Abstract
Background
The purpose of this study was to evaluate the extubation process in bed-ridden elderly intensive care patients receiving inspiratory muscle training (IMT) and identify predictors of successful weaning.
Methods
Twenty-eight elderly intubated patients in an intensive care unit were randomly assigned to an experimental group (n = 14) that received conventional physiotherapy plus IMT with a Threshold IMT® device or to a control group (n = 14) that received only conventional physiotherapy. The experimental protocol for muscle training consisted of an initial load of 30% maximum inspiratory pressure, which was increased by 10% daily. The training was administered for 5 minutes, twice daily, 7 days a week, with supplemental oxygen from the beginning of weaning until extubation. Successful extubation was defined by the ventilation time measurement with noninvasive positive pressure. A vacuum manometer was used for measurement of maximum inspiratory pressure, and the patients’ Tobin index values were measured using a ventilometer.
Results
The maximum inspiratory pressure increased significantly (by 7 cm H2O, 95% confidence interval [CI] 4–10), and the Tobin index decreased significantly (by 16 breaths/ min/L, 95% CI −26 to 6) in the experimental group compared with the control group. The Chi-squared distribution did not indicate a significant difference in weaning success between the groups (χ2 = 1.47; P = 0.20). However, a comparison of noninvasive positive pressure time dependence indicated a significantly lower value for the experimental group (P = 0.0001; 95% CI 13.08–18.06). The receiver-operating characteristic curve showed an area beneath the curve of 0.877 ± 0.06 for the Tobin index and 0.845 ± 0.07 for maximum inspiratory pressure.
Conclusion
The IMT intervention significantly increased maximum inspiratory pressure and significantly reduced the Tobin index; both measures are considered to be good extubation indices. IMT was associated with a reduction in noninvasive positive pressure time in the experimental group.
Introduction
Maximum respiratory system function is reached between the ages of approximately 20 and 25 years. As people age, there is a gradual reduction in pulmonary performance, and in elderly people these physiological alterations can seriously impact cardiorespiratory functional reserve.Citation1 In addition, respiratory muscle strength is also affected by poor nutrition and sarcopenia, both of which are associated with aging and bedridden patients.Citation2–Citation4
In 20%–25% of cases, patients have difficulty in discontinuing the use of mechanical ventilation.Citation5 Weaning begins with the reduction of ventilatory support, at which point the patients become capable of some independent ventilation, and ends with removal of the patient from mechanical ventilation, including extubation (removal of the endotracheal tube).Citation6,Citation7
Numerous indices have been utilized to predict the success of interruption of ventilatory and extubation following mechanical ventilation. These different indices reflect the mechanics of respiration, ie, pulmonary gas exchange, respiratory control, and functioning of the respiratory musculature.Citation8 Although there are a variety of predictors, Vallverdú et alCitation9 observed that the Tobin index and maximum inspiratory pressure are good predictors of weaning success. A common finding in patients who fail weaning and extubation is a raised Tobin index (respiratory frequency/ vital capacity, in liters).Citation10 Currently, maximum inspiratory pressure is used to evaluate the strength of the inspiratory musculature.Citation11
Chronic dependence on mechanical ventilation is not only a major medical problem,Citation2 but also produces extreme discomfort for patients, with important physiological complications and negative social implications and restrictions.Citation12 Therefore, some investigators have suggested use of inspiratory muscle training (IMT) to reduce respiratory muscle fatigueCitation13 and facilitate weaning from mechanical ventilation.Citation14 However, these studies have only involved tracheostomized patients. This study aimed to evaluate the extubation process in bedridden elderly patients receiving IMT and correlate successful predictors of weaning.
Materials and methods
Sample
A randomized trial was conducted with participants from the intensive care unit of a single hospital in Brazil. After confirming their eligibility and baseline measurements, the participants were randomly allocated to either an experimental group or a control group. The enrolling investigator contacted another investigator to request participant allocation from a concealed list of random allocations that had been generated by drawing numbers from a bag. This other investigator was not otherwise involved in the study.
During the recruitment period, 198 patients were screened, and 67 were eligible and monitored daily to assess their readiness to begin weaning. Of these 67 patients, 20 were tracheostomized, five died, and one was transferred to another center before weaning began. The remaining 41 were randomized, with 21 assigned to the experimental group and 20 to the control group. However, four participants in each group died before extubation. Three participants in the experimental group and two in the control group were tracheostomized before extubation. The experimental group (n = 14, age 82 ± 4 years, mechanical ventilation period 10 days) underwent conventional physiotherapy plus IMT with a Threshold IMT® device (Philips Respironics, Murrysville, PA), and the control group (n = 14, age 81 ± 6 years, mechanical ventilation period 11 days) received only conventional physiotherapy that favored inspiratory muscle strengthening.
To be included, the sample participants were required to have undergone mechanical ventilation for at least 48 hours in a controlled manner,Citation13 because intubation is diagnostic for acute respiratory injury type 1 and has a maximum inspiratory pressure value of −20 cm H2O.15
Patients were excluded if they had any type of acute condition (eg, cardiac arrhythmia) or chronic condition (eg, insufficient congestive heart failure) that could compromise weaning or impede the inspiratory muscle training (neuropathy, myopathy). Tracheostomized patients (in the pretest), patients with neurological problems (cerebral vascular accident, cerebrospinal trauma, spinal medullar trauma), morbidly obese patients, patients receiving medicine that could cause attention disorders, and cases of autoextubation were also excluded. The inclusion and exclusion criteria were evaluated via examination of the patients’ medical records and daily physical examination. Informed consent was obtained from the patients’ representatives, and the experimental procedures were conducted in accordance with the 1975 Declaration of Helsinki.Citation16 This study was submitted to and approved by the Committee of Ethics in Research Involving Human Beings of the Euro-American Network of Human Kinetics (protocol number 005/2007). This trial is registered at ClinicalTrials.gov as NCT0922493.
Procedures
The evaluation procedures used during pretesting (the first day that the patient initiated ventilation with support pressure) and post-testing (before extubation) were maximum inspiratory pressure and the Tobin index (rate of breath/tidal volume in liters). The outcomes were measured or recorded by physiotherapists in the intensive care unit.
Maximum inspiratory pressure measurements
Before training, it was necessary to evaluate maximum inspiratory pressure using a vacuum manometer (Critical Care, US, Rio de Janeiro, Brazil). Marini et alCitation17 suggested an evaluation method that requires little contribution from the patient. The equipment is attached to the orotracheal tube via a connector with an expiratory unidirectional valve, which means there is no resistance in the patient’s expiration. Therefore, the individual is obliged to make an inspiratory effort to start the respiratory cycle, at which point the maximum inspiratory pressure is measured. An evaluation duration of 25 seconds produces the best results.Citation18 The patients are placed in a dorsal decubitus position with the backrest raised 45 degrees.Citation19 The maximum inspiratory pressure cutoff point to be considered for study purposes is −20 cm H2O.Citation20
Measurement of rapid shallow breathing
A Mark 8 mechanical ventilometer was used (DHD Medical Products, Brooklyn, NY) to calculate the Tobin index. First, the patient was disconnected from the ventilatory prosthesis. Next, the ventilometer was attached to the connecting piece of tube; for one minute, the patient was allowed to breathe spontaneously,Citation15 and the current volume and respiratory frequency were measured. For the purposes of the study, the Tobin index cutoff point was 100 ipm/L.Citation21 Inspiratory muscle training was conducted on the first day that the patient initiated spontaneous ventilation and continued until the moment before extubation.
Threshold IMT inspiratory muscle training protocol
After maximum inspiratory pressure was measured, inspiratory muscle training was initiated. The Threshold-IMT device generates a linear pressure load that produces resistance to inspiration through use of a flow-independent one-way valve. The suggested protocol is as follows: an initial load of 30% of the maximum inspiratory pressure, increasing daily by 10%, with training for 5 minutes, twice a day, 7 days a week, from the beginning of mechanical ventilation weaning until extubation of the patient.Citation22 An essential factor is the use of supplemental oxygen as needed by the patient.
The training was interrupted when respiratory insufficiency and/or hemodynamic instability was observed with any of the following: respiratory frequency ≥ 35 ipm (or higher than 50% of the initial value); SpO2 < 90%; systolic pressure > 180 mmHg or <80 mmHg and tachycardia > 140 beats per minute or 20% higher than the initial measurement; paradoxical breathing; agitation; depression; hemoptysis; and arrhythmia and/or sweating.Citation23 If any of the above clinical signs were observed, the next training session did not involve an additional load. Instead, the training was conducted at the previous level.
The control group followed the protocol of conventional physiotherapy with a reduction in support pressure to 8 cm H2O, but without any specific training to strengthen the respiratory musculature. The conventional physiotherapy intervention included passive-assisted to active-assisted mobilization of the limbs, chest compression, decompression traction chest, aspiration of the endotracheal tube, and positioning. Physiotherapy was performed for an average duration of 15 minutes, with the intensity varying according to patient cooperation and vital signs.
For extubation, patients were required to satisfy the following conditions: improvement in the underlying etiology that resulted in respiratory insufficiency, a cough reflex, hemodynamic stability, nonfebrile (body temperature ≤ 38°C), no vasoactive drug use (with the exception of dopamine 5 mg/kg per minute), stable electrolyte levels (mainly calcium, magnesium, and phosphate) and a normal radiological evaluation (without pneumothorax, congestion, large pleural effusion, or atelectasis). In addition, mechanical ventilation and blood gas analyses were required to fall within the following parameters: 7.30 < pH < 7.60 and PaCO2 < 60 mmHg,Citation24 inspired fraction of O2 (FiO2) ≤40%, and PaO2/FiO2 ratio ≥ 200.Citation25,Citation26
The patient had to present without signs or parameters of ventilatory discomfort, such as paradoxical breathing, utilization of accessory musculature, respiratory frequency ≥ 35 ipm (or 50% increase), and sweating.
The protocol for extubation was as follows. The support pressure was reduced to 8 cm H2O, ensuring that a minimum volume of 6 mL/kg was maintained. Next, a T-tube was utilized for 30 minutes.Citation27 Extubation was considered a failure if the patient returned to mechanical ventilation within 48 hoursCitation19 or required a tracheostomy.
Statistical analysis
Descriptive statistics, including average and standard deviation, were calculated. The normality of the sample was evaluated with the Shapiro-Wilk test. A kappa test was used to evaluate agreement between the evaluators. A 2 × 2 analysis of variance test was used to compare within groups and between groups, and this was followed by a post-hoc Tukey’s test to identify any possible differences. A Student’s t-test was performed to compare permanence times for the noninvasive positive pressure after extubation. A Chisquare distribution analysis was used to evaluate extubation. Sensitivity and specificity were calculated to evaluate the weaning prediction power of the analyzed variables. In addition, the receiver-operating characteristic (ROC) curve was calculated and plotted. The area below the ROC curve for each variable summarizes the performance of each index in predicting weaning. The statistical significance level adopted was P < 0.05.
Results
The baseline characteristics of the two groups are shown in . Weaning predictor data are presented with the descriptive statistics in . After the pretest and post-test predictor group results (for maximum inspiratory pressure and Tobin index) were compared, the 2 × 2 analysis of variance test indicated significant differences in both variables (P < 0.05). As shown in , there was a significant and unsatisfactory increase in Tobin index for the control group (95% confidence interval [CI] −4.47 to −24.44, P = 0.002) and a satisfactory increase in maximum inspiratory pressure in the experimental group (95% CI 7.09–12.62, P = 0.001). The post-test indicated a significant reduction in Tobin index (95% CI −26.23 to −6.05, P = 0.001) and a significant increase in maximum inspiratory pressure (95% CI 4.67–10.19, P = 0.001) when compared with the control group. A kappa test value of 0.68 suggested good inter-rater reliability. Analysis of the extubation results is shown in .
Table 1 Baseline characteristics of patients in the study
Table 2 Results of descriptive statistics and inferential analysis of predictors of weaning
Figure 1 Evaluation of extubation.
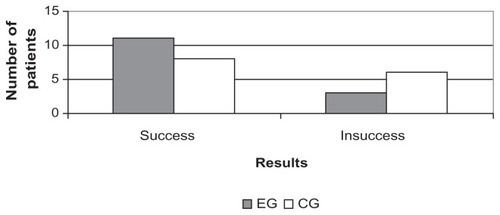
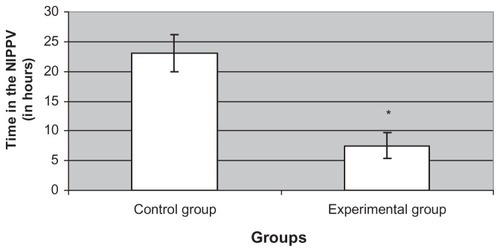
The Chi-squared distribution test detected no significant difference in extubation success between the groups (χ2 = 1.47; P = 0.20), although shorter weaning times were noted in the experimental group (3.64 ± 1.50 days) compared with the control group (5.36 ± 1.87 days). However, hospital protocol required reduced ventilation in patients who underwent noninvasive positive pressure after extubation because the procedure is unfavorable for reintubation. shows a comparison of the noninvasive positive pressure time dependence in each group. Note that the experimental group had reduced dependence on noninvasive positive pressure compared with the control group (95% CI 13.08–18.06, P = 0.0001).
Figure 2 Time on noninvasive positive pressure.
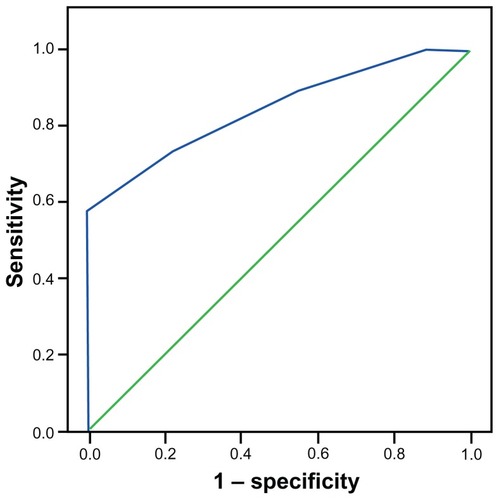
An ROC sensitivity and specificity curve was used to evaluate and compare the weaning predictors with data regarding actual successful extubation. The ROC curve for the Tobin index () had an area below the curve of 0.877 ± 0.06. The sensitivity and the specificity of the Tobin index was 1.00 and 0.36, respectively. Sensitivity and specificity as determined by the ROC curve as shown in . The curve indicated a sensitivity of 0.86 and a specificity of 0.72. The area below the curve was 0.845 ± 0.07.
Figure 3 Receiver-operating characteristic curve for Tobin index.
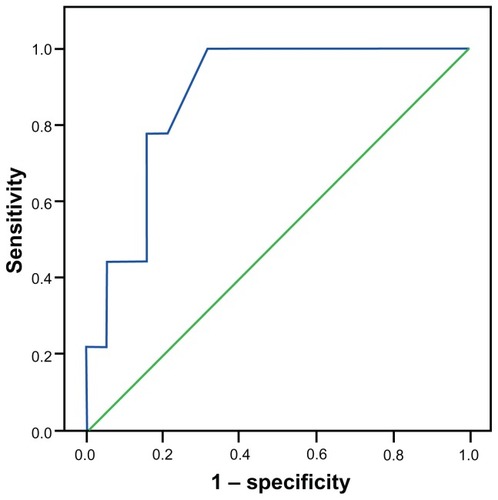
Figure 4 Receiver-operating characteristic curve of maximum inspiratory pressure.
Discussion
Lack of blinding was a limitation of this study. However, informed consent was provided by the relatives of these critically ill patients, so the potential for placebo and Hawthorne effects was reduced. Although we screened 198 patients in the intensive care unit, a large number of these critically ill patients died or were tracheostomized before or after commencement of weaning. This pattern is typical of inspiratory muscle training research in intensive care settings.Citation13,Citation19 As a result, another limitation of the study was its sample size. In addition, inclusion of 10 participants allowed an 80% probability of detecting a difference of 10 cm H2O in maximal inspiratory pressure at a two-sided 5% significance level. We anticipated that a substantial proportion of these critically ill participants would die or receive a tracheostomy, and thus be disqualified from inclusion in our study. Therefore, we increased the sample recruited to 20 to account for possible loss of participants. Therefore, recruitment of 20 participants ensured that the study was adequately powered.
In a study of ventilated patients, Caruso et alCitation28 did not find that ventilator manipulations provided an effective training stimulus for inspiratory muscles. In contrast, two recent randomized trials demonstrated favorable results with IMT using a removable threshold device. The first studyCitation22 examined IMT in 28 ventilated patients aged 70 years and older and found that a twice-daily 5-minute training regimen beginning at an intensity of 30% of maximum significantly increased the inspiratory muscle strength (mean difference in maximum inspiratory pressure of 7.6 cm H2O, 95% CI 5.8–9.4) and a reduction in the weaning period (mean difference of 1.7 days, 95% CI 0.4–3.0). The second studyCitation29 investigated IMT in 69 patients who had failed on conventional weaning methods. These researchers used a high-intensity interval training strategy (ie, four sets of 6–10 breaths) using the highest tolerated resistance. In the IMT group, mean inspiratory muscle strength increased from 44.4–54.1 cm H2O, whereas no significant difference was detectable in the sham training group. The training strategies of the two aforementioned studies involved the same training logistics as those in the present study in that they also centered on high-intensity loads. These studies were the focus of a recent systematic review.Citation30
Although the results regarding the success of extubation were satisfactory in the present study, the measurements were not significantly different when compared with the control group (). However, hospital protocol required that all patients utilize noninvasive positive pressure after extubation, which contributes to airway stabilization and aids in preventing reintubation of patients who might have had extubation issues, as described in the literatureCitation31,Citation32 ().
Limited information is available concerning respiratory muscle training for patients with difficulty weaning,Citation23 although some studies describe the contributions of IMT during mechanical ventilation.Citation13,Citation14 Chang et alCitation33 observed a post-weaning reduction in the inspiratory muscle strength of patients who had undergone a lengthy period of mechanical ventilation. These results are in agreement with those for the control group, as shown in .
shows that the Tobin index has high sensitivity and low specificity, which is in agreement with a study by Yang and Tobin,Citation15 who observed that the Tobin index has a sensitivity of 0.97 and a specificity of 0.64. Utilizing a cutoff of −17 cm H2O for maximum inspiratory pressure, Conti et alCitation23 found a sensitivity of up to 0.95 and a specificity of 0.42. Although the cutoff value is not identical to the one used in our study (−20 cm H2O), the sensitivity and specificity values for maximum inspiratory pressure showed the same trend as those shown in (high sensitivity and low specificity). However, as previously mentioned, the low specificity values also justify use of noninvasive positive pressure ventilation.
Conclusion
From our study sample, it can be inferred that inspiratory muscle training contributed to a significant increase in maximum inspiratory pressure (both within groups and between groups) and a reduction in Tobin index (within groups). These variables are considered good weaning predictors, and their related ROC curves indicate that IMT was associated with reduction in noninvasive positive pressure time in the experimental group.
Disclosure
The authors report no conflicts of interest in this work.
References
- JanssensJPPacheJCNicodLPPhysiological changes in respiratory function associated with ageingEur Respir J199913119720510836348
- AmbrosinoNWeaning and respiratory muscle dysfunction: the egg-chicken dilemmaChest2005128248148316100126
- AlfieriFMRibertoMGatzLSRibeiroCPLopesJABattistellaLRComparison of multisensory and strength training for postural control in the elderlyClin Interv Aging2012711912522654512
- VinsnesAGHelbostadJLNyronningSHarklessGEGranboRSeimAEffect of physical training on urinary incontinence: a randomized parallel group trial in nursing homesClin Interv Aging20127455022334767
- VassilakopoulosTPetrofBJVentilator-induced diaphragmatic dysfunctionAm J Respir Crit Care Med2004169333634114739134
- MeadeMGuyattGCookDPredicting success in weaning from mechanical ventilationChest2001120Suppl 6400S424S11742961
- RobriquetLGeorgesHLeroyODevosPD’EscrivanTGueryBPredictors of extubation failure in patients with chronic obstructive pulmonary diseaseJ Crit Care200621218519016769465
- BrutonAA pilot study to investigate any relationship between sustained maximal inspiratory pressure and extubation outcomeHeart Lung200231214114911910389
- VallverduICalafNSubiranaMNetABenitoSManceboJClinical characteristics, respiratory functional parameters, and outcome of a two-hour T-piece trial in patients weaning from mechanical ventilationAm J Respir Crit Care Med19981586185518629847278
- GoldstoneJThe pulmonary physician in critical care. 10: difficult weaningThorax2002571198699112403884
- VolianitisSMcConnellAKKoutedakisYJonesDASpecific respiratory warm-up improves rowing performance and exertional dyspneaMed Sci Sports Exerc20013371189119311445767
- AppendiniLPurroAPatessioAPartitioning of inspiratory muscle workload and pressure assistance in ventilator-dependent COPD patientsAm J Respir Crit Care Med19961545130113098912740
- ChangATBootsRJBrownMGParatzJHodgesPWReduced inspiratory muscle endurance following successful weaning from prolonged mechanical ventilationChest2005128255355916100137
- Del RosarioNSassoonCSChettyKGGruerSEMahutteCKBreathing pattern during acute respiratory failure and recoveryEur Respir J19971011256025659426095
- YangKLTobinMJA prospective study of indexes predicting the outcome of trials of weaning from mechanical ventilationN Engl J Med199132421144514502023603
- World Medical OrganizationDeclaration of HelsinkiBMJ199631314481449
- MariniJJSmithTCLambVEstimation of inspiratory muscle strength in mechanically ventilated patients: The measurement of maximal inspiratory pressureJ Crit Care1986113238
- CarusoPFriedrichCDenariSDRuizSADeheinzelinDThe unidirectional valve is the best method to determine maximal inspiratory pressure during weaningChest199911541096110110208214
- SpragueSSHopkinsPDUse of inspiratory strength training to wean six patients who were ventilator-dependentPhys Ther200383217118112564952
- AfessaBHogansLMurphyRPredicting 3-day and 7-day outcomes of weaning from mechanical ventilationChest1999116245646110453876
- EpsteinSKCiubotaruRLInfluence of gender and endotracheal tube size on preextubation breathing patternAm J Respir Crit Care Med19961546164716528970349
- CaderSAValeRGCastroJCInspiratory muscle training improves maximal inspiratory pressure and may assist weaning in older intubated patients: a randomised trialJ Physiother201056317117720795923
- ContiGMontiniLPennisiMAA prospective, blinded evaluation of indexes proposed to predict weaning from mechanical ventilationIntensive Care Med200430583083615127195
- VenkataramanSTKhanNBrownAValidation of predictors of extubation success and failure in mechanically ventilated infants and childrenCrit Care Med20002882991299610966284
- MartinezASeymourCNamMMinute ventilation recovery time: a predictor of extubation outcomeChest200312341214122112684314
- Frutos-VivarFFergusonNDEstebanARisk factors for extubation failure in patients following a successful spontaneous breathing trialChest200613061664167117166980
- BolesJMBionJConnorsAWeaning from mechanical ventilationEur Respir J20072951033105617470624
- CarusoPDenariSDRuizSAInspiratory muscle training is ineffective in mechanically ventilated critically ill patientsClinics200560647948416358138
- MartinADSmithBKDavenportPDInspiratory muscle strength training improves weaning outcome in failure to wean patients: a randomized trialCrit Care2011152R8421385346
- MoodieLHReeveJCVermeulenNElkinsMRInspiratory muscle training to facilitate weaning from mechanical ventilation: protocol for a systematic reviewBMC Res Notes2011428321835031
- MattePJacquetLVan DyckMGoenenMEffects of conventional physiotherapy, continuous positive airway pressure and non-invasive ventilatory support with bilevel positive airway pressure after coronary artery bypass graftingActa Anaesthesiol Scand2000441758110669276
- HilbertGGrusonDVargasFNoninvasive ventilation in immunosuppressed patients with pulmonary infiltrates, fever, and acute respiratory failureN Engl J Med2001344748148711172189
- ChangATBootsRJHendersonRParatzJDHodgesPWCase report: inspiratory muscle training in chronic critically ill patients – a report of two casesPhysiother Res Int200510422222616411617