
Abstract
Purpose
Older persons have been identified as a vulnerable population with respect to the novel coronavirus outbreak, COVID-19. Aiming to “flatten the curve” a strict Movement Control Order (MCO) was implemented in Malaysia. Older adults with cognitive frailty are prone to physical, cognitive and psychosocial decline. This study aims to compare physical activity patterns, psychological wellbeing and coping strategies of older persons with cognitive frailty in the “WE-RISE” trial (intervention versus control) throughout this period.
Materials and Methods
This study was conducted as a sub-analysis of the ongoing “WE-RISE” randomized controlled trial. This study included 42 community-dwelling older adults, aged 60 years and above, with cognitive frailty, stratified into intervention (n=21) and control (n=21) groups who are receiving a multi-domain intervention and usual care, respectively, within the Klang Valley, Malaysia. Phone call interviews were conducted during the MCO period. Physical activity patterns were assessed using International Physical Activity Questionnaire (IPAQ) and Functional Activities Questionnaire (FAQ). Psychological wellbeing was assessed using Flourishing Scale (FS) and General Health Questionnaire (GHQ-12), while the Brief Coping Orientation to Problems Experienced (COPE) assessed coping strategies. Data were analysed descriptively and with independent samples t-test.
Results
The WE-RISE intervention group had significantly higher levels of estimated resting energy expenditure (MET) for “walking activity” (I:μ=1723.1±780.7;C:μ=537.4±581.9)(p<0.001), “moderate activity” (I:μ=1422.8±1215.1;C:μ=405.7±746.9)(p=0.002) and “total physical activity” (I: μ=3625.9±3399.3;C:μ=994.6±1193.9)(p=0.002). The intervention group was also significantly more independent in functional activities (μ=1.76±1.73) as compared to the control group (μ=5.57±8.31) (p<0.05). Moreover, significant higher self-perception of living a meaningful life and feeling respected (p<0.05) was demonstrated in regard to psychological well-being in the intervention group. Regarding coping strategies, the intervention group relied significantly on the domains of religion (I:μ=6.43±0.99;C:μ=6.09±1.09)(p<0.05) and planning (I:μ=4.81±0.75; C:μ=4.04±1.28)(p<0.05) whilst the control group relied on humour (C:μ=3.14±1.19; I:μ=2.38±0.74)(p<0.05).
Conclusion
Participants of the WE-RISE intervention group were more physically active, functionally independent and had higher self-perceived social-psychological prosperity regarding living a meaningful life and feeling respected; whilst both groups relied on positive coping strategies during the MCO. These results indicate that it is vital to ensure older persons with cognitive frailty remain physically active and preserve their psychosocial wellbeing to be more resilient in preventing further decline during a crisis such as the COVID-19 pandemic.
Video Abstract

Point your SmartPhone at the code above. If you have a QR code reader the video abstract will appear. Or use:
The highly infectious, novel coronavirus disease (COVID-19) was declared a global pandemic by the World Health Organization (WHO) in March 2020 as a result of its rapid spread across the globe, including Malaysia.Citation1 Described as a respiratory illness emulating viral pneumonia, the transmission of the COVID-19 virus occurs through the transfer of respiratory droplets among infected individuals or contact with contaminated objects and surfaces. The most common symptoms of infection include fever, dry cough and fatigue.Citation1,Citation2
Following the vast spread of the disease, COVID-19 was labelled a “public health emergency of international concern”; forcing affected countries into a nationwide “lock down” to limit and prevent the spread of the disease.Citation3,Citation4 Malaysia implemented a strict Movement Control Order (MCO) from the 18th of March to the 3rd of May 2020 aimed to “break the chain of infection” which enforced all citizens to remain at home with the exception of obtaining essentials.Citation5 Individuals who did not adhere to the MCO regulations were held accountable under the Malaysian Laws of Prevention and Control of Infectious Diseases Act 1988.Citation6 The MCO was followed by a Conditional Movement Control Oder (CMCO). Malaysia was in the Recovery Movement Control Oder (RMCO) phase which begun in August 2020 and was expected to last till the 31st of December 2020.Citation7 Unfortunately, as of October 2020, Malaysia has entered the third wave of the COVID-19 pandemic, causing “red zone” areas (including the Klang Valley) to revert to the CMCO ruling.Citation7
The general population is vulnerable to the COVID-19.Citation8 However, evidence has established that older persons who are immunocompromised, with pre-existing diseases (diabetes, hypertension, cardiovascular disease and cerebrovascular disease) are more predisposed to infection.Citation1,Citation9 The vulnerability of older persons leads to critical illnesses, admission to intensive care unit (ICU) and higher mortality rates.Citation8 In Europe, 95% of fatalities due to COVID-19 were among those aged 60 years and above and is causing ‘hidden deaths’ across the continent.Citation10 The majority of the deceased had at least one underlying chronic condition.Citation10 However, in the United States, 8 out of 10 deaths due to COVID-19 infections have been in older persons aged 65 years and above.Citation11 In the Malaysian context, the Ministry of Health’s mortality review established that the age-group with the highest COVID-19 deaths is between 61 and 70 years (32.2%) followed secondly by the 71 to 80 age-group (19.2%); hence, older persons aged 60 years and older are a “high-risk group”.Citation12
Older persons are known to be typically less active than the younger population and are more at risk of poor health outcomes.Citation13 The routine activities of daily living of older persons have been abruptly halted due to the requirement of “physical distancing” and staying at home throughout the MCO period. Given the vulnerability of the older population to COVID-19, it is highly likely that they will have to continue adhering to these strict precautionary protocols and restrictions until a vaccine is authorized for distribution.Citation3 As a consequence of physical isolation, older persons may be subjected to sedentary behavior due to a decline in physical activity.Citation13 The MCO has led to restrain and the inability to carry out regular daily tasks such as outdoor daily chores, halted participation in community activities and social gatherings, as well as engagement in formal exercises such as community-based group exercises, daily walks, usual exercise regimes and more. Physical and social isolations have also highly compromised the mental wellbeing of older adults.Citation14
Malaysia is en route to attaining the status of an aged nation by the year 2030 as older persons increase in population as well as life expectancy, resulting in increased susceptibility to morbidity and disability.Citation15,Citation16 Cognitive frailty is a geriatric syndrome characterized by the simultaneous presence of cognitive impairment and physical frailty without the presence of dementia.Citation17 Physical frailty is a multi-faceted, age-related syndrome caused by multiple physiological dysfunctions and is characterized by weakness, slowness, shrinking, exhaustion and diminished physical function.Citation18 Cognitive impairment is a noticeable and measurable deterioration of cognitive function.Citation19 Risk factors of cognitive impairment include polypharmacy, chronic illness (hypertension, diabetes mellitus, heart disease, brain disease), metabolic disorders, depression, infections and smoking.Citation20 The presence of cognitive impairment within older persons with frailty has been found to occur without the presence of evident brain disease.Citation20 Physical frailty is a predictor of cognitive impairment and vice-versa, hence its coalition as cognitive frailty.Citation20
Physical frailty was found to be highly prevalent at 56.6% among Malaysian older persons residing in institutions and has been strongly associated with cognitive decline.Citation21 Within the community-dwelling population, cognitive frailty has been reported to be prevalent at 2.2%.Citation22 Among the significant predictors of this potentially debilitating condition are depression, decline in functional mobility, physical frailty and increasing age.Citation23 It has been suggested that both constructs are potentially reversible should it be detected at the early stages of development such as pre-frailty or mild cognitive impairment.Citation17,Citation20 In an effort to specifically address the clinical manifestations of cognitive frailty and potential reversibility, a multi-domain intervention (The WE-RISE intervention) was conducted prior to the pandemic in senior citizen activity centers among community-dwelling older persons with this condition.Citation24
Physical inactivity and poor mental health have been labelled as ‘adverse effects’ of physical and social isolation measures in combatting the spread of COVID-19.Citation13,Citation25 Frailty has been identified as a predictor of poor prognosis amongst older persons with COVID-19.Citation26 “Inflammaging” is the concept referring to the dysregulation of inflammatory mediators within the ageing body resulting in a persistent low-intensity inflammation which is often the cause for age-related disorders, including frailty.Citation10 This leads to the inability to fight against infections such as COVID-19 due to the pro-inflammatory state, resulting in the risk of severe disease complications.Citation26 A decline in physical function may lead to further severity of frailty status. Where cognitive function and psychosocial impact are a concern, the pandemic has been associated with the worsening of neuropsychiatric symptoms, sleep disorders, high levels of anxiety and lower self-perceived psychological wellbeing attributed to the drastic change in lifestyle and fear of infection itself among older persons with or without cognitive impairment.Citation27 The lack or absence of social contact, social support and inadequate social network has been postulated to accelerate neurological ageing and increase the risk of dementia development among older persons.Citation14
Older persons with cognitive frailty are already prone to functional disability and decline in cognitive function.Citation17 Hence, there is a possibility that the strictly imposed “stay at home” restrictions may have had an impact upon their physical and psychosocial wellbeing. There is inadequate evidence highlighting the effect of isolation specifically among the population with cognitive frailty. The aim of this current study was to compare physical activity patterns, psychosocial wellbeing and coping strategies among older persons with cognitive frailty in the ongoing WE-RISE trial (intervention versus control) throughout the MCO due to the COVID-19 outbreak.
Materials and Methods
This cross-sectional study is a sub-analysis conducted among Malaysian older persons with cognitive frailty, aged 60 years and above who are participants in an ongoing randomized controlled trial, the “WE-RISE Trial”. Participants of this 6-month trial consisted of two matched community-dwelling older persons groups whereby the Intervention group received the WE-RISE intervention encompassing multi-component exercise regimen, cognitive stimulation, dietary counselling and psychosocial support; whereas the Control group continued active usual care from their respective activity centers.
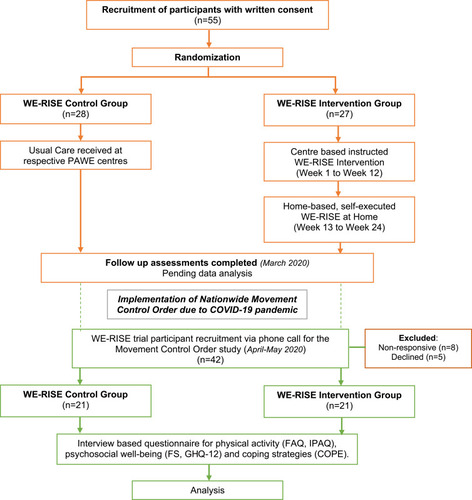
The operational definition of cognitive frailty in the WE-RISE trial is as defined by the International Consensus Group at the International Academy on Nutrition and Aging (I.A.N.A) and the International Association of Gerontology and Geriatrics (I.A.G.G).Citation17 It is understood as the co-existence of physical frailty based on that developed in the Cardiovascular Health Study and mild cognitive impairment (MCI) defined as objective evidence in one or more cognitive domains and preserved independence in functional abilities (Clinical Dementia Rating Scale (CDR) score of 0.5).Citation17 The classification of the cognitive frailty groups in the WE-RISE Trial is as outlined in .Citation17 summarizes the trial flow and further detailed information on the WE-RISE trial has been described in the protocol paper.Citation24
Table 1 Operational Definition and Classification of Cognitive Frailty Groups.
Figure 1 Study trial flow diagram.
Study Population
The participants of the WE-RISE trial are registered members of the Activity Centers for Older Persons; known locally as “Pusat Aktiviti Warga Emas” (PAWE) within the Klang Valley.Citation28 The participants were contacted via a phone call between April to May 2020, during the MCO period and the duration of the interview was between 45 and 60 minutes long. Verbal consent was obtained for voluntary participation in this study with the assurance of anonymity.
Sociodemographic Data, Clinical Characteristics and Self-Rated Satisfaction of Life
Sociodemographic data obtained included gender, age, ethnicity, education level, marital status, status of employment, average household income and smoking history. Medical history included history of falls, surgery and hypercholesterolemia as well as a robust list of co-morbidities adapted from the Self-Administered Comorbidity Questionnaire (SCQ).Citation29 Comorbidity was determined with the simultaneous presence of two or more chronic diseases.Citation30 Depression was evaluated using the validated Malay version of the Geriatric Depression Scale (M-GDS–14) with a cut-off point of 5/6 to indicate clinically significant depression.Citation31 Satisfaction with current life and access to health services during the MCO was self-reported based binary responses (yes/no) to the questions “Are you satisfied with your current state of living?” and “Are currently obtaining the health services that you require?”.
Physical Activity Pattern
The Functional Activities Questionnaire (FAQ) evaluates the level of independence of older persons when carrying out activities of daily living. The 10-items screened for are ability to handle finances, taxes and important documents, shopping for essentials, playing games or hobbies, making a hot drink, preparing a meal, awareness of current events, attention to media (television, books, magazine), remembering vital dates or events and travelling. Scoring of the questionnaire ranges from 0 to 30 with a cut-off point at 9 (dependency in at least three activities); implying the possibility of impaired functioning.Citation32
International Physical Activity Questionnaire (IPAQ) short form was used as a surveillance of physical activity levels within a population. The quantification of physical activity uses the metabolic equivalent of task (MET) values as follows: walking = 3.3 METs, moderate activity = 4.0 METs and vigorous activity = 8.0 METs. Final scores are calculated in MET-minutes per week (MET-min week −1) using the formula: minutes of activity/day × days/week × MET value for each activity category. Total MET-min week −1 is a sum of all three categories. The activity of “sitting” in the IPAQ is used as a measure of time spent doing sedentary activities per week and is not included as a part of the physical activity scores. The “sitting” component is reported in median values and interquartile ranges as outlined in the IPAQ guideline.Citation33,Citation34
Psychological Wellbeing and Coping Strategies
The Brief-Coping Orientation to Problems Experienced (COPE) scale assessed coping strategies of older persons in this study resorted to during the MCO. The scale comprises 28 items, with a 4-point Likert scale ranging from “I haven’t been doing this at all” to “I have been doing this a lot”. The 14 domains of coping strategies are active coping, use of emotional support, use of instrumental support, positive reframing, planning, acceptance, self-distraction, denial, substance abuse, behavioral disengagement, venting, self-blame, humor and religion. There is no overall total score, only total scores for each of the 14 domains which range between 2 and 8 points. Higher scores indicate a higher dependency on the particular domain as a coping mechanism.Citation35,Citation36
The Flourishing Scale (FS) is an assessment of “social-psychological prosperity” in terms of subjective well-being. The 8-item questionnaire consists of recognized psychological needs for human functioning, namely, purposefulness, social relationships, competence, optimism, self-respect, self-acceptance, contributing to others’ wellbeing and engagement in activities. Each item is scored between 1 (strongly disagree) to 7 (strongly agree), and total score ranges between 8 and 56. Higher scores indicate that the respondent perceives themselves to be on the more positive spectrum and have healthier psychological well-being.Citation37
The General Health Questionnaire (GHQ-12) is a measure of overall psychological distress. The 12-items items include psychological factors such as sleep disturbance, stress, inability to overcome problems and feeling happy or depressed. Each item assesses the level of psychological well-being ever since the commencement of MCO using a 4-point scale ranging from “more than usual” to “much less than usual”. For the purpose of this study the scoring method selected was 0-0-1-1 instead of the Likert scale scoring of 0-1-2-3; aimed at eliminating bias. Total score ranges from 0 to 12, whereby higher scores indicate higher levels of psychological distress.Citation38
Statistical Analysis
Sociodemographic data and clinical characteristics of the participants were descriptively analyzed, stratified by the intervention and control groups. Physical activity patterns, psychological wellbeing and coping strategies were analyzed using independent samples t-test with the participant groups (intervention/control) as the dependent variable. Significance level was set at p<0.05 and data were analyzed using the Statistical Package for Social Sciences (SPSS) software, version 23.0.
Results
A total of 42 participants (Intervention=21; Control=21) were successfully contacted and agreed to participate in the present study, summing the response rate at 76.4%. The participants in this study were not infected with the COVID-19 virus upon interview and were in strict adherence to the imposed MCO. The sociodemographic and clinical characteristics of the participants are as outlined in . Participants were mostly females (88.1%) with a mean age of 69.3±6.0 years. Ethnically, participants comprised Malay (69.0%), Chinese (9.5%) and Indian (21.4%) which are the predominant ethnicities in Malaysia. Mean body mass index (BMI) of the participants is 27.3±4.6 kg/m2 which is within the “normal” range for older persons.Citation39 In terms of clinical characteristics, the three most prevalent chronic diseases among the participants were hypertension (66.7%), hypercholesterolemia (69.0%) and diabetes mellitus (47.6%). Interestingly, 9.5% of the participants, all of whom were from the control group reported to experiencing back pain during the MCO (p<0.05). Participants were generally satisfied with their current lives and had no unmet health needs throughout this period.
Table 2 Sociodemographic, Clinical Characteristics, Life Satisfaction and Need for Health Needs of the WE-RISE Participants During the MCO
The IPAQ scores of the participants are outlined in . During the MCO, participants in the intervention group scored significantly higher MET-min per week for the “walking” category as they walked at home, around the neighborhood or to obtain essentials as recreation, exercise or leisure (p<0.001). Likewise, the intervention group also participated more in “moderate” activities which encompass cycling, carrying light weights, gardening or exercises requiring moderate physical effort (p<0.05). Participants in the control group were found to spend longer minutes per week engaging in passive activities in sitting or lying down positions. The total IPAQ scores imply that the control group was more sedentary during the MCO as they had lower MET-min per week as compared to the intervention group (p<0.05). The independence levels of the participants during the MCO are as described in . In terms of the specific activities, the control group required assistance or were dependent on carrying out skilled tasks, making a hot beverage, preparing meals, keeping updated with current events, paying attention and remembering important information (p<0.05) as compared to the intervention group. This is reflected in the total FAQ scores which are significantly higher in the control group than the intervention group (p<0.05).
Table 3 IPAQ Scores of the WE-RISE Participants During the MCO
Table 4 FAQ Scores of the WE-RISE Participants During the MCO
Overall scores of the FS indicate that both groups experienced similar levels of social-psychological prosperity throughout the MCO (). However, when each item of the scale was individually analyzed, the intervention group had significantly higher scores in terms of purposefulness and feeling respected (P<0.05) as compared to the control group. The GHQ-12 scores of the participants in this study imply that both groups did not experience concerning levels of psychological distress during the MCO period (). When stratified by items of the GHQ-12, the psychological distress that the participants experienced most was loss of sleep and the least was feeling worthless. Coping strategies employed by the participants during the MCO period are as described in . Both groups relied the most on the domain of “religion” as a coping strategy though it was significantly higher among the intervention group (p<0.05). Likewise, the intervention group relied significantly more on the domain of “planning” (p<0.05). Contrastingly, the control group sought the “humor” domain as a coping mechanism more significantly than the intervention group (p<0.05).
Table 5 Social-Psychological Prosperity Scores of the WE-RISE Participants During the MCO
Table 6 Psychological Distress Experienced by the WE-RISE Participants During the MCO
Table 7 Coping Strategies Sought by the WE-RISE Participants During the MCO Based on the Brief COPE Scale
Discussion
This study describes the physical activity patterns, psychosocial well-being status and coping strategies of older persons with cognitive frailty of the ongoing WE-RISE trial during the government imposed MCO period (March to May 2020) in Malaysia due to the COVID-19 pandemic. The drastic but necessary precautionary effort was noted to be effective in “breaking the chain of infection”.Citation5 Nonetheless, this extended period of quarantine has challenged the resilience of the ageing population in terms of economic well-being, social exclusion, mental health, physical inactivity and vulnerability to adverse health outcomes.Citation40,Citation41
Sociodemographically, there is no disparity between the intervention and control groups as the samples were pair-matched prior to the commencement of the WE-RISE trial. Clinically there were no changes in the presence of chronic illnesses from the time of baseline screening, but older persons from the control group (9.5%) reported experiencing “back pain” at the time of the phone call interviews which they previously had not been diagnosed with prior to the MCO. The home quarantine restrictions have been reported to increase the likelihood of older persons engaging in prolonged periods of sedentary behavior.Citation13,Citation42 Sedentary behavior during the MCO may explain the sudden onset of back pain as it has been significantly associated with multiple detrimental health outcomes which include chronic back pain among older persons.Citation43
The importance of physical activity and its role in extending functional independence, preserving cognitive reserves and promoting quality of life within the ageing population are well established.Citation44 Physical activity guidelines for older persons which encompass endurance, resistance, flexibility and balance exercises have been outlined.Citation45 Nevertheless, older persons still remain the least physically active population as they have not been meeting these recommendations, even during ‘pre-COVID-19ʹ times.Citation3,Citation44,Citation46 A further exacerbated reduction in physical activity and increase in dormancy among older persons can be inferred, given the strict “Stay at Home” ruling imposed by the government. A cross-sectional study by Yamada et al (2020) studying the effects of the COVID-19 pandemic on community-dwelling older persons reported a significant decrease in time spent engaging in physical activity among those who were frail.Citation47 In the present study, this phenomenon can be observed amongst the participants of the control group who spent more time (expressed in MET-min week−1) partaking in sedentary activities (in sitting, reclined or lying postures) as compared to engaging in light (walking) or moderate physical activities. Physical exercise is a vital component of cognitive frailty management.Citation17 Continuous disengagement from physical activity may result in further degradation in functionality and disability in time.Citation47
The results of this study have shown that older persons who are engaging in the WE-RISE intervention were more physically active during the MCO period. The WE-RISE intervention includes a guided 3-month home program (WE-RISE at Home) which may have enabled the participants to carry out multi-component exercise training safely and effectively on their own.Citation24 It can be hypothesized that given their exposure to the intervention and awareness of the importance of maintaining an active lifestyle, these participants may have been more motivated to execute some form of physical activity in the comforts of their own homes during the MCO. Regarding the functional independence of the participants in our study, both groups have considerably adequate levels of functional independence. The total scores of the FAQ were way below the cut-off value (>9); implying that they may not be completely dependent but require some assistance in carrying out certain functional tasks. However, the control group required more assistance than the intervention group for tasks that involved executive function, attention and memory which could be attributed to their pre-existing deficits in cognitive functioning.Citation48
Physical inactivity could consequently lead to a compromise in immunity among older persons hence increasing exposure to infection by way of exacerbating existing age-related pathologies.Citation49 The severity of COVID-19 infection is not just caused by the virus itself but also heavily relies on the immune response of the host.Citation49 Lower physical activity levels are associated with immunosenescence; understood as a decline in the immune system parallel to increasing age. This in turn results in a risk of chronic diseases, frailty, mortality, reduced efficacy in response to vaccine and decline in cognitive function.Citation49 This could imply that engaging in regular exercise and physical activity could suppress or delay the risks and age-related adverse outcomes with a stronger immune system.
The COVID-19 vaccine is on the cusp of dissemination around the world. Seeing as the ageing population with frailty has been the most heavily impacted by the pandemic, it can be assumed that older persons would most likely be prioritized for vaccination.Citation50 The developed COVID-19 vaccines are new and its efficacy amongst the older population has yet to be determined. Older persons with frailty and those with comorbidities have been excluded in the majority of the vaccine study trials, despite being the most vulnerable to infection.Citation50 Taking immunosenescence into consideration, theoretically the vaccines may be less effective in older persons as a result of inadequate antibody levels.Citation50 With the uncertainty of how the immune system may response to the vaccine, there is a possibility of increasing overall risk to adverse outcomes especially among the already predisposed older persons with frailty.Citation50 Therefore, preventing physical inactivity and boosting the body’s immunity via engagement in regular exercise and functional activities could possibly mitigate these potential adverse outcomes.
In relation to psychosocial well-being, both groups expressed relatively favorable overall levels of self-perceived success. Contrastingly when analyzed by each domain of the scale, intervention group participants seem to have a higher sense of self-worth in the sense that they reported leading a purposeful and meaningful life and that they are respected by other people. The WE-RISE intervention incorporated the element of psychosocial support as evidence has advocated its incorporation for the promotion of adherence to physical activity and stimulation of cognitive function.Citation24,Citation51 A two-way relationship has been established whereby older persons with higher levels of psychological well-being have been associated with higher physical activity levels.Citation41 Likewise, active engagement in physical activity resulted in the improvement of mental and emotional well-being among older persons;Citation52 corroborating with the findings in this present study.
Coping is understood as a self-protective mechanism that is used to help in the management of potential psychological stress when experiencing a stressful circumstance.Citation53 In this study, “religion”, “acceptance” and “positive reframing” were the top three coping strategies recruited which fall under “approach coping”, while “self-blame”, “denial” and “substance abused” which fall under “avoidant coping” were the least popular choices. When compared between both groups, older persons from the intervention group relied more on the coping strategy of “planning” (approach coping) than their control group counterparts. Approach coping strategies are a more valuable method of responding to adverse circumstances. It reflects the ability to adapt and react to situations with better emotional composure and taking control of the situation appropriately.Citation53 Whereas resorting to avoidance coping strategies may result in emotional numbness, disruptive behaviors and non-productive outcomes.Citation53
Heavy reliance and belief in the religion of the participants is in congruence with existing evidence that asserts religion as a vital coping strategy among older persons.Citation54 Among the ageing population, religion and spirituality have been strongly associated with positive psychological well-being as it provides support, sense of belonging, purpose in life and aids in ameliorating distress; especially in the face of adversity.Citation54 Humor was significantly more tapped into by the control group during the MCO. From a psychological standpoint, humor and laughter are significantly helpful coping mechanisms that bring about positive mental outcomes and when dealing with unexpected calamities, such as a global pandemic.Citation55 With these findings, it can be deduced that the participants in this study (both control and intervention groups) pursued positive coping strategies to get by the challenging MCO circumstances.
The mental and psychological vulnerability faced by older persons worldwide during the pandemic can be considered “social frailty”. Social frailty is an understudied frailty phenotype that requires more understanding as its relevance is unquestionable in the times of social isolation brought forth by the pandemic.Citation56 Older persons without dementia were found to experience high stress levels, anxiety, depression and peri-traumatic stress during COVID-19 related isolation. Whereas older adults with mild cognitive impairment and dementia faced agitation, apathy, depression, irritability, restlessness and sleep difficulty, which improved with social engagement (such as video calls with family members).Citation14 The participants in the present study did not experience symptoms associated with the COVID-19 virus and were not diagnosed with the disease during the period of data collection. However, existing literature has reported that older persons express symptoms of delirium and agitation upon acute infection of the COVID-19 virus.Citation14 The direct and indirect effects of the COVID-19 infection upon brain function and psychiatric well-being require further research. If the infection triggers damage to neural tissue, it could result in cognitive decline and psychological dysfunction and will require early attention to halt or delay its progression.Citation14
It has been suggested that with the continuation of quarantine and physical isolation, the general older population are predisposed to mental health disturbances, functional disability and frailty.Citation57 The already predisposed older population with cognitive frailty is at greater risk of further physical and cognitive functional decline as well as an overwhelming psychological burden. Malaysians have expressed positive attitudes towards battling COVID-19 and recognize the importance of quarantine and adhering to the standard operating procedures in order to “flatten the curve”.Citation58 Nevertheless, a symbiosis between ‘pre-COVID-19ʹ and current times must be met. The WHO has encouraged maintaining social activities virtually and engage in regular physical activity at home as alternatives to maintaining regular daily activities during this pandemic.Citation59
To our knowledge, there is yet to be a study describing the physical activity patterns and psychosocial well-being of older persons with cognitive frailty during the nationwide MCO brought forth by the COVID-19 crisis. Observing these physical and psychosocial domains provides insight into their overall well-being during the pandemic. Addressing the limitations of this study, data analyzed for this present study were self-reported and there is a possibility of the participants providing responses that they perceive to be socially desirable. In addition, an analysis of the variables stratified by gender was not executed due to the imbalance of male and female participants in this study. There is evidence supporting that men are less forthcoming when participating in health promotion programs, as experienced in the WE-RISE trial participant recruitment.Citation60 However, all samples were pair-matched during randomization and there were no significant differences between the groups despite the small number of male participants. The sample size of this study is relatively small and employs a univariate analysis; however, these findings can be used as a platform for larger and more explorative future research undertakings. In addition, the WE-RISE intervention was developed with the aim of reversing cognitive frailty. The difference in physical activity patterns could potentially indicate that some reversal or improvement of frailty symptoms have taken place in this ongoing trial as the results of the trial have yet to be analyzed. There is a need for larger studies investigating the effects of other existing potential factors such as genetic and nutritional variables on cognitive status and physical activity patterns (independently or interactively) among older adults with cognitive frailty. As a recommendation, home-based intervention packages that address the components of physical, psychosocial and mental well-being among older persons should be disseminated. In the light of this global crisis, it is important to create awareness that physical and social isolation is not a deterrent to maintaining normalcy in terms of physical and psychological well-being.
Considering the existing association between frailty, cognitive impairment, immunosenescence and susceptibility to infection and other inflammatory diseases, it can be assumed that older persons with cognitive frailty are at higher risk of COVID-19 infection with higher severity, poorer prognosis and are less likely to respond to vaccination.Citation10 This study hopes to highlight the importance of targeted research and treatment development with respect to the older persons with frailty and comorbidities as they are the population that requires it the most. Frailty screenings are important amongst the older population because chronological ageing does not necessarily equate to the physiological differences brought upon by biological ageing.Citation26 The potential reversal of cognitive frailty in its early stages (pre-frailty and mild cognitive impairment) emphasizes the importance of early assessment as it may improve prognosis with prompt management.Citation20,Citation26 Further understanding of COVID-19 and its impact upon the multi-facets of frailty and cognitive impairment is required for strategic and efficient management by public health sectors. Age-specific, client-tailored management of COVID-19 may prevent infection, hospitalization due to complications and reduce fatalities. Preservation of physical and cognitive function, delaying the age-related degradation of both constructs and the potential reversibility of cognitive frailty among older persons is vital and may improve the efficacy of immunization and provide long-lasting protection from the COVID-19 virus.
Conclusion
To conclude, our study observed that older persons with cognitive frailty from the intervention group who were engaged in the WE-RISE community-based multi-domain intervention were more physically active, functionally independent and had higher self-perceived social-psychological prosperity regarding living a meaningful life and feeling respected; while both control and intervention groups sought positive coping strategies during the MCO. Ensuring that older persons remain physically active with the preservation of psycho-social well-being is fundamental during these unprecedented times to promote resilience, prolong functional independence, prevent further deterioration of physical and cognitive reserves and to be prepared for immunization.
Ethics
The studies involving human participants were reviewed and approved by the Research Ethics Committee of Universiti Kebangsaan Malaysia (UKM PPI/111/8/JEP-2018-558) and the Department of Social Welfare Malaysia (MyResearch Reference: JKMM 100/12/5/2: 2018/405). The authors affirmed that informed consent was obtained from the participants involved with assurance of anonymity. This study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
We would like to extend our gratitude and appreciation to the WE-RISE participants who participated in this study during this trying period for not only the nation but also the world. We thank the Department of Social Welfare Malaysia and “Pusat Aktiviti Warga Emas” (PAWE) for their continuous support. We would also like to thank Prof Dr Michael Fenech, Distinguished Professor, Faculty of Health Sciences, UKM, for reviewing and proofreading this manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
- Cucinotta D, Vanelli M. WHO declares COVID-19 a pandemic. Acta Biomed. 2020;91(1):157–160. doi:10.23750/abm.v91i1.939732191675
- Shah AUM, Safri SNA, Thevadas R, et al. COVID-19 outbreak in Malaysia: actions taken by the Malaysian government. Int J Infect Dis. 2020;97:108–116. doi:10.1016/j.ijid.2020.05.09332497808
- Said CM, Batchelor F, Duque G. Physical activity and exercise for older people during and after the coronavirus disease 2019 pandemic: a path to recovery. J Am Med Dir Assoc. 2020;21(7):977–979. doi:10.1016/j.jamda.2020.06.00132674830
- World Health Organization. Public health emergency of international concern (PHEIC). 2020. Available from: https://www.who.int/blueprint/priority-diseases/key-action/Global_Research_Forum_FINAL_VERSION_for_web_14_feb_2020.pdf. Accessed 818, 2020.
- Prime Minister’s Office of Malaysia. Perutusan Khas COVID-19 (18Mac 2020) – stay at home. 2020. Available from: https://www.pmo.gov.my/2020/03/perutusan-khas-covid-19-18-mac-2020/. Accessed 818, 2020.
- Ministry of Health Malaysia. . COVID-19: Akta pencegahan dan pengawalan penyakit berjangkit 1988. 2020. Available from: http://covid-19.moh.gov.my/faqsop/akta-342. Accessed 818, 2020.
- National Security Council. COVID-19: movement control order. 2020. Available from: https://www.mkn.gov.my/web/ms/covid-19/.Accessed 1020, 2020.
- Liu K, Chen Y, Lin R, Han K. Clinical features of COVID-19 in elderly patients: a comparison with young and middle-aged patients. J Infect. 2020;80:e14–e18. doi:10.1016/j.jinf.2020.03.005
- Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497–506. doi:10.1016/S0140-6736(20)30183-531986264
- Palermo S. Covid-19 pandemic: maximizing future vaccination treatments considering aging and frailty. Front Med. 2020;7:1–11. doi:10.3389/fmed.2020.558835
- Centers for Disease Control and Prevention. Coronavirus disease: older adults. 2020. Available from: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/older-adults.html. Accessed 818, 2020.
- Ministry of Health Malaysia. Press statement: updates on the coronavirus disease 2019 (COVID-19) situation in Malaysia. 2020. Available from: http://covid-19.moh.gov.my/terkini/052020/situasi-terkini-03-mei-2020/103%20Kenyataan%20Akhbar%20KPK%20COVID-19%20(3%20Mei%202020)%20-%20EN.pdf. Accessed 54, 2020.
- Roschel H, Artioli GG, Gualano B. Risk of increased physical inactivity during COVID-19 outbreak in older people: a call for actions. J Am Geriatr Soc. 2020;68(6):1126–1128. doi:10.1111/jgs.1655032392620
- Manca R, De Marco M, Venneri A. The impact of COVID-19 infection and enforced prolonged social isolation on neuropsychiatric symptoms in older adults with and without dementia: a review. Front Psychiatry. 2020;11. doi:10.3389/fpsyt.2020.585540
- Masud J, Tengku Aizan H, Sharifah AH. Measuring poverty among elderly Malaysians. AJPS. 2015;1(1):73–81.
- Crimmins EM. Lifespan and healthspan: past, present, and promise. Gerontologist. 2015;55(6):901–911. doi:10.1093/geront/gnv13026561272
- Kelaiditi E, Cesari M, Canevelli M, et al. Cognitive frailty: rational and definition from an (I.A.N.A./I.A.G.G.) international consensus group. Astrophys J. 2012;756(1):59.
- Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol Ser a Biol Sci Med Sci. 2001;56(3):M146–M157. doi:10.1093/gerona/56.3.M14611253156
- Petersen RC, Caracciolo B, Brayne C, Gauthier S, Jelic V, Fratiglioni L. Mild cognitive impairment: a concept in evolution. J Intern Med. 2014;275(3):214–228. doi:10.1111/joim.1219024605806
- Morley JE, Morris JC, Berg-weger M, et al. Brain health: the importance of recognizing cognitive impairment. J Am Med Dir Assoc. 2016;16(9):731–739. doi:10.1016/j.jamda.2015.06.017
- Murukesu M, Singh S, Subramaniam S, et al. Prevalence of frailty and its association with cognitive status and functional fitness among ambulating older adults residing in institutions within west coast of Peninsular Malaysia. Int J Environ Res Public Health. 2019;16(23):1–13. doi:10.3390/ijerph16234716
- Rivan NFM, Shahar S, Rajab NF, et al. Cognitive frailty among Malaysian older adults: baseline findings from the LRGS TUA cohort study. Clin Interv Aging. 2019;14:1343–1352. doi:10.2147/CIA.S21102731413555
- Rivan NFM, Shahar S, Rajab NF, et al. Incidence and predictors of cognitive frailty among older adults: a community-based longitudinal study. Int J Environ Res Public Health. 2020;17(5):1–17. doi:10.3390/ijerph17051547
- Murukesu RR, Kaur D, Singh A, Shahar S. A multi-domain intervention protocol for the potential reversal of cognitive frailty: “WE-RISE” randomized controlled trial. Front Public Heal. 2020;8(471):1–11.
- Mukhtar S. Psychological impact of COVID-19 on older adults. Curr Med Res Pract. 2020;10:201–202.32839732
- Ma Y, Hou L, Yang X, et al. The association between frailty and severe disease among COVID-19 patients aged over 60 years in China: a prospective cohort study. BMC Med. 2020;18(1):1–8. doi:10.1186/s12916-020-01761-031898501
- Forte G, Favieri F, Tambelli R, Casagrande M. The enemy which sealed the world: effects of COVID-19 diffusion on the psychological state of the Italian population. J Clin Med. 2020;9(6):1802. doi:10.3390/jcm9061802
- Department of Social Welfare. Activity center for older person. 2016. Available from: http://www.jkm.gov.my/jkm/index.php?r=portal/left&id=aC90Vy81SVhKTEZDcVoxRE5JRzNRZz09. Accessed 518, 2020.
- Sangha O, Stucki G, Liang MH, Fossel AH, Katz JN. The self-administered comorbidity questionnaire: a new method to assess comorbidity for clinical and health services research. Arthritis Rheum. 2003;49(2):156–163. doi:10.1002/art.1099312687505
- Valderas JM, Starfi B, Sibbald B, Salisbury C, Roland M. Defining comorbidity: implications for understanding health and health services. Ann Fam Med. 2009;7(4):357–363. doi:10.1370/afm.98319597174
- Teh EE, Ismail HC. Validation of Malay version of geriatric depression scale among elderly inpatients. Priory. 2005.
- Pfeffer RI, Kurosaki TT, Harrah CH, Chance JM, Filos S. Measurement of functional activities in older adults in the community. J Gerontol. 1982;37(3):323–329.7069156
- International Physical Activity Questionnaire (IPAQ). IPAQ scoring protocol: guidelines for data processing and analysis of the international physical activity questionnaire (IPAQ) – short and long forms. 2005. Available from: http://www.ipaq.ki.se/scoring.pdf. Accessed 216, 2020.
- Chu AHY, Moy FM. Reliability and validity of the Malay international physical activity questionnaire (IPAQ-M) among a Malay population in Malaysia. Asia-Pacific J Public Heal. 2015;27(2):1–9.
- Carver CS. You want to measure coping but your protocol’s too long: consider the brief COPE. Int J Behav Med. 1997;4(1):92–100. doi:10.1207/s15327558ijbm0401_616250744
- Yusoff N, Low WY, Yip CH. Reliability and validity of the Malay version of Brief COPE Scale: a study on Malaysian women treated with adjuvant chemotherapy for breast cancer. MJP. 2009;18(1).
- Diener E, Wirtz D, Tov W, et al. New well-being measures: short scales to assess flourishing and positive and negative feelings. Soc Indic Res. 2010;97(2):143–156. doi:10.1007/s11205-009-9493-y
- Zulkefly NS, Baharudin R. Using the 12-item general health questionnaire (GHQ-12) to assess the psychological health of Malaysian college students. Glob J Health Sci. 2010;2(1):73–80. doi:10.5539/gjhs.v2n1p73
- Winter JE, MacInnis RJ, Wattanapenpaiboon N, Nowson CA. BMI and all-cause mortality in older adults: a meta-analysis. Am J Clin Nutr. 2014;99(4):875–890. doi:10.3945/ajcn.113.06812224452240
- United Nations. Policy brief: the impact of COVID-19 on older persons. 2020. Available from: https://unsdg.un.org/sites/default/files/2020-05/Policy-Brief-The-Impact-of-COVID-19-on-Older-Persons.pdf. Accessed 818, 2020.
- Goethals L, Barth N, Guyot J, et al. Impact of home quarantine on physical activity among older adults living at home during the COVID-19 pandemic: qualitative interview study. J Med Internet Res. 2020;22(5):1–5.
- Ricci F, Izzicupo P, Moscucci F, et al. Recommendations for physical inactivity and sedentary behavior during the coronavirus disease (COVID-19) pandemic. Front Public Heal. 2020;8(471):8–11.
- Vancampfort D, Stubbs B, Koyanagi A. Physical chronic conditions, multimorbidity and sedentary behavior amongst middle-aged and older adults in six low- and middle-income countries. Int J Behav Nutr Phys Act. 2017;14(1):1–13. doi:10.1186/s12966-016-0456-928057008
- Sun F, Norman IJ, While AE. Physical activity in older people- a systematic review. BMC Public Health. 2013;13(449):1–17. doi:10.1186/1471-2458-13-44923280303
- Chodzko-Zajko WJ, Proctor DN, Fiatarone Singh MA, et al. American college of sports medicine position stand. Exercise and physical activity for older adults. Med Sci Sports Exerc. 2009;41(7):1510–1530. doi:10.1249/MSS.0b013e3181a0c95c19516148
- Singh DKA, Rahman NNAA, Rajaratnam BS, Yi TC, Shahar S. Validity and reliability of physical activity scale for elderly in Malay language (PASE-M). Malaysian J Public Heal Med. 2018;1:116–123.
- Yamada M, Kimura Y, Ishiyama D, et al. Effect of the COVID-19 epidemic on physical activity in community-dwelling older adults in Japan: a cross-sectional online survey. J Nutr Heal Aging. 2020;2020:1–3.
- Sachdev PS, Blacker D, Blazer DG, et al. Classifying neurocognitive disorders: the DSM-5 approach. Nat Rev Neurol. 2014;10(11):634–642. doi:10.1038/nrneurol.2014.18125266297
- Damiot A, Pinto AJ, Turner JE, Gualano B. Immunological implications of physical inactivity among older adults during the COVID-19 pandemic. Gerontology. 2020;66(5):431–438. doi:10.1159/00050921632585674
- Soiza RL, Scicluna C, Thomson EC. Efficacy and safety of COVID-19 vaccines in older people. Age Ageing. 2020;1–5.
- Frost R, Belk C, Jovicic A, et al. Health promotion interventions for community-dwelling older people with mild or pre-frailty: a systematic review and meta-analysis. BMC Geriatr. 2017;17(1):1–13. doi:10.1186/s12877-017-0547-828049446
- Delle Fave A, Bassi M, Boccaletti ES, et al. Promoting well-being in old age: the psychological benefits of two training programs of adapted physical activity. Front Psychol. 2018;9:1–13. doi:10.3389/fpsyg.2018.0082829410639
- Roth S, Cohen LJ. Approach, avoidance, and coping with stress. Am Psychol. 1986;41(7):813–819. doi:10.1037/0003-066X.41.7.8133740641
- Vitorino LM, Low G, Vianna LAC. Linking spiritual and religious coping with the quality of life of community-dwelling older adults and nursing home residents. Gerontol Geriatr Med. 2016;2:1–9. doi:10.1177/2333721416658140
- Berk RA. The greatest veneration: humor as a coping strategy for the challenges of aging. Soc Work Ment Health. 2015;13(1):30–47. doi:10.1080/15332985.2014.890152
- Lozupone M, La Montagna M, Di Gioia I, et al. Social frailty in the COVID-19 pandemic era. Front Psychiatry. 2020;11:1–8. doi:10.3389/fpsyt.2020.57711332116830
- Chen LK. Older adults and COVID-19 pandemic: resilience matters. Arch Gero. 2020;89:104124.
- Azlan AA, Hamzah MR, Sern TJ, Ayub SH, Mohamad E. Public knowledge, attitudes and practices towards COVID-19: a cross-sectional study in Malaysia. PLoS One. 2020;15(5):1–15. doi:10.1371/journal.pone.0233668
- World Health Organization. Mental health and psychosocial considerations during the COVID-2019 outbreak. 2020. Available at: https://www.who.int/docs/default-source/coronaviruse/mental-health-considerations.pdf. Accessed 825, 2020.
- Ryan J, Lopian L, Le B, et al. It’s not raining men: a mixed-methods study investigating methods of improving male recruitment to health behaviour research. BMC Public Health. 2019;19(1):1–9. doi:10.1186/s12889-019-7087-430606151