
Abstract
Objective
Limited data are available on the predictors of major adverse cardiac events (MACE) after a successful coronary chronic total occlusion (CTO) percutaneous coronary intervention (PCI) and medical therapy. This study aimed to identify predictors of MACE in CTO patients undergoing successful recanalization and medical therapy.
Methods
A total of 2015 patients with CTOs were enrolled. About 718 patients underwent successful CTO recanalization, and 1297 patients received medical therapy. The primary outcome was the frequency of MACE, defined as a composite of cardiac death, myocardial infarction, and target-vessel revascularization. Multivariate models were used to determine predictors of MACE.
Results
In successful CTO recanalization group, MACE occurred in 123 (17.1%) patients. In multivariate analysis, heart failure (hazard ratio [HR] 1.77, 95% confidence interval [CI]: 1.04–3.04, p = 0.036) was identified as independent predictors for MACE in successful CTO recanalization. Additionally, in medical therapy group, the significant predictors of MACE were male gender (HR 1.53, 95% CI: 1.13–2.05, p = 0.005), diabetes mellitus (HR 1.39, 95% CI: 1.11–1.74, p = 0.003), heart failure (HR 1.44, 95% CI: 1.10–1.87, p = 0.007), J-CTO score (HR 1.17, 95% CI: 1.07–1.28, p = 0.001) and multivessel disease (HR 2.20, 95% CI: 1.42–3.39, p < 0.001).
Conclusion
Heart failure was predictor for composite cardiovascular events in patients with CTO after successful recanalization. Male gender, diabetes mellitus, heart failure, J-CTO score and multivessel disease were predictors of MACE in CTO patients with medical therapy.
Introduction
Coronary chronic total occlusion (CTO) occurs in about 10–20% of patients with coronary artery disease who underwent coronary angiography, limiting coronary intervention.Citation1,Citation2 However, procedural success rates of CTO percutaneous coronary intervention (PCI) have significantly improved to 80–90% (experienced operators) due to the availability of new techniques and dedicated devices.Citation3 Successful CTO intervention improves short and long-term clinical outcomes.Citation4,Citation5 However, PCI is performed in only 10–15% of patients undergoing CTO angioplasty procedures.Citation6–Citation8 Nonetheless, there are limited data on the predictors of major cardiovascular events after a successful CTO intervention. Furthermore, the factors impacting the long-time prognosis of patients with medical therapy are unknown. This study aimed to identify predictors of major adverse cardiac events (MACE) in CTO patients undergoing successful recanalization and medical therapy.
Materials and Methods
Study Design and Population
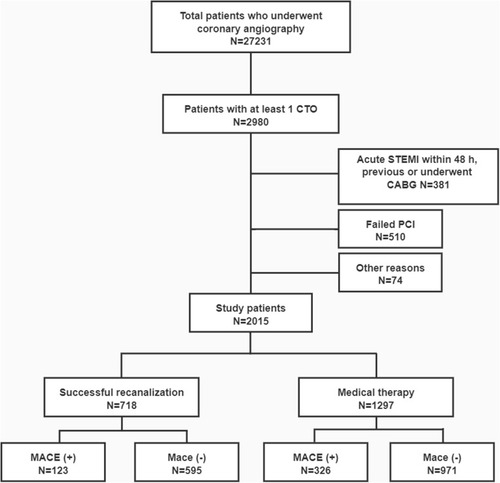
This study included all patients with at least one coronary CTO lesion at our center between January 2007 and December 2018. Exclusion criteria were: patients with failed CTO-PCI or coronary artery bypass grafting (CABG), ST-segment elevation myocardial infarction (STEMI), a history of CABG, cardiogenic shock, or malignant tumor. A total of 2015 patients were included in the study (). Patients were referred for PCI if they had CTO-related symptoms or objective evidence of viability/ischemia in the area of the CTO artery. Inducible myocardial ischemia was evaluated by echocardiography or myocardial perfusion scan and myocardial viability was assessed on cardiac magnetic resonance imaging. In symptomatic patients, even without information on viability or in asymptomatic patients with viability, PCI was preferred. In asymptomatic patients who did not have viability data available or in subjects with proved absence of viability, medical therapy was strongly preferred. The decision to perform PCI for CTO patients was also dependent on several factors, including co-morbidity, the extent of other coronary artery disease, CTO location, technical difficulty, doctors’ and patients’ preference.Citation9–Citation11 Detailed data on demographic and clinical characteristics, procedures, complications were recorded and reviewed in the hospital database. Follow-up data were obtained through inpatient observation, telephone contact or outpatient visit.
Figure 1 Study flow chart.
Ethics
This was a single-center, retrospective observational study approved by the Ethics Committee of the First Affiliated Hospital of Dalian Medical University. The protocol followed the ethical principles in the Declaration of Helsinki. All patients gave their written informed consent prior to any study procedures.
Endpoint and Definitions
CTO was defined as complete coronary occlusion with thrombolysis in myocardial infarction (TIMI) grade 0 flow for three months or longer.Citation12 Duration of occlusion was defined as the time from sudden symptom onset to myocardial infarction (MI) or based on previous angiographic reports. Technical success was defined as restoration of TIMI 3 flow with residual stenosis <30% within the treated segment. The primary endpoint was defined as MACE occurrence, including cardiac death, MI, and target-vessel revascularization (TVR). Cardiac death was defined as a death caused by cardiovascular diseases in the absence of established cardiovascular etiology. MI was defined as the presence of clinical symptoms, ECG change and elevation of CK-MB, troponin I or T levels >3 fold of the upper limit of the normal value.Citation13 TVR was defined as the repeated revascularization of the target vessel via PCI or CABG. HF was defined as symptoms resulting from the left ventricle (LV) systolic dysfunction confirmed via resting transthoracic echocardiography, with left ventricular ejection fraction (LVEF) <35%.
Interventional Procedure and Medical Treatment
All patients were given aspirin (300 mg) (orally), clopidogrel loading dose (300 mg), and weight-adjusted unfractionated heparin (80–100 U/kg) (intravenously) before the procedure. CTO PCI was performed using standard techniques. The post-procedural antiplatelet regimen consisted of lifelong aspirin and clopidogrel (75 mg/day) for at least one year. Statins, antiplatelet medication, β-blockers, nitrate, and renin-angiotensin system blockade, were the medical therapies.Citation14
Statistical Analysis
Continuous variables were expressed as means ± standard deviation and compared using Student’s t-test, Mann–Whitney or Wilcoxon tests. The Kolmogorov–Smirnov test was used to assess whether there was a normal distribution. Categorical data were expressed as frequencies and percentages and were compared using the chi-square test and Fisher’s exact tests. Cox regression proportional hazard model was used to construct univariate and multivariate survival analyses to identify predictors of MACE occurrence. The following variables were included in the Cox regression model: ≥65 years, males, smoking, hypertension, diabetes mellitus, hyperlipidemia, previous MI, chronic kidney disease (CKD), heart failure, LVEF <40%, left ascending coronary artery (LAD) CTO, Japanese-chronic total occlusion (J-CTO) score (per point increment) and multivessel disease. Variables with a univariate P-value <0.1 were included in the multivariate analyses. Hazard ratios (HR) with 95% confidence intervals (CI) and the p-values were determined. All p-values were from two-sided tests, and the level of statistical significance was set at 0.05. SPSS V.24.0 (SPSS Inc, Chicago, IL) and Stata 15 (StataCorp, College Station, TX, USA) were used for all statistical analyses.
Results
Baseline, Angiographic and Procedural Characteristics of Patients
A total of 718 patients underwent successful CTO recanalization, and 1297 patients received medical therapy. The baseline characteristics of the two groups are summarized in . MACE occurred in 123 (17.1%) patients in the successful CTO recanalization group. MACE patients had a higher prevalence of previous MI, heart failure, calcified lesion, and low LVEF than those without MACE. There were no significant differences in procedural characteristics and complications and in-hospital death between the MACE and non-MACE patients. Besides, MACE occurred in 326 (25.1%) patients in the medical therapy group. The patients had prior MI, left circumflex coronary artery (LCX) CTO lesion, multivessel disease, calcified lesion, and high J-CTO score. The prevalence of clinical characteristics was not significantly different between the MACE and non-MACE patients except for the history of MI.
Table 1 Baseline Clinical, Angiographic and Procedural Characteristics and in-Hospital Outcome of All Patients According to the Occurrence of MACE in the Successful Recanalization and Medical Therapy Groups
Clinical Follow-Up and Multivariate Analysis
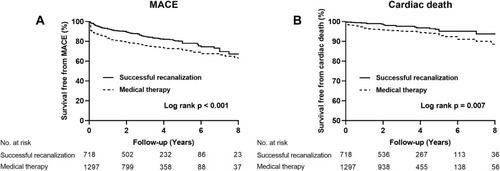
Long-term clinical outcomes are shown in . The median follow-up time was 2.6 (interquartile range (IQR), 1.2–4.7) years. Kaplan-Meier analyses for the occurrence MACE and cardiac deaths during follow-up are shown in . MACE and cardiac deaths were less in patients with successful CTO recanalization than in patients in the medical therapy group (17.1% vs 25.1%, p < 0.001; 3.2% vs 5.1%, p = 0.007, respectively). Multivariate analysis was conducted to identify the risk factors of MACE occurrence. Heart failure (hazard ratio [HR] 1.77, 95% confidence interval [CI]: 1.04–3.04, p = 0.036) was identified as the independent predictor for MACE in successful CTO recanalization (). Additionally, male gender (HR 1.53, 95% CI: 1.13–2.05, p = 0.005), diabetes mellitus (HR 1.39, 95% CI: 1.11–1.74, p = 0.003), heart failure (HR 1.44, 95% CI: 1.10–1.87, p = 0.007), J-CTO score (HR 1.17, 95% CI: 1.07–1.28, p = 0.001) and multivessel disease (HR 2.20, 95% CI: 1.42–3.39, p < 0.001) were independently associated with MACE in medical therapy group ().
Table 2 Clinical Outcomes of All Patients with CTOs in the Successful Recanalization and Medical Therapy Groups
Table 3 Univariate and Multivariate Analyses of the MACE in Patients Who Underwent Successful Recanalization for CTOs
Table 4 Univariate and Multivariate Analyses of the MACE in Patients Who Underwent Medical Therapy for CTOs
Figure 2 Kaplan–Meier curves for MACE (A) and cardiac death (B) during follow-up for successful recanalization versus medical therapy in total patients.
Discussion
Herein, (1) successful CTO PCI group significantly reduced the risk of MACE and cardiac death compared with the medical therapy group. Also, (2) Heart failure after a successful CTO intervention increased MACE occurrence. (3) Male gender, diabetes mellitus, heart failure, J-CTO score, and multivessel disease were predictors of MACE in CTO patients treated with medical therapy.
CTO patients with heart failure had a higher risk profile with more comorbidities and more diffuse and complex coronary lesions. Moreover, they were associated with poor prognosis, an increased risk of sudden death, ventricular arrhythmias based on the COMMIT-HF (COnteMporary Modalities In Treatment of Heart Failure) registry.Citation15,Citation16 Notably, Galassi et al reported that LVEF ≤35% could not predict the occurrence of major cardiac and cerebrovascular events (MACCE) (HR: 1.52; 95% CI: 0.66 to 2.92; p = 0.398) in patients undergoing CTO PCI,Citation17 consistent with this study. Previous studies have also demonstrated that heart failure is associated with MACE in CTO patients.Citation18,Citation19 CTO patients with heart failure may have a high ischemic burden caused by CTO and relevant donor vessels. A retrospective study showed that multivessel disease is the most effective predictor of 5-year MACE.Citation20 CTO patients with heart failure or multivessel disease are associated with a high risk of ventricular tachycardia or ventricular fibrillation.Citation16,Citation21 Therefore, implantable cardioverter-defibrillator (ICD) may benefit these patients, especially those with ischemic cardiomyopathy or low LVEF.Citation22
However, no study has reported on MACE predictors among patients treated with medication alone. Male patients are frequent smokers, have a history of MI, chronic obstructive pulmonary disease, multivessel disease, long and tortuosity lesions compared with female patients, which may increase MI in CTO patients.Citation19,Citation23 Additionally, the CAD process may be delayed in women, possibly due to the potential protective effects of estrogen against coronary atherosclerosis until menopause. Therefore, women with CTOs are more likely to be older than men with CTO.Citation24 Herein, diabetes mellitus was associated with MACE, consistent with previous reports.Citation25,Citation26 Diabetic patients have more comorbidities, significant atherosclerotic burden, longer and more complex coronary lesions, and more adverse cardiovascular events, probably due to frequent hyperplasia, platelet hyperreactivity, increased fibrinogen levels, thromboxane, proinflammatory states, systemic endothelial dysfunction, and metabolic disorders.Citation27,Citation28 Notably, collateral circulation development is less common in diabetic patients than in non-diabetic patients when coronary arteries become occluded. Particularly, well-developed coronary collateral circulation can supply the downstream perfusion area in CTO patients, thereby alleviating myocardial ischemia, preserving viable myocardium, reducing infarct area, improving left ventricular function, and decreasing cardiovascular mortality.Citation29,Citation30 This may indicate the worse outcome of CTO patients with DM.
Prior study demonstrated that the age, creatinine, ejection fraction (ACEF) score might have a sufficient predictive value for in-hospital death in patients with cardiogenic shock secondary to STEMI.Citation31 Furthermore, acute kidney injury (AKI) was an independent prognostic factor for long-term mortality among these patients treated with primary PCI.Citation32 Interestingly, for CTO patients, age and CKD had no predictive value,Citation33–Citation35 possibly due to the different study populations. Besides, CKD was not routinely evaluated among CTO patients in previous studies.Citation26,Citation33,Citation36 In present study, only 51 (7%) patients were with CKD in successful CTO PCI group in our study, and the mean contrast volume was 227mL. Hydration, before and after the CTO procedure, was effective to reduce the occurrence of CIN.Citation35 For the rare patients who need dialysis, it was done immediately after procedure. Therefore, after hydration or dialysis, AKI rate was very low among these patients.
LAD CTO was also not correlated with subsequent adverse clinical outcomes, consistent with previous studies.Citation25,Citation37 However, a high J-CTO score was correlated with the occurrence of composite cardiovascular events. The J-CTO score system is one of the most useful tools to predict CTO PCI success.Citation38 Occlusion length >20 mm represents a higher ischemic burden caused by CTO, and relevant donor vessels and calcification represent an increased atherosclerosis progression.Citation38
Limitations
This study has some limitations. First, this was a non-randomized study. Although the CTO registries have some limitations, this study included several CTO PCI patients. Second, regular angiographic follow-up was not conducted, and thus some adverse events, such as TVR, might not be accurately recorded. Third, the estimated glomerular filtration rate (eGFR) after CTO procedure was not evaluated routinely for all patients at our center, and the data of AKI rate was not recorded in our study. Fourth, symptom improvement, as assessed using the Seattle angina questionnaire, was not assessed before and after revascularization. Fifth, femoral artery is an important vascular approach, especially for CTO procedures due to more dual injection application. The rate of femoral approach was relatively low in the present study. Tokarek et al reported that higher experience in radial approach might be linked to worse outcome in PCI via femoral approach and operators on training should be encouraged to develop proficiency in both radial approach and femoral approach.Citation39 However, most CTO patients were treated with conservative therapy. Therefore, the findings on the high-risk subset may be meaningful.
Conclusion
Heart failure increased the occurrence of MACE in patients with successful recanalized CTO. Male gender, diabetes mellitus, heart failure, J-CTO score, and multivessel disease were MACE predictors in CTO patients treated with medical therapy.
Abbreviations
CTO, chronic total occlusion; MACE, major adverse cardiovascular events; MI, myocardial infarction; PCI, percutaneous coronary intervention.
Data Sharing Statement
The data used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgment
The authors acknowledge the assistance of the Ying Liu, from The First People’s Hospital of Jinzhou.
Disclosure
The authors report no conflicts of interest in this work.
References
- Fefer P, Knudtson ML, Cheema AN, et al. Current perspectives on coronary chronic total occlusions: the Canadian Multicenter Chronic Total Occlusions registry. J Am Coll Cardiol. 2012;59(11):991–997. doi:10.1016/j.jacc.2011.12.00722402070
- Guo L, Wu J, Zhong L, et al. Two-year clinical outcomes of medical therapy vs. revascularization for patients with coronary chronic total occlusion. Hellenic J Cardiol. 2019;61(4):264–271. doi:10.1016/j.hjc.2019.03.00630951874
- Galassi AR, Tomasello SD, Reifart N, Werner GS, Sianos G. In-hospital outcomes of percutaneous coronary intervention in patients with chronic total occlusion: insights from the ERCTO (European Registry of Chronic Total Occlusion) registry. EuroIntervention. 2011;7:472–479. doi:10.4244/EIJV7I4A7721764666
- Guo L, Wang J, Ding H, et al. Long-term outcomes of medical therapy versus successful recanalisation for coronary chronic total occlusions in patients with and without type 2 diabetes mellitus. Cardiovasc Diabetol. 2020;19(1):100. doi:10.1186/s12933-020-01087-432622353
- George S, Cockburn J, Clayton TC, et al. Long-term follow-up of elective chronic total coronary occlusion angioplasty: analysis from the U.K. Central Cardiac Audit Database. J Am Coll Cardiol. 2014;64(3):235–243. doi:10.1016/j.jacc.2014.04.04025034057
- Guo L, Zhang X, Lv H, et al. Long-term outcomes of successful revascularization for patients with coronary chronic total occlusions: a report of 1655 patients. Front Cardiovasc Med. 2020;7:116. doi:10.3389/fcvm.2020.0011632793636
- Tomasello SD, Boukhris M, Giubilato S, et al. Management strategies in patients affected by chronic total occlusions: results from the Italian Registry of Chronic Total Occlusions. Eur Heart J. 2015;36:3189–3198. doi:10.1093/eurheartj/ehv45026333367
- Brilakis ES, Banerjee S, Karmpaliotis D, et al. Procedural outcomes of chronic total occlusion percutaneous coronary intervention: a report from the NCDR (National CardiovascularData Registry). JACC Cardiovasc Interv. 2015;8(2):245–253. doi:10.1016/j.jcin.2014.08.01425700746
- Windecker S, Kolh P, Alfonso F, et al. 2014 ESC/EACTS Guidelines on myocardial revascularization: the Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS)Developed with the special contribution of the European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur Heart J. 2014;35(37):2541–2619.25173339
- Levine GN, Bates ER, Blankenship JC, et al. 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention. A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. J Am Coll Cardiol. 2011;58(24):e44–122.22070834
- Guo L, Zhang S, Wu J, et al. Successful recanalisation of coronary chronic total occlusions is not associated with improved cardiovascular survival compared with initial medical therapy. Scand Cardiovasc J. 2019;53(6):305–311. doi:10.1080/14017431.2019.164535131315453
- Sianos G, Werner GS, Galassi AR, et al. Recanalisation of chronic total coronary occlusions: 2012 consensus document from the EuroCTO club. EuroIntervention. 2012;8(1):139–145. doi:10.4244/EIJV8I1A2122580257
- Cutlip DE, Windecker S, Mehran R, et al. Clinical end points in coronary stent trials: a case for standardized definitions: a case for standardized definitions. Circulation. 2007;115(17):2344–2351. doi:10.1161/CIRCULATIONAHA.106.68531317470709
- Guo L, Zhong L, Chen K, Wu J, Huang RC. Long-term clinical outcomes of optimal medical therapy vs. successful percutaneous coronary intervention for patients with coronary chronic total occlusions. Hellenic J Cardiol. 2018;59:281–287. doi:10.1016/j.hjc.2018.03.00529605686
- Tajstra M, Pyka L, Gorol J, et al. Impact of chronic total occlusion of the coronary artery on long-term prognosis in patients with ischemic systolic heart failure: insights from the COMMIT-HF Registry. JACC Cardiovasc Interv. 2016;9(17):1790–1797. doi:10.1016/j.jcin.2016.06.00727609252
- Guo L, Meng S, Lv H, et al. Long-term outcomes of successful recanalization compared with optimal medical therapy for coronary chronic total occlusions in patients with and without left ventricular systolic dysfunction. Front Cardiovasc Med. 2021;8:654730. doi:10.3389/fcvm.2021.65473033959643
- Galassi AR, Boukhris M, Toma A, et al. Percutaneous coronary intervention of chronic total occlusions in patients with low left ventricular ejection fraction. JACC Cardiovasc Interv. 2017;10(21):2158–2170. doi:10.1016/j.jcin.2017.06.05829055762
- Guo L, Lv H, Zhong L, et al. Comparison of long-term outcomes of medical therapy and successful recanalisation for coronary chronic total occlusions in elderly patients: a report of 1294 patients. Cardiovasc Diagn Ther. 2019;9(6):586–595. doi:10.21037/cdt.2019.11.0132038948
- Guo L, Lv H, Zhong L, et al. Gender differences in long-term outcomes of medical therapy and successful percutaneous coronary intervention for coronary chronic total occlusions. J Interv Cardiol. 2019;24:484–488.
- Hoye A, Van Domburg RT, Sonnenschein K, Serruys PW. Percutaneous coronary intervention for chronic total occlusions: the Thoraxcenter experience 1992–2002. Eur Heart J. 2005;26(24):2630–2636. doi:10.1093/eurheartj/ehi49816183693
- Behnes M, Mashayekhi K, Kuche P, et al. Prognostic impact of coronary chronic total occlusion on recurrences of ventricular tachyarrhythmias and ICD therapies. Clin Res Cardiol. 2020;110(2):281–291. doi:10.1007/s00392-020-01758-y33150467
- Chi WK, Gong M, Bazoukis G, et al. Impact of coronary artery chronic total occlusion on arrhythmic and mortality outcomes: a systematic review and meta-analysis. JACC Clin Electrophysiol. 2018;4(9):1214–1223. doi:10.1016/j.jacep.2018.06.01130236396
- Mannem S, Rattanawong P, Riangwiwat T, et al. Sex difference and outcome after percutaneous intervention in patients with chronic total occlusion: a systematic review and meta-analysis. Cardiovasc Revasc Med. 2020;21(1):25–31. doi:10.1016/j.carrev.2019.03.003
- Cheney A, Kearney KE, Lombardi W. Sex-based differences in chronic total occlusion management. Curr Atheroscler Rep. 2018;20(12):60. doi:10.1007/s11883-018-0760-830406420
- Mehran R, Claessen BE, Godino C, Dangas GD, Obunai K. Long-term outcome of percutaneous coronary intervention for chronic total occlusions. JACC Cardiovasc Interv. 2011;4(9):952–961. doi:10.1016/j.jcin.2011.03.02121939934
- Kim GS, Kim BK, Shin DH, et al. Predictors of poor clinical outcomes after successful chronic total occlusion intervention with drug-eluting stents. Coron Artery Dis. 2017;28(5):381–386. doi:10.1097/MCA.000000000000049828542030
- Davi G, Catalano I, Averna M, et al. Thromboxane biosynthesis and platelet function in type II diabetes mellitus. N Engl J Med. 1990;322(25):1769–1774. doi:10.1056/NEJM1990062132225032345567
- Schofield I, Malik R, Izzard A, Austin C, Heagerty A. Vascular structural and functional changes in type 2 diabetes mellitus: evidence for the roles of abnormal myogenic responsiveness and dyslipidemia. Circulation. 2002;106(24):3037–3043. doi:10.1161/01.CIR.0000041432.80615.A512473548
- Shen Y, Ding FH, Dai Y, et al. Reduced coronary collateralization in type 2 diabetic patients with chronic total occlusion. Cardiovasc Diabetol. 2018;17(1):26. doi:10.1186/s12933-018-0671-629422093
- Meier P, Hemingway H, Lansky AJ, Knapp G, Pitt B, Seiler C. The impact of the coronary collateral circulation on mortality: a meta-analysis. Eur Heart J. 2012;33(5):614–621. doi:10.1093/eurheartj/ehr30821969521
- Cinar T, Hayiroglu MI, Seker M, et al. The predictive value of age, creatinine, ejection fraction score for in-hospital mortality in patients with cardiogenic shock. Coron Artery Dis. 2019;30(8):569–574. doi:10.1097/MCA.000000000000077631490203
- Hayiroglu MI, Bozbeyoglu E, Yildirimturk O, Tekkesin AI, Pehlivanoglu S. Effect of acute kidney injury on long-term mortality in patients with ST-segment elevation myocardial infarction complicated by cardiogenic shock who underwent primary percutaneous coronary intervention in a high-volume tertiary center. Turk Kardiyol Dern Ars. 2020;48(1):1–9.
- Tian T, Guan C, Gao L, et al. Predictors for adverse outcomes of patients with recanalized chronic total occlusion lesion. Eur J Clin Invest. 2021;51(2):e13368. doi:10.1111/eci.1336832748956
- Godino C, Bassanelli G, Economou FI, et al. Predictors of cardiac death in patients with coronary chronic total occlusion not revascularized by PCI. Int J Cardiol. 2013;168(2):1402–1409. doi:10.1016/j.ijcard.2012.12.04423317549
- Guo L, Lv H, Huang R. Percutaneous coronary intervention in elderly patients with coronary chronic total occlusions: current evidence and future perspectives. Clin Interv Aging. 2020;15:771–781. doi:10.2147/CIA.S25231832546995
- Guo L, Ding H, Lv H, et al. Impact of renal function on long-term clinical outcomes in patients with coronary chronic total occlusions: results from an observational single-center cohort study during the last 12 years. Front Cardiovasc Med. 2020;7:550428. doi:10.3389/fcvm.2020.55042833304926
- Jones DA, Weerackody R, Rathod K, et al. Successful recanalization of chronic total occlusions is associated with improved long-term survival. JACC Cardiovasc Interv. 2012;5(4):380–388. doi:10.1016/j.jcin.2012.01.01222516393
- Morino Y, Abe M, Morimoto T, et al. Predicting successful guidewire crossing through chronic total occlusion of native coronary lesions within 30 minutes: the J-CTO (Multicenter CTO Registry in Japan) score as a difficulty grading and time assessment tool. JACC Cardiovasc Interv. 2011;4(2):213–221. doi:10.1016/j.jcin.2010.09.02421349461
- Tokarek T, Dziewierz A, Plens K, et al. Radial approach expertise and clinical outcomes of percutanous coronary interventions performed using femoral approach. J Clin Med. 2019;8(9):1484. doi:10.3390/jcm8091484