inclusion or exclusion criterion in recruitment.
The ethics approval of this study was obtained from the Survey and Behavioural Research Ethics Committee of the Chinese University of Hong Kong. Participants confirmed their agreement to participate in this study by signing informed consent before the exercise began.
Coordination training (CT)
A physiotherapist from the Jockey Club Centre for Positive Ageing (JCCPA, see http://www.jccpa.org.hk) developed an 8-week exercise program, called Coordination Training (CT), which is a simplified version of Tai Chi. It focuses on the coordination and conscious control of the body. It was easy for the elderly to learn, and required a relatively low level of mobility to practice. The eleven movements included coordination of fingers, hands, eyes, and legs. A brief description of the eleven movements is set out in . The elements of Movement 4 are tabulated in and graphically represented in as an example. Movement 4 helped to train participants’ coordination of upper limbs, and was intended to imitate the movements of Tai Chi.
Table 1 Coordination training: 11 movements
Table 2 Coordination training: Movement 4
Figure 1 Graphical illustrations of Movement 4 of the coordination training. (A) Straighten two arms and point both index fingers to the front. (B) Touch the left or right ear with corresponding index finger, while the other hand remains straight. (C) Switch and practice ten cycles (left and right) with 1 second rest (easy) or without rest (medium and hard) between each cycle.
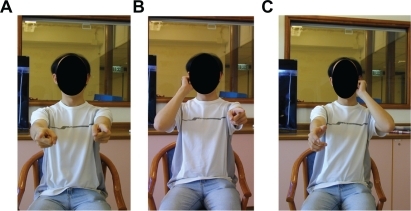
Figure 2 Changes in Chinese Dementia Rating Scale (CDRS) scores before and after the coordination training program (CT) or towel exercise program (TE) in respective groups.
Towel exercise (TE)
The training protocol of TE was developed by the Leisure and Cultural Services Department, the Government of the Hong Kong Special Administrative Region in 2005.Citation17 Similar to Movement 4 in CT, TE was a type of stretching exercise mainly to train upper limb and bilateral arm movements, but utilize a towel as a tool. It was strongly promoted by the government because it was easy for elderly people with various locomotive abilities to master.Citation18 TE benefited the elderly by improving circulation and helping to control weight, and aimed to reduce the chance of falling.Citation19
Procedure
For the sake of convenience of participation and better monitoring of participants’ progress, those in one center were allocated to practice CT, and those in another center were allocated to practice TE. TE was chosen to compare with CT because these exercies were similar in a number of ways. Both exercises required subjects to follow instructions, and to coordinate upper limb and bilateral arm movements. Yet TE did not require such fine motor coordination as CT.
CT and TE were conducted for 8 consecutive weeks, with one 40-minute session per week. Both groups had a 10-minute warm-up period at the beginning and a 10-minute cool-down period at the end of the session to prevent injury. The remaining 20 minutes would be taken up with the actual CT or TE exercise. Both exercise groups were conducted by qualified instructors trained by the physiotherapist, mentioned above.
For CT, there were three levels of difficulty: easy, medium, and difficult (see ). The level of difficulty was increased mainly by reducing the rest time (demanding higher concentration as well as physical strength of participants), and by closing the eyes when performing the actions (demanding higher psychomotor balance of participants). In this study, when the participants self-reported being able to handle the movement comfortably, which was confirmed by the trainer, they were required to practice the movement at an advanced difficulty level in order to avoid the ceiling effect.Citation19
Instruments
Assessment tools including Chinese Mini-Mental State Examination (CMMSE), Chinese Dementia Rating Scale (CDRS), and Timed Up-and-Go test (TUG) were administered to participants in both groups before and after the training sessions by trained occupational therapists and clinical psychologists.
CMMSE and CDRS were used to assess participants’ cognitive functioning. General cognitive status was assessed using the CMMSE, which was translated and validated by Chiu et al in the Hong Kong Chinese population.Citation20 The full mark was 30. The Cronbach’s alpha was 0.86. The test had excellent clinical utilities in screening general cognitive decline.
CDRS measured the level of cognitive functioning of the participants. It examined five different aspects of cognitive ability, namely, attention, initiation-perseveration, construction, conceptualization, and memory. The maximum score of the unadjusted scale was 144, with the Cronbach’s alpha of 0.89. Good psychometric properties were observed in both the original DRS and the Chinese version.Citation21,Citation22
TUG was a good instrument to measure the general physical mobility of participants, and thus was administrated in this study to measure the effects of relevant exercises.Citation23 The longer time spent to finish TUG (slower), the poorer the performance of participants, and vice versa.
Statistical analysis
SPSS software v 15 (IBM Corp, Somers, NY) was used for data analyses. Independent sample t-tests were conducted to compare the pre-test scores (obtained in pre-test period) between CT and TE groups. Paired sample t-tests were performed to compare the post-test scores (obtained in the ninth week, after the 8-week exercise period) with the pre-test scores in each group. Analysis of covariance (ANCOVA) was used to compare the scores of CMMSE, CDRS, and TUG of the two groups after the training program, using participants’ age and the pre-test scores as covariates. Statistical significant difference was set at P < 0.05.
Results
Forty people (three males, 37 females) aged 66 to 90 years (mean = 79.0, SD = 5.8) were recruited. The average ages of the elderly in the CT and TE groups were 77.7 ± 6.0 and 80.3 ± 5.5, respectively. Baseline characteristics are tabulated in . No significant difference was found in demographic features or cognitive and physical functioning test scores between the two groups.
Table 3 Baseline characteristics of participants in CT and TE groups
Comparisons of participants’ pre-test (baseline) and post-test cognitive functioning by CMMSE amd CDRS scores and physical mobility by TUG scores are shown in . Paired t-tests showed that the CDRS scores of the CT group had improved significantly from 114.8 ± 15.5 at pre-test to 119.3 ± 18.0 at post-test (CDRS t(17) = −2.25, P = 0.045). The CDRS scores of the TE group improved slightly from 114.9 ± 14.8 at pre-test to 116.9 ± 12.5 at post-test. No significant change was found in CMMSE (t(18) = −0.931, P = 0.368), and TUG (t(17) = −0.334, P = 0.747) in CT group, as well as CMMSE (t(19) = 0.665, P = 0.516), CDRS (t(19) = −0.891, P = 0.384) and TUG (t(19) = −1.908, P = 0.086) in the TE group.
Table 4 Means and standard deviations and the changes in CMMSE, CDRS, and TUG scores between pre-test (baseline) and post-test (eighth week) in CT and TE groups
Different ANCOVA (between-subject factor: group [CT, TE] and covariates: age and the pre-test scores) models show the following findings. For CMMSE, the covariate age (F(1,28) = 0.17, P = 0.690, ηp2 = 0.003) and the exercise groups (F(1,28) = 3.41, P = 0.570, ηp2 = 0.139) were not significantly related to the CMMSE post-test scores. Only the covariate pre-test scores of CMMSE were significantly related to the post-test scores (F(1,28) = 16.32, P < 0.001, ηp2 = 0.428). For CDRS, exercise groups were not significantly related to the CDRS post-test scores (F(1,28) = 0.02, P = 0.904, ηp2 = 0.001). Only the covariate age (F(1,28) = 9.14, P = 0.005, ηp2 = 0.462) and the covariate pre-test scores of CDRS (F(1,28) = 59.12, P < 0.001, ηp2 = 0.738) were significantly related to the CDRS post-test scores. For TUG, the covariate age (F(1,26) = 0.01, P = 0.940, ηp2 = <0.001) and the exercise groups (F(1,26) = 0.11, P = 0.740, ηp2 = 0.005) were not significantly related to the TUG post-test scores. Only the covariate pre-test scores of TUG were significantly related to the TUG post test scores (F(1,26) = 83.50, P < 0.001, ηp2 = 0.791).
Discussion
The above findings served to compare the effectiveness of the two exercise programs, coordination training (CT) and towel exercise (TE), in improving cognitive functioning and physical mobility in the elderly. The results showed that CT group participants had significant improvements in global cognition after the 8-week exercise program.
CT group gained significant improvement in CDRS scores after the exercise training, while the TE group participants did not. The lack of significant group difference in the changes in CDRS might be caused by the small sample size. Further investigation of the effectiveness of CT is recommended following this prospective study, through a large-scale clinical trial with appropriate numbers of samples in each group to detect the group differences.
For the physical mobility measure, TE tended to improve mobility while CT did not. This pattern was probably expected, because CT was designed to improve cognition, not mobility. There was also no significant difference between CT and TE after controlling for age. The insignificant difference in physical mobility measure might suggest that CT, which required less in mobility, had a similar effect to TE, a common physical exercise, on the cognitive and physical functioning of the elderly population. The elderly with low mobility might benefit from physical exercise by practicing CT. Further investigation is needed to confirm this observation.
Mind–body exercise to improve cognitive function
Mind–body exercise can improve cognitive functions and other health indicators, although the role of physical exercise in modulating cognitive decline is complex. The improvements can be described through (1) psychosocial indicators and (2) physiological responses.
Psychosocial indicators
Practicing regular physical exercise was found to be associated with better cognitive test performance and decreased arousal.Citation3,Citation24 A moderate exercise program followed twice a week significantly slowed, by one-third, the progressive deterioration in ability to perform activities of daily living in people with Alzheimer’s disease living in nursing homes.Citation25 Mind–body exercises produce effects similar to those of regular cardiovascular exercises, suggesting an alternative model of exercise for the elderly, who are less able to exercise vigorously, to lower the risk of sport-related injuries and cardiac hazards.Citation15 Elderly people with the habit of regular physical exercise have been shown to be associated with socialization and environmental enrichment, which may also help attenuate the rate of cognitive decline.Citation3 Tai Chi, a well-known mind–body exercise, employs cognitive tools of both visualization and focused internal awareness to strengthen, relax, and integrate the body and mind.Citation26 Tai Chi can also improve locomotion balance in seniors.Citation27,Citation28 A study evaluating a Tai Chi program called “Taiji (Tai Chi) Buddies Program” found that the program encouraged social participation and supported partner involvement, which may have a positive influence on exercise persistence and the health and well-being of the support partner.Citation28 A 12-week Tai Chi exercise program has been found adequate to reduce perceived stress and improve mood state, as well as increase perceived social support.Citation29 The findings of this research showed that CT exercise, a simplified form of Tai Chi developed in this study specifically for the elderly with low activity, shares similar advantages, improving cognitive functions.
Physiological responses to mind–body exercise
Studies reviewing the physiological responses to mind–body exercise explain this phenomenon further. Mind–body exercise enhances cardiovascular function, muscle strength, body balance, and physical function; these improvements have a positive correlation with reduced stress, anxiety, and depression, resulting in an improved quality of life.Citation24,Citation30,Citation31 A study utilizing electroencephalogram (EEG) recorded an increased cordance value at left hemisphere (a sign of enhanced cerebral perfusion) in a patient with chronic epilepsy after practicing Dejian mind–body intervention (one of the components being mind–body exercise).Citation32 The changes in brain activities reflected by EEG underlie the observed improvements in cognitive functions.Citation32 In addition, practicing mind-body exercise, which exerts similar effects to aerobic exercise, helps to increase volume in both gray and white matters primarily located in prefrontal and temporal cortices – brain areas which are involved in age-related deterioration, as observed by MRI images.Citation33 As demonstrated by animal models, exercise-induced up-active pathways are associated with enhancement of several neurotransmitter systems afferent to the hippocampus, including the norepinephrine, serotonin, acetylcholine, and γ-aminobutyric acid systems, which are important to hippocampal function.Citation34 These changes in brain activities and functioning demonstrate that regular, moderate physical exercise has beneficial effects on brain health.
The findings of this study are consistent with previous reports that have shown that subjects practicing regular physical exercise are associated with better cognitive test performance, and there is a positive correlation between cardiovascular and mind–body exercise and cognitive function among the Chinese elderly.Citation3,Citation15 These exercises, however, might not be effective for the elderly suffering from moderate and severe dementia, who are likely to be immobile or even bed-bound. The “coordination training” exercise applied in this study, which requires a lesser level of physical movement, sheds light on improving cognitive functions for dementia patients who may find difficulty undertaking regular physical exercise because they are physically less active or less mobile. Additional, large-scale randomized control studies are recommended to elaborate on the efficacy of mind–body exercise on cognitive functioning.
Limitations of this study
The limitations of the study include the small sample size, and the absence of a control group (without any exercise). Participants in this study self-reported a habit of performing regular physical activities, and thus they are likely to be more health conscious with a lower cardiovascular burden.Citation3
Conclusion
This prospective study attempted to provide evidence for the potential benefits of a customized coordination training exercise to improve the cognitive functioning of the elderly. The findings demonstrate that low physical level exercise similar to Tai Chi for example is beneficial for cognitive function and helps maintain the physical mobility of the elderly. The findings also give insight into developing further exercise regimes, which are more suitable for elderly people with a limited level of physical fitness or who are hospitalized. Additional research is encouraged to further confirm the effectiveness of the coordination training exercise.
Disclosure
The authors declare no conflicts of interest in relation to this paper.
References
- EtgenTSanderDHuntgeburthUPoppertHFörstlHBickelHPhysical activity and incident cognitive impairment in elderly persons: the INVADE studyArch Intern Med2010170218619320101014
- GedaYERobertsROKnopmanDSPhysical exercise, aging, and mild cognitive impairment: a population-based studyArch Neurol2010671808620065133
- LamLCTamCWLuiVWModality of physical exercise and cognitive function in Hong Kong older Chinese communityInt J Geriatr Psychiatry2009241485318615844
- LaurinDVerreaultRLindsayJMacPhersonKRockwoodKPhysical activity and risk of cognitive impairment and dementia in elderly personsArch Neurol200158349850411255456
- PodewilsLJGuallarEKullerLHPhysical activity, APOE genotype, and dementia risk: findings from the Cardiovascular Health Cognition StudyAm J Epidemiol2005161763965115781953
- WeuveJKangJHMansonJEBretelerMMWareJHGrodsteinFPhysical activity, including walking, and cognitive function in older womenJAMA2004292121454146115383516
- YaffeKBarnesDNevittMLuiLYCovinskyKA prospective study of physical activity and cognitive decline in elderly women: women who walkArch Intern Med2001161141703170811485502
- ColcombeSKramerAFFitness effects on the cognitive function of older adults: a meta-analytic studyPsychol Sci200314212513012661673
- van GelderBMTijhuisMAKalmijnSGiampaoliSNissinenAKromhoutDPhysical activity in relation to cognitive decline in elderly men: the FINE StudyNeurology200463122316232115623693
- Anderson-HanleyCNimonJPWestenSCCognitive health benefits of strengthening exercise for community-dwelling older adultsJ Clin Exp Neuropsychol2010329996100120408001
- CassilhasRCVianaVAGrassmannVThe impact of resistance exercise on the cognitive function of the elderlyMed Sci Sports Exerc20073981401140717762374
- HeynPAbreuBCOttenbacherKJThe effects of exercise training on elderly persons with cognitive impairment and dementia: a meta-analysisArch Phys Med Rehabil200485101694170415468033
- LanCLaiJSChenSYWongMK12-month Tai Chi training in the elderly: its effect on health fitnessMed Sci Sports Exerc19983033453519526879
- LanCLaiJSChenSYWongMKTai Chi Chuan to improve muscular strength and endurance in elderly individuals: a pilot studyArch Phys Med Rehabil200081560460710807099
- ChanASHoYCCheungMCAlbertMSChiuHFLamLCAssociation between mind-body and cardiovascular exercises and memory in older adultsJ Am Geriatr Soc200553101754176016181176
- KwokTCYChauWWYuenKSLWho would benefit from memory training? A pilot study examining the ceiling effect of concurrent cognitive stimulationClin Inter Aging2011
- Leisure and Cultural Services Department HKSARHealthy Exercise for All CampaignVirtual Class for Healthy ExerciseHong KongLeisure and Cultural Services Department HKSAR. Healthy Exercise for All Campaign2003 [updated May 23, 2007]. Available from: http://www.lcsd.gov.hk/healthy/en/virtual.php. Accessed January 15, 2011
- wenweipo.com. Available from http://paper.wenweipo.com/2004/01/19/OG0401190003.htm. Accessed January 18, 2011
- TaguchiNHigakiYInoueSKimuraHTanakaKEffects of a 12-month multicomponent exercise program on physical performance, daily physical activity, and quality of life in very elderly people with minor disabilities: an intervention studyJ Epidemiol2010201212919897943
- ChiuHFKLeeHCChungWSKwongPKReliability of validity of the Cantonese version of Mini-Mental State Examination: a preliminary studyJournal of Hong Kong College of Psychiatry199442
- ChanASChoiAChiuHLamLClinical validity of the Chinese version of Mattis Dementia Rating Scale in differentiating dementia of Alzheimer’s type in Hong KongJ Int Neuropsychol Soc200391
- ChanASPoonMWChoiACheungMCDementia Rating ScaleHong KongThe Chinese University of Hong Kong2001
- NgSSHui-ChanCWThe timed up and go test: its reliability and association with lower-limb impairments and locomotor capacities in people with chronic strokeArch Phys Med Rehabil20058681641164716084820
- La ForgeRMind-body fitness: encouraging prospects for primary and secondary preventionJ Cardiovasc Nurs199711353659095454
- RollandYPillardFKlapouszczakAExercise program for nursing home residents with Alzheimer’s disease: a 1-year randomized, controlled trialJ Am Geriatr Soc200755215816517302650
- WaynePMBuringJEDavisRBTai Chi for osteopenic women: design and rationale of a pragmatic randomized controlled trialBMC Musculoskelet Disord2010114020193083
- IvesJCSosnoffJBeyond the mind-body exercise hypePhys Sportsmed2000283678120086629
- KleinPJRiversLTaiji for individuals with Parkinson disease and their support partners: a program evaluationJ Neurol Phys Ther2006301222716630368
- Taylor-PiliaeREHaskellWLWaters CM, Froelicher ES. Change in perceived psychosocial status following a 12-week Tai Chi exercise programmeJ Adv Nurs200654331332916629916
- WangCTai chi and rheumatic diseasesRheum Dis Clin North Am2011371193221220083
- GrodsteinFCardiovascular risk factors and cognitive functionAlzheimers Dement200732 SupplS16S2219595969
- ChanASSzeSLCheungM-CLamJMShiDDejian mind-body intervention improves the functioning of a patient with chronic epilepsy: a case reportCases Journal20092908020062717
- ColcombeSJEricksonKIScalfPEAerobic exercise training increases brain volume in aging humansJ Gerontol A Biol Sci Med Sci200661111166117017167157
- MaQBeneficial effects of moderate voluntary physical exercise and its biological mechanisms on brain healthNeurosci Bull200824426527018668156