
Abstract
Purpose
We developed a simple method to minimize leg length discrepancy (LLD) during hip arthroplasty. The purpose of this study is to evaluate the accuracy of the method.
Patients and methods
A total of 47 patients who suffered from unilateral femoral neck fracture and underwent hip hemiarthroplasty between 2015 and 2018 were enrolled in this study. We measured the diameter of the contralateral femoral head (D) and the distance (L) between the center of the femoral head and the top of lesser trochanter in the antero-posterior pelvic X-ray view before the operation, the ratio (R) of D to L was calculated. During the operation, the diameter of the femoral head (d) was measured using a Vernier caliper. Then, the distance should be obtained from the center of the femoral head prosthesis to the lesser trochanter was calculated according to the contralateral ratio R.
Results
The mean LLD was 4.4±3.2 mm (−4.0 to 11.1 mm), 80.9% of the patients had LLD <6 mm, 93.6% of the patients with LLD <10 mm, only 6.4% ≥10 mm LLD.
Conclusion
This method is a simple, cost-effective, fast and accurate way to reduce the postoperative leg length discrepancy.
Introduction
With the progressive aging of the population, it is estimated that the incidence of hip fracture will reach 6.3 million all over the world by the year 2050.Citation1 Although hip arthroplasty has achieved significant pain relief and functional restoration of the hip-joint, it is still beset with defects like leg length discrepancy (LLD).Citation2–Citation6 It is reported that the incidence of LLD after hip arthroplasty is as high as 62%.Citation7 Unequal leg length can lead to lower back pain, poor gait, dislocation of hip, neurological impairment and patient dissatisfaction or even revision surgery,Citation3,Citation8–Citation10 and 15–50% of the patients may require elevated shoes.Citation4,Citation11 A survey enrolled 1114 patients undergoing total hip arthroplasties shows that LLD occurs in 30% of the patients, of which 49% are unsatisfied with the effect of operation and 4% regret having had the operation.Citation12 In addition, LLD is the second most common reason for hip arthroplasty-related litigations.Citation13 We developed a simple and effective new method to minimize LLD during such operations, with satisfactory accuracy.
Patients and methods
Ethical statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the Beijing Friendship Hospital (2019-P2-071-01). All patients provided written informed consent before participating.
Inclusion and exclusion criteria
Patients who underwent hip hemiarthroplasty (Tri-lock stem, Corail collarless standard offset/high offset stem, and bipolar femoral head; DePuy Orthopaedics, Inc, Warsaw, IN, USA and DePuy France SAS, Cedex, France) between 2015 and 2018 were retrospectively analyzed. The inclusion criteria for the patients were: 1) underwent bipolar femoral head replacement after unilateral femoral neck fracture and 2) received antero-posterior pelvic X-ray on both lower extremities at 10–15° internal rotation before and after the operation. The exclusion criteria were as follows: 1) developmental dysplasia of hip on the fractured or the contralateral side; 2) osteoarthritis, avascular necrosis of the femoral head, previous trauma or surgery, or other causes leading to a deformed femoral head that affected the accuracy of measurement; and 3) requiring increased off-set to ensure joint stability due to hemiplegia or other reasons. A total of 47 patients (19 males and 28 females) met the above criteria, with an average age of 75.9±4.5 years (68–89 years).
Methods
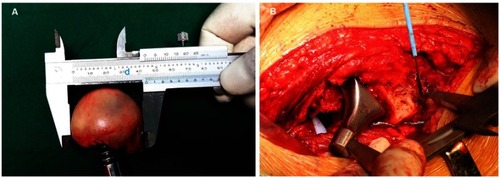
The diameter of the contralateral femoral head (D) was measured in the antero-posterior pelvic X-ray view using the picture-archiving communication system, and the center of the femoral head was marked. Since cartilage could not be visualized by X-ray, the circle for measuring the diameter of the femoral head was drawn from the middle of the gap between the superior surface of the femoral head and the acetabulum (). The distance (L) between the center of the femoral head and the top of lesser trochanter was measured, and the ratio (R) of D to L was calculated. All operations were performed with the postero-lateral approach, with exposed lesser trochanter. During the operation, the diameter of coronal plane of the femoral head (d) was measured by a Vernier caliper, and the distance from the center of the femoral head prosthesis to the lesser trochanter was calculated according to the contralateral ratio R. Then, this distance was checked using a Vernier caliper after implanting the femoral component ().
Figure 1 The diameter of the contralateral femoral head (D) and the distance between the center of the femoral head and the top of lesser trochanter (L).
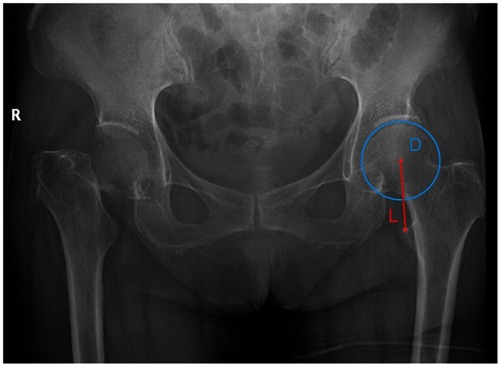
Figure 2 (A) The femoral head (d) was measured by a vernier caliper. (B) The distance should be obtained from the center of the femoral head prosthesis to the lesser trochanter during operation.
Statistical analysis
SPSS V23 software (IBM, Armonk, NY, USA) was used for statistical analysis. Kolmogorov–Smirnov test was used for checking the normality of the date. The LLD results conformed to the normal distribution and were expressed by mean and SD.
Results
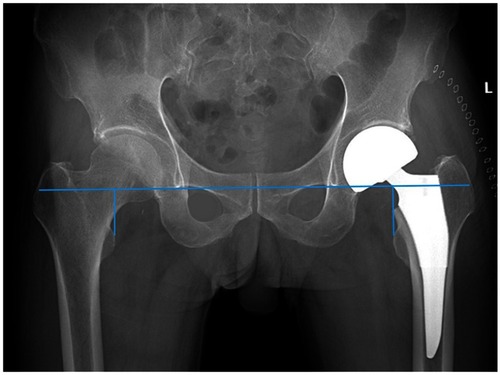
LLD was assessed according to KimCitation14 and Yu Takeda,Citation15 by measuring the vertical distances from the lower edge of the teardrop line to the lesser trochanters in the post-operational antero-posterior pelvis X-ray view (). The mean LLD between the fractured and the contralateral sides was 4.4±3.2 mm (−4.0 to 11.1 mm). We set the threshold of LLD at 6 mm according to RanawatCitation16 and Woolson’sCitation17 studies and 80.9% of the patients had LLD <6 mm. 93.6% of the patients with LLD <10 mm, only 6.4% ≥10 mm LLD.
Figure 3 Measurement of the postoperative LLD with reference to inter-teardrop line.
Discussion
There are several ways to avoid LLD after hip replacement: (1) fix Kirschner wires on bones to serve as references points, and measure the distance before and after installation of the prosthesis by a ruler or similar device,Citation5,Citation16,Citation18 (2) use a navigation system during the operation,Citation4,Citation5,Citation15,Citation19 (3) direct manual comparison of the positions of bilateral patellas or heels in surgery,Citation9,Citation20 (4) similar to our method, measure the distance between the center of the femoral head and the top of lesser trochanter of the fractured side before femoral neck osteotomy and after the prosthesis implantation,Citation21,Citation22 (5) template measuring on X-ray film before operation to confirm the osteotomy position according to the lesser trochanter or the fracture line,Citation14 and (6) compare the tip of the greater trochanter and the femoral head center during operation.Citation14
Kirschner wires or other bone-fixed markers require drilling holes on the bones, which is invasive, can cause peri-pinhole fractures.Citation9,Citation16,Citation23 Furthermore, the accuracy of this method is significantly affected by the position of the lower extremities. A previous study indicates that 5 degrees of abduction/adduction mal-positioning can cause a measurement error of almost 8 mm in the leg length.Citation24 Intraoperative navigation is more accurate, but its fixation markers may require additional skin incisions, could cause pin sit pain and irritation, even increase the risk of peri-pinhole fractures.Citation23,Citation25,Citation26 Some pinless navigation systemsCitation4,Citation27 do not require bone-fixation markers, but still need additional equipment that can increase both operation time and costs. The accuracy of the manual comparison of the position of bilateral patellas and heels is not high, which depends on the patient’s position and surgical drapes.Citation9 This method could result in 27% of patients with LLD >10 mm.Citation20 Maybe preoperative template measurement should be recommended, but its accuracy depends on the correct magnification of the X-ray filmCitation28 and the surgeon’s experience.Citation29 In addition, X-ray magnification can be approximately 15% less or 25% more in thin or obese patients, respectively.Citation28 For obese patients especially, the location of the marker may also be inaccurate.Citation14
Although the accuracy of our method cannot be compared with navigation systems, but compared with previous studies (),Citation5,Citation16,Citation18,Citation21 the accuracy is still quite satisfactory. In addition, our method is relatively simple, time-saving, cost-effective, does not require a particularly accurate preoperative magnification X-ray film and the corresponding template, or additional debugging of complex equipment. The time taken for each measurement using our method is <1 min.
Table 1 Previous reports of LLD
There are however some limitations in our study. The actual diameter of the femoral head cannot be measured accurately by X-ray due to the presence of cartilage. The circle for measuring the diameter of the femoral head was drawn through the middle of the gap between the superior surface of the femoral head and the acetabulum. According to Shepherd’s study, the superior part of femoral head cartilage thickness is 1.76+0.30 mm, and that of the corresponding acetabular part is 1.59+0.31 mm, with mean difference of 0.17 mm.Citation30 We consider this difference is much smaller than 6 mm, and may not have a significant impact on the LLD.
Acetabular position has an impact on LLD,Citation26 which is a factor that needs to be excluded when judging the accuracy of our method. So unlike other studies,Citation5,Citation16,Citation18,Citation21 we did not include total hip replacement cases in our study. But we believe that our method also helps to reduce LLD in total hip arthroplasty.
Conclusion
The method is a simple, cost-effective, fast and accurate way to reduce the postoperative LLD. It is worth of using for reference in clinical practices especially in the absence of navigation system and other high-precision measurement equipment.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Disclosure
The authors report no conflicts of interest in this work.
References
- Cooper C, Campion G, Melton LR, Hip fractures in the elderly: a world-wide projection. Osteoporos Int. 1992;2(6):285–289. doi:10.1007/bf16231841421796
- Whitehouse MR, Stefanovich-Lawbuary NS, Brunton LR, Blom AW. The impact of leg length discrepancy on patient satisfaction and functional outcome following total hip arthroplasty. J Arthroplasty. 2013;28(8):1408–1414. doi:10.1016/j.arth.2012.12.00923507069
- Renkawitz T, Weber T, Dullien S, et al. Leg length and offset differences above 5 mm after total hip arthroplasty are associated with altered gait kinematics. Gait Posture. 2016;49:196–201. doi:10.1016/j.gaitpost.2016.07.01127450670
- Weber M, Thieme M, Kaiser M, et al. Accuracy of leg length and offset restoration in femoral pinless navigation compared to navigation using a fixed pin during total hip arthroplasty. Biomed Res Int. 2018;2018:1639840. doi:10.1155/2018/163984030046589
- Grosso P, Snider M, Muir JM. A smart tool for intraoperative leg length targeting in total hip arthroplasty: a retrospective cohort study. Open Orthop J. 2016;10:490–499. doi:10.2174/187432500161001049027843511
- Kayani B, Pietrzak J, Hossain FS, Konan S, Haddad FS. Prevention of limb length discrepancy in total hip arthroplasty. Br J Hosp Med (Lond). 2017;78(7):385–390. doi:10.12968/hmed.2017.78.7.38528692359
- Kim WY. The importance of leg length discrepancy after total hip arthroplasty. J Bone Joint Surg Br. 2005;87(9):1307. doi:10.1302/0301-620X.87B8.16725
- Friberg O. Clinical symptoms and biomechanics of lumbar spine and hip joint in leg length inequality. Spine (Phila Pa 1976). 1983;8(6):643–651. doi:10.1097/00007632-198309000-000106228021
- Clark CR, Huddleston HD, Schoch ER, Thomas BJ. Leg-length discrepancy after total hip arthroplasty. J Am Acad Orthop Surg. 2006;14(1):38–45.16394166
- McWilliams AB, Lampropoulos A, Stone MH. Revision surgery for leg length inequality after primary hip replacement. Hip Int. 2018;28(5):554–558. doi:10.1177/112070001775256829865895
- Ranawat CS. The pants too short, the leg too long! Orthopedics. 1999;22(9):845–846.10507342
- Wylde V, Whitehouse SL, Taylor AH, Pattison GT, Bannister GC, Blom AW. Prevalence and functional impact of patient-perceived leg length discrepancy after hip replacement. Int Orthop. 2009;33(4):905–909. doi:10.1007/s00264-008-0563-618437379
- Zhang Y, He W, Cheng T, Zhang X. Total hip arthroplasty: leg length discrepancy affects functional outcomes and patient’s gait. Cell Biochem Biophys. 2015;72(1):215–219. doi:10.1007/s12013-014-0440-425516289
- Kim JI, Moon NH, Shin WC, Suh KT, Jeong JY. Reliable anatomical landmarks for minimizing leg-length discrepancy during hip arthroplasty using the lateral transgluteal approach for femoral neck fracture. Injury. 2017;48(11):2548–2554. doi:10.1016/j.injury.2017.08.06528882379
- Takeda Y, Fukunishi S, Nishio S, Fujihara Y, Yoshiya S. Accuracy of component orientation and leg length adjustment in total hip arthroplasty using image-free navigation. Open Orthop J. 2017;11:1432–1439. doi:10.2174/187432500171101143229387288
- Ranawat CS, Rao RR, Rodriguez JA, Bhende HS. Correction of limb-length inequality during total hip arthroplasty. J Arthroplasty. 2001;16(6):715–720. doi:10.1054/arth.2001.2444211547369
- Woolson ST, Harris WH. A method of intraoperative limb length measurement in total hip arthroplasty. Clin Orthop Relat Res. 1985;4(194):207–210.
- McGee HM, Scott JH. A simple method of obtaining equal leg length in total hip arthroplasty. Clin Orthop Relat Res. 1985;4(194):269–270.3978924
- Kitada M, Nakamura N, Iwana D, Kakimoto A, Nishii T, Sugano N. Evaluation of the accuracy of computed tomography-based navigation for femoral stem orientation and leg length discrepancy. J Arthroplasty. 2011;26(5):674–679. doi:10.1016/j.arth.2010.08.00120870379
- Nossa JM, Munoz JM, Riveros EA, Rueda G, Marquez D, Perez J. Leg length discrepancy after total hip arthroplasty: comparison of 3 intraoperative measurement methods. Hip Int. 2018;28(3):254–258. doi:10.5301/hipint.500057729192732
- Nam D, Sculco PK, Abdel MP, Alexiades MM, Figgie MP, Mayman DJ. Leg-length inequalities following THA based on surgical technique. Orthopedics. 2013;36(4):e395–e400. doi:10.3928/01477447-20130327-1123590775
- Lim YW, Chang YJ, Kwon SY, Kim YS. A simple method using a PACS to minimize leg length discrepancy in primary THA: a method to minimize leg length discrepancy. J Arthroplasty. 2013;28(10):1791–1795. doi:10.1016/j.arth.2013.02.02223540533
- Lambers AP, Salim XG, Jennings R, Bucknill AT. Morbidity and safety of iliac crest reference array pins in navigated total hip arthroplasty: a prospective cohort study. J Arthroplasty. 2018;33(5):1557–1561. doi:10.1016/j.arth.2017.12.03229352689
- Sarin VK, Pratt WR, Bradley GW. Accurate femur repositioning is critical during intraoperative total hip arthroplasty length and offset assessment. J Arthroplasty. 2005;20(7):887–891. doi:10.1016/j.arth.2004.07.00116230240
- Schmerwitz U. Total hip arthroplasty: first experiences with pinless THA software to determine leg length and offset. Orthopedics. 2007;30(10 Suppl):S124–S126.17983113
- Nishio S, Fukunishi S, Fukui T, Fujihara Y, Yoshiya S. Adjustment of leg length using imageless navigation THA software without a femoral tracker. J Orthop Sci. 2011;16(2):171–176. doi:10.1007/s00776-011-0038-221394632
- Ulivi M, Orlandini L, Pascale W, Consonni O, Sansone V. Intraoperative validation of navigated limb measurements in THA using a pinless femoral array. J Arthroplasty. 2014;29(5):1026–1029. doi:10.1016/j.arth.2013.09.03824210668
- Della VA, Padgett DE, Salvati EA. Preoperative planning for primary total hip arthroplasty. J Am Acad Orthop Surg. 2005;13(7):455–462.16272270
- Carter LW, Stovall DO, Young TR. Determination of accuracy of preoperative templating of noncemented femoral prostheses. J Arthroplasty. 1995;10(4):507–513.8523011
- Shepherd DE, Seedhom BB. Thickness of human articular cartilage in joints of the lower limb. Ann Rheum Dis. 1999;58(1):27–34. doi:10.1136/ard.58.1.2710343537