
Abstract
Purpose
The study aimed to investigate the association between body composition and frailty in elder inpatients.
Patients and Methods
This is a cross-sectional study including 656 elder inpatients (275 females and 381 males) aged ≥65 years, from department of geriatrics of Zhejiang Hospital between January 2018 and March 2019. Sociodemographic, health-related data and anthropometric measurements were evaluated. Body composition was assessed by bioimpedance analysis (BIA), mainly including skeletal muscle mass, body fat mass, total body water, fat-free mass,percent body fat, basal metabolic rate. Frailty was assessed by Clinical Frailty Scale (CFS). Univariate logistic regression was used to analyze the association between body composition and frailty.
Results
Frailty was present in 43.9% of the participants. Frail inpatients showed higher waist circumference, body fat mass and percent body fat, non-frail inpatients showed greater upper arm circumference, calf circumference, skeletal muscle mass, total body water, fat-free mass and basal metabolic rate. Subjects with underweight (body mass index (BMI)<18.5 kg/m2; odds ratio (OR), 95% confidence interval (CI)=4.146 (1.286–13.368) P=0.017) and those with high waist circumference (OR 95% CI=1.428 (0.584–3.491) P<0.001), body fat mass (OR, 95% CI=1.143 (0.892–1.315) P<0.001) presented a higher risk of frailty compared to normal subjects. Skeletal muscle mass (OR; 95% CI=0.159 (0.064–0.396) P<0.001) was a protective factor for frailty.
Conclusion
Frailty in elder Chinese inpatients was characterized by a body composition phenotype with underweight, high waist circumference, low skeletal muscle mass and high body fat mass. Underweight, abdominal obesity and sarcopenic obesity may, therefore, be targets for intervention of frailty.
Introduction
Frailty is a progressive age-related decline in physiological systems that results in decreased reserves of intrinsic capacity, which confers extreme vulnerability to stressors.Citation1–Citation3 As a result, frail old people are at increased risk of disease, disability, hospitalization and death.Citation4–Citation6 For inpatients, frailty also affects hospitalization time, expenses and mortality. However, the etiology and mechanism of frailty are not fully understood. There are several risk factors related to frailty such as aging, chronic disease, skeletal muscle disuse and cognitive function decline.Citation5,Citation7 Many studies have sought to assess frailty. The model of FriedCitation1 is most commonly used. Rockwood et alCitation2 developed Clinical Frailty Scale (CFS) and validated its ability in predicting adverse health outcomes. The CFS does not need complex questionnaire and special facilities. It has some advantages to assess frailty, especially for inpatients. For example, when the CFS assessment is performed, the patient is not required to complete a lot of actions. Although it has been used in other countries, CFS has not been fully validated in older Chinese people.
The body composition changes with age, especially in the elder people. Some studies show that body composition of the elder people is loss of muscle mass, loss of fat-free mass and increase in total fat mass.Citation8,Citation9 These changes in body composition in the elders have a great impact on the health and quality of life and expose the elders to the risk of malnutrition and could lead to conditions of disability.Citation9
The relationship between body composition and frailty is complex and unclear. Ferriolli et alCitation10 found that elder Brazilian subjects with elevated waist circumference presented a higher risk of frailty. Falsarella et alCitation11 found that frail elder people have the characteristics of lower muscle mass, lower bone mass and higher fat percentage. Reinders et alCitation12 reviewed recent literatures and found that obesity and high waist circumference show a high risk of association with frailty and the relationship between muscle mass, muscle fat infiltration and frailty remains unclear. Subjects of previous studies were mainly elder residents of the community-dwelling and little research studied the body composition of inpatients and its correlation with frailty.
The association between frailty and body composition has not been examined systematically in inpatients, although a better understanding of the pathogenesis of frailty is very important, especially for inpatients. Firstly, we compared the different characteristics of frail and non-frail inpatients. Then, we used logistic regression to investigate the association between body composition and frailty in elder inpatients. We hypothesized that low skeletal muscle mass and BMI, high body fat mass and waist circumference are high-risk factors of frailty in elder inpatients.
Materials and Methods
Study Subjects
The study used a cross-sectional design. Subjects were elder inpatients recruited from the department of geriatrics of Zhejiang Hospital between January 2018 and March 2019. The inclusion criteria were ≥65 years of age and the ability to communicate. The subjects with the following characteristics were excluded from this study: significant cognitive deficit-Mini-Mental-State-Examination (MMSE) (≤14) and poor compliance to evaluation. Inpatients with peripheral amputation and life-sustaining transplantable medical instruments such as pacemakers in the body, for whom we were unable to use the BIA analyzer due to these conditions, were also excluded. All subjects underwent anthropometric assessment and body composition evaluation by well-trained nurses. Our study was conducted in accordance with the Declaration of Helsinki and was approved by the clinical research ethics committee of Zhejiang Hospital. Written informed consent was obtained from each subject.
Instruments and Measures
Sociodemographic and Health-Related Characteristics
Sociodemographic and health-related characteristics including age, gender, hearing, eyesight, fall, comorbidity, polypharmacy, smoking history, drinking history were collected. A fall is a sudden, involuntary, unintentional change of body position, falling to the ground or a lower plane.Citation13 Comorbidities were defined as coexisting five kinds or more diseases. Participants who took five or more oral prescription medications were considered as polypharmacy.Citation14
Anthropometric Measurements
Weight (kg) was measured by a standard electronic scale and height (m) by a fixed graduation rule in the wall. Body mass index (BMI) was calculated by weight/height2, i.e., BMI=weight/height2. BMI is classified according to criteria proposed by WHO.Citation15 Underweight was defined as BMI<18.5 kg/m2, normal weight as 18.5≤BMI<25.0 kg/m2, overweight as 25≤BMI<30.0kg/m2, obesity as BMI≥30 kg/m2. Upper arm circumference was measured using a tape around the thickest part of the upper arm. Waist circumference was measured at the narrowest part of the body between the chest and hips. According to the criteria of WHO,Citation15 waist circumference of 88 cm or more (for women) and 102 cm or more (for men) was defined as abdominal obesity (high waist circumference). Calf circumference was measured in the most prominent region of the leg with the subject in a sitting position with both legs on the floor and relaxed.
Body Composition Measurements
Body composition was assessed by BIA with a body composition device, InBody S10 (BioSpace, Seoul, Korea). InBody S10 is based on multi-frequency BIA that analyzes body composition in 5 segments of the body (right upper limb, left upper limb, trunk, right lower limb, left lower limb) at 6 different frequencies (1, 5, 50, 250, 500, and 1000 kHz). The device measured the amount of skeletal muscle mass, body fat mass, total body water, fat-free mass, percent body fat and basal metabolic rate.
Frailty Measurements
In the study, frailty was assessed by CFS and determined by a geriatrician trained for scoring with the CFS scale. The CFS was assigned from 1 to 9 (1, very fit; 2, well; 3, managing well; 4, vulnerable; 5, mildly frail; 6, moderately frail; 7, severely frail; 8, very severely frail; 9, terminally ill) (2). The CFS ≥ 5 was considered as frail and CFS≤ 4 as non-frail.Citation2,Citation16
Statistical Analyses
Categorical variables were presented through percentages, while means and standard deviation were applied for continuous variables. The student’s t test (for normally distributed continuous data, such as age, height, weight, body compositions) and Chi-square test (for covariate variables, such as gender, comorbidities, polypharmacy, hearing loss, eyesight loss, fall, smoking history, drinking history and BMI categories) were used to compare the differences in the non-frail group and the frail group. Furthermore, we used the univariate logistic regression to analyze the association between frailty and body composition in total sample; and the frail status was considered as the dependent variable, those variables of P<0.1 in univariate analysis and genderCitation17 were defined as covariates. At last, after adjusting for age, gender, hearing loss, eyesight loss, fall, comorbidity and polypharmacy, the multinomial logistic regression was used to explore these two relationships. The odds ratio (OR) for significant values was calculated by using the logistic regression analysis. The analyses of all variables were calculated with a 95% confidence interval (CI) and P<0.05 was considered as statistically significant. Statistical analysis was performed using PASW Statistics (version 18.0, SPSS Inc., Chicago, IL).
Results
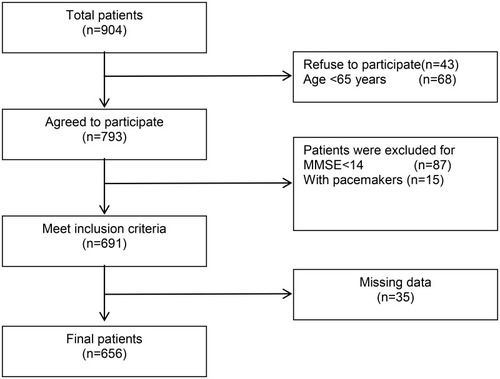
There were 904 inpatients in the department of geriatrics of Zhejiang Hospital between Jan 2018 and Mar 2019. 248 were excluded from analysis due to: refusal to participate (n=43), age <65 years (n =68), missing data (n=35), with MMSE below 14 (n=87), with pacemakers (n=15). At last, a total of 656 elder inpatients were included in this study with a mean age of 83.29±8.29 years (range: 65–100 years) (). As shown in , 368 participants (56.1%) were determined as non-frail and 288 participants (43.9%) were frail based on the CFS. Gender, weight, height, smoking and drinking were not different between frail and non-frail participants (p>0.05). Hearing loss, eyesight loss, comorbidity, polypharmacy, age and fall were more frequent in frail participants than non-frail participants (p<0.001).
Table 1 Participants’ Characteristics by Frailty Subgroups
Figure 1 Flowchart of patient inclusion.
For the body composition, frail participants showed significantly higher waist circumference, body fat mass and body fat percentage than non-frail participants (p<0.05), while non-frail participants showed significantly greater upper arm circumference, calf circumference, skeletal muscle mass, total body water, fat-free mass and basal metabolic rate than frail participants (all p<0.05, ).
shows each risk factor associated with frailty by univariate logistic regression analysis. The results indicated that age, eyesight loss, hearing loss, fall, comorbidity and polypharmacy were associated with frailty (all p<0.05). For the body composition, calf circumference, arm circumference, high waist circumference, skeletal muscle mass, body fat mass, total body water, body fat percentage, basal metabolic rate, underweight were associated with frailty (all p<0.05). However, gender and fat-free mass were not associated with frailty (p>0.05).
Table 2 Risk Factors Associated with Frailty by Univariate Logistic Regression Analysis
After adjustment of age, gender, hearing loss, eyesight loss, fall, comorbidity and polypharmacy, we found that underweight, high waist circumference, body fat mass and skeletal muscle mass were associated with frailty (). Skeletal muscle mass was a protective factor for frailty, while underweight, high waist circumference, high body fat mass were risk factors for frailty.
Table 3 Association Between Waist Circumferences, Skeletal Muscle Mass, Body Fat Mass, BMI and Frailty by Multinomial Logistic Regression
Discussion
The main findings of the present study were that frail elder inpatients had the characteristics of underweight, high waist circumference, high body fat mass and low skeletal muscle mass.
In the present study, underweight in elder inpatients was associated with an almost four-fold increased risk of developing frailty as compared to those with normal weight. However, overweight and obesity elder inpatients showed no higher risk of frailty. The relationship between frailty and BMI is discordance. Some studies showed that low BMI and obesity were both associated with a higher risk of frailty in the elders. Blaum et alCitation18 conducted a study including 599 community-dwelling adults aged 70–79 years and found obesity was significantly associated with pre-frailty and frailty. Another study identified lower BMI as risk factors for frailty in 109 community-dwelling elder women.Citation19 But other studies showed no higher risk of frailty among obese underweight/normal elder adults.Citation11,Citation20 BMI is affected by many factors, such as body size, skeletal and muscular weight, and it does not reflect the body fat distribution. Underweight may develop chronic diseases, undernourishment and sarcopenia, which were also associated with increased risk for frailty.
In general, BMI is related to general obesity and waist circumference can more accurately reflect abdominal obesity. Ramsay et alCitation21 found that frail men in British had high waist circumference when compared with non-frail men. The similar results were reported in other studies.Citation10,Citation22 Liao et alCitation23 further found that abdominal obesity is more closely associated with incidence of frailty than general obesity in the elders. Consistently, in the present study, we found that high waist circumference and body fat mass in elder inpatients were risk factors for frailty. Abdominal obesity is associated with systemic inflammation, oxidative stress and insulin resistance.Citation24,Citation25 Abdominal obesity is also related to cardiovascular disease and diabetes. It is known that adipose tissue is a metabolic tissue that secretes hormones and proteins. For example, it produces cytokines such as leptin, adiponectin, resisting, Tumor necrosis factor, interleukin-6 and visfatin. Increased inflammation and insulin resistance contribute to decline of muscle mass and strength,Citation26–Citation28 which have been proposed to mediate the mechanisms leading to frailty.
Spira et alCitation29 studied the association between appendicular lean mass and frailty status in a sample of community-dwelling elder adults and found that low appendicular lean mass was associated with a 2.4-times increase of risk of prefrail or frail. Idoate et alCitation30 found that 29 frail elder adults had lower-dense muscle tissue when compared to 13 non-frail older adults. But Williams et alCitation31 only found a weak association between muscle mass and frailty in the sample of elder adults with cancer. Makizako et alCitation32 found that social frailty was not independently associated with loss of skeletal muscle mass after adjusting for covariates. In the present study, skeletal muscle mass in frail inpatients was less than that in non-frail inpatients. Skeletal muscle mass is important for the health of the elders. Low skeletal muscle mass is related to the decline in the nutritional, functional, endocrine and cognitive status while higher muscle mass is associated with better survival in the elders,Citation33 which may be one reason for the higher comorbidity in frail inpatients in the present study.
In the present study, frail patients had high body fat mass and low skeletal muscle mass. Some studies have described this symptom as “sarcopenic obesity”. The pathogenesis of sarcopenic obesity is complex, with an interplay between aging, lifestyle, hormones, oxidative stress, neuromuscular changes, vascular and immunological factors.Citation34,Citation35 Sarcopenic obesity may affect the disorders of metabolism, physical capacity, and quality of life.Citation34 The combination of high body fat mass and low skeletal muscle mass would be more strongly associated with health risk and disability than either condition alone.Citation36 Hirani et alCitation37 found that men with sarcopenic obesity had an increased risk of frailty. Jarosz et alCitation38 also thought that sarcopenic obesity is an emerging cause of frailty in elder adults.
Thus, the present study supports the view that the effect of body composition on frailty is mainly through three pathways. The first one is underweight to develop chronic diseases, undernourishment and sarcopenia. The second one is sarcopenic obesity which may affect physical capacity and result disorders of metabolism. The last one is abdominal obesity, involving inflammation, oxidative stress, insulin resistance, cardiovascular disease and diabetes as the primary causes.
It should be pointed out that the frailty prevalence in the present study was higher than previous reports,Citation1,Citation2 which may be attributed by elder and hospitalized participants in the present study. Because of the different definitions of frailty, inclusion criteria, exclusion criteria, areas, genders, ages, the prevalence of frailty may be widely differing between studies. In a systematic review, a total of 21 studies reported frailty prevalence rates of 4.0–59.1%.Citation39 There were also some other limitations in the present study and its results should be viewed with caution. This is a cross-sectional study, and the associations observed could not establish a causal nexus between the studied variables and frailty. Our study was an observational research and subjects were from one hospital, which may limit the potential for extrapolating study results. A lot of factors were included in the present study, we cannot exclude some residual confounding influence due to co-morbid conditions. Further prospective studies are needed to explore the association between frailty and body composition.
Conclusion
This study highlights the relationship of body composition with frailty. The body composition of the frail elder inpatients was found to be characterized by low skeletal muscle mass, underweight and high body fat mass, high waist circumference compared with the non-frail inpatients. Underweight, abdominal obesity and sarcopenic obesity may, therefore, be targets for intervention for frailty.
Acknowledgments
The study was supported by funds from Zhejiang Medical Science and Technology Project (2017KY177,2018KY198,2018ZH001,2019KY004,2019KY261).
Disclosure
The authors report no conflicts of interest in this work.
References
- Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol a Biol Sci Med Sci. 2001;56(3):M146–156. doi:10.1093/gerona/56.3.M14611253156
- Rockwood K, Song XW, MacKnight C, et al. A global clinical measure of fitness and frailty in elderly people. CMAJ. 2005;173(5):489–495. doi:10.1503/cmaj.05005116129869
- WHO. World Report On Ageing And Health. Geneva, Switzerland: World Health Organization; 2015.
- Gale CR, Cooper C, Sayer AA. Prevalence of frailty and disability: findings from the English longitudinal study of ageing. Age Ageing. 2015;44(1):162–165. doi:10.1093/ageing/afu14825313241
- Runzer-Colmenares FM, Samper-Ternent R, Al SS, Ottenbacher KJ, Parodi JF, Wong R. Prevalence and factors associated with frailty among Peruvian older adults. Arch Gerontol Geriatr. 2014;58(1):69–73. doi:10.1016/j.archger.2013.07.00523978328
- González-Vaca J, de la Rica-escuín M, Silva-Iglesias M, et al. Frailty in institutionalized older adults from albacete. The final study: rationale, design, methodology, prevalence and attributes. Maturitas. 2014;77(1):78–84. doi:10.1016/j.maturitas.2013.10.00524189222
- Eyigor S, Kutsal YG, Duran E, et al. Frailty prevalence and related factors in the older adult-FrailTURK Project. Age. 2015;37(3):9791. doi:10.1007/s11357-015-9791-z25948502
- Buffa R, Floris GU, Putzu PF, Marini E. Body composition variations in ageing. Coll Antropol. 2011;35(1):259–265.
- Genton L, Karsegard VL, Chevalley T, Kossovsky MP, Darmon P, Pichard C. Body composition changes over 9 years in healthy elderly subjects and impact of physical activity. Clin Nutr. 2011;30(4):436–442. doi:10.1016/j.clnu.2011.01.00921324569
- Ferriolli E, Pessanha FPADS, Moreira VG, Dias RC, Neri AL, Lourenço RA. Body composition and frailty profiles in Brazilian older people: frailty in Brazilian older people study-FIBRA-BR. Arch Gerontol Geriatr. 2017;71:99–104. doi:10.1016/j.archger.2017.03.00828395196
- Falsarella GR, Gasparotto LPR, Barcelos CC, et al. Body composition as a frailty marker for the elderly community. Clin Interv Aging. 2015;10:1661–1666. doi:10.2147/CIA26527868
- Reinders I, Visser M, Schaap L. Body weight and body composition in old age and their relationship with frailty. Curr Opin Clin Nutr Metab Care. 2017;20(1):11–15. doi:10.1097/MCO.000000000000033227749713
- Lamb SE, Jorstad-Stein EC, Hauer K, Becker C. Development of a common outcome data set for fall injury prevention trials: the prevention of falls Network Europe consensus. J Am Geriatr Soc. 2005;53(9):1618–1622. doi:10.1111/j.1532-5415.2005.53455.x16137297
- Viktil KK, Blix HS, Moger TA, Reikvam A. Polypharmacy as commonly defined is an indicator of limited value in the assessment of drug-related problems. Br J Clin Pharmacol. 2007;63(2):187–195. doi:10.1111/bcp.2007.63.issue-216939529
- WHO. Waist Circumference and Waist–Hip Ratio: Report of a WHO Expert Consultation. Geneve: WHO; 2008.
- Kahlon S, Pederson J, Majumdar SR, et al. Association between frailty and 30-day outcomes after discharge from hospital. CMAJ. 2015;187(11):799–804. doi:10.1503/cmaj.15010026009583
- Bredella MA. Sex differences in body composition. Adv Exp Med Biol. 2017;1043:9–27.29224088
- Blaum CS, Xue QL, Michelon E, Semba RD, Fried LP. The association between obesity and the frailty syndrome in older women: the women’s health and aging studies. J Am Geriatr Soc. 2005;53(6):927–934. doi:10.1111/jgs.2005.53.issue-615935013
- Sewo Sampaio PY, Sampaio RA, Coelho Júnior HJ, et al. Differences in lifestyle, physical performance and quality of life between frail and robust Brazilian community-dwelling elderly women. Geriatr Gerontol Int. 2016;16(7):829–835. doi:10.1093/gerona/60.10.127826245307
- Woo J, Yu R, Wong M, Yeung F, Wong M, Lum C. Frailty screening in the community using the FRAIL scale. J Am Med Dir Assoc. 2015;16(5):412–419. doi:10.1016/j.jamda.2015.01.08725732832
- Ramsay SE, Arianayagam DS, Whincup PH, et al. Cardiovascular risk profile and frailty in a population-based study of older British men. Heart. 2015;101(8):616–622. doi:10.1136/heartjnl-2014-30647225480883
- Vieira RA, Guerra RO, Giacomin KC, et al. Prevalence of frailty and associated factors in community-dwelling elderly in Belo Horizonte, Minas Gerais State, Brazil: data from the FIBRA study. Cad Saude Publica. 2013;29(8):1631–1643. doi:10.1590/S0102-311X201300120001524005928
- Liao QJ, Zheng Z, Xiu SL, Chan P. Waist circumference is a better predictor of risk for frailty than BMI in the community-dwelling elderly in Beijing. Aging Clin Exp Res. 2018;30(11):1319–1325. doi:10.1007/s40520-018-0933-x29589287
- Zuliani G, Volpato S, Galvani M, et al. Elevated C-reactive protein levels and metabolic syndrome in the elderly: the role of central obesity data from the InChianti study. Atherosclerosis. 2009;203(2):626–632. doi:10.1016/j.atherosclerosis.2008.07.03818845301
- Ershler WB. A gripping reality: oxidative stress, inflammation, and the pathway to frailty. J Appl Physiol. 2007;103(1):3–5. doi:10.1152/japplphysiol.00375.200717431088
- Schaap LA, Pluijm SM, Deeg DJ, et al. Higher inflammatory marker levels in older persons: associations with 5-year change in muscle mass and muscle strength. J Gerontol a Biol Sci Med Sci. 2009;64(11):1183–1189. doi:10.1093/gerona/glp09719622801
- Abbatecola AM, Ferrucci L, Ceda G, et al. Insulin resistance and muscle strength in older persons. J Gerontol a Biol Sci Med Sci. 2005;60(10):1278–1282.16282559
- Barzilay JI, Cotsonis GA, Walston J, et al. Insulin resistance is associated with decreased quadriceps muscle strength in nondiabetic adults aged >or=70 years. Diabetes Care. 2009;32(4):736–738. doi:10.2337/dc08-178119171728
- Spira D, Buchmann N, Nikolov J, et al. Association of low lean mass with frailty and physical performance: a comparison between two operational definitions of sarcopenia-data from the berlin aging study II (BASE-II). J Gerontol a Biol Sci Med Sci. 2015;70(6):779–784. doi:10.1093/gerona/glu24625638537
- Idoate F, Cadore EL, Casas-Herrero A, et al. Adipose tissue compartments, muscle mass, muscle fat infiltration, and coronary calcium in institutionalized frail nonagenarians. Eur Radiol. 2015;25(7):2163–2175. doi:10.1007/s00330-014-3555-525510447
- Williams GR, Deal AM, Muss HB, et al. Frailty and skeletal muscle in older adults with cancer. J Geriatr Oncol. 2018;9(1):68–73. doi:10.1016/j.jgo.2017.08.00228844849
- Makizako H, Kubozono T, Kiyama R, et al. Associations of social frailty with loss of muscle mass and muscle weakness among community-dwelling older adults. Geriatr Gerontol Int. 2019;19(1):76–80. doi:10.1111/ggi.1357130575241
- Han SS, Kim KW, Kim KI, et al. Lean mass index: a better predictor of mortality than body mass index in elderly Asians. J Am Geriatr Soc. 2010;58(2):312–317. doi:10.1111/j.1532-5415.2009.02672.x20070416
- Polyzos SA, Margioris AN. Sarcopenic obesity. Hormones (Athens). 2018;17(3):321–331. doi:10.1007/s42000-018-0049-x30014320
- Molino S, Dossena M, Buonocore D, Verri M. Sarcopenic obesity: an appraisal of the current status of knowledge and management in elderly people. J Nutr Health Aging. 2016;20(7):780–788. doi:10.1007/s12603-015-0631-827499312
- Roubenoff R. Sarcopenic obesity: the confluence of two epidemics. Obes Res. 2004;12(6):887–888. doi:10.1038/oby.2004.10715229325
- Hirani V, Naganathan V, Blyth F, et al. Longitudinal associations between body composition, sarcopenic obesity and outcomes of frailty, disability, institutionalisation and mortality in community-dwelling older men: the concord health and ageing in men project. Age Ageing. 2017;46(3):413–420. doi:10.1093/ageing/afw21427932368
- Jarosz PA, Bellar A. Sarcopenic obesity: an emerging cause of frailty in older adults. Geriatr Nurs. 2009;30(1):64–70. doi:10.1016/j.gerinurse.2008.02.01019226689
- Collard RM, Boter H, Schoevers RA, Oude Voshaar RC. Prevalence of frailty in community-dwelling older persons: a systematic review. J Am Geriatr Soc. 2012;60(8):1487–1492. doi:10.1111/jgs.2012.60.issue-822881367