Abstract
Background
Using telemedicine for older adults with multiple comorbid conditions is a potential area for growth in health care. Given this older, ailing population, providers should discuss end-of-life care with patients.
Objective
To determine the relationship between telemonitoring and hospice enrollment compared to usual care among older adults with chronic health problems.
Methods
This was a secondary evaluation of a randomized controlled trial. The trial was performed at an academic medical center. Patients who were over the age of 60 and had a high risk of hospitalization and emergency department visits were recruited to the study. The primary outcome was hospice enrollment, and the secondary outcome was the mean number of days in hospice. The data were analyzed using Chi-squared tests and time-to-event analysis.
Results
The average age of the cohort was 80.3 years. Nine patients (9.6%) in the telemonitoring group were enrolled in hospice care, whereas four patients (4.0%) in the usual care group were enrolled (P = 0.12). The mean number of days in hospice was 57.9 (SD ± 99.2) for the telemonitoring group, and 119.3 (SD ± 123.8) for the usual care group (P = 0.36). There was no significant difference regarding time to hospice referral.
Conclusion
In this pilot analysis, there were no differences noted between groups in the number of patients that entered into hospice or the amount of time they stayed in hospice care. This was a small trial, and the power to detect a difference was 36%. It was encouraging that twice the number of patients enrolled in hospice care in the telemonitoring group compared to usual care despite the insignificant finding. Further research may determine the effect of telemonitoring upon hospice referral.
Introduction
Case management and telemonitoring are important clinical practice strategies for older adults with chronic health conditions. Indeed, many patients have clinically advanced conditions that require intensive monitoring, and this may sometimes be completed through the use of telemonitoring. For older at-risk adults, providers will likely place greater emphasis on case management. In many previous telemonitoring trials, investigators studied hospitalizationCitation1,Citation2 or process measures like hemoglobin A1c levels.Citation3 Patients care about these outcomes; however, researchers have not evaluated the effects of telemonitoring on hospice enrollment. Risk-stratified patients receiving telemonitoring suffer chronic medical conditions that place them at risk for hospitalization. These chronically ill patients may require hospice care. In this medically complex cohort, mortality may be as high as 22% over a 2-year time period.Citation4 Providers may encourage end-of-life discussions while patients are under intense disease monitoring, as both the provider and the patient learn more about the prognosis of the chronic illness.
One important aspect of telemonitoring is that it may be a potential route through which to offer hospice services to appropriate patients. The literature describes telemonitoring in hospice care after patients have been enrolled in hospice. It is evident that hospice visits through the use of a videophone may improve the quality of life for hospice patients.Citation5 With the frequent monitoring of patients, one might expect that a patient’s prognosis and the options surrounding hospice care (if appropriate) might be discussed. However, it is unclear whether intensive patient management using telemonitoring alone influences hospice referrals. To answer this question, we performed a secondary analysis of the data from a previous randomized controlled trialCitation6 to assess the impact of telemonitoring versus usual care in hospice admissions among older at-risk adults in the community. We hypothesized that older adults receiving telemonitoring will have a higher rate of hospice referrals compared to those receiving usual care.
Methods
The specific details of the study protocol have been published previously.Citation7 The following methods provide an overview of the study. This study was approved by the Mayo Clinic Institutional Review Board.
Design
This was a randomized controlled trial of older adults accessing health care services at four sites in southeastern Minnesota. Three sites were in Rochester and one was in rural Kasson. Changes to the trial (enrollment, design, outcomes) were not made after initiation of the study.
Participants
All subjects were over the age of 60 and had a primary care provider at the Mayo Clinic. Subjects were stratified based on an Elder Risk Assessment (ERA) score above 15.Citation8 Participants were selected if they were considered to be at high risk for future hospital stays. Patients’ ERA scores were based on age, days of previous hospitalization, and comorbid conditions like heart disease, diabetes, chronic obstructive pulmonary disease, and dementia.
Exclusion
Patients were excluded from the study if they were diagnosed with dementia during pre-enrollment screening. They were also excluded if they were enrolled in a hospice prior to randomization; this information was obtained via self-report. Patients were excluded if they could not speak English. Patients unable to use the telemonitoring device were also excluded.
Interventions
The Intel® Health Guide (Intel Corporation, Santa Clara, CA) is a Food and Drug Administration-approved device that was used daily by the intervention group. Patients in the telemonitoring group relayed biometric and clinical information asynchronously to a registered nurse, who reviewed this information daily. When required, the medical care team would communicate with the patient via phone or videoconferencing. The telemonitoring program did not include a specific program, checklist, guideline, or algorithm for enrollment into hospice care. Patients were enrolled in hospice care when deemed clinically appropriate by the primary care doctor.
Usual care was applied to both the telemonitoring and usual care groups. Patients in both groups had full access to primary and specialty care. They had access to a nurse by telephone, they also had access to the emergency department, and they were provided with follow-up phone calls after a hospital visit. In addition, patients had access to in-hospital palliative care, outpatient palliative care, and hospice care.
Outcomes
While enrolled in the study, the primary outcome measured was hospice referral. Patients and their primary physician made the mutual clinical decision for hospice entry. Secondary outcomes included the amount of time spent in hospice, measured both as a mean and median, and the time to hospice referral after enrollment in the study. The referral to any hospice was clearly documented in the electronic medical record (EMR).
Predictor variables
At baseline, initial characteristics were compared between groups. These included demographic factors (age, sex) and functional factors (grip strength, gait speed, and results on the Timed Up and Go test). The predictors also included the scores from the following assessment measures: the ERA,Citation8 the Kokmen Short Test of Mental Status (dementia),Citation9 the SF-12® (mental and physical subscales for quality of life; Mental Outcomes Trust, Hanover, NH),Citation10 the Patient Health Questionnaire nine-item scale (depression), and the Barthel Index.Citation11 We measured grip strength using a gripstrength dynamometer.Citation12 Gait speed was reported in meters per second; gait speed of less than 1 meter per second has previously been associated with increased mortality.Citation13 The Timed Up and Go test involves having a patient start from a seated position, stand, walk, turn, and return to his or her seat. The Timed Up and Go test has commonly been used as a predictor for falls.Citation14,Citation15
Data collection
The outcomes data were collected directly from each patient’s clinical chart using the EMR. The Mayo Clinic has a comprehensive EMR that records all encounters with the patient. The entry of patients into hospices was clearly recorded.
Sample size
The sample size was designed to evaluate hospitalizations.Citation6 This study represents a secondary analysis of this cohort, and was not initially powered to look directly at hospice enrollment.
Randomization and blinding
The study used block randomization based on each patient’s site of primary care enrollment. The blocks encompassed two to four individuals. The method of randomization was computer-generated by a statistician who was not involved with the analysis. The randomization decisions were placed in sequential, sealed envelopes. This study was not blinded because of the practical limitations of the intervention. Analysis of the outcomes was blinded to group type.
Statistical methods
Descriptive statistics will be used to review the characteristics of the overall cohort. Our previous study revealed that there were no baseline differences between the telemonitoring group and the usual care group, and no adjustments to the outcomes were made.Citation6 The demographics, comorbid conditions, and the patient’s overall quality of life will be reported and compared between the intervention group and the usual care group at baseline. The primary outcome of hospice enrollment will be analyzed using logistic regression analysis. Time-to-event analysis will be used to examine the time to hospice referral and time to death in hospice patients. All tests will assume a two-sided P-value with significance at 0.05. All analyses were run on SAS 9.2 (SAS Institute, Inc, Cary, NC).
Results
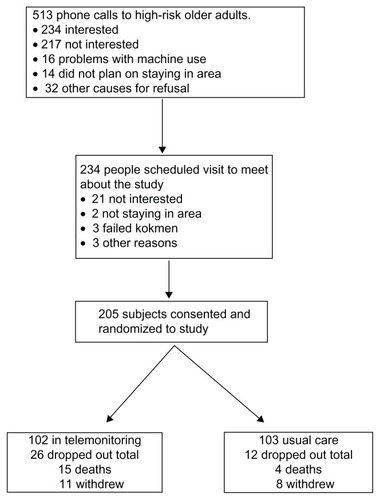
A total of 205 participants were enrolled in the study. The characteristics of this cohort have been previously discussed.Citation6 The initial flow of patients is noted in .Citation6 The study was conducted from November 2009 until July 2011 and was completed when both the enrollment and time goals were reached. There were no clinical differences between the intervention group and the usual care group (). The SF-12® mental scores were slightly different between both groups; however, the results were not adjusted as a result of this difference.
Table 1 Baseline characteristics of overall group and by randomized group for 205 patients
Figure 1 Flow of patients from recruitment to randomization for 205 patients over 60 years.
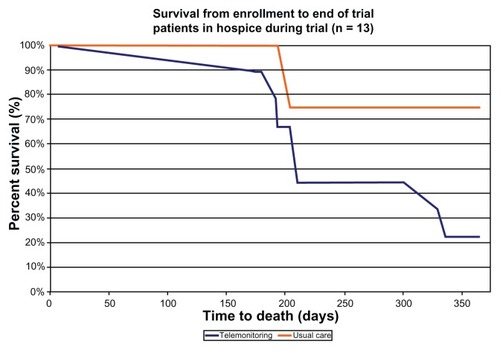
Regarding the primary outcome of hospice referral, nine patients (9.6%) in the telemonitoring group were enrolled in hospice care, compared to four patients (4.0%) in the usual care group, although this result was insignificant (P = 0.12). The mean number of days from time of enrollment in the trial and concluding with entry into hospice care was not different between the two groups. The mean number of days in hospice care tended to be higher in the usual care group with an average of 119.3 days (SD ± 123.8 days) when compared to the intervention group, who stayed in hospice for an average of 57.9 days (SD ± 99.2 days). The median numbers of days in hospice care were 106.0 days and 27.0 days, respectively. These findings are noted in . The time-to-event curves for both entry into hospice after study enrollment () and mortality () were not different between the two groups. Of the nine hospice patients in the telemonitoring group, seven were referred to local hospices and two were referred to the Mayo Hospice. In usual care, two of the four patients were referred to the Mayo Hospice. For patients in the Mayo Hospice, there was no difference in the number of hospice visits (face-to-face) between the intervention group (13.8 notes; SD ± 24.4) and the usual care group (14.5 notes; SD ± 17.4). Information on the number of visits to the regional hospices was not available.
Table 2 Hospice referrals in telemonitoring and usual care in 205 older adults
Figure 2 Time from enrollment to hospice entry among patients enrolled in hospice (n = 13).
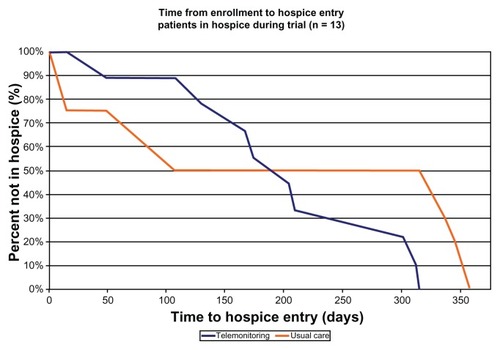
Figure 3 Survival from enrollment in hospice care (n = 13).
The power analysis was calculated based on the above findings from this exploratory study. Using the outcome of hospice enrollment, one finds a 36% power to detect a difference in hospice enrollment between telemonitoring and usual care. This assumes a one-sided Chi-squared test of 0.05 with 9/94 patients in telemonitoring and 4/100 usual care patients. To attain 80% statistical power in the present study in order to detect a difference between both groups, the study would require 284 patients in each arm (total n = 568).
Discussion
In this analysis we explored at-risk older adults using telemonitoring versus those receiving usual care as part of their health care plan. We did not find any differences in the utilization of hospice care between patients who used telemonitoring and those who did not. Although this difference was not significant, more patients enrolled in hospice care overall, with 9 of 94 participants (9.6%) in the telemonitoring group enrolling in a hospice, compared to 4 of 100 subjects (4.0%) enrolling in a hospice in the usual care group (P = 0.12). There were no significant differences found between the groups regarding time until entry into hospice. The average and median times in hospice were longer in the usual care group compared to the telemonitoring group, but these results were also not significant. These findings are not conclusive and serve as initial pilot information for future work with community-based telemonitoring. To our knowledge, hospice enrollment has not been assessed as an outcome in previous telemonitoring studies. It should be noted that this pilot study was underpowered with a power calculation of 36% pertaining to the number of outcomes in our population. It is possible that different case management programs involving telemonitoring can help with end-of-life discussions and appropriate referrals to hospice. Given that high mortality rates are expected among older patients with complex, chronic health conditions, it is possible that hospice care might be appropriate for many individuals in this population.
The primary limitation of this study concerned the small number of subjects involved with this trial. Hospice enrollment was an uncommon event despite the number of medically complex patients. It should be noted that this analysis was a secondary evaluation of data from a previous randomized controlled trial, and it was not powered to detect a full effect. A second potential limitation is that this study did not employ a specific intervention through which to evaluate and enroll patients into hospice care. From this standpoint, a specific intervention or set of guidelines may have increased hospice enrollment. There are also other potential biases in this study. Subjects were not blinded because the presence of a telemonitoring device in the home prevented blinding. This could lead to the Hawthorne effect and to clinical differences in care due to more intensive monitoring.Citation16 The psychological bias associated with telemonitoring could potentially shift the subjects towards health care that is more medically aggressive than hospice care. The primary care team was aware of the intervention (ie, the use of the telemonitoring device); however, the decision for hospice care was determined by clinical necessity. The entry into hospice was well documented in the EMR, and deaths that occurred during the study were also recorded. The Mayo Clinic has an extensive EMR with an informatics infrastructure, which captures outcomes like palliative care, hospice enrollment, and death.Citation17 Lastly, measuring the number of home hospice visits performed by nurses as a secondary outcome was challenging because many patients were in a private hospice, and therefore we did not have access to the number of hospice visits received by the patients.
Although the evidence for hospice entry and telemonitoring are limited, previous studies have explored the relationship between case management and hospice enrollment. Heart failure is a common illness for case management and was the primary condition for the largest randomized trial in telemedicine.Citation1 In patients dying of heart failure and who were eligible to be enrolled in a hospice, only 18.4% received hospice care.Citation18 Within the nursing home population, a structured evaluation for goals of care resulted in 20% enrollment among the hospice evaluation intervention versus 1% in the usual care group.Citation19 Some qualitative studies indicate that multiple barriers (like psychosocial factors) can affect hospice referral outside of medical eligibility.Citation20 Despite these barriers, some studies have indicated that increased hospice referral arises from case management. A 2009 study of a comprehensive case management program resulted in increased numbers of patients accessing hospice care, and the average length of hospital stay also increased. The authors found that hospice referrals increased from 30.8% to 71.7% among group members who were in a case management program compared to controls, respectively.Citation21 Thus, it may be possible that telemonitoring increases hospice referrals; however, future research will likely require a specific intervention to further demonstrate this effect, as the use of monitoring by itself may not be adequate.
One important finding from this study involves the overall length of stay (LOS) within hospice care. The overall average LOS in the cohort as a whole was 76.8 days (SD ± 106.1), and within the telemonitoring cohort, the LOS was 57.9 days (SD ± 99.2); these findings were compared to data from 2007 that reported an overall national cohort level LOS of 65 days.Citation22 Thus, the study findings are consistent with national benchmark standards for average LOS and median LOS. Interestingly, the median LOS was 106 days in the usual care group, which was much longer than benchmark averages. Given the small number of overall hospice referrals (n = 4), it is difficult to draw conclusions from this finding. Many recognize that there appears to be a dichotomous pattern of short stays in hospice (just before death) and long stays in hospice.Citation23 In our study, we found a similar pattern, with the median and mean LOS days diverging considerably. One goal of telemonitoring would be to increase the utilization of palliative care and hospice services. We did not see this increase within our study, perhaps because the study was small and underpowered.
Future directions of this pilot study offer researchers the chance to answer a number of different questions. A larger trial with adequate numbers (potentially up to 568) will shed further light on the relationship between telemonitoring and hospice enrollment. Future studies should implement specific guidelines and infrastructure to increase hospice enrollment when appropriate. Furthermore, investigating palliative care and hospice outcomes in this high-risk group might be important for future work. More importantly, initiating a discussion surrounding palliative care and end-of-life issues might be appropriate for this population.
Conclusion
In this small, randomized controlled trial, patients who were randomized to telemonitoring did not enter hospice more frequently or spend a greater length of time in hospice. The study was small, with 205 subjects, and was underpowered. In spite of this, more people did enroll in hospice care after using telemonitoring services (9.6%) compared to usual care (4.0%). It is hoped that with larger trials, one can fully determine the relationship between telemonitoring and hospice enrollment.
Acknowledgments
We acknowledge Betty Wirt and Jenny Hurt for their help in study coordination. The authors would also like to thank Jody Clikeman from Mayo Clinic Grant and Publication Support Services for providing editorial assistance.
Disclosure
Intel provided the Intel® Health Guides and technical support. The authors received research support from the Mayo Clinic. No competing financial interests exist.
References
- ChaudhrySIMatteraJACurtisJPTelemonitoring in patients with heart failureN Engl J Med2010363242301230921080835
- WoodendAKSherrardHFraserMStueweLCheungTStruthersCTelehome monitoring in patients with cardiac disease who are at high risk of readmissionHeart Lung2008371364518206525
- TriefPMTeresiJAEimickeJPSheaSWeinstockRSImprovement in diabetes self-efficacy and glycaemic control using telemedicine in a sample of older, ethnically diverse individuals who have diabetes: the IDEATel projectAge Ageing200938221922519171951
- TakahashiPYTungEECraneSJChaudhryRChaSHansonGJUse of the elderly risk assessment (ERA) index to predict 2-year mortality and nursing home placement among community dwelling older adultsArch Gerontol Geriatr2012541343821397346
- DemirisGOliverDPWittenberg-LylesEWashingtonKUse of videophones to deliver a cognitive-behavioural therapy to hospice caregiversJ Telemed Telecare201117314214521303934
- TakahashiPYPecinaJLUpatisingBA randomized controlled trial of telemonitoring in older adults with multiple health issues to prevent hospitalizations and emergency department visitsArch Intern Med20121721077377922507696
- TakahashiPYHansonGJPecinaJLA randomized controlled trial of telemonitoring in older adults with multiple chronic conditions: the Tele-ERA studyBMC Health Serv Res20101025520809953
- CraneSJTungEEHansonGJChaSChaudhryRTakahashiPYUse of an electronic administrative database to identify older community dwelling adults at high-risk for hospitalization or emergency department visits: the elders risk assessment indexBMC Health Serv Res20101033821144042
- KokmenENaessensJMOffordKPA short test of mental status: description and preliminary resultsMayo Clin Proc19876242812883561043
- WareJJrKosinskiMKellerSDA 12-Item Short-Form Health Survey: construction of scales and preliminary tests of reliability and validityMed Care19963432202338628042
- WadeDTCollinCThe Barthel ADL Index: a standard measure of physical disability?Int Disabil Stud198810264673042746
- WangCYChenLYGrip strength in older adults: test-retest reliability and cutoff for subjective weakness of using the hands in heavy tasksArch Phys Med Rehabil11201091111747175121044721
- CesariMKritchevskySBPenninxBWPrognostic value of usual gait speed in well-functioning older people – results from the Health, Aging and Body Composition StudyJ Am Geriatr Soc200553101675168016181165
- BeauchetOFantinoBAllaliGMuirSWMontero-OdassoMAnnweilerCTimed Up and Go test and risk of falls in older adults: a systematic reviewJ Nutr Health Aging2011151093393822159785
- PodsiadloDRichardsonSThe timed “Up and Go”: a test of basic functional mobility for frail elderly personsJ Am Geriatr Soc19913921421481991946
- McCarneyRWarnerJIliffeSvan HaselenRGriffinMFisherPThe Hawthorne Effect: a randomised, controlled trialBMC Med Res Methodol200773017608932
- HerasevichVPickeringBWDongYPetersSGGajicOInformatics infrastructure for syndrome surveillance, decision support, reporting, and modeling of critical illnessMayo Clin Proc201085324725420194152
- BerryJIHospice and heart disease: missed opportunitiesJ Pain Palliat Care Pharmacother2010241232620345196
- CasarettDKarlawishJMoralesKCrowleyRMirschTAschDAImproving the use of hospice services in nursing homes: a randomized controlled trialJAMA2005294221121716014595
- WalsheCChew-GrahamCToddCCaressAWhat influences referrals within community palliative care services? A qualitative case studySoc Sci Med200867113714618433963
- SpettellCMRawlinsWSKrakauerRA comprehensive case management program to improve palliative careJ Palliat Med200912982783219719372
- CaffreyCSenguptaMMossAHarris-KojetinLValverdeRHome health care and discharged hospice care patients: United States, 2000 and 2007Natl Health Stat Report20113812721568135
- ConnorSRUS hospice benefitsJ Pain Symptom Manage200938110510919615634