
Abstract
Introduction
Maintaining skeletal muscle function throughout life is a crucial component of successful aging. Disadvantaged socioeconomic position (SEP) is associated with adverse health outcomes, but has not been extensively studied for the muscle disease sarcopenia. We aimed to determine the prevalence of probable sarcopenia, a precursor to sarcopenia diagnosis, based on the European Working Group on Sarcopenia in Older People 2 (EWGSOP2) guidelines overall, and according to SEP.
Methods
This cross-sectional study comprised 3342 community-dwelling older adults [mean age (SD) 68.9 ± 6.3 years] from Wave 1 of the Irish Longitudinal Study on Ageing. Probable sarcopenia was identified using gender-specific cut-off values for handgrip strength as recommended by EWGSOP2. SEP was defined by educational attainment. Multivariate regression analysis was employed to determine associations between probable sarcopenia and pre-defined risk factors.
Results
Overall, 23.4% of the population had probable sarcopenia and was significantly higher in the subset with low compared with high SEP (28.9% vs 18.1%, p<0.001). Consistent with this, multivariate logistic regression analysis showed that disadvantaged SEP was a significant determinant of probable sarcopenia [OR, CI 1.48 (1.17, 1.87) p<0.001]. Other known risk factors, namely, increased age, low physical activity, comorbidity, and osteoarthritis were significantly associated with an increased likelihood of probable sarcopenia, while overweight/obesity appeared to be protective.
Conclusion
Disadvantaged SEP was an independent determinant of probable sarcopenia in community-dwelling older adults. These findings highlight that SEP and health inequality should be considered in prevention and treatment policy for sarcopenia in the community.
Video abstract

Point your SmartPhone at the code above. If you have a QR code reader the video abstract will appear. Or use:
Introduction
The Global Burden of Disease report highlights the strong association between health and sociodemographic indices such as total income per capita and educational attainment.Citation1 Disadvantaged socioeconomic position (SEP) is associated with health inequalities, namely, higher prevalence and earlier onset of disease and difficulties in accessing health services across the life course, including older age.Citation2,Citation3 While SEP has been linked with several chronic diseases in aging, the relationship between SEP and the muscle disease sarcopenia has not been extensively studied in older populations.
Sarcopenia, a public health issue, is associated with the accelerated loss of muscle mass and strength and is a major preventable cause of disability amongst older populations globally.Citation4 Sarcopenia is associated with poor health outcomes such as increased risk of falls, impaired ability to perform activities of daily living, hospitalization, disability and mortality.Citation4–Citation6 In 2018, the European Working Group on Sarcopenia in Older People (EWGSOP) updated their original definition of sarcopenia to reflect recent scientific and clinical evidence. EWGSOP2 emphasized reduced muscle strength, rather than mass, as a major determinant of sarcopenia amongst older adults.Citation6 This focus on low muscle strength as a key characteristic is reflected in the introduction of the concept of probable sarcopenia as a precursor to sarcopenia diagnosis.
To aid the identification of low muscle strength, EWGSOP2 provided gender-specific cut-off points for hand grip strength (HGS) and/or poor performance in the chair rise test, which indicate the presence of probable sarcopenia. According to EWGSOP2 guidelines, which recommend measuring muscle strength as an initial assessment for sarcopenia, weak HGS <16kg for females and <27 kg for males indicates the presence of probable sarcopenia. This decline in muscle strength, known as probable sarcopenia, was the focus of the present study. The introduction of clear criteria for probable sarcopenia is advantageous, as this can be measured easily and inexpensively using hand grip strength and/or chair rises, applicable to community-dwelling populations. Following this initial assessment, sarcopenia diagnosis is confirmed by examining muscle quantity or quality, and severity of disease is determined by physical performance measures such as Timed Up and Go Test (TUG).Citation4 Importantly, if probable sarcopenia is identified, this is considered an appropriate time-point to initiate interventions.Citation4
The prevalence of probable sarcopenia and its risk factors have not been extensively investigated within large community-dwelling populations. Previous research has described the prevalence as between 19% and 47% amongst community-dwelling older adults, with higher prevalence observed amongst older cohorts.Citation7–Citation10 Several risk factors for probable sarcopenia have been identified, which include older age, physical inactivity, osteoarthritis and impaired performance in activities of daily living.Citation7,Citation9,Citation10 Recent research has shown associations between probable sarcopenia and increased length of stay in hospital, and greater risk of mortality amongst older adult populations.Citation6
Previous research has suggested socioeconomic position (SEP) is associated with poorer physical function, specifically, muscle function amongst older adults.Citation11 There are few studies, however, examining SEP and probable sarcopenia. Dodds et al found no association between manual occupation class and probable sarcopenia (n= 1686).Citation7 Recently, a study from Colombia reported a high prevalence of probable sarcopenia (46.5%) in a population which also appeared to have a relatively high proportion of socioeconomic disadvantage.Citation9 To the best of the authors’ knowledge, this is the first study to specifically investigate probable sarcopenia and socioeconomic disadvantage. We used educational attainment, which is considered a robust indicator of SEP amongst older adult populations.Citation12
Further research is required to identify at-risk groups for sarcopenia onset, including those meeting the criteria for probable sarcopenia if effective preventative policies are to be developed. This study aimed to estimate the prevalence of probable sarcopenia, as defined by the EWGSOP2 guidelines, overall and according to SEP in a large population of community-dwelling older adults. Furthermore, we sought to investigate if SEP was a determinant of probable sarcopenia. We hypothesized that probable sarcopenia would be more prevalent in older adults with lower compared with higher SEP. It was anticipated that the findings may assist in the development of strategies for early detection and treatment of sarcopenia and support the diverse needs older adults in the community.
Methods
Study Design and Population
This study was based on a publicly available dataset of Wave 1 of the Irish Longitudinal Study on Ageing (TILDA). TILDA is a nationally representative, ongoing longitudinal study which includes adults aged 50 years and older in Ireland.Citation13 Wave 1 took place in 2009–2011 and included a total of 8504 community-dwelling older adults. Participants were invited to take part in a health centre or home-based health assessment of which 6152 adults enrolled (72.3%). The TILDA study was conducted according to the guidelines set out in the Declaration of Helsinki, and ethical approval was granted by the Trinity College Dublin Research Ethics Committee.Citation14 Written informed consent was obtained from all participants.
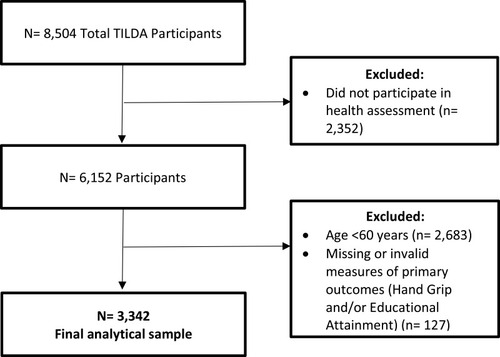
For the present study, the inclusion criteria were as follows: community-dwelling adults, aged 60 years and older, participated in the health assessment, completed the hand grip strength assessment and with available data on educational attainment. Hand grip strength was required to determine probable sarcopenia and educational attainment to determine SEP.Citation4 Of those who participated in a health assessment, 3469 individuals were aged 60 years and older and only those with measured hand grip strength were included in the study (n= 3342) ().
Figure 1 Study inclusion and exclusion criteria.
Assessing Probable Sarcopenia
Probable sarcopenia was defined as per the EWGSOP2 cut-off criteria for hand grip strength of less than 27kg in males and 16kg in females.Citation4 Grip strength was assessed using a Baseline Hydraulic Hand Dynamometer with two measures taken per hand and the maximum value for the dominant hand used in analyses, in line with previous studies.Citation6,Citation7 Studies show that the Baseline Hydraulic Hand Dynamometer measures hand grip strength with the same accuracy as the Jamar Hydraulic Hand Dynamometer.Citation15
Determining Socioeconomic Position
Socioeconomic position was categorized using the highest reported level of formal education completed. Completion of none, part or all of primary education was classified as low education, indicating low SEP. Participants who exited formal education following the completion of Junior/Intermediate Certificate or Leaving Certificate (high school) examinations were classified as the intermediate SEP group. Completion of a third-level qualification was classified as high SEP. Highest educational qualification was previously identified as a suitable indicator of SEP amongst older adult populations.Citation12
Health and Lifestyle Risk Factors
Demographic variables available included gender (dichotomous variable) and age (continuous variable) with participants aged 80 years or older top coded as 80 years old, frequently applied to preserve anonymity in public release data. Potential risk factors for probable sarcopenia were selected based on the current evidence.Citation4 Physical activity levels were assessed using the short form International Physical Activity Questionnaire (IPAQ) and categorized into high, moderate and low physical activity levels. Participants self-reported the typical amount of time per day spent sitting, walking, or doing physical activity classified as vigorous or moderate intensity in the previous week. Respondents were classified as either high, moderate or low activity levels based on previously defined criteria.Citation16
Body Mass Index was calculated based on weight (kg) and height (m2) and was classified as underweight range (≥15–18.5 kg/m2), normal (≥18.5–25 kg/m2), overweight (≥25–30 kg/m2) and obese range (≥30 kg/m2).Citation17 Comorbidities were classified according to the Functional Comorbidity Index (FCI) which was modified as per previous studies, based on the available participant data.Citation18 The FCI produced a continuous score (0–16) for self-reported physician-diagnosed long-term conditions.Citation18,Citation19 The number of chronic conditions were categorized as none, one or two or more conditions, similar to previous studies.Citation7 Osteoarthritis was recorded as present if a participant reported that a diagnosis was provided by a physician. Smoking was self-reported and classified as never smoked, past smoker or current smoker. Alcohol consumption status was recorded as a dichotomous variable: current alcohol consumer or non-consumer.
Statistical Analysis
Descriptive statistics are reported as means ± SD or percentages. Chi-square test for independence was applied to compare sociodemographic and health variables of interest for the probable sarcopenic group. Independent Student’s t-tests were used for comparing continuous variable characteristics of the study group with the reference group. Following univariate analysis, factors showing significant associations (p<0.05) with probable sarcopenia were entered into the multivariate logistic regression model. Adjusted odds ratios (ORs) and 95% confidence intervals (CIs) are reported for multivariate logistic regression analyses. All analyses were performed using IBM SPSS Statistics V24 software.
Results
Study Population
The study population () was of mean age 68.9 ± 6.3 years, with 42.4% aged 70 years and older and 53.1% female. Based on educational attainment as a marker of SEP, 34.9% of participants exited formal education at primary level (n= 1166), 36.1% after completion of Junior or Leaving Certificate (high school) examinations (n= 1207) and 29.0% completed third-level education (n= 969). Overweight and obesity were common (78.4%), and just under one-third (32.7%) of participants reported low levels of physical activity. A majority of the population reported being current or past smokers (86.9%) and consumed alcohol (70.4%). Most of the study population had two or more documented chronic conditions (54.2%).
Table 1 Characteristics of the Study Population Overall and by Gender (n = 3342)
Prevalence of Probable Sarcopenia Overall and According to Socioeconomic Position
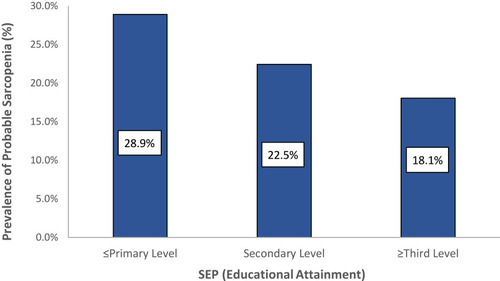
The prevalence of probable sarcopenia was 23.4% (n= 783) as defined by the EWGSOP2 cut-off criteria for weak hand grip strength (). Probable sarcopenia was highest (28.9%, n= 337) among older adults with primary education only and lowest in those with tertiary education (18.1%, n= 175) (p<0.001) (). Probable sarcopenia was documented for 22.5% (n= 271) of those with secondary level education.
Figure 2 Prevalence of probable sarcopenia amongst community-dwelling older adults based on socioeconomic position as defined by educational attainment (n= 3342, p<0.001).
Characteristics of Older Adults with Probable Sarcopenia
The profile of the study population with probable sarcopenia is shown in , including educational attainment, used as a marker of SEP. A significantly higher proportion of participants with probable sarcopenia exited formal education at primary level (43.0% v 32.4%, p<0.001) and fewer had completed a third-level qualification compared with the reference group (22.3% vs 31.0% p<0.001).
Table 2 Characteristics of the Population Group Based on the Presence of Probable Sarcopenia as Defined by the EWGSOP2 Criteria for Weak Hand Grip Strength (n = 3342)
The findings support other known risk factors for sarcopenia, namely advanced age, osteoarthritis, and low physical activity levels. Participants with probable sarcopenia were significantly older (mean age 72.3 ± 6.7 v reference group 67.9 ± 5.9, p<0.001) and more physically inactive (43.3% vs 29.5%, p<0.001). Among those with probable sarcopenia, a significantly greater number of participants had a BMI in the healthy range (24.6% vs 19.9%, p= 0.004) compared to the reference group, and fewer were overweight (39.0% vs 44.1%, p=0.011). Long-term chronic conditions (2 or more) were more prevalent among those with probable sarcopenia (64.8% vs 51.0%, p<0.001) compared to the reference group. Of note, osteoarthritis was more common amongst the probable sarcopenia group (21.7% vs 16.3%, p<0.001). Probable sarcopenia did not differ between the groups based on gender or smoking status.
Multivariate Analysis of Factors Associated with Probable Sarcopenia
Following univariate analysis, lower educational attainment was entered into the logistic regression model with other risk factors for sarcopenia, namely age, gender, body mass index (BMI), physical activity level, smoking status, alcohol consumption status, osteoarthritis, and number of long-term conditions. The significant association persisted between SEP and probable sarcopenia following multivariate regression analysis (). Older adults with primary level education only were 1.48 times more likely to have probable sarcopenia [OR, CI 1.48 (1.17, 1.87), p<0.001] than those who completed third-level education. The model supported associations of low physical activity [OR, CI 1.67 (1.32, 2.11), p<0.001], older age [OR, CI 1.10 (1.08, 1.11, p<0.001], comorbidity [OR, CI 1.44 (1.08, 1.93, p= 0.013], and osteoarthritis [OR, CI 1.34 (1.05, 1.68), p= 0.018] with probable sarcopenia. Overweight and obese BMI were associated with a lower risk of probable sarcopenia compared to a BMI in the healthy range [OR, CI 0.74 (0.58, 0.93), p=0.010 and 0.64 (0.50, 0.83), p<0.001, respectively].
Table 3 Multivariable Logistic Regression Model of Risk Factors for Probable Sarcopenia (N= 3342)
Discussion
The muscle disease sarcopenia is a public health issue and is a major preventable cause of disability amongst older populations globally.Citation4 The decline in muscle strength alone is a marker of probable sarcopenia and was the focus of the present study. We showed that disadvantaged socioeconomic position (SEP), measured as educational attainment, was an independent predictor of probable sarcopenia in a large study of community dwelling adults aged 60 years and older (n= 3342). Overall, 23% of the study population had probable sarcopenia, and this was significantly higher in participants with the fewest years in formal education (29%) compared to those with third-level education (18%). The findings suggest that specific attention should be given to socioeconomic disadvantage in the design of screening and prevention strategies for sarcopenia in community-dwelling older adults.
We assessed the prevalence of probable sarcopenia based on the EWGSOP2 guidelines for hand grip strength. In 2018, the EWGSOP2 updated the definition of sarcopenia and introduced the concept of probable sarcopenia to reflect up-to-date scientific and clinical evidence.Citation4 Overall, we identified probable sarcopenia in 23.4% of study population aged 68.9 ± 6.3 years. This is broadly in agreement with previous studies of probable sarcopenia based on EWGSOP2 guidelines. Some authors, in assessing muscle weakness for probable sarcopenia, used hand grip strength,Citation9,Citation10 while others also included performance on chair rise test.Citation7,Citation8 Wearing et al reported a prevalence of 26.3% and 28.0% for probable sarcopenia in females and males, respectively (n = 219), although this study was conducted in a study population of advanced age (84.1 ± 5.7 years).Citation10 In an analysis of the Korean Frailty and Ageing Cohort Study (n= 2099, mean age 75.9 ± 4.0 years),Citation8 24% of participants had probable sarcopenia. While Dodds et al estimated a prevalence of 19% amongst the 1946 British birth cohort aged 69 years (n = 1686).Citation7 Pérez-Sousa et al reported a prevalence of 47% amongst a representative sample of Colombian older adults; however, the prevalence of low socioeconomic status (76%) and physical inactivity (83%) was strikingly higher than in other studies of probable sarcopenia. Assessment of hand grip strength is a simple and inexpensive screening tool for sarcopenia in community-dwelling older populations, given that sarcopenia diagnosis requires more complex diagnostic measures of muscle mass or quality.Citation4
The present study specifically aimed to investigate the prevalence of sarcopenia in older adults living with disadvantaged SEP. There is an abundance of evidence showing an association between disadvantaged SEP and a higher prevalence and earlier onset of adverse health outcomes with specific evidence available for this cohort based on educational attainment.Citation1,Citation20,Citation21 In the present study, we showed the prevalence of probable sarcopenia was significantly greater in participants with the fewest years in formal education (28.9%) compared to those with third-level education (18.1%). Few studies have examined probable sarcopenia in terms of socioeconomic position. Dodds et al utilized occupation class as a measure of SEP but found that no significant association persisted when controlled for other known risk factors.Citation7 Pérez-Sousa et al reported that individuals of high SEP, defined as social class, were significantly less likely to meet the criteria for probable sarcopenia compared to those of low SEP.Citation9 Previous studies have examined associations between low muscle strength and SEP employing a range of indicators. Associations between low hand grip strength and SEP, when measured by wealth, have previously been reported.Citation20 Additionally, an earlier study found an association between sarcopenia prevalence and SEP when defined by income. Furthermore, early childhood circumstance has been identified as a predictor of low muscle strength in later life.Citation11 Given that there are several relatively simple and inexpensive markers for both socioeconomic disadvantage and probable sarcopenia, identifying and targeting those most at risk of sarcopenia would likely yield benefits.
The present study identified educational attainment as a determinant of probable sarcopenia when adjusted for other known risk factors. Older adults with fewest years of education (<8 years) had a 48% increased risk of probable sarcopenia when compared to those with tertiary education. The model confirmed other known risk factors for sarcopenia, namely, older age, physical inactivity, number of chronic conditions and osteoarthritis. Osteoarthritis was an independent predictor of probable sarcopenia which has previously been shown to increase the risk of low grip strength.Citation22 Overweight and obese BMI suggested protective effects when compared to those of normal range BMI. This is in line with previous studies which found a positive association between overweight and obese BMI with HGS.Citation23 One hypothesis is that older adults with obese or overweight BMI may have greater muscle mass and less fat mass than those with weak HGS.Citation24 Few participants were underweight (0.6%). Similar to previous findings, low physical activity was identified as the most important modifiable risk factor, with physically inactive older adults 1.7 times more likely to have probable sarcopenia.Citation9 Resistance training has been shown as an effective tool for the management and treatment of sarcopenia; however, this study’s findings suggest specific attention should be given to low SEP groups who have been identified as less likely to engage in physical activity programmes.Citation4,Citation25
In the present study, we identified that older people with the fewest years of education had the highest prevalence of probable sarcopenia and represent an important group for future interventions. This is important, as the Covid-19 pandemic has exposed and amplified existing inequalities in society, with individuals of disadvantaged SEP most affected.Citation26 Furthermore, the implementation of movement confinement measures in response to the ongoing pandemic has the potential to accelerate sarcopenia amongst this vulnerable group.Citation27 The findings suggest that specific attention should be given to socioeconomic disadvantage in the design and implementation of detection and prevention strategies for sarcopenia in the community. Given that educational attainment, or other markers of disadvantaged SEP, are relatively easy to collect routinely, population groups with indicators of disadvantaged SEP should be considered as priority for screening probable sarcopenia in older adults. Studies have shown, a decline in muscle strength, probable sarcopenia is observed as early as middle age.Citation28 This may present opportunity for timely intervention which could prevent or delay further decline amongst those most at-risk of probable sarcopenia onset.Citation4 The findings highlight the importance of forming inclusive intervention practices which take socioeconomic position into account.
This study included analysis on an open-access dataset of The Irish Longitudinal Study on Ageing, a nationally representative sample of community-dwelling older adults in Ireland.Citation13 This is the largest study to specifically focus on SEP and the prevalence and predictors of probable sarcopenia amongst community-dwelling older adults in Ireland. Educational attainment was selected as a robust indicator of SEP in the present study as it has been shown that longer duration of education predicts several health advantages which includes improved physical function amongst older adults.Citation29,Citation30 Previous research has identified educational attainment as a robust indicator of SEP amongst older adult populations.Citation12 Some study limitations must be acknowledged. It is important to note that this was a cross-sectional study and therefore, cannot show cause and effect for the higher prevalence of probable sarcopenia amongst older adults with disadvantaged SEP. Furthermore, previous analysis has shown that older adults of low SEP were less likely to participate in the health assessment component of TILDA.Citation31 Additionally, the dataset did not specify ethnicity or nutritional factors, including protein, energy intake and vitamin D, which may also influence sarcopenia and muscle function.Citation32–Citation34 These limitations may result in an underestimation of the prevalence of probable sarcopenia. Similar to previous studies, probable sarcopenia was defined by hand grip strength; however, future work could include other measures of muscle strength such as chair rise test and application of the Sarc-F screening tool.Citation9,Citation10 Furthermore, future work should seek to actively include those living with socioeconomic disadvantage and ethnic minority populations in research.
Conclusions
The recognition of probable sarcopenia as a precursor to sarcopenia onset may aid early detection of low muscle strength and with timely intervention, may prevent or delay further decline. In the present study, the prevalence of probable sarcopenia was 23.4% amongst a large nationally representative sample of community-dwelling older adults in Ireland (n= 3342). Probable sarcopenia was most prevalent amongst older adults with fewest years in formal education, identifying an important group for future intervention. Our findings suggest that disadvantaged socioeconomic position, older age, physical inactivity, comorbidity, and osteoarthritis are associated with increased risk of probable sarcopenia. The findings highlight the importance of forming inclusive intervention practices which take socioeconomic position into account.
Data Sharing Statement
The dataset analyzed in the current study is available from Inter-university Consortium for Political and Social Research [distributor], 2018-08-01. https://doi.org/10.3886/ICPSR34315.v2r [ICPSR 34315]
Ethical Approval and Consent to Participate
The study was conducted according to the guidelines of the Declaration of Helsinki, and ethical approval was granted by the Faculty of Health Sciences Research Ethics Committee at Trinity College Dublin, Ireland.Citation13 Informed consent was obtained from all subjects involved in the study.
Acknowledgments
We would like to thank all the staff working on The Irish Longitudinal Study on Ageing (TILDA) and the participants in the project.
Disclosure
The abstract of this paper was presented at the ESPEN Virtual Conference 2020 as a poster presentation with interim findings. The poster’s abstract was published in “Poster Abstracts” in Clinical Nutrition Espen (https://clinicalnutritionespen.com/article/S2405-4577(20)31032-9/fulltext).
Ms Lauren Swan reported grants from North Dublin Home Care, during the conduct of the study. The authors declare that they have no other potential conflicts of interest for this work.
References
- Murray CJL, Abbafati C, Abbas KM, et al. Five insights from the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1135–1159. doi:10.1016/S0140-6736(20)31404-533069324
- Davies JM, Sleeman KE, Leniz J, et al. Socioeconomic position and use of healthcare in the last year of life: a systematic review and meta-analysis. PLoS Med. 2019;16(4):e1002782. doi:10.1371/journal.pmed.100278231013279
- Kollia N, Caballero FF, Sánchez-Niubó A, et al. Social determinants, health status and 10-year mortality among 10,906 older adults from the English longitudinal study of aging: the ATHLOS project. BMC Public Health. 2018;18(1):1357. doi:10.1186/s12889-018-6288-630526556
- Cruz-Jentoft AJ, Bahat G, Bauer J, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019;48(1):16–31. doi:10.1093/ageing/afy16930312372
- Landi F, Cruz-Jentoft AJ, Liperoti R, et al. Sarcopenia and mortality risk in frail older persons aged 80 years and older: results from ilSIRENTE Study. Age Ageing. 2013;42(2):203–209. doi:10.1093/ageing/afs19423321202
- Sobestiansky S, Michaelsson K, Cederholm T. Sarcopenia prevalence and associations with mortality and hospitalisation by various sarcopenia definitions in 85–89 year old community-dwelling men: a report from the ULSAM Study. BMC Geriatr. 2019;19(1):318. doi:10.1186/s12877-019-1338-131747923
- Dodds RM, Murray JC, Robinson SM, Sayer AA. The identification of probable sarcopenia in early old age based on the SARC-F tool and clinical suspicion: findings from the 1946 British birth cohort. Eur Geriatr Med. 2020;11(3):433–441. doi:10.1007/s41999-020-00310-532297269
- Kim M, Won CW. Prevalence of sarcopenia in community-dwelling older adults using the definition of the European working group on sarcopenia in older people 2: findings from the Korean Frailty and Aging Cohort Study. Age Ageing. 2019;48(6):910–916. doi:10.1093/ageing/afz09131329815
- Pérez-Sousa MÁ, Pozo-Cruz J, Cano-Gutiérrez CA, Izquierdo M, Ramírez-Vélez R. High prevalence of probable sarcopenia in a representative sample from Colombia: implications for geriatrics in Latin America. J Am Med Dir Assoc. 2020. doi:10.1016/j.jamda.2020.10.021
- Wearing J, Konings P, de Bie RA, Stokes M, de Bruin ED. Prevalence of probable sarcopenia in community-dwelling older Swiss people – a Cross-Sectional Study. BMC Geriatr. 2020;20(1):307. doi:10.1186/s12877-020-01718-132847545
- Cheval B, Boisgontier MP, Orsholits D, et al. Association of early- and adult-life socioeconomic circumstances with muscle strength in older age. Age Ageing. 2018;47(3):398–407. doi:10.1093/ageing/afy00329471364
- Grundy E, Holt G. The socioeconomic status of older adults: how should we measure it in studies of health inequalities? J Epidemiol Community Health. 2001;55(12):895–904. doi:10.1136/jech.55.12.89511707484
- Kenny RA, Whelan B, Cronin H, et al. The Design of the Irish Longitudinal Study on Ageing. The Irish Longitudinal Study on Ageing; 2010. doi:10.38018/TildaRe.2010-00
- Kearney PM, Cronin H, O’Regan C, et al. Cohort profile: the Irish Longitudinal Study on ageing. Int J Epidemiol. 2011;40(4):877–884. doi:10.1093/ije/dyr11621810894
- Mathiowetz V, Vizenor L, Melander D. Comparison of baseline instruments to the jamar dynamometer and the B&L engineering pinch gauge. Occup Ther J Res. 2000;20(3):147–162. doi:10.1177/153944920002000301
- Craig C, Marshall A, Sjostrom M, et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc. 2003;35(8):1381–1395. doi:10.1249/01.MSS.0000078924.61453.FB12900694
- Centers for Disease Control and Prevention. Defining adult overweight and obesity. Overweight & obesity. CDC; 9 17, 2020. Available from: https://www.cdc.gov/obesity/adult/defining.html. Accessed 1027, 2020.
- O’Connell J, Henman MC, Burke É, et al. Association of drug burden index with grip strength, timed up and go and Barthel index activities of daily living in older adults with intellectual disabilities: an Observational Cross-Sectional Study. BMC Geriatr. 2019;19(1):173. doi:10.1186/s12877-019-1190-331234775
- Fan E, Gifford J, Chandolu S, Colantuoni E, Pronovost P, Needham D. The functional comorbidity index had high inter-rater reliability in patients with acute lung injury. BMC Anesthesiol. 2012;12(1):21. doi:10.1186/1471-2253-12-2122974239
- Steptoe A, Zaninotto P. Lower socioeconomic status and the acceleration of aging: an outcome-wide analysis. Proc Natl Acad Sci. 2020;117(26):14911–14917. doi:10.1073/pnas.191574111732541023
- Barrett A, Burke H, Cronin H, et al. Fifty Plus in Ireland 2011 First Results from the Irish Longitudinal Study on Ageing (TILDA). The Irish Longitudinal Study on Ageing; 2011. Available from: https://www.lenus.ie/handle/10147/129741. Accessed 520, 2021.
- Wen L, Shin M-H, Kang J-H, et al. Association between grip strength and hand and knee radiographic osteoarthritis in Korean adults: data from the Dong-Gu Study. PLoS One. 2017;12(11):e0185343. doi:10.1371/journal.pone.018534329190722
- Pengpid S, Peltzer K. Hand grip strength and its sociodemographic and health correlates among older adult men and women (50 years and older) in Indonesia. Curr Gerontol Geriatr Res. 2018;2018:e3265041. doi:10.1155/2018/3265041
- Jeong S, Choi S, Kim K, Kim SM, Kim S, Park SM. Association among handgrip strength, body mass index and decline in cognitive function among the elderly women. BMC Geriatr. 2018;18(1):225. doi:10.1186/s12877-018-0918-930249201
- McPhee JS, French DP, Jackson D, Nazroo J, Pendleton N, Degens H. Physical activity in older age: perspectives for healthy ageing and frailty. Biogerontology. 2016;17(3):567–580. doi:10.1007/s10522-016-9641-026936444
- Rimmer A. Covid-19: tackling health inequalities is more urgent than ever, says new alliance. BMJ. 2020;371:m4134. doi:10.1136/bmj.m413433106336
- Kirwan R, McCullough D, Butler T, Perez de Heredia F, Davies IG, Stewart C. Sarcopenia during COVID-19 lockdown restrictions: long-term health effects of short-term muscle loss. GeroScience. 2020;42(6):1547–1578. doi:10.1007/s11357-020-00272-333001410
- Keller K, Engelhardt M. Strength and muscle mass loss with aging process. Age and strength loss. Muscles Ligaments Tendons J. 2014;3(4):346–350. doi:10.32098/mltj.04.2013.1724596700
- Louie GH, Ward MM. Socioeconomic and ethnic differences in disease burden and disparities in physical function in older adults. Am J Public Health. 2011;101(7):1322–1329. doi:10.2105/AJPH.2010.19945521164082
- Ross CE, Wu C-L. Education, age, and the cumulative advantage in health. J Health Soc Behav. 1996;37(1):104–120. doi:10.2307/21372348820314
- Kearney PM, Cronin H, O’Regan C, Kamiya Y, Whelan BJ, Kenny RA. Comparison of centre and home-based health assessments: early experience from the Irish Longitudinal Study on Ageing (TILDA). Age Ageing. 2010;40(1):85–90. doi:10.1093/ageing/afq12420870732
- Jeng C, Zhao L-J, Wu K, Zhou Y, Chen T, Deng H-W. Race and socioeconomic effect on sarcopenia and sarcopenic obesity in the Louisiana Osteoporosis Study (LOS). JCSM Clin Rep. 2018;3(2). Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6712972/.
- Kwon Y-J, Kim HS, Jung D-H, Kim J-K. Cluster analysis of nutritional factors associated with low muscle mass index in middle-aged and older adults. Clin Nutr. 2020;39(11):3369–3376. doi:10.1016/j.clnu.2020.02.02432192777
- Aspell N, Laird E, Healy M, Lawlor B, O’Sullivan M. Vitamin D deficiency is associated with impaired muscle strength and physical performance in community-dwelling older adults: findings from the English longitudinal study of ageing. Clin Interv Aging. 2019;14:1751–1761. doi:10.2147/CIA.S22214331686797