Abstract
Background
The aim of this study was to examine the trend in increasing life expectancy in relation to heart attack and cardiac catheterization.
Methods
A retrospective study of very elderly patients over 90 years of age (study group) and between 70 and 79 years of age (control group) with myocardial infarction and acute coronary syndrome who underwent coronary angiography was conducted.
Results
A total of 1100 cardiac catheterizations were performed in the cardiac catheterization laboratory of Vinzentius-Hospital in Landau, Germany from 2007 to 2011. The number of coronary angiographies performed in patients aged over 90 years and those aged 70–79 years was 36 and 354, respectively, during this same time period. No increase in the number of evidence-based therapy for coronary heart disease by cardiac catheterization was observed in the very elderly patients over this time period.
Conclusion
An increase in the number of patients aged over 90 years and a rise in heart attacks, as evaluated by coronary angiography, could not be found in this study.
Introduction
An increase in life expectancy has been reported in developed countries and the result will be an aging population.Citation1 A consequence of this development is an increase in heart attacks in older people.
Despite the extensive published information regarding the treatment of acute coronary syndrome (ACS), there are few data available for the guidance and evaluation of ACS management in the elderly, since only a minority of published clinical trials include elderly patients.Citation2 Even when elderly patients are enrolled in clinical trials, they typically account for a disproportionately small portion of the study population, and age-subset-specific results are often not reported.Citation3,Citation4 Indeed, patients older than 75 years of age comprise only 9% of clinical trial populations, and only about 50% of trials enroll patients above the age of 75 years.Citation5 Data guiding coronary reperfusion in elderly ACS patients are limited and consist mostly of subset analyses from major trials and retrospective studies.Citation6
According to guidelines, patients with non-ST-elevation myocardial infarction (NSTEMI) and acute ST-segment elevation myocardial infarction (STEMI) on the electrocardiogram should undergo a primary percutaneous coronary intervention.Citation7 Although no age limit for this treatment is specified in the guidelines, older patients with myocardial infarction are less often treated with invasive treatment.Citation8 The most common cause of death in developed countries is ischemic heart disease in patients over 65 years of age.Citation9 This is most evident in Europe, where the aging of the population has led to an increase in coronary heart disease.Citation10 This current trend is expected to continue with the increase in life expectancy. Citation10 This study investigates the trend of increasing life expectancy in relation to myocardial infarction and left heart catheterization.
Methods
Study groups
This study was retrospective, and examined patients aged 90–100 years (study group) with angina pectoris, NSTEMI, and acute STEMI on an electrocardiogram. These patients were compared with patients between 70 and 79 years of age who had the same symptoms and diagnoses (control group) from 2007 to 2011. In total, 1100 patients were evaluated during this time period. All patients in this study underwent coronary angiography. The cardiovascular risk factors examined were elevated blood pressure, diabetes mellitus, hyperlipidemia, obesity, smoking, and a family history of cardiovascular disease. Comorbidities and the length of hospital stay of patients admitted to hospital were also compared between the two groups. All patients with myocardial infarction were treated with a loading dose of aspirin (500 mg), clopidogrel (300 mg), and a single dose of heparin (5000 IU), followed by a typical daily dose of aspirin and clopidogrel. A major adverse cardiac event was defined as death, history of stroke, or myocardial infarction.
Statistical analysis
The confidence interval of a proportion was calculated given the necessary size of this study and results. The Kolmogorov– Smirnov test was used to compare the length of the hospital stay. The survival rate for both groups was calculated using the Kaplan–Maier method and comparison of gender distribution among groups was calculated using the Kruskal–Wallis test. Data were checked afterwards for normality using the Kolmogorov–Smirnov test. A P value of <0.05 was considered statistically significant. Mean and standard deviation (SD) were also calculated.
Results
Primary percutaneous coronary intervention
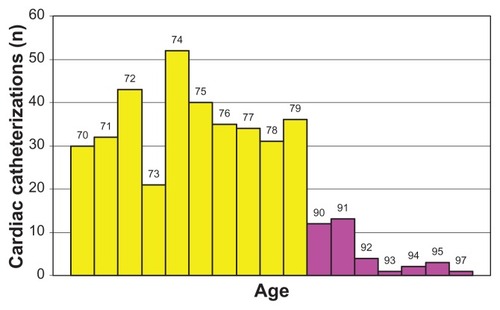
A total of 1100 left heart catheterizations were performed in this Vinzentius-Hospital in Landau, Germany from 2007 to 2011. Only 36 (3.27%) patients over 90 years of age were treated by cardiac catheterization from 2007 to 2011, whereas 354 (32.18%) patients aged 70–79 years underwent coronary angiography in the same time period. In 2007, 39 coronary angiographies were carried out, with four (10.26%) and six (15.38%) of them performed in the study and control groups, respectively. In 2008, the number of invasive examinations significantly increased to 231. Eight (3.46%) and 81 (35.06%) patients in the study and control groups, respectively, underwent coronary angiography. In 2009, 15 (4.63%) patients in the study group and 111 (34.26%) in the control group from a total of 324 invasive treatments underwent coronary angiography. A slight decline in numbers of coronary angiographies to a total of 283 was observed in 2010, thus, seven (2.47%) patients in the study group and 89 (31.45%) in the control group were examined. Finally, the number of invasive investigations decreased to 223 in 2011 (). This decrease was observed in both groups. Two (0.90%) patients in the study group and 67 (30.04%) in the control group were treated by coronary angiography.
Figure 1 The number of cardiac catheterizations in the two groups: 70 to 79 years of age and 90 to 97 years of age in 2007–2011.
Age and gender distribution
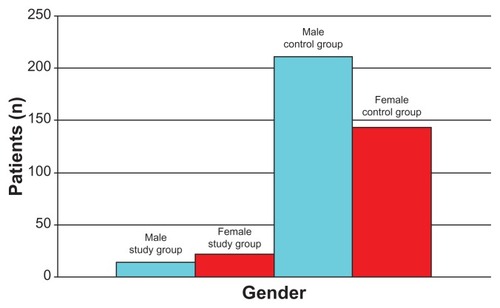
The mean age of the study and control groups was 91.5 (SD ± 1.8) and 74.6 (SD ± 2.8) years, respectively. The oldest patient was a 97-year-old man. Among the 36 patients in the study group, 14 (38.89%) men and 22 (61.11%) women underwent cardiac catheterization, whereas 211 (59.60%) men and 143 (40.40%) women underwent the procedure in the control group (). According to the Kruskal–Wallis test, significantly more women than men underwent cardiac catheterization in the study group, whereas more men than women underwent the procedure in the control group.
Figure 2 The gender distribution of the two groups.
Clinical appearance
Most cases of 235 (60.26%) were ACS. Nine (3.83%) were in the study group, whereas 226 (96.17%) were in the control group. Meanwhile, 134 (34.36%) patients had NSTEMI, with 25 (18.66%) patients and 109 (81.34%) in the study and control groups, respectively. At least 21 (5.38%) patients had STEMI: two (9.52%) in the study group and 19 (90.48%) in the control group. In the control group, coronary angiography was performed because of abnormal ergometry in four patients.
Cardiovascular risk factors
Among the 36 patients in the study group, 30 (83.33%) had hypertension, 18 (50%) diabetes, six (16.67%) hyperlipidemia, and four (11.11%) were obese. One patient smoked. Among the 354 patients in the control group, 296 (83.62%) had hypertension, 194 (54.80%) diabetes, 159 (44.92%) hyperlipidemia, 64 (18.08%) were obese, 54 (15.25%) had a nicotine habit, and 17 (4.8%) had a positive family history for cardiovascular disease.
Coronary heart disease
A total of 271 (69.49%) patients in both groups had coronary heart disease. Of these, 30 (11.07%) and 241 (88.93%) were in the study and control groups, respectively. In contrast, only 95 (24.36%) patients had no coronary artery disease. Five (5.26%) of these patients were in the study group, while 90 (94.74%) were in the control group. Nineteen (4.87%) patients in the control group and five (1.28%) in the study group had coronary atherosclerosis.
Length of hospital stay
The average length of the hospital stay was 12.6 (SD ± 8.154) days in the study group and 8 (SD ± 5.669) days in the control group. The Kolmogorov–Smirnov test showed that the normal distribution in the study and control groups was 4.566 and 33.762, respectively, with a significant deviation of at least 99% from a normal distribution.
Comorbidities
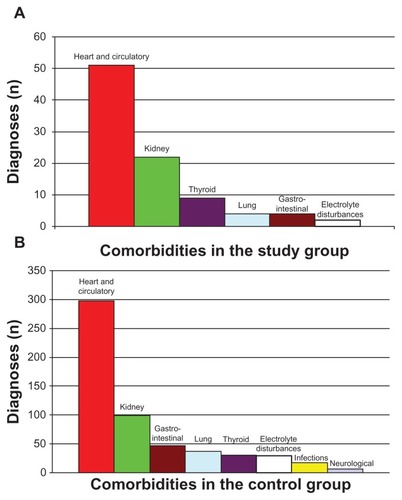
The accompanying diseases in the study group involved heart and circulatory (51 diagnoses), kidney (22), thyroid (9), lung (4), gastrointestinal (4), and electrolyte disturbances (2). Meanwhile, the comorbidities in the control group were heart and circulatory (298 diagnoses), kidney (99), gastrointestinal (47), lung (37), thyroid (31), electrolyte disturbances (29), infections (17), and neurological disorders (7) ().
Figure 3 The various comorbidities in the two groups over the last few years. (A) Study group; (B) Control group.
Major adverse cardiac event
In the study group, one patient had a history of stroke compared with 47 patients in the control group. Among the 36 patients in the study group, no deaths occurred, so the probability of survival using the Kaplan–Meier method was 100% (95% confidence interval [CI]: 100%–100%). In the control group, 3/351 died, giving a probability of survival of 99.15% (95% CI: 98.19%–100%).
Discussion
An increase in the number of coronary angiographies was observed in both groups; however, a continuous increase was not detected in this present study. From 2007 to 2011, ~10% of the angiographies in this study were performed in patients aged 90 years or older relative to the control group.
NSTEMI occurred most frequently in the study group, whereas ACS was more common in the control group. Elderly ACS patients are more likely to have comorbid conditions such as diabetes mellitus, renal insufficiency, cerebrovascular disease, and heart failure.Citation11,Citation12 Moreover, limited functional capacity and dementia are also more common within this group of patients, so that these factors must be taken into account in management decisions.Citation11,Citation12 Further, in a previous study by Tespili et al, elderly patients, who were primarily female, had more comorbidities and more extensive cardiovascular disease prior to stroke.Citation13 In this current study, however, the cardiovascular risk factors differed only slightly between the two groups, but older patients in the study group had more comorbidities (), while stroke and death was more common in the control group. The probability of survival was markably better in the study group. Finally, the study group had a higher proportion of women than men.
According to recent studies, invasive therapy significantly improves the survival of elderly patients with acute myocardial infarction.Citation14 In this current study, the probability of survival was notably better among older elderly patients than younger ones. Patients with advanced age, pre-existing coronary artery disease, prior stroke, pre-existing renal failure, obesity, NSTEMI, prior ACS, and presence of supraventricular arrhythmias were found to be significantly more likely to undergo conservative treatment.Citation15 In-hospital mortality was significantly higher in conservatively treated patients.Citation13 This trend of conservative treatment in elderly with myocardial infarction appears to continue, according to this study.
Elderly patients represent a substantial proportion of the population admitted to hospital with myocardial infarction, and receive less evidenced-based therapy.Citation16 Further, age is an independent predictor of short- and medium-term mortality.Citation16 In addition, a significant decrease in the utilization rate of invasive diagnostic coronary angiography and increased in-hospital mortality were observed as patient age increased.Citation17 Approximately 33% of all ACS episodes occur in patients over 75 years old and account for approximately 60% of overall mortality due to ACS.Citation18–Citation20 The incidence of ACS in the elderly is projected to increase due to advances in prior ACS treatment in an aging population.Citation21,Citation22
Conclusion
This study did not observe an increase in evidence-based therapy for coronary heart disease by cardiac catheterization in very elderly patients over recent years.
Disclosure
The author reports no conflicts of interest in this work.
References
- AndrawesWFBussyCBelminJPrevention of cardiovascular events in elderly peopleDrugs Aging20052285987616245959
- JokhadarMWengerNKReview of the treatment of acute coronary syndrome in elderly patientsClin Interv Aging2009443544419966912
- ThygesenKAlpertJSWhiteHDJoint ESC/ACCF/AHA/WHF Task Force for the Redefinition of Myocardial InfarctionUniversal definition of myocardial infarctionEur Heart J2007282525253817951287
- DeWoodMASporesJNotskeRPrevalence of total coronary occlusion during the early hours of transmural myocardial infarctionN Engl J Med19803038979027412821
- DeWoodMASporesJHensleyGRCoronary arteriographic findings in acute transmural myocardial infarctionCirculation198368I39496602670
- LiebsonPRKleinLWThe non-Q wave myocardial infarction revisited: 10 years laterProg Cardiovasc Dis1997393994449122424
- Hunyadi-AnticevićSColakZFuntakILEuropean Resuscitation Council guidelines for resuscitation2010Lijec Vjesn2011133114
- RymuzaHKowalikIDrzewieckiASuccessful primary coronary angioplasty improves early and long-term outcomes in ST segment elevation acute coronary syndromes in patients above 80 years of ageKardiol Pol20116934635421523668
- KestelootHSansSKromhoutDDynamics of cardiovascular and all-cause mortality in Western and Eastern Europe between 1970 and 2000Eur Heart J20062710711316204263
- EscanedJRydénLZamoranoJLTrends and contexts in European cardiology practice for the next 15 years: the Madrid Declaration: a report from the European Conference on the Future of CardiologyMadridJune 2–3, 2006Eur Heart J20072863463717283000
- AlexanderKPNewbyLKCannonCPAcute coronary care in the elderly, part I: Non-ST-segment-elevation acute coronary syndromes: a scientific statement for healthcare professionals from the American Heart Association Council on Clinical Cardiology: in collaboration with the Society of Geriatric CardiologyCirculation20071152549256917502590
- AlexanderKPNewbyLKCannonCPAcute coronary care in the elderly, part II: ST-segment-elevation myocardial infarction: a scientific statement for healthcare professionals from the American Heart Association Council on Clinical Cardiology: in collaboration with the Society of Geriatric CardiologyCirculation20071152570258917502591
- TespiliMGuagliumiGValsecchiOIn-hospital clinical outcome in elderly patients with acute myocardial infarction treated with primary angioplastyItal Heart J2003419319812784746
- PolewczykAJanionMGasiorMGierlotkaMPolońskiLBenefits from revascularisation therapy in the elderly with acute myocardial infarction. Comparative analysis of patients hospitalised in 1992–1996 and in 2005–2006Kardiol Pol20106887388120730715
- RittgerHSchnuppSSinhaAMPredictors of treatment in acute coronary syndromes in the elderly: Impact on decision making and clinical outcome after interventional vs conservative treatmentCatheter Cardiovasc Interv2011Epub Nov25
- TimóteoATRamosRTosteAImpact of age on treatment and outcomes after acute myocardial infarction, particularly in very elderly patientsRev Port Cardiol2011 Epub Nov 21. Portuguese
- HsiehTHWangJDTsaiLMImproving in-hospital mortality in elderly patients after acute coronary syndrome-A nationwide analysis of 97,220 patients in Taiwan during 2004–2008Int J Cardiol2011 Epub Nov 5
- AlexanderKPRoeMTChenAYEvolution in cardiovascular care for elderly patients with non-ST-segment elevation acute coronary syndromes: Results from the CRUSADE National Quality Improvement InitiativeJ Am Coll Cardiol2005461479148716226171
- GoldbergRJMcCormickDGurwitzJHAge-related trends in short- and long-term survival after acute myocardial infarction: a 20-year population-based perspective 1975–1995Am J Cardiol19988211131113179856911
- RogerVLJacobsenSJWestonSATrends in the incidence and survival of patients with hospitalized myocardial infarction, Olmsted County, Minnesota, 1979 to 1994Ann Intern Med2002136534134811874305
- MackayJMensahGThe Atlas of Heart Disease and StrokeGenevaWorld Health Organization2004
- Center for Disease ControlPublic health and aging: Trends in aging: United States and worldwideMMWR20035210110612645839