Abstract
Background
Innovative Vision Products, Inc. (IVP)’s scientists developed the lubricant eye drops (Can-C™) designed as 1% N-acetylcarnosine (NAC) prodrug of l-carnosine containing a mucoadhesive cellulose-based compound combined with corneal absorption promoters in a sustained drug delivery system. Only the natural l-isomeric form of NAC raw material was specifically synthesized at the cGMP facility and employed for the manufacturing of Can-C™ eye drops.
Objective and study design
In the present clinical study the authors assessed vision before and after 9 month term of topical ocular administration of NAC lubricant eye drops or placebo in 75 symptomatic patients with age-related uncomplicated cataracts in one or both eyes, with acuity in one eye of 20/40 or worse (best-corrected distance), and no previous cataract surgery in either eye and no other ocular abnormality and 72 noncataract subjects ranged in age from 54 to 78 years.
Setting
Subjects in these subsample groups have reported complaints of glare and wanted to administer eye drops to get quick eye relief and quality of vision for their daily activities including driving and computer works. Following 9 months of treatment with NAC lubricant eye drops, most patients’ glare scores were improved or returned to normal in disability glare tests with Halometer DG. Improvement in disability glare was accompanied with independent improvement in acuity. Furthermore, patients with the poorest pretreatment vision were as likely to regain certain better visual function after 9 months of treatment with N-acetylcarnosine lubricant eye drops as those with the worth pretreatment vision.
Patients or other participants
The authors made a reference to electronic records of the product sales to patients who have been made the repurchase of the Can-C™ eye drops since December 2001.
Intervention
Based on this analysis of recorded adjustments to inventory, various parameters were analyzed during the continued repurchase behavior program, including testimonials from buyers. With these figures, researchers judged on the patients’ compliance rate to self-administer NAC eye-drops.
Main outcome measure and results
The ophthalmic drug showed potential for the non-surgical treatment of age-related cataracts for participants after controlling for age, gender and daily activities and on a combined basis of repurchases behavior reports in more than 50,000 various cohort survivors, has been demonstrated to have a high efficacy and good tolerability for prevention and treatment of visual impairment determined for the older population with relative stable pattern of causes for blindness and visual impairment. The mechanisms of prevention and reversal of cataracts with NAC ophthalmic drug are considered which include prevention by the intraocular released carnosine of free-radical-induced inactivation of proprietary lens antioxidant enzymes (superoxide dismutase); prevention of carbohydrate and metal-catalyzed autooxidation of ascorbic acid-induced cross-linking glycation reactions to the lens proteins; transglycation properties of carnosine, allowing it to compete for the glycating agent, protecting proteins (lens crystallins) against modification; universal antioxidant and scavenging activity towards lipid hydroperoxides, aldehydes and oxygen radicals; activation with l-carnosine ingredient of proteasome activity in the lens; chaperone-like disaggregating to lens crystallins activity of NAC and of its bioactivated principal carnosine. Blindness incidence increased with advancing age, such as cataract and glaucoma, which are by far the commonest causes of blindness in our sample and in all age groups, glaucomatous neurodegeneration can be treated with developed NAC autoinduction prodrug eye drops equipped with corneal absorption promoters. The common blinding affections presenting in developed countries such as, senile macular degeneration, hereditary chorioretinal dystrophies, diabetic retinopathy are poorly represented in our current summary of vital-statistics and will be reported inherent in next N-acetylcarnosine ophthalmic drug studies.
Conclusion
The authors present evidence, about why only a certain kind of NAC is safe, and why only certain formulas designed by IVP for drug discovery are efficacious in the prevention and treatment of senile cataract for long-term use. Overall cumulated studies demonstrate that the designed by IVP new vision-saving drug NAC eye drops help the aging eye to recover by improving its clarity, glare sensitivity, color perception and overall vision.
Nature, like a Sphinx, And the temptation of humans with Her mysteries is stronger Considering that maybe there are no mysteries at all.
Introduction
Carnosine (β-alanyl-l-histidine) was discovered and its structure determined in the very beginning of the 20th century.Citation1 It was the first and the simplest example of biologically active peptides (actually a dipeptide), opening the long list of widespread natural protein and peptide regulators of metabolism. The biological role of carnosine is illustrated by a clear correlation between its concentration and the functional activity of muscles, by the period of its accumulation related to a specific step of ontogeny, and by the presence of special enzymes providing synthesis and metabolic transformation of carnosine. Recently we have originally discovered that some natural compounds of a peptide character or their metal chelates may be among the most potent lipoperoxidase mimetics that have ever been characterized.Citation2 l-carnosine and its ophthalmic prodrug bioactivating N-acetylcarnosine (NAC) are part of this group of products.Citation3 NAC, like its parent compound, carnosine, occurs naturally throughout the human body. Both compounds are found primarily in the heart and skeletal muscles and in the brain. However, we have found appreciable levels of l-carnosine in transparent human lenses which are markedly depleted in mature cataracts.Citation4 The concentration of carnosine in transparent crystalline lenses detected was about 25 μM. At different stages of cataract development, the level of carnosine fell, reaching about 5 μM.1 Research with NAC demonstrates that it is effective not only in preventing cataracts but also in treating them. NAC has been shown to improve vision by partially reversing the development of the cataract, thus increasing the transmissivity of the lens to light.Citation5
One of the obscure aspects of the carnosine problem is the biological significance of the enzymatic metabolism of carnosine or its derivatives in tissues. Thus, in order to change an antioxidant status, tissue enzymes can modify the NAC molecule and deacetylation will increase in vivo the resistance of lens tissues and its cells to oxidative stress. This modification of NAC may serve as a regulator of reactive oxygen species level in the ocular biological tissues and fluids. The topical administration of NAC as a universal bioactivating antioxidant for vision in the developed and patented lubricant eye drop formulations delivers pure l-carnosine and allows its increased intraocular absorption into the aqueous humor surrounding the lens, thus enabling significant improvements in anticataract drug efficacy and the minimization of side-effect from either local or systemic drug absorption/bioavailability to the eye, and also creates optimization effects in the number of ocular degenerative age-dependent disorders.Citation5
The research and development team at Innovative Vision Products, Inc. (IVP; County of New Castle, DE USA) studied the effects of lubricant eye drops designed as 1% NAC prodrug of l-carnosine containing a mucoadhesive cellulose-based compound combined with corneal absorption promoters in a drug delivery system. The predicted responses of the corneal and conjunctival penetrations to the synergistic promoters are useful in controlling the extent and pathway of the ocular and systemic absorptions of instilled NAC prodrug in designed ophthalmic formulations thereof.Citation5 The developed by IVP NAC prodrug and codrug lubricating eye drop systems (including principal regulatory registered eye drops design Clarastill™ and Can-C™ lubricating eye drops) have been marketed under numerous brand labels. Several expert antiaging companies are supplying the eye health comfort NAC drops on the market today with more than 5 years of experience and consequently, there exists empirically successful reasoning that NAC lubricant eye drops are reputed to cure cataracts and other eye diseases.
The risk, cost and social requirement factors drive the investigation of pharmaceutical approaches to the management of cataracts. More than 17 million people are blind because of cataract and 28,000 new cases are reported daily worldwide.Citation6 In the United States, over 1.3 million cataract operations are performed annually at a cost of $3.5 billion.Citation7 Forty-three percent of all visits to ophthalmologists by Medicare patients are associated with cataract.Citation7 Approximately 25% of the population over 65 and about 50% over 80 have serious loss of vision because of cataract. Since the population over 55 is most susceptible to lens opacification and is expected to increase 4-fold worldwide and significantly in the United States,Citation8 cataract is a major disease both in terms of numbers of people involved and in economic impact.
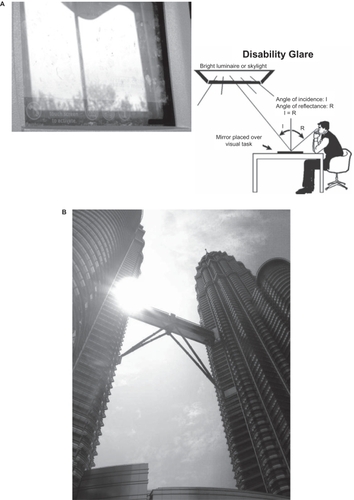
The importance of quality of vision (QOV) along with quality of life (QOL) in antiaging medicine has been recently widely recognized. We have conducted studies to quantitatively analyze factors related to QOV using the Halometer DG (Disability Glare) tester, a clinically developed ophthalmic diagnostic instrument.Citation9 Glare is broadly defined as representing those effects of light that impair visual efficiency. The physical mechanisms and physiological causes of glare in human vision are reported.Citation9 These mechanisms are scattering in the cornea, lens, and retina, and diffraction in the coherent cell structures on the outer radial areas of the lens. This scattering and diffraction are responsible for the “bloom” and “flare lines” seen around very bright objects. The diffraction effects cause the “lenticular halo”. The quantitative assessment of these glare effects was reported by our group, and an algorithm for using these clinical characteristics of vision to add glare effects to digital lens images in age-related human cataracts was presented.Citation9–Citation12 Disability glare (DG) results when a light source reflects from or otherwise covers the visual task, like a veil, obscuring the visual target, reducing its contrast and making the viewer less able to see and discriminate what is being viewed. The problem is illustrated in .
Figure 1 Disability glare results when a light source reflects from or otherwise covers the visual task, like a veil, obscuring the visual target, reducing its contrast and making the viewer less able to see and discriminate what is being viewed. A. This drawing illustrates the problem. In this example, bright light from a ceiling/window light fixture or skylight is reflected from the visual task surface, and into the observer’s eyes, veiling his recognition of the target visual content. Nearly as much light is reflected from the white paper as from the black ink making the letters, so that the contrast is low and the text is washed out and difficult to read. Such glare “disables” the process of reading. B. The example of outdoor glare.
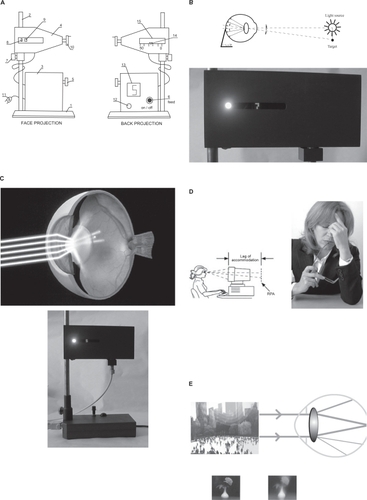
In this paper, the CIE term, DG is used to represent retinal exposure from a glare source that results in diffused intraocular light scattering within the ocular media. This diffused light induces an unwanted optical veil of luminance that reduces contrast and target visibility. Currently, there are no good instruments for measuring DG, and there is no good “metric” for quantifying DG. Despite the fact that several tests designed to “penetrate” lens opacification in order to assess visual function at the retinal-neural level are in use clinically, each has rather severe limitations, particularly in cases where the need for clear definition of functional integrity is greatest. For patients with cataract, visual function in everyday conditions is poorly predicted by classical Snellen acuity, grating acuity, and grating contrast sensitivity when test measurements are made under “minimal-glare” conditions.Citation13 This statement was supported by the Committee on Ophthalmic Procedures Assessment of the American Academy of Ophthalmology on contrast sensitivity and glare testing in the evaluation of anterior segment disease.Citation14 It’s believed that DG assessment should become an integral part of eye exams for people over 50 years of age. We have recently designed an innovative Halometer DG tester () that overcomes previous deficiencies.Citation9–Citation12 IVP patented the original Halometer DG concept and designed the vision diagnostic device for commercial implementation.Citation9–Citation12 The Halometer DG tester is vital for aging drivers with poor vision resulting from aging, cataract, and ocular disease(s). Glare testing provides secondary information concerning cognitive and physical performance. The Halometer DG is sensitive even to mild impairments. Such information is often ignored or denied until it is advanced with marked functional impairment resulting in a serious accident. Relationships between computer task performance (accuracy and speed) and visual function parameters (visual acuity, glare sensitivity, visual field, and color vision) are also important.Citation14 Among this cohort of patients with age-related cataracts and ocular degenerative disorders, visual acuity, disability glare sensitivity, and color vision defects are significant predictors of computer task performance. Visual function parameters of the better eye usually plays a more significant role than parameters of the worse eye, and disability glare is the significant predictor of computer task accuracy.Citation14 The symptoms include headaches, blurred distance vision, halos, double vision, and generally irritated and fatigued eyes ().
Figure 2 A Halometer DG (face and rear) projection 1, device base; 2, support bar; 3, feed source; 4, block unit for glare testing as seen by subject; 5, rheostat to regulate source brightness; 6, button to turn on/off the voltage feed; 7, clamp; 8, glare source window; 9, moveable optotypes (target); 10, mechanical mechanism for moving the optotypes to/from the glare source; 11, voltage feed plug; 12, a button for choosing among different optotypes, operator side; 13, electronic display of shifted optotype position, operator side; 14, metric scale of optotype distance from glare source, operator side; 15, metric distance scale of the optotype distance from glare source, operator side. B. Principle of the disability glare test, based on the measurement of the glare radius (r, mm) a new metric for glare sensitivity. I0 = Indicatrix of light scatter; ϕ = angle. The technique utilizes a self-illuminating red or green optotype target and tangential 2 mm ‘point light source’ seen from a distance of 30 cm. The patient’s task is to move the optotype closer to the glare source until it disappears due to the veiling glare from the glare source. A halometer score is determined as follows. The illuminous (in red or green) target is approached from the source so that the patient becomes unable to distinguish the target from the source and then, the target is slowly taken away until the exact moment when the patient distinguishes the target; at this time, the incident light angle ϕ between the source and the target is measured. The target is always fixated with the foveal vision. The target and the ‘point light source’ are viewed in the same vertical plane, tangential to the plane of emitted light. In this case, to measure the angle ϕ of the incident light between the source and the target, it is necessary only to measure its projection on this vertical plane, which means to measure the distance between the source and the target. The measured glare radius is defined as a target image projection for the vector of light scatter (indicator of light scatter I = I0cos 2 ϕ) when the glare source is activated and the patient is asked to recognize the target during illumination of the eye with a glare source. C. Photograph of working prototype of the Halometer DG tester. Halometer DG instrument can provide the valuable data on the intraocular light scatter in cataracts. The instrument can be used in the pre-testing examination room of optometrist and ophthalmologists offices, at Department of Motor Vehicle licensure facilities or incorporated within automobiles, for self testing. D. Vision problems during computer use. The eyes find it difficult to focus on the pixel characters. They can focus on the plane of the computer screen, but cannot sustain that focus. The eyes focus on the screen and relax to a point behind the screen, which is called the resting point of accommodation (RPA) or dark focus. The RPA is different for every individual, but for almost everyone, it is further away than the working distance to the computer. The working distance is the distance from the computer user’s eyes to the front of the screen. Therefore the eyes are constantly relaxing to the RPA, and then straining to refocus on the screen. This constant flexing of the focusing (ciliary body) muscles is what creates fatigue, and generates burning and tired eyes. In clinical studies, it has been found that there is a significant difference in the glasses prescription required for focusing on a standard printed near card (called a Snellen card) and focusing on the image of a typical computer screen, both at a viewing distance of 20 inches. Many patients needed a different correction in each eye. E. As light passes through the cataractous lens, it is diffused or scattered. The result is blurred or defocused vision.

In the present clinical study we assessed vision before and after the 9-month term of topical ocular administration of NAC lubricant eye drops or placebo in 75 symptomatic patients with age-related uncomplicated cataracts in one or both eyes, with acuity in one eye of 20/40 or worse (best-corrected distance), and no previous cataract surgery in either eye and no other ocular abnormality and 72 noncataract subjects ranged in age from 54 to 78 years. Subjects in these subsample groups have reported complaints of glare and wanted to administer eye drops to get quick eye relief and quality of vision. Glare sensitivity was measured with the Halometer DG tester. Prior to treatment with NAC lubricant eye drops there was significant disability glare that was not correlated with acuity. The disability glare was especially manifested under nighttime conditions and expressed during a prolong work with a computer-controlled video display.
Following 9 months of treatment with NAC lubricant eye drops (Can-C™) (, ), most patients’ glare scores were improved or returned to normal in disability glare tests with Halometer DG. Improvement in disability glare was accompanied with independent improvement in acuity (). Furthermore, patients with the poorest pretreatment vision were as likely to regain certain better visual function after 9 months of treatment with NAC lubricant eye drops as those with the better pretreatment vision.
Table 1 Specification of cGMP manufactured N-acetyl-l-carnosine used in IVP drug Can-C™ development and clinical studies
Table 2 Computer user questionnaire Do you notice any of these visual symptoms? Please rate the following symptoms by underlining the appropriate description
Table 3 Demographic and ergonomic occupational characteristics of cataract and no cataract adult subjects enrolled in the study
Table 4 Distribution of visual acuity and disability glare in the cataract and noncataract groups of the adult subjects enrolled in the study at baseline examination
Table 5 Linear correlation coefficients (R) between the characteristics of older subjects with cataract and noncataract older adult subjects measured by visual acuities (VA) and glare radius (GR at red and green targets) at baseline and at 9-month follow-up ophthalmic examinations
Figure 3 Can-C™ N-acetylcarnosine lubricant eye drops developed, manufactured at the cGMP manufacturing facility and worldwide patented by Innovative Vision Products, Inc, Formulation.Citation21–Citation23 The composition is in the form of isotonic solution. Because the composition is applied to the eye, the composition is sterile. The isotonicity of ophthalmic preparation was measured and adjusted as calculated correctly by addition of small concentrations of sodium chloride. The specification of the unique nonracemized natural (l)-isomer form of N-acetylcarnosine (see 3D structural formula) recipient included in the Can-C™ is presented in .
NAC prodrug and codrug ophthalmic formulations are applied topically to the eye and moreover, its controlled time-released ophthalmic ingredient, l-carnosine, exerts antiglycation, bioactivating antioxidant properties in the lens and cornea as a scavenger of lipid peroxides, singlet oxygen, and OH·radicals and spatial aspects of intracellular pH regulation.Citation5,Citation15 In contrast to the possible pirated brands of NAC eye drops available on the market that employ D/L-isomeric forms of NAC, in the IVP conducted clinical studies only the natural l- isomeric form of NAC raw material was specifically synthesized at the cGMP facility and employed for the manufacturing of the Can-C™ eye drops.
In the initial stages and the planning of the present study, the enrolled patients suffered from different degrees of glare problems. The purpose of this study is to examine the effects of a most often recommended short-term 9-month treatment with 1% NAC in ophthalmic formulation with a lubricant, carboxymethylcellulose, on improvement of visual impairment and glare disability in older adult subjects and older patients with cataract whose occupations frequently involve driving or computer activities.
Strengths of this study design are the use of a comparison group of patients with cataract and older subjects (including drivers or computer users) who were treated with placebo (Control group) followed prospectively over the same time period and the statistical adjustment for potential differences in the treated with NAC groups that could serve as the indication for the hypothesized improvement effect on vision for better occupation returns. We used a randomized design that was ethical since NAC is an accepted and proven therapeutic modality of vision care available on the market of antiaging medicine since 2002.Citation10,Citation15–Citation18
What we have found is there is currently a significant rise in the purchase orders that request a vendor/supplier to furnish the Can-C™ eye drops. We have first made a reference to electronic records of the product sales to patients who have been made the repurchase of the Can-C™ eye drops since December 2001. Based on this analysis, we record adjustments to inventory, making record sale during the continued repurchase program and analyze simultaneously the various parameters, including testimonials. With these figures, researchers judged on the patients’ compliance rate to self-administer eye-drops.
Materials and methods
The first enrolled cohort of examined subjects consisted of 75 older adults with age-related uncomplicated cataracts in one or both eyes, and 72 adult subjects who did not have cataract in either eye. Patients in these subsamples suffered from different degrees of glare problems. Those with cataract ranged in age from 53 years to 83 years (mean ± SD, 69 ± 8 years), with 48% female, 100% white and of non-Hispanic origin. The noncataract subjects ranged in age from 54 to 78 years (mean ± SD, 66 ± 8 years); 53% were female, with 100% being white. Subjects who were cataract free had to meet the same inclusion criteria as the subjects with cataract described previously.Citation9,Citation10,Citation16–Citation18 All subjects with cataract were required to meet the following inclusion criteria: (1) cataract in one or both eyes with best-corrected visual acuity of 20/40 or worse in one or both eyes as indicated by the medical record; (2) no previous cataract surgery in either eye; (3) a primary diagnosis of cataract in the medical record; (4) living independently in the community; specific items were needed to be addressed if appropriate; (5) driving skills: legally licensed to drive and drove during the 5 years prior to enrollment; (6) related general or eye health problems experienced during computer use: this was assessed by asking subjects if they have any symptom problems in the specific areas listed in , . Among participants, bilateral cataracts were present in 95% of subjects according to the medical record from the most recent eye examination (within 1 month of enrolment). In the right eye, 46% had nuclear sclerotic cataract, 8% had cortical cataract, 9% had posterior subcapsular cataract, and 38% had a combination of at least two types. The breakdown was similar in the left eye, with 49% nuclear sclerotic, 10% cortical, 7% posterior subcapsular, and 35% combination. Seventy-four percent of subjects with cataract had no additional ocular conditions other than refractive error; 6% had early nonexudative age-related maculopathy, 9% had primary open-angle glaucoma (POAG) associated with cataract, 3% had diabetic retinopathy, 1% had a combination of two of these problems, and 7% had another ocular condition. Subjects who were cataract-free had to meet the same inclusion criteria as the subjects with cataract, except that they were required to be free of cataract and to have a best-corrected visual acuity of 20/25 in each eye, according to medical record review. No cataract-free subjects had secondary eye conditions other than refractive error.
Patients with known or presumed hypersensitivity to any component of the ophthalmic preparations (active substances or excipients), and those treated with drugs that could interfere with this trial, were also excluded from the study. The subjects were recruited and examined by IVP ophthalmology practices. The study protocol was approved by the corporative review board for human use. After the purpose of the study had been explained, each subject was asked to sign a document of informed consent before enrolling. Demographic data, driving status during the prior 5 years and computer use at work were confirmed by interview ().
Procedures
After enrolment, subjects were computer-randomized into two groups assigned according to the double blind method: to receive treatment with NAC 1% eye drops (Can-C™), or to a control group who received placebo eye drops. The blinded testing was carried out by an independent medical worker who handed out the NAC versus placebo eye drops (control group) to the randomized subject members of the clinical groups. The enrolled subjects underwent follow-up examinations at baseline and after 9 months of enrolment. Test examiners were masked to the driving histories of all subjects. Two types of visual functions were assessed: visual acuity and glare sensitivity (DG). All acuity measurements were made while subjects wore the lens correction they typically used during the performance of everyday distance activities, including driving. Each eye was assessed separately. Distance acuity was measured as described before using the letter chart and its standard protocol, and was expressed as log minimum angle resolvable.Citation9,Citation10,Citation16–Citation20 For each eye, visual acuity measurements were grouped into four categories: 20/25 or better, 20/25–20/30, 20/35–20/50, and worse than 20/50. These cut-off points were chosen because they were the approximate quartiles of the acuity distribution and included the practically significant cut-off point for driving licensure in many countries (20/40 to 20/50). Some of the vision problems from this course will include computer-related work and the circumstances under which that work is performed.
Slit-lamp biomicroscopic examination or exampled photographic registration was performed after pupil dilation to a minimum of 6 mm with tropicamide.
DG was defined with an optical instrument and method for measuring susceptibility to glare of a human vision system as describedCitation9–Citation12,Citation16–Citation18 and schematically presented in –C. A constant “point”-like bright glare source is used to create the glare condition (). The examining room was dark (less than 20 foot-candles) as typical when working with the glare testers to assure maximum contrast of the projected target. Tests were performed with the best correction in place. The indicator of optotypes on the front or back panels of the instrument indicated the tested optotype to the patient or clinician, respectively. The diagnostic block of a device contained source light window (glare source) and the moving indicator of the optotypes illuminated with red or green light (). The back panel of the Halometer device facing the clinician was equipped with a chart/scale and with a moving indicator of the optotype transition. According to a special embodiment of the invention,Citation9–Citation12,Citation16–Citation18 for the clinical testing of glare sensitivity of a patient we used an illuminated target with red or green color, which enables the assessment of the effect of wavelength on the scattered light.
Treatments with NAC 1% lubricant eye drops
NAC eye drops (Can-C™) contained a 1% solution of NACCitation21–Citation23 with a lubricant, 0.3% carboxymethylcellulose, in the isotonic ophthalmic formulation in borate buffer with preservative benzyl alcohol (corneal absorption promoter) and showed the increased intraocular absorption of the active principle (l-carnosine) in the aqueous humor compared to topical administration of a pure 1% NAC solution:
The ophthalmic formulation thus creates a facility to examine the efficacy of treatment for improvements of vision during the short-term periods of administration of NAC 1% eye drops (9 months in the present study).The administration schedule was two drops instilled twice daily, for patients assigned to NAC and those assigned to placebo (the same formulation without NAC, 1%) alone for 9 months. The use of other topical or nutritional antioxidants was not measured or evaluated between the two groups. The control groups and the treated group did not take any prescribed antioxidant vitamins that might have added to the antioxidant level. Neither the investigators nor the patients knew who was receiving NAC.
Statistical analyses
Statistical analysis was performed by Student’s t test; p = 0.05 was taken as the upper limit of significance. To assess associations, correlation and linear regression analyses were used.
Repurchase earnings analysis
The major factors that led to the sharp increase in net earnings for the quarters of 2007 compared to the corresponding quarters of 2003 were a significant increase in selling, general and administrative expenses for the promotion of Can-C™ NAC lubricant eye drops to public. The launch of Can-C™ ophthalmic formulation and continuing strong sales as the anticataract and antiglare product contributed most of the sales growth in the USA and Europe. The Computer-Based Facilities Inventory and Utilization Management Information Subsystem allowed authors to analyze the trades that occurred and ongoing from the fourth quarter of 2002 till the third quarter of 2007 and now they have in place a publicly-announced repurchase program that, after calculation of the number of sold eye drops, generally supports the enhanced patient’s compliance and improved safety of the drug candidate in subjects who may self-administer the prescribed by IVP medication (NAC lubricant eye drops) for the reduction or treatment of cataracts, and every challenge opportunity is taken to promote self-care.
Patient compliance in both groups described in this study to self-administer NAC lubricant eye drops (Can-C™) was considered excellent.
Results
Sample characteristics
lists the demographic and ergonomic occupational characteristics of the cataract (n = 75) and noncataract groups (n = 72). Those with cataract were similarly older on average with the noncataract group of subjects. Both groups were split evenly between males and females, and had similar racial composition in a totally white population.
lists the visual function for both groups enrolled in the study and the distribution of visual acuity and disability glare scores for subjects with cataract and those without. As would be expected by the case definition for cataract group membership, those in the cataract group had impairments in visual function as compared to the no-cataract group. This was true for both the “worse” and better” eyes. In addition, visual acuity in the range of 20/35 to 20/50 and disability glare readings in the range of glare radius more than 12 mm was associated with driving difficulties (such as crash involvement) and computer-related injuries (). Although not statistically significant, there was also a possible relationship between visual acuity worse than 20/50 and crashing during driving experience.Citation24 DG (glare radius measured in millimeters) was correlated for statistical significance with visual acuity at red and green targets at baseline and 9-month examination interval in the total samples of older subjects with cataract and noncataract older adult subjects ().
Older subjects enrolled in the study were divided into two groups: treated with NAC and control group ( and ). lists the analogous and adjusted analyses for the worse eye, which generated results in the eyes with cataract upon treatment with NAC prodrug ophthalmic formulation are qualitatively similar to those for the better eye. None of the baseline differences between the different groups was significant. The two groups were similar in smoking history, sunlight exposure, and alcohol use. There was no substantial difference in the use of sunglasses, where the patients lived, or occupational hazard exposure between the two groups.
Table 6 Visual function in the better and worse eyes after 9 months of treatment with N-acetylcarnosine 1% eye drops (Can-C™) versus baseline examination
Table 7 Visual function in the better and worse eyes after 9 months of treatment with placebo (Control group) versus baseline examination
Ophthalmic examinations indicated that the methodological variances of measurements were approximately equal. Correlations of glare sensitivity at red versus green targets were significant (). Intraoperator correlation coefficients obtained as repeated measurements for each combination of operator, eye (right or left), and glare radius (at red and green targets) were statistically significant and presented earlier.Citation9,Citation10,Citation16–Citation18 Overall, the reproducibility for the one operator was good. – summarize the effects of study treatment on visual acuity and glare sensitivity over 9 months in older subjects with cataract and no cataract. In the control placebo-treated group, comparison with baseline values showed some variability of data in gradual worsening of glare sensitivity at red and green targets and minimal visual acuity changes over 9 months (). Glare sensitivity indicated mostly changes in lens clarity and confirmed the tiny changes in the optical media of the eye at the short-term follow up examinations when slit lamp associated image analysis data and densitometric readings did not differ significantly with baseline.Citation9,Citation10,Citation16–Citation18
Table 8 Mean ± SD of changes (improvement) in visual functions
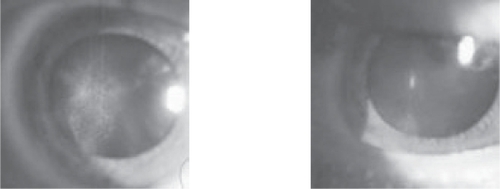
In the NAC-treated group, 9-month follow-up generally showed an improvement in visual acuity (according to the distribution score of distance acuities in worse and better eyes) and a significant improvement in glare sensitivity at red and green targets was documented in worse and better eyes using a critical cut point halometer score (, ). Visual acuity was mostly improved in older subjects with cataract in a worse and better eyes and an improvement in glare sensitivity was found both in older subjects with cataract and noncataract older adult subjects in worth and better eyes after 9 months of treatment with NAC. The exampled images of cataract reversal in older subjects are presented on the slit lamp images just for note (see ).
Figure 4 The pictures show the treatment of human cataract in the older subject with the eye drops of 1% Can-C™ for the period of 5 months. The left image shows the appearance of cataract which resembles a bat in its form and the right image shows that this opacity has disappeared after the cited period after treatment with n-acetylcarnosine is completed. The lens has become clearer.
The NAC-treated eyes had statistically significant difference in VA, glare sensitivity compared with the control group (p < 0.001) at 9-month time point of treatment, as supported by the overall t-test results of the ratio of the follow-up data to the baseline values (). The previously published data illustrate examinations over 24 months of the eyes that were treated with NAC to show that the effect of treatment is sustainable over more prolonged periods.Citation10,Citation16–Citation18 In the eyes of older subjects with different localization and grade of cataract and in noncataract older adult subjects, short-term and prolonged treatment with NAC did not seem to result in a worsening of the visual outcome in this study and elsewhere.Citation10,Citation16–Citation18 Topical short- or long-term administration of 1% NAC to the eye was very well tolerated, with no ocular or systemic adverse effects, no hyperemia of conjunctival vessels, and no signs of allergy or other toxic manifestations being reported. No clinically significant changes from baseline, and no statistically significant differences between the treatment and control groups, were observed regarding ocular comfort and ocular signs and symptoms (lack of burning and stinging, blurred vision, ocular dryness, superficial punctate keratitis, foreign body sensation, itching, ocular discharge, ocular pain, tearing, ocular inflammation, photophobia). All patients completed the study without any problems related to their allocated treatment.
The board of directors analyzed the repurchase behavior of Can-C™ in open market programs. The product has been on the market since November, 2001 and it is well known according to the records how many boxes of Can-C™ are actually repurchased. The analyses in this paper demonstrate the repurchase behavior of patients in more than 50,000 individual buyback programs. We find that repurchase announcements during 5 recent years of follow-up give the credible figure of 50,000 patients who are compliant users of Can-C™ eye drops for published therapeutic indications (including treatment of cataracts) and demonstrate the safety of all-in-one eye drops on a daily basis. On average, these patients repurchase more boxes of the drug than they originally authorized over the last four quarters following the announcement of greater sales, though there is considerable variation across patients’ requests. We examine the factors influencing repurchase behavior, and find that repurchases in the latest quarters are associated with a number of variables, including the efficacy of the product and its persistent safety to control the signs of glare sensitivity, cataract amelioration, and quality of vision during daily life activities. We also consider the past and current returns, profitability, and prior repurchase activity.
According to the records of repurchase behavior, the unique and patented NAC lubricant all-in-one eye drops formula Can-C™ can also provide beneficial results with the following eye-disorders:
Presbyopia.Citation15,Citation23
Open-angle primary glaucoma (in combination with beta-blockers).
Corneal disorders.
Computer vision syndrome.
Eyestrain.
Ocular inflammation.
Blurred vision.
Dry eye syndrome.
Retinal diseases.
Vitreous opacities and lesions.
Complications of diabetes mellitus and other systemic diseases.
Contact lens difficulties, particularly with soft contact lenses. (Not only do the lubricants in the Can-C™ NAC eye-drop help to make contact lenses more comfortable, but NAC is also believed to reduce the build up of lactic acid in the eye, thus enabling the lens to be left safely in the eye for longer).
We also investigate how sales outstanding change following repurchase program announcements. Over the test last year period the average increase in sales is about 80% and only about 35% of the number is repurchased. For the most part, changes in sales of Can-C™ are influenced by the same factors affecting repurchases and in the predicted direction of warranted efficacy and safety of the product. is presenting the exampled but most typical and standard testimonials received from patients who have purchased originally Can-C™. The NAC lubricant eye drops have been successfully used for medically oriented home health care usually helping seniors recover or exercise with aid in recovery from visual impairment or illness including cataracts (). Medically oriented home-health care represents less than half of formal home-health services rendered to the long-term-care population. It is important to note that most work for home health agencies, hospitals, or public health departments are licensed by the state.
Table 9 Can-C™ testimonials
Figure 5 Home health care service. The doctors are often committed to improving a vision healthcare and quality of life of a patient by providing access to the N-acetylcarnosine lubricant eye drops (Can-C™). To ensure the perfect plan of care, the distributor of eye drops will communicate frequently with the primary physician and with family members if a patient so desires. For insurance coverage, a doctor will write an order for home health nursing.
Discussion
It is foreseen that the health problems of the elderly are multiplying exponentially with the demographic changes in our aging population. Visual impairment represents one of the most significant of these problems, not only in terms of eye diseases, but because of the associated dangers affecting the rest of the body.Citation25
The four most prevalent age-related ocular diseases are macular degeneration, open-angle glaucoma, cataract, and diabetic retinopathy.Citation26,Citation27 Normal visual changes that occur with aging include presbyopia, decreased contrast sensitivity, decreased dark/light adaptation, and delayed glare recovery.Citation28 This decline in vision is associated in part with an increase in vehicular accidents per mile driven by the elderly.Citation29 The visually demanding computer task had a more pronounced effect on the elderly than on the young. In this study, we examined the visual function and glare disability of older subjects without cataract and in the presence of cataract as a patients’ perception of their daily living ability to perform vision dependent tasks. The traditional clinical measurement of vision, Snellen letter visual acuity, can provide an inadequate measure of forward light scatter relevant to glare effects in adult subjects.Citation30,Citation31 To determine whether glare sensitivity (halos) was significantly responsible for the change in visual functions in older subjects with cataract, we proposed a new halometer process, which is a form of disability glare test. In a previous study,Citation9 we indicated that a set of halometric examination data at red and green targets would indicate that the condition of optical changes (improvement or deterioration) is related rather to the lens than the cornea. The visual and glare testing for both the better and worse eyes can give the results in the reference task for computer works and prognosticate impairments which significantly affect driving performance for any of the driving tasks (eg, the effects of cataracts, binocular visual field restriction, monocular vision).
We evaluated NAC 1% eye drops in the short-term 9-month therapy of cataracts and for improvement of visual functions in older subjects with no cataract. The NAC 1% eyedrops seem to improve the vision of the older adult subjects regardless of whether they have cataracts or not, but the improvement of visual acuity was significantly better in the group of cataract subjects versus the older adult subjects in the noncataract matched older adult group. This is an additional mode of evidence suggesting that carnosine applied in the form of NAC reverses lens opacity in humans [Citation5,Citation10, Citation16–Citation18, Citation21–Citation23]. Utilizing the specific purity NAC ingredient manufactured at the cGMP facility according to specification developed by IVP (), as a source of pharmacological principal l-carnosine, we have created the ophthalmic sustained drug delivery formulation (), which contains varying amounts of the actives tailoring the enhanced intraocular absorption of the beneficial ingredient, naturally occurring dipeptide l-carnosine, to optimize its specific effect and purpose in producing the basic bioactivating antioxidant activity in vivo and reducing toxic effects of lipid peroxides to the crystalline lens. When cataract was accompanied with POAG, NAC was prescribed 15 min prior the topical application of beta-blocker, specifically used to decrease the intraocular pressure.Citation23 The improvement of visual functions in patients with cataracts associated with POAG was accompanied with significant decrease of intraocular pressure and increase in the outflow facility in the eyes of patients with POAG treated with the indicated combined therapy.Citation23 The treatment with NAC is improving eyesight in older adult cataract-free patients as intraocular released carnosine reacts with oxygen radicals, lipid peroxidation products, and carbohydrate oxidation products accumulated in the crystalline human lens with aging.Citation3,Citation5
The entire body of supporting research on NAC and its bioactivated principle carnosine reveals its promise as a water-soluble universal antioxidant that works at several levels to defend against the oxidative stresses to the lens, glycosylation problems, and protect the lens proteins and the membrane lipids from oxidative damages thus preventing and reversing age-related cataracts in human eyes. Carnosine has been proposed to act as antioxidant in vivo and its activity in the crystalline lens can be related to the prevention of the free-radical-induced inactivation of activity of the proprietary antioxidant enzymes in the crystalline lens, such as Cu, Zn-superoxide dismutase (SOD). The protective effects of carnosine and related compounds against the oxidative damage of human SOD by peroxyl radicals generated from 2,2’-azobis(2-amidinopropane) dihydrochloride (AAPH) were established.Citation32 Carnosine exhibits an ability to inhibit lipid peroxidation (LPO) catalysts besides inhibiting free metals, scavenging OH · and lipid peroxyl (RO2·) radicals or donating hydrogen ions. In addition to inhibiting the generation of lipid peroxyl radicals, carnosine catabolyzes lipid hydroperoxides to their alcohols both in aqueous medium and in a phospholipid system.Citation2 A possibility exists from our studies that carnosine is reacting directly with MDA and other aldehydes/ketones. Indeed carnosine has been shown to protect against MDA-induced crosslinking and toxicity, and a hydroxynonenal-carnosine adduct has recently been characterized, providing further evidence for carnosine’s potential as an aldehyde scavenger.Citation33 The ability of l-carnosine to inhibit LPO reactions as well as to diminish the content of LPO products makes its ophthalmic prodrug NAC applied with lubricant carboxymethylcellulose a prominent tool in the therapy especially, of the posterior subcapsular and cortical cataracts, whose mechanism can be related with the toxic effects of LPO products.Citation34
In the cataractous lens, crosslinking of proteins by any means increases their effective molecular weight and produces light scattering and consequent lenticular opacity. The production of such high molecular weight protein complexes by disulphide bridges and covalent links with dialdehydes has been implicated in the formation of senile and other cataracts in humans. Both types of cross-linking may be caused by depletion of the lens’ reduced glutathione and accumulation of LPO products in the lens tissue. The results of our studies strongly suggest that l-carnosine released from its ophthalmic prodrug NAC during its application to the eyes with cataracts is able to prevent the loss of reduced glutathione and to remove the secondary LPO products in biological systems. This, in turn, may lead to dissociation of the intermolecular protein cross-links due to glutathione-protein thiol-disulphide exchange mechanism and utilization of lipid peroxides and dialdehydes derived from LPO process, anchoring protein-lipid complexes in the lens.Citation35 There is a rising evidence that carnosine prevents oxidation and glycation, both of which contribute to the crosslinking of proteins.Citation36 The results suggest that histidine is the representative structure of l-carnosine for an anticrosslinking agent, containing the necessary functional groups for optimal protection against crosslinking agents. It has been proposed that the imidazolium group of histidine of carnosine may stabilize adducts formed at the primary amino group.Citation36 Cellular aging is often associated with an increase in protein carbonyl groups arising from oxidation and glycation-related phenomena and suppressed proteasome activity. These “aged” polypeptides may either be degraded by 20S proteasomes or cross-link to form structures intractable to proteolysis and inhibitory to proteasome activity. For example, effects of l-carnosine on proteasome activity in the lens might explain the apparent decline in cataract, as proteasome activity is known to decline during lenticular ageing.Citation37,Citation38
Protein glycation, which promotes aggregation, involves the unwanted reaction of carbohydrate oxidation products with proteins. Glycation of lens α-crystallin occurs in vivo and may contribute to cataractogenesis. Antiglycation compounds such as carnosine may be preventive, but interestingly carnosine reverses lens opacity in human trials. The mechanism for this observation may involve carnosine’s ability to disaggregate glycated protein. Seidler and colleaguesCitation39 recently investigated this hypothesis using glycated α-crystallin as the in vitro model. The obtained in the present study data can be satisfactorily explained by the cited above ability of carnosine to protect cellular and tissue structures from aldehydes, which in excess may be toxic because of the nonenzymatic glycosylation of proteins. Glycation, preferentially modifies the ɛ-amino group of lysine residues in proteins, especially when proline neighbors lysine. It is likely that the structural similarity between lysyl-proline and β-alanyl-histidine allows carnosine to demonstrate its transglycation properties, eg to compete for the glycating agent, protecting proteins (lens crystallins) against modification.Citation40 This cited core action of carnosine may totally protect lens tissue and cellular proteins from aldehydes, and this effect may be the main mechanism by which carnosine protects the crystalline lens against osmotic shock, oxidative stress, or toxic effects of several metabolites, including the eventual crosslinking of crystalline lens biomacromolecules with sugar(s)’ metabolites and/or ascorbic acid oxidation byproducts. Actually, carnosine may prevent accumulation of Amadori products (forming after rearrangements of products of primary glycation) within lens cells and tissues as well as cross-linking of biomolecules.Citation40 At moderately high concentrations, carnosine also reverses protein-aldehyde cross-linking, a reaction that is difficult to reverse, thus providing a rejuvenating effect on the lens for vision. Aggregation of crystallins, the lens proteins, is one of the basic stages of cataract formation. Among the protein aggregation models used to study the molecular mechanisms of the initial stages of lenticular opacity, UV-induced aggregation of βl-crystallin is most close to the in vivo conditions. Both carnosine and the carnosine derivative NAC have been shown to be effective in inhibiting the UV-induced aggregation of βl-crystallin at 20 mM concentration. The molecular chaperon-like properties similar to those of α-crystallin underlie the anticataract mechanism of action of carnosine and of the acetyl derivative of carnosine (prodrug).Citation5
Carnosine when present at surprisingly high levels (about 20 mM or over) can delay senescence of cells and reverse the senescent phenotype, restoring a more juvenile appearance. As better antioxidants/free-radical scavengers than carnosine do not demonstrate these antisenescent effects,Citation41 additional properties of carnosine must contribute to its antisenescent activity. Having shown that carnosine can react with protein carbonyls, thereby generating “carnosinylated” polypeptides using model systems,Citation41 it might be generally proposed that similar adducts can be generated in senescent cataractous lens fiber cells exposed to carnosine during the therapeutical treatments with 1% NAC lubricant eye drops in vivo.
These observations suggest that NAC may prevent and reverse cataracts. This therapeutic modality gives the most efficacious uptake of l-carnosine in the aqueous humor protecting carnosine from the short-term hydrolysis and this dipeptide is known to be an endogenous component in the mammalian and lens tissues.Citation23 NAC was used as a prodrug of an antioxidant that is resistant to hydrolysis with human serum carnosinase.Citation3 The l-carnosine liberated in aqueous humor can provide antioxidant protection in the areas around the lens, and penetrate and accumulate in the lens tissue.Citation3
The developed light-scattering factor of glare sensitivity recorded with a colored luminous target is shown to be a valuable clinical index of lens transparency. After 9 months, the worse and better eyes of older adult drivers and older drivers with cataract treated with 1% NAC generally showed an improvement of visual functions as compared with baseline. The results of glare testing shows a reduction of light scattering in the worse and better eyes of older drivers. Glare sensitivity improvement was accompanied by improvement in visual acuity more pronounced in the eyes with cataract during treatment with NAC. The data of visual functions (visual acuity, glare sensitivity) in older adult subjects and older subjects with cataract treated with 1% NAC showed significant improvement as compared, by contrast with the control group which showed generally no improvement in visual functions, with no difference from baseline in visual acuity and glare sensitivity readings. In most of the patients treated, study treatment was well tolerated and no ocular or systemic adverse events were reported. Use of NAC to treat cataract and aging lens can lead to diminishing of light scattering units in the lens which raise glare effect, probably by prevention of the oxidative modification of crystallins and utilization of lipid peroxides.Citation42
NAC acts as a universal antioxidant both in the lipid phase of the cellular lens membranes and in their aqueous environment and protects the crystalline lens from oxidative stress-induced damage.Citation3
Conclusion
The results of this study provide a substantial basis for further evaluation of NAC in the treatment and prevention of visual impairment in the temporal cross-sections of an older population several years apart. This ophthalmic drug showed potential for the nonsurgical treatment of age-related cataracts for participants after controlling for age, gender and daily activities and on a combined basis of repurchases behavior reports in various significant cohort survivors, now has been demonstrated to have a high efficacy and good tolerability for prevention and treatment of visual impairment determined for the older population with relative stable pattern of causes for blindness and visual impairment.
Acknowledgements
This work was planned, organized, and supported by Innovative Vision Products, Inc. (IVP; County of New Castle, DE, USA). IVP is a holder of the worldwide patent (including PCT International Publication Number WO 2004/028536 A1) for the application of N-acetylcarnosine for the treatment of ophthalmic disorders, including cataracts. IVP is a pharmaceutical and nanotechnology development company with a direct practical focus on a clinical research in the fields of ophthalmology, research and development of innovative chemical entities, drug-delivery systems, and unique medical devices to target specific biomedical applications. Over the last decade IVP has developed a track record in developing these technologies to effectively address the unmet needs of specific diseased populations.
Notes
* Or what is necessary to bring the solution up to a pH of ∼6.3–6.8.
References
- GulewitschWAmiradzibiS[Uber das carnosin, eine neue organische Base des Fleischextraktes.]Ber Deutch Chem Ges19003319023
- BabizhayevMASeguinM-CGueyneJL-Carnosine (β-alanyl-L-histidine) and carcinine (β-alanylhistamine) act as natural antioxidants with hydroxyl-radical-scavenging and lipid peroxidase activitiesBiochem J1994304509167998987
- BabizhayevMAYermakovaVNSakinaNLN-acetylcarnosine is a prodrug of L-carnosine in ophthalmic application as antioxidantClin Chim Acta19962541218894306
- BoldyrevAADupinAMBuninAYThe antioxidative properties of carnosine, a natural histidine containing dipeptideBiochem Int1987151105133326603
- BabizhayevMADeyevAIYermakovaVNRevival of the lens transparency with N-acetylcarnosineCurr Drug Ther2006191116
- KupferCUnderwoodBGillenTLeading causes of visual impairment worldwideAlbertDMJakobiecFAPhiladelphiaWB Saunders and Co1994124955
- Vision Research A National Plan 1999–2002Report of the National Advisory CouncilNational Eye Institute199859
- KupferCThe conquest of cataract: a global challengeTrans Ophthalmol Soc1984104110
- BabizhayevMADeyevAIYermakovaVNImage analysis and glare sensitivity in human age-related cataractsClin Exp Optom2003861577212767250
- BabizhayevMADeyevAIYermakovaVNEfficacy of N-acetylcarnosine in the treatment of cataractsDrugs R D200238710312001824
- BabizhayevMAGlare disability and driving safetyOphthalmic Res200335192512566859
- BabizhayevMASeguinM-CProcess of assessment of ocular dysfunctions and implementation devices of this process US Patent No. 6,007,203. Date of patent: December 28, 1999
- BaileyILBullimoreMAA new test for the evaluation of disability glareOptom Vis Sci199168911171787947
- American Academy of OphthalmologyContrast sensitivity and glare testing in the evaluation of anterior segment diseaseOphthalmology (Rochester)19909712337
- BabizhayevMAOphthalmic pharmacology of N-acetylcarnosine lubricant eye dropsJ Pharmacol Toxicol2006120133
- BabizhayevMADeyevAIYermakovaVNN-Acetylcarnosine, a natural histidine-containing dipeptide, as a potent ophthalmic drug in treatment of human cataractsPeptides2001229799411390029
- BabizhayevMAYermakovaVNDeyevAIImidazole-containing peptidomimetic NACA as a potent drug for the medicinal treatment of age-related cataract in humansJ Anti-Aging Med200034362
- BabizhayevMARejuvenation of visual functions in older adult drivers and drivers with cataract during a short-term administration of N-acetylcarnosine lubricant eye dropsRejuvenation Res200471869815588519
- FerrisFLKassoffABresnickGHNew visual acuity charts for clinical researchAm J Ophthalmol1982949167091289
- FerrisFLSperdutoRDStandardized illumination for visual acuity testing in clinical researchAm J Ophthalmol1982949787091290
- BabizhayevMABozzo CostaEComposizioni farmaceutiche contenenti N-acetilcarnosina per il trattamento della cataratta Italian Patent A61K gruppo 37/00 20122 MI, Priority. October 15, 1993
- BabizhayevMABozzo CostaEPharmaceutical compositions containing N-acetylcarnosine for the treatment of cataract Patent PCT/EP 94/03340 SCB 238 PCT. October 10, 1994
- BabizhayevMAMethod for topical treatment of eye disease and composition and device for said treatment PCT Patent Application. International Publication Number WO 2004/028536 A1. April 8, 2004
- OwsleyCStalveyBTWellsJVisual risk factors for crash involvement in older drivers with cataractArch Ophthalmol2001119881711405840
- WrightISKeeping an eye on the rest of the bodyOphthalmology198794119683684238
- FishmanGABacaWAlexanderKRVisual acuity in patients with best vitelliform macular dystrophyOphthalmology19931001665708233392
- WuDZWuLChangFXVisual rehabilitation in low vision patients with aging macular degenerationJ Am Optom Assoc19956639417884140
- CarterTLAge-related vision changes: a primary care guideGeriatrics19944937478088558
- KleinRAge-related eye disease, visual impairment, and driving in the elderlyHum Factors19913352151769672
- ElliottDBBullimoreMAAssessing the reliability, discriminative ability, and validity of disability glare testsInvest Ophthalmol Vis Sci199334108198425818
- Van den BergTJTPImportance of pathological intraocular light scatter for visual disabilityDoc Ophthalmol198661327333948666
- KangJHKimKSChoiSYProtective effects of carnosine, homocarnosine and anserine against peroxyl radical-mediated Cu,Zn-superoxide dismutase modificationBiochim Biophys Acta20021570899611985892
- AldiniGCariniMBerettaGCarnosine is a quencher of 4-hydroxy-nonenal: through what mechanism of reactionBiochem Biophys Res Commun200229869970612419310
- BabizhayevMADeyevAILens opacity induced by lipid peroxidation products as a model of cataract associated with retinal diseaseBiochim Biophys Acta19891004124332742866
- BabizhayevMAAntioxidant activity of L-carnosine, a natural histidine-containing dipeptide in crystalline lensBiochim Biophys Acta19891004363712758030
- HobartLJSeibelIYeargansGSAnti-crosslinking properties of carnosine: Significance of histidineLife Sci20047513798915234195
- TaylorADaviesKJProtein oxidation and loss of protease activity may lead to cataract formation in the aged lensFree Radic Biol Med1987337173322949
- MurakamiKJahngenJHLinSWLens proteasome shows enhanced rates of degradation of hydroxyl radical modified alpha-crystallinFree Radic Biol Med19908217222341052
- SeidlerNWYeargansGSMorganTGCarnosine disaggregates glycated alpha-crystallin: an in vitro studyArch Biochem Biophys20044271101515178493
- GuiottoARuzzaPBabizhayevMAMalondialdehyde scavenging and aldose-derived Schiff bases' transglycation properties of synthetic histidyl-hydrazide carnosine analogsBioorg Med Chem20071561586317604632
- HipkissARBrownsonCBertaniMFReaction of carnosine with aged proteins: another protective processAnn N Y Acad Sci20029592859411976203
- BabizhayevMAFailure to withstand oxidative stress induced by phospholipid hydroperoxides as a possible cause of the lens opacities in systemic diseases and ageingBiochim Biophys Acta1996131587998608175