 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Objective
As a standard indicator of renal function, the glomerular filtration rate (GFR) is vital for the prognostic analysis of elderly patients with coronary artery disease (CAD). Thus, the search for the calculation equation of GFR with the best prognostic ability is an important task. The most commonly used Modification of Diet in Renal Disease (MDRD) equation and the Chinese version (CMDRD) of the MDRD equation has many shortcomings. The newly developed Mayo Clinic quadratic (Mayo) and Chronic Kidney Disease (CKD) Epidemiology Collaboration (CKD-EPI) equations may overcome these shortcomings. Because the populations involved in these equation-related studies are almost completely devoid of subjects > 70 years of age, there are more debates on the performance of these equations in the elderly. This study was designed to compare the prognostic abilities of different calculation formulas for the GFR in elderly Chinese patients with CAD.
Methods
This study included 1050 patients (≥60 years of age) with CAD. The endpoint was all-cause mortality over a mean follow-up period of 417 days.
Results
The median age was 86 years (60–104 years). The median values for the MDRD-GFR, CMDRD-GFR, CKD-EPI-GFR, and Mayo-GFR were 66.0, 69.2, 65.6, and 75.8 mL/minute/1.73 m2, respectively. The prevalence of GFR < 60 mL/minute/1.73 m2 based on these measures was 39.3%, 35.4%, 43.0%, and 28.7%, respectively. Their area under the curve values for predicting death were 0.611, 0.610, 0.625, and 0.632, respectively. Their cut-off points for predicting death were 54.1, 53.5, 48.0, and 57.4 mL/minute/1.73 m2, respectively. Compared with the MDRD-GFR, the net reclassification improvement values of the CMDRD-GFR, CKD-EPI-GFR, and Mayo-GFR were 0.02, 0.10, and 0.14, respectively.
Conclusion
The prognostic abilities of the CKD-EPI and Mayo equations were significantly superior to the MDRD and CMDRD equations; the Mayo equation had a mild, but not statistically significant superiority compared with the CKD-EPI equation in elderly Chinese patients with CAD.
Introduction
On a global scale, evolving changes in demographics have led to an aging population, along with an increasing prevalence of renal function impairment in patients with coronary artery disease (CAD).Citation1 The latter might result in a higher mortality rate.Citation2–Citation4 Thus, as the standard indicator of renal function, the glomerular filtration rate (GFR) is vital for the prognostic analysis of elderly patients with CAD. To search for the calculation equation of GFR derived from serum creatinine (Scr) with the best prognostic ability is therefore an important task. The poorer prognostic ability of the most commonly used Modification of Diet in Renal Disease (MDRD) study equation in subjects with an elevated GFR, such as women, younger, and white subjects without comorbidities, has been well-established.Citation5–Citation7 The newly developed Mayo Clinic quadratic (Mayo) and Chronic Kidney Disease (CKD) Epidemiology Collaboration (CKD-EPI) equations consist of the same four variables as the MDRD equation, but may have better prognostic ability.Citation8–Citation10 Race is an important determinant of the GFR calculation. Unfortunately, Asians have not been included in MDRD and CKD-EPI studies; thus the Chinese MDRD (CMDRD) equation is based on the original MDRD equation for use in Chinese patients,Citation11 but there is still no modification of the CKD-EPI equation in the People’s Republic of China. The populations involved in these equation-related studies were almost completely devoid of subjects > 70 years of age, subjects who are known to have the greatest burden of GFR-related adverse outcomes.Citation8,Citation9 Therefore, debates on the performance of these equations in the elderly continue.
Currently, there is no study that has compared the four equations in populations composed mainly of the elderly, men, and Chinese with CAD, as opposed to women, younger, and white subjects without comorbidities. Since these formulas may not perform equally in different subjects, the comparison made between the formulas depends on the subjects under study.Citation12 The current study was designed to compare the prognostic abilities of different calculation formulas for the GFR in elderly Chinese patients with CAD.
Methods
Population
Patients ≥ 60 years of age who were diagnosed with CAD were enrolled in this study. The diagnosis was based on history, symptoms of typical angina, cardiac markers, and specific cardiac examinations, such as an electrocardiogram (resting/exercise), echocardiography, radionuclide imaging, computed tomography, and coronary arteriography, and was performed by chief physicians or associate chief physicians according to the American College of Cardiology/American Heart Association (ACC/AHA) and European Society of Cardiology (ESC) guidelines.Citation13,Citation14 The exclusion criteria included severe aortic stenosis, anticipated cardiac transplantation, and use of a left ventricular assist device. The current study was comprised of 1050 cases, on which the following analysis was based. The Chinese People’s Liberation Army General Hospital was the designated hospital for all patients, and had integrated long-term medical and final death records, which made it easier for us to follow up effectively and judge endpoints accurately. The study protocol was approved by the local Ethics Committee and in accordance with the Helsinki Declaration of 1975 (as revised in 1983).
Baseline variables
All information was carefully obtained, preserved, and verified by trained researchers. The basic characteristics included demographics (age and gender) and physical examination findings (mean systolic blood pressure). The body mass index was defined as the weight in kilograms divided by the square of the height in meters. The Scr concentration was measured using an enzymatic method, and the calibration formula was as follows:Citation15
Jaffe’s kinetic method:
The enzymatic method Scr was used in the CKD-EPI formula, and the Jaffe’s kinetic method Scr was used in the other three formulas. The GFR of all 1050 subjects was evaluated with different equations as follows.
MDRD formula:Citation5
Chinese MDRD formula:Citation11
Mayo Clinic quadratic formula:Citation10
CKD-EPI formulaCitation8
If female and if Scr ≤ 0.7 mg/dL:
If female and if Scr > 0.7 mg/dL:
If male and if Scr ≤ 0.9 mg/dL:
If male and if Scr > 0.9 mg/dL:
Determination of diseases
Hypertension was considered to be present if the systolic blood pressure was ≥140 mmHg, the diastolic blood pressure was ≥90 mmHg, and/or the subject was taking an antihypertensive drug. A subject was considered to have diabetes mellitus if the fasting plasma glucose was ≥7.0 mmol/L, the postprandial blood glucose (2-hour venous blood glucose) was ≥11.1 mmol/L, and/or the subject was taking a hypoglycemic drug or insulin. Atrial fibrillation (AF) and chronic heart failure (CHF) were defined on the basis of the ACC/AHA/ESC 2006 guideline for AF,Citation16 and the ESC 2008 guideline for CHF,Citation17 respectively.
Outcome
Given the priority of all-cause mortality in outcome studies, as well as the high incidence of multiple organ failure in the elderly, all-cause mortality was chosen as the endpoint and was ascertained from death records.
Statistical analysis
The variables were described by the mean and standard deviation for continuous variables with a normal distribution, the median and 25th–75th percentiles for nonnormally distributed continuous variables, and the percentage of the total for categorical variables. The differences between any two equations were tested by the Wilcoxon signed-rank test. The GFR was divided into six different categories (>90, 60–89, 45–59, 30–44, 15–29, and <15 mL/minute/1.73 m2). The differences between the GFR categories were tested by one-way analysis of variance for continuous variables (normal distribution), the Kruskal–Wallis test for continuous variables (abnormal distribution), and x2 analysis for categorical variables. The correlations between any two equations were determined with Spearman’s test. The proportion of patients with a GFR < 60 mL/minute/1.73 m2 was defined as the prevalence and the differences were examined with a Kappa test.
Not only the receiver-operating characteristic (ROC) curve and area under the curve (AUC) values, but also the net reclassification improvement (NRI), as described by Pencina et alCitation18 were used to assess the prognostic value of different equations. The best cut-off value of the GFR for predicting mortality was derived from the ROC curve, and was the cut-off point at which the sum of the sensitivity and specificity was the highest. The NRI was calculated as the sum of the proportion of participants reclassified downward to a lower GFR category for people who died and the proportion of participants reclassified upward to a higher GFR category for people who survived, minus the sum of the proportion of participants reclassified upward for people who died and the proportion of participants reclassified downward for people who survived. The Z statistic was used to compare the c-statistics and to determine the significance of NRI. To judge the independent predictive value of renal function impairment for mortality, covariates with a P < 0.10 were identified by Cox regression univariate analysis and taken into the multivariate Cox regression model with mortality as the dependent variable, which was divided into two steps, including the backward stepwise (likelihood ratio test) with a P < 0.10 and enter with a two-tailed P < 0.05 to avoid collinearity of the variables. The β value is the coefficient of variables in the Cox regression model, and the hazard ratio (HR) is the exp (β). Statistical analysis was conducted using the Statistical Package for the Social Sciences 17 (SPSS, Inc, Chicago, IL, USA) and MedCalc 11.6 for Windows (MedCalc Software bvba, Mariakerke, Belgium).
Results
The median age of the participants was 86 years (60–104 years), and 80.8% (848 patients) of the participants were >80 years of age. The majority (89.2%) of the participants were male, and all the participants were Chinese (100%). lists the clinical characteristics of the participants at different GFR categories computed using four equations. The median values (25th–75th percentiles) for the MDRD-GFR, CMDRD-GFR, CKD-EPI-GFR, and Mayo-GFR were 66.0 (51.6, 78.0), 69.2 (53.3, 82.3), 65.6 (46.9, 80.2), and 75.8 (56.5, 88.5) mL/minute/1.73 m2, respectively. The GFR computed by any two equations showed strong correlations (correlation coefficients: MDRD-GFR and CMDRD-GFR: 0.996; MDRD-GFR and CKD-EPI-GFR: 0.980; MDRD-GFR and Mayo-GFR: 0.959; CMDRD-GFR and CKD-EPI-GFR: 0.987; CMDRD-GFR and Mayo-GFR: 0.955; and CKD-EPI-GFR and Mayo-GFR: 0.963; all P < 0.001). The significant differences in the computed GFR were observed with respect to any two equations (all P < 0.001). As shown in , the GFR determined by each equation decreased as the 10-year age categories increased.
Table 1 Clinical characteristics of participants at different GFR categories computed using four equations
Figure 1 GFR determined by each equation and prevalence of a GFR < 60 mL/minute/1.73 m2. (A) The GFR determined by each equation decreased as the 10-year age categories increased. (B) The prevalence of a GFR < 60 mL/minute/1.73 m2 was proportional to the 10-year age categories.
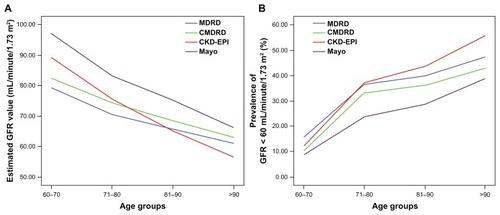
According to the MDRD-GFR, CMDRD-GFR, CKD-EPI-GFR, and Mayo-GFR, the prevalence of GFR < 60 mL/minute/1.73 m2 in elderly patients with CAD was 39.3% (413 patients), 35.4% (372 patients), 43.0% (452 patients), and 28.7% (301 patients), respectively. Compared with the MDRD-GFR, the prevalence of GFR < 60 mL/minute/1.73 m2, according to the CMDRD-GFR (kappa value: 0.917, P < 0.001), CKD-EPI-GFR (kappa value: 0.908, P < 0.001), and Mayo-GFR (kappa value: 0.761, P < 0.001) showed significant differences. The number of patients in the different GFR categories is reported in . The prevalence of GFR < 60 mL/minute/1.73 m2 was proportional to the 10-year age categories ().
Table 2 Numbers of patients and mortality rates at each GFR category
There was a mean follow-up period of 417 days (median: 319 days; 25th–75th percentiles: 185–557 days) for the entire cohort, with 218 deaths (20.8%). The mortality rates for each GFR category are displayed in . The mortality rates of the patients with a GFR < 60 mL/minute/1.73 m2 determined by the MDRD, CMDRD, CKD-EPI, and Mayo equations were 8.6% (118 patients), 30.1% (112 patients), 28.5% (129 patients), and 33.6% (101 patients), respectively. Compared with the MDRD equation, the mortality rates of the patients with a GFR < 60 mL/minute/1.73 m2 determined by other equations had no clear difference (CMDRD equation: P = 0.637; CKD-EPI equation: P = 0.992; Mayo equation: P = 0.154). The AUC values for predicting death with respect to the MDRD-GFR, CMDRD-GFR, CKD-EPI-GFR, and Mayo-GFR were 0.611 [95% confidence interval (CI): 0.563–0.659], 0.610 (95% CI: 0.562–0.658), 0.625 (95% CI: 0.579–0.672), and 0.632 (95% CI: 0.586–0.677), respectively. Despite no significant difference between the MDRD-GFR and CMDRD-GFR (P = 0.651), the AUC values of the CKD-EPI-GFR and Mayo-GFR varied significantly from the MDRD-GFR and CMDRD-GFR (all P < 0.001). Compared with the CKD-EPI-GFR, a larger but statistically insignificant AUC value was observed with the Mayo-GFR (P = 0.244). The cut-off points for the MDRD-GFR, CMDRD-GFR, CKD-EPI-GFR, and Mayo-GFR with the best accuracy for predicting death were at 54.1 mL/minute/1.73 m2 (sensitivity: 0.762; specificity: 0.477), 53.5 mL/minute/1.73 m2 (sensitivity: 0.797; specificity: 0.450), 48.0 mL/minute/1.73 m2 (sensitivity: 0.787; specificity: 0.463), and 57.4 mL/minute/1.73 m2 (sensitivity: 0.791; specificity: 0.454), respectively.
Compared with the MDRD-GFR, the CMDRD-GFR reclassified two (0.2%) to higher, and 96 (9.1%) to lower categories, the CKD-EPI-GFR reclassified 202 (19.2%) to higher, and 25 (2.4%) to lower categories, and the Mayo-GFR reclassified 38 (3.6%) to higher, and 268 (25.5%) to lower categories. Compared with the CKD-EPI-GFR, the Mayo-GFR reclassified 22 (2.1%) to higher and 429 (40.9%) to lower categories. The reclassification of patients in different GFR categories is shown in . The NRI in the risk of mortality was calculated and shown in . Compared with the MDRD-GFR and CMDRD-GFR, the NRI of the CKD-EPI-GFR was calculated at 0.10 and 0.09, and was highly significant (P = 0.004 and P < 0.001). Similar results were observed for the Mayo-GFR (NRI: 0.14, P < 0.001; NRI: 0.12, P < 0.001); however, there was no significant distinction in the NRI between the MDRD-GFR and CMDRD-GFR (NRI: 0.02, P = 0.258) or between the CKD-EPI-GFR and Mayo-GFR (NRI: 0.04, P = 0.221).
Table 3 The reclassification of patients at different GFR categories
Table 4 The net reclassification improvement in risk of mortality
Based on univariate analysis, a GFR < 60 mL/minute/1.73 m2 was associated with mortality regardless of the equation used (MDRD-GFR, HR: 1.98, 95% CI: 1.52–2.59, P < 0.001; CMDRD-GFR, HR: 2.14, 95% CI: 1.64–2.79, P < 0.001; CKD-EPI-GFR, HR: 2.10, 95% CI: 1.60–2.75, P < 0.001; Mayo-GFR, HR: 2.46, 95% CI: 1.88–3.20, P < 0.001). The associations of the MDRD-GFR < 54.1 mL/minute/1.73 m2 (HR: 2.58, 95% CI: 1.98–3.37, P < 0.001), CMDRD-GFR < 53.5 mL/minute/1.73 m2 (HR: 2.76, 95% CI: 2.11–3.60, P < 0.001), CKD-EPI-GFR < 48.0 mL/minute/1.73 m2 (HR: 2.75, 95% CI: 2.11–3.60, P < 0.001), and Mayo-GFR < 57.4 mL/minute/1.73 m2 (HR: 2.73, 95% CI: 2.09–3.56, P < 0.001) with higher mortality were all stronger. After adjusting for age, gender, CHF, acute myocardial infarction, AF, hypertension, diabetes mellitus, body mass index, and mean systolic blood pressure, patients with a GFR < 60 mL/minute/1.73 m2 experienced a significantly higher mortality than patients with a GFR ≥ 60 mL/minute/1.73 m2 (MDRD-GFR, HR: 1.57, 95% CI: 1.19–2.07, P = 0.002; CMDRD-GFR, HR: 1.63, 95% CI: 1.23–2.15, P = 0.001; CKD-EPI-GFR, HR: 1.62, 95% CI: 1.22–2.15, P = 0.001; Mayo-GFR, HR: 1.86, 95% CI: 1.40–2.46, P < 0.001). In addition, the MDRD-GFR < 54.1 mL/minute/1.73 m2 (HR: 1.97, 95% CI: 1.48–2.60, P < 0.001), CMDRD-GFR < 53.5 mL/minute/1.73 m2 (HR: 2.07, 95% CI: 1.54–2.75, P < 0.001), CKD-EPI-GFR < 48.0 mL/minute/1.73 m2 (HR: 2.05, 95% CI: 1.54–2.72, P < 0.001), and Mayo-GFR < 57.4 mL/minute/1.73 m2 (HR: 2.05, 95% CI: 1.54–2.72, P < 0.001) showed more identifiable relationships with mortality.
Discussion
The NHANES study has shown that there is a higher level of GFR and a lower prevalence of renal function impairment in the general population when using the CKD-EPI equation compared with the MDRD equation,Citation19 but in the light of a recent study directed at the elderly, the result appeared to be the opposite for the elderly.Citation20 Similarly, we found in elderly Chinese that the order of the median GFR from high to low was the Mayo-GFR, CMDRD-GFR, MDRD-GFR, and EPI-GFR. The order of GFR < 60 mL/minute/1.73 m2 prevalence from high to low was the CKD-EPI-GFR, MDRD-GFR, CMDRD-GFR, and Mayo-GFR. Previous trials with the general population as the study subjects mainly attributed the higher level of GFR and a lower prevalence of renal function impairment using the CKD-EPI equation to the subgroups at low risk for CKD (age < 60 years, women, and white subjects). For these subgroups, there were lower levels of GFR and a higher prevalence of renal function impairment according to the MDRD equation.Citation21 Our study was aimed directly at the elderly Chinese with CAD, who tended to be older, male, and at high risk for renal function impairment.
Recent studies have shown that people at lower risk for renal function impairment, such as women, younger, and white subjects, were mainly reclassified to lower GFR categories using the CKD-EPI equation and had a lower risk of death, indicating that the CKD-EPI equation improved categorization concerning mortality compared with the MDRD equation.Citation21–Citation24 However, the better reclassification of the CKD-EPI was not validated by another study with a focus on the elderly.Citation25 In the current study, the AUC and NRI values showed that the prognostic abilities of the EPI-GFR and Mayo-GFR were far superior to the MDRD-GFR and CMDRD-GFR. Moreover, even without statistical significance, the Mayo equation still categorized individuals more appropriately than the CKD-EPI equation and might better predict adverse outcomes.
Several studies, such as the Health, Aging, and Body Composition study, showed that a GFR < 60 mL/minute/1.73 m2 compared with a GFR > 60 mL/minute/1.73 m2, was a strong predictor of cardiovascular death.Citation26 However, Go et alCitation27 believed that a GFR < 45 mL/minute/1.73 m2, rather than a GFR < 60 mL/minute/1.73 m2, was the threshold below which all-cause mortality significantly increased. In addition, the Alberta Provincial Project for Outcomes Assessments in Coronary Heart Disease (APPROACH) Registry proposed that a GFR < 79 mL/minute/1.73 m2, but not a GFR > 90 mL/minute/1.73 m2, was the cut-off value for a significant increase in all-cause mortality.Citation28 In fact, all of the studies transformed the GFR to a categorical variable with the levels set in advance, compared the correlation of different categories with mortality, and selected one preset level as the cut-off point, which was limited by the subjective factor. Unlike those studies, the current study used the GFR as a continuous variable and defined the cut-off value with the ROC curve, showing stronger objectivity and accuracy, which demonstrated that even with the presence of better cut-off values, a GFR < 60 mL/minute/1.73 m2 was still a significant predictor of mortality, independent of which equation was used. The National Kidney Foundation acknowledged that identifying subjects with impaired renal function based on the GFR, without reference to age, gender, race, and comorbidity, might lead to an inappropriate prognostic assessment of CKD.Citation29 For elderly Chinese patients with CAD, the current study demonstrated that the optimal cut-off values to predict a significant increase in mortality were set at 54.1 mL/minute/1.73 m2 for the MDRD-GFR, 53.5 mL/minute/1.73 m2 for the CMDRD-GFR, 48.0 mL/minute/1.73 m2 for the CKD-EPI-GFR, and 57.4 mL/minute/1.73 m2 for the Mayo-GFR.
To summarize, the prognostic abilities of the CKD-EPI and Mayo equations were significantly superior to the MDRD and CMDRD equations, and the Mayo equation had a mild, but not statistically significant superiority compared with the CKD-EPI equation in elderly Chinese patients with CAD. Although a GFR < 60 mL/minute/1.73 m2 was still an independent predictor of high mortality independent of which equation was used, the optimal GFR cut-off values indicating a significant increase in mortality were set at 54.1 mL/minute/1.73 m2 for the MDRD-GFR, 53.5 mL/minute/1.73 m2 for the CMDRD-GFR, 48.0 mL/minute/1.73 m2 for the CKD-EPI-GFR, and 57.4 mL/minute/1.73 m2 for the Mayo-GFR.
Acknowledgment
The study was supported by the Central Health Special Foundation (Beijing, People’s Republic of China).
Disclosure
The authors report no conflicts of interest in this work.
References
- LiuHYuJChenFLiJHuDInpatients with coronary heart disease have a high prevalence of chronic kidney disease based on estimated glomerular filtration rate (eGFR) in ChinaHeart Vessels200722422322817653515
- MoeSMChenNXMechanisms of vascular calcification in chronic kidney diseaseJ Am Soc Nephrol200819221321618094365
- AnavekarNSMcMurrayJJVelazquezEJRelation between renal dysfunction and cardiovascular outcomes after myocardial infarctionN Engl J Med2004351131285129515385655
- ManjunathGTighiouartHCoreshJLevel of kidney function as a risk factor for cardiovascular outcomes in the elderlyKidney Int20036331121112912631096
- LeveyASBoschJPLewisJBGreeneTRogersNRothDA more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equationAnn Intern Med1999130646147010075613
- StevensLACoreshJFeldmanHIEvaluation of the modification of diet in renal disease study equation in a large diverse populationJ Am Soc Nephrol200718102749275717855641
- GlassockRJReferrals for chronic kidney disease: real problem or nuisance?JAMA2010303121201120320332411
- LeveyASStevensLASchmidCHfor CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration)A new equation to estimate glomerular filtration rateAnn Intern Med2009150960461219414839
- StevensLASchmidCHZhangYLDevelopment and validation of GFR-estimating equations using diabetes, transplant and weightNephrol Dial Transplant201025244945719793928
- RuleADLarsonTSBergstralhEJSlezakJMJacobsenSJCosioFGUsing serum creatinine to estimate glomerular filtration rate: accuracy in good health and in chronic kidney diseaseAnn Intern Med20041411292993715611490
- MaYCZuoLChenJHModified glomerular filtration rate estimating equation for Chinese patients with chronic kidney diseaseJ Am Soc Nephrol200617102937294416988059
- PoggioEDRuleADA critical evaluation of chronic kidney disease – should isolated reduced estimated glomerular filtration rate be considered a ‘disease’?Nephrol Dial Transplant200924369870019103736
- FoxKGarciaMAArdissinoDTask Force on the Management of Stable Angina Pectoris of the European Society of Cardiology, ESC Committee for Practice Guidelines (CPG)Guidelines on the management of stable angina pectoris: executive summary: The Task Force on the Management of Stable Angina Pectoris of the European Society of CardiologyEur Heart J200627231341138116735367
- ThygesenKAlpertJSWhiteHDfor Joint ESC/ACCF/AHA/WHF Task Force for the Redefinition of Myocardial InfarctionUniversal definition of myocardial infarctionCirculation2007116222634265317951284
- ZhangLZuoLXuGCommunity-based screening for chronic kidney disease among populations older than 40 years in BeijingNephrol Dial Transplant20072241093109917210584
- FusterVRydénLECannomDSfor American College of Cardiology/American Heart Association Task Force on Practice Guidelines, European Society of Cardiology Committee for Practice Guidelines, European Heart Rhythm Association, Heart Rhythm SocietyACC/AHA/ESC 2006 Guidelines for the Management of Patients with Atrial Fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Revise the 2001 Guidelines for the Management of Patients With Atrial Fibrillation): developed in collaboration with the European Heart Rhythm Association and the Heart Rhythm SocietyCirculation20061147e257e35416908781
- DicksteinKCohen-SolalAFilippatosGfor ESC Committee for Practice Guidelines (CPG)ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2008: the Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2008 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association of the ESC (HFA) and endorsed by the European Society of Intensive Care Medicine (ESICM)Eur Heart J200829192388244218799522
- PencinaMJD’AgostinoRBSrD’AgostinoRBJrVasanRSEvaluating the added predictive ability of a new marker: from area under the ROC curve to reclassification and beyondStat Med2008272157172 discussion 207–21217569110
- JonesCAMcQuillanGMKusekJWSerum creatinine levels in the US population: third National Health and Nutrition Examination SurveyAm J Kidney Dis19983269929999856515
- CorsonelloAPedoneCLattanzioFfor PharmacosurVeillance in the elderly Care study groupChronic kidney disease and 1-year survival in elderly patients discharged from acute care hospitals: a comparison of three glomerular filtration rate equationsNephrol Dial Transplant201126136036420921298
- StevensLASchmidCHGreeneTComparative performance of the CKD Epidemiology Collaboration (CKD-EPI) and the Modification of Diet in Renal Disease (MDRD) Study equations for estimating GFR levels Above 60 mL/min/1.73 m2Am J Kidney Dis201056348649520557989
- MatsushitaKSelvinEBashLDAstorBCCoreshJRisk implications of the new CKD Epidemiology Collaboration (CKD-EPI) equation compared with the MDRD Study equation for estimated GFR: the Atherosclerosis Risk in Communities (ARIC) StudyAm J Kidney Dis201055464865920189275
- WhiteSLPolkinghorneKRAtkinsRCChadbanSJComparison of the prevalence and mortality risk of CKD in Australia using the CKD Epidemiology Collaboration (CKD-EPI) and Modification of Diet in Renal Disease (MDRD) Study GFR estimating equations: the AusDiab (Australian Diabetes, Obesity and Lifestyle) StudyAm J Kidney Dis201055466067020138414
- StevensLALiSKurella TamuraMComparison of the CKD Epidemiology Collaboration (CKD-EPI) and Modification of Diet in Renal Disease (MDRD) study equations: risk factors for and complications of CKD and mortality in the Kidney Early Evaluation Program (KEEP)Am J Kidney Dis2011573 Suppl 2S9S1621338849
- StengelBMetzgerMFroissartMEpidemiology and prognostic significance of chronic kidney disease in the elderly – the Three-City prospective cohort studyNephrol Dial Transplant201126103286329521677301
- DeoRFyrCLFriedLFfor Health ABC studyKidney dysfunction and fatal cardiovascular disease – an association independent of atherosclerotic events: results from the Health, Aging, and Body Composition (Health ABC) studyAm Heart J20081551626818082491
- GoASChertowGMFanDMcCullochCEHsuCYChronic kidney disease and the risks of death, cardiovascular events, and hospitalizationN Engl J Med2004351131296130515385656
- HemmelgarnBRSouthernDAHumphriesKHCulletonBFKnudtsonMLGhaliWAfor Alberta Provincial Project for Outcomes Assessment in Coronary Heart Disease (APPROACH) InvestigatorsRefined characterization of the association between kidney function and mortality in patients undergoing cardiac catheterizationEur Heart J200627101191119716574688
- VassalottiJAStevensLALeveyASTesting for chronic kidney disease: a position statement from the National Kidney FoundationAm J Kidney Dis200750216918017660017