Abstract
The purpose of this study was to characterize quadriceps femoris muscle fatigue of both lower extremities in patients with knee osteoarthritis (OA). Sixty-two subjects (mean age 68.2 years, standard deviation [SD] ± 7.9 years) with knee OA participated in the study. Significantly higher knee pain was reported in the involved knee than in the contralateral knee, as determined by a visual analog scale. Significant differences were demonstrated between the lower extremities in terms of maximal voluntary isometric contraction, in favor of the less involved leg (P = 0.0001). In contrast, the degree of fatigue of the quadriceps femoris muscle, as measured by the decrement in force production following ten repeated contractions, was significantly higher in the contralateral leg (P = 0.0002). Furthermore, normalization of the fatigue results to the first contraction yielded a similar result (P < 0.0001). Similar results were noted when analysis was performed separately for subjects whose involvement was unilateral or bilateral. The results indicate that, irrespective of the initial strength of contraction, the rate of muscle fatigue in the contralateral leg is significantly higher than in the involved leg. Hypotheses for these unexpected results are suggested. Rehabilitation of patients with knee OA should focus on increasing quadriceps muscle strength and endurance for both lower extremities.
Introduction
Decline in quadriceps femoris muscle strength is common in individuals with knee osteoarthritis (OA),Citation1 and is due primarily to disuse atrophy and impaired ability of the central nervous system to recruit existing motor units despite maximum conscious effort.Citation2 In contrast to strength, muscle fatigue, which is defined as a temporary loss or decrease in force-generating ability due to recent contractions,Citation3 has rarely been examined in patients with knee OA. Although methods to assess muscle fatigue in patients with knee OA have been validated,Citation4,Citation5 to the best of our knowledge, the only direct measure of muscle fatigue in this population was reported by Fisher et al.Citation6 Their study of 15 male subjects (67.6 ± 6.1 years) with knee OA demonstrated that muscle strength and endurance were 50% lower than in an age-matched control group.
Muscle fatigue has important clinical implications due to the significant role of quadriceps muscle endurance for functional capabilities in the activities of daily living, such as walking and climbing stairs. As these capabilities are particularly affected in patients with knee OA,Citation7 there is a need to expand our understanding of the characteristics of quadriceps muscle fatigue in this population.
The scope of the literature regarding quadriceps muscle performance in patients with knee pathologies has changed in recent years, shifting from a previous focus only on the symptomatic knee to a broader view of both lower extremities.Citation8 This is probably due to the fact that patients often demonstrate symptoms in both legs. Furthermore, even when one leg is asymptomatic, cartilage degeneration might already exist and may be confirmed by radiography.Citation9,Citation10 In addition, muscle dysfunction in one leg may be a factor in hastening the progression of joint breakdown in the contralateral leg.Citation11,Citation12 Accordingly, there is justification for evaluating quadriceps muscle performance and, particularly, quadriceps muscle fatigue of both lower extremities in patients with knee OA.
The purpose of this study was to compare the fatigability of the quadriceps muscle by assessing isometric contraction properties of both lower extremities in patients with knee OA. It was expected that the affected (or more affected) leg would have weaker maximal voluntary isometric contraction (MVIC) and a higher rate of fatigue compared to the contralateral leg.
Study methodology
Subjects
All patients referred to an orthopedic outpatient physical therapy clinic between September 2008 and December 2009 with the diagnosis of idiopathic knee OA were screened by a physical therapist from the clinic using an eligibility checklist. This descriptive study is a subset of a larger cohort randomized controlled trial.Citation13
Inclusion criteria were: (1) radiographic evidence of knee OA at a grade ≥ II, according to the Kellgren and Lawrence classification;Citation14 (2) age above 50; (3) compliance matching with the classification of the American College of Rheumatology;Citation15 (4) knee pain for at least 3 months, with pain presenting at least 3 days a week during the last month; (5) ability to ambulate independently for at least 10 meters; and (6) ability to follow simple instructions. Exclusion criteria were: (1) use of a pacemaker; (2) history of cardiovascular, neurological, or orthopedic problems that could affect functional performance; (3) previous knee surgery other than arthroscopy; (4) injections to the knee joint during the previous 6 months; and (5) change in pain medication in the previous month.
The study coordinator explained the purpose and procedures of the study to the eligible participants. The study was approved by the Helsinki committee of the Emek Medical Center, and all subjects signed an informed consent form prior to assessment.
Procedures
The subjects completed questionnaires regarding their knee pain intensity, followed by an assessment of their quadriceps muscle performance.
Pain assessment
Subjects evaluated their level of knee pain during the previous week on a visual analog scale (VAS), with 0 representing no pain and 10 representing the most severe pain (intraclass correlation coefficient [ICC] = 80).Citation16
Assessment of the quadriceps femoris muscle isometric contraction
A computerized myometry system (Quantitative Muscle Assessment [QMA] system; Aeverl Medical, Gainesville, GA, USA) was used for all quadriceps muscle assessments. Test–retest reliability for this apparatus was previously determined in our laboratory (ICC = 0.89).Citation17 Assessment included the following tests: (1) quadriceps muscle MVIC test; (2) quadriceps muscle fatigue test. The two tests were implemented in the same order for all patients, and there was a 5-minute rest period between tests.
Both knees were tested with the uninvolved or less painful leg (in the case of bilateral knee involvement) tested first, followed by the involved leg. All quadriceps muscle assessments were carried out while the subjects were seated on a straight-back chair, with hips flexed at 90° and knees flexed as close to 90° as could be tolerated a protocol previously used for muscle assessment with knee OA.Citation18–Citation20 The thigh, chest, and pelvis were stabilized using inelastic straps with hook-and-loop closures to prevent substitution movements by the body, and the arms were positioned across the chest. The ankles were attached to a padded strap placed 2 cm above the lateral malleolus and connected to a high-tension wire with a strain gauge (SM250 force transducer). The system’s software provided summary data of force and force-integral outputs at a 50 Hz data acquisition rate.
MVIC
The subjects first performed a 5-minute warm-up on a stationary bicycle with no resistance. The subjects were then seated in the testing apparatus and following a 5-minute rest period performed three to five isometric contractions against the strain gauge at 50%, 75%, and 100% of their perceived MVIC.Citation21 To achieve this goal, the subjects were instructed to “push the strain gauge at 50%, 75%, and 100% of what you perceive your maximum force to be.” The intensity of these contractions was monitored on the screen of the computer by the researcher to ensure that the subjects understood the instructions. The data for these preliminary contractions were excluded from the analysis.
Following a second 5-minute rest break, participants performed three consecutive brief (∼5-second) MVICs of the quadriceps, each separated by 90 seconds of rest. The investigators offered standardized verbal encouragement throughout the testing protocol. An additional contraction was attained when one of the consecutive MVICs differed by more than 5% from the others. The mean of the three MVIC trials was utilized for subsequent calculations. In addition, the values were normalized to the subjects’ weight.
Fatigue test procedure
The subjects were asked to perform ten consecutive MVICs of the quadriceps muscle, each lasting 10 seconds.Citation22,Citation23 Two indexes were utilized in order to quantify quadriceps muscle fatigue in each leg: (1) the fatigue index was calculated by subtracting the value of the tenth MVIC from the value of the first MVIC; (2) the fatigue index normalized to the first contraction. For the fatigue index, the first contraction was defined as 100%, and all other contractions were defined as a percentage of this contraction. The index value was calculated as the tenth contraction (in percentage) subtracted from 100. Thus, in both indexes, lower numbers indicate greater fatigue.
Statistical analyses
The following variables were considered for analysis: VAS; MVIC; fatigue index; normalized fatigue index. Additionally, the muscle force and fatigue measures were normalized to body-weight. Descriptive statistics (means, standard deviations [SDs]) were calculated for all outcome measures. Normalized distribution was determined for all variables using the Shapiro–Wilk test. One-way analyses of variance (ANOVAs) were performed to determine differences between the involved leg and the contralateral leg with all subjects grouped together, as well as separately for subjects whose involvement was unilateral or bilateral. Since a large variability in body mass index (BMI) was observed, the analysis was repeated with the BMI as a covariant, for the entire group as well as for each group separately, for all outcome measures. Level of significance was set at α = 0.05. Statistical analyses were performed using JMP (SAS Institute, Cary, NC, USA).
Results
Of the 134 patients with a diagnosis of knee OA who were considered as potential candidates for the study, 62 subjects (51 females, eleven males) were found to be eligible to take part in the study based on the inclusion/exclusion criteria. The characteristics of the 62 subjects are presented in .
Table 1 The subjects’ characteristics (n = 62)
Forty-three subjects had a bilateral leg involvement and 19 subjects had a unilateral involvement. In case of bilateral involvement, the more painful leg was considered the involved leg. The muscle performance results of the entire group, as well as the separate results of the group with unilateral involvement and the group with bilateral involvement, are presented in . As the results of the statistical analysis of all the muscle performance variables normalized for weight did not differ from the results of the non normalized values, only the non normalized values are presented (see ). Additionally, analysis with BMI as a covariant determined no significant effect of BMI on any of the outcome measures.
Table 2 Quadriceps femoris muscle isometric contraction performance of both legs (mean ± SD) and comparison between the legs (P-value) of the entire group and of the groups with unilateral and bilateral leg involvement
Pain intensity
The mean (SD) pain intensities of the entire group of the involved knee and contralateral leg were 7.2 cm (1.95) and 3.2 cm (2.86), respectively. The overall difference between the legs with respect to pain intensity was statistically significant (P < 0.0001). In the group with unilateral involvement, mean (SD) VAS of the involved leg was 6.3 cm (2.14), with no pain reported in the contralateral leg. In the group with bilateral involvement, mean (SD) VAS of the more affected sides and the less affected side were 7.6 cm (1.66) and 4.6 cm (2.26), respectively. In both subgroups with the unilateral and bilateral leg involvement the difference between the legs with respect to pain intensity was statistically significant (P < 0.0001).
Quadriceps femoris muscle isometric contraction performance
The 90° knee flexion position was well tolerated by all subjects. The MVIC in the involved leg of the entire group was significantly lower than in the contralateral leg (P = 0.0001). Similar statistical differences were observed in the groups with unilateral and with bilateral leg involvement (see ).
Fatigue test performance
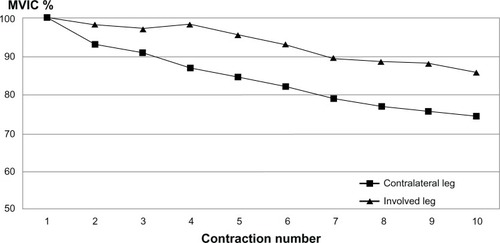
The mean (±SD) force of the first and tenth contractions in the fatigue tests of the entire group, and of the groups with unilateral and bilateral involvement, are presented in . The degree of fatigue of the quadriceps muscle, as indicated by the fatigue index of the entire group, was significantly greater in the contralateral leg than in the involved leg (P = 0.002) (see and ). This significant difference between the legs held true even when the fatigue index was normalized to the first contraction (P < 0.0001) (see and ). This additional analysis was conducted as the first MVIC of the contralateral leg was significantly stronger than the first contraction of the involved leg (see above; P = 0.0001). The separate analysis, by group, indicated significant leg difference in the two fatigue indexes in the groups with unilateral and with bilateral leg involvement (P = 0.04, P < 0.0001, respectively), except that in the group with unilateral involvement (n = 19), the comparison between legs for the normalized fatigue index did not quite reach significance (P = 0.12).
Table 3 The mean (±SD) force of the first and tenth contractions in the fatigue tests of the entire group and of the groups with unilateral and bilateral leg involvement
Figure 1 Mean strength of ten consecutive quadriceps femoris muscle maximal voluntary isometric contractions (MVICs) of both legs.
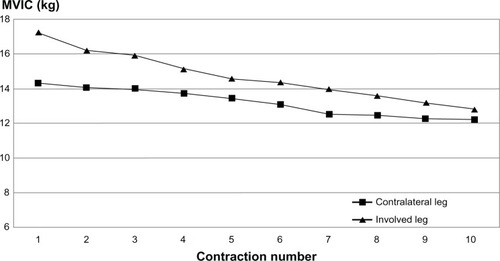
Figure 2 Mean strength of ten consecutive quadriceps femoris muscle maximal voluntary isometric contractions (MVICs) normalized to the first contraction of both legs.
Discussion
Significant differences were observed between the lower extremities in terms of MVIC of the quadriceps muscle in the entire group and in the subgroups with the unilateral and bilateral leg involvement, in favor of the less involved leg. In contrast, surprisingly, the degree of fatigue (decrement in force generating ability following recent repeated contractions) of the quadriceps muscle was significantly higher in the less involved or uninvolved knee. It appears these results have never been previously reported.
As the contralateral leg was significantly stronger to start with, in the overall group and in the subgroups, which could affect fatigue difference between legs, a normalization of the fatigue results was done to the first contraction. Yet, this analysis provided similar results which may indicate that irrespective of the initial strength of contraction, the rate of muscle fatigue in the contralateral leg is significantly higher than in the involved leg. The only exception to this rule was demonstrated in the normalized fatigue index for the subgroup of patients with unilateral involvement where the comparison between legs did not reach significance. However, this may be due to the small size of the group (n = 19), which did not provide sufficient power for the analysis. While it may be claimed that the greater fatigability of the less involved leg is due to a floor effect, the raw data () indicate that this is not a likely cause for the observed results.
We can only hypothesize as to the causes of this unexpected phenomenon. It might be that the pain related to OA stimulates nociceptive afferents that decrease the initial maximal force produced, as indicated by a central activation failure during MVIC.Citation2,Citation13 Consequently, the lower reduction of muscle strength during the fatigue test observed in the involved limb could be the result of submaximal muscle contraction during the consecutive isometric contractions. This may prevent muscle overload during repeated contractions and therefore reduce maximal utilization of the metabolic and excitation-coupling abilities of the muscle, subsequently reflected in the observed lower degree of muscle fatigue.
Another possibility may be related to differences in the muscle fiber composition between the quadriceps muscle of the two extremities. Selective atrophy of type II fast-twitch fibers in quadriceps muscle has been repeatedly demonstrated in histological studies involving subjects with knee OA.Citation24–Citation26 This selective fiber atrophy is suggested to occur as a consequence of pain-related immobilization due to OA.Citation27,Citation28 Muscles with a higher percentage of fast-twitch fibers have been shown to fatigue more rapidly than muscles with a greater percentage of slow-twitch fibers.Citation29 Thus, perhaps, the contralateral leg, which was significantly less painful than the involved leg, had a lower decline rate in type II fast-twitch fibers, resulting in a lower proportion of type I fatigue-resistant fibers. Accordingly, the asymmetric decline in type II fibers between the extremities rendered the quadriceps muscle of the involved leg more fatigue resistant. A similar rationale has been suggested for sex-related differences in quadriceps muscle fatigue in patients with knee OA.Citation24 A higher proportion of slow, fatigue-resistant, type I fibers noted in women is suggested as the reason for the higher degree of fatigue observed in age-matched male subjects with knee OA;Citation30–Citation32 however, further studies are needed to substantiate these speculative hypotheses.
Limitations
The current experimental design used dynamometry, which has been shown to be reliable and valid, and which is readily available in the clinical setting.Citation33 However, in spite of standardized verbal encouragements, the results may have been affected by the subjects’ motivation and pain, particularly during repeated contractions.Citation34 Further studies with larger samples should examine whether the results are affected by the severity of OA and should include a healthy control group.
Conclusion
The results of this study indicate that, while the quadriceps muscle of the involved leg is weaker than the quadriceps muscle of the contralateral leg, the decrement in quadriceps muscle force production following repeated contractions – that is, muscle fatigue – is greater in the contralateral leg. It is recommended that the rehabilitation of patients with knee OA include exercises aimed at increasing quadriceps muscle endurance for both lower extremities.
Disclosure
The authors report no conflicts of interest in this work.
References
- O’ReillySCJonesAMuirKRDohertyMQuadriceps weakness in knee osteoarthritis: the effect on pain and disabilityAnn Rheum Dis199857588949893569
- LewekMDRudolphKSSnyder-MacklerLQuadriceps femoris muscle weakness and activation failure in patients with symptomatic knee osteoarthritisJ Orthop Res20042211011514656668
- AagaardPSimonsenEBAndersenJLMagnussonPDyhre-PoulsenPIncreased rate of force development and neural drive of human skeletal muscle following resistance trainingJ Appl Physiol2002931318132612235031
- CallaghanMJMcCarthyCJOldhamJAThe reliability of surface electromyography to assess quadriceps fatigue during multi joint tasks in healthy and painful kneesJ Electromyogr Kinesol200919172180
- McCarthyCJCallaghanMJOldhamJAThe reliability of isometric strength and fatigue measures in patients with knee osteoarthritisMan Ther20081315916417296324
- FisherNMWhiteSCYackHJSmolinskiRJPendergastDRMuscle function and gait in patients with knee osteoarthritis before and after muscle rehabilitationDisabil Rehabil19971947559058029
- GuccioneAAFelsonDTAndersonJJThe effects of specific medical conditions on the functional limitations of elders in the Framingham StudyAm J Public Health1994843513588129049
- PietrosimoneBGHertelJIngersollCDHartJMSalibaSAVoluntary quadriceps activation deficits in patients with tibiofemoral osteoarthritis: a meta-analysisPM R20113153162 ; quiz 162.21333954
- ZeniJAJrSnyder-MacklerLEarly postoperative measures predict 1- and 2-year outcomes after unilateral total knee arthroplasty: importance of contralateral limb strengthPhys Ther201090435419959653
- ZhangYJordanJEpidemiology of osteoarthritisClin Geriatr Med20102635536920699159
- SlemendaCBrandtKDHeilmanDKQuadriceps weakness and osteoarthritis of the kneeAnn Intern Med1997127971049230035
- MikeskyAEMazzucaSABrandtKDPerkinsSMDamushTLaneKAEffects of strength training on the incidence and progression of knee osteoarthritisArthritis Rheum20065569069917013851
- Elboim-GabyzonMRozenNLauferYDoes neuromuscular electrical stimulation enhance the effectiveness of an exercise programme in subjects with knee osteoarthritis? A randomized controlled trialClin Rehabil20132724625722952305
- KellgrenJHLawrenceJSRadiological assessment of osteo-arthrosisAnn Rheum Dis19571649450213498604
- AltmanRDCriteria for classification of clinical osteoarthritisJ Rheumatol Suppl19912710122027107
- BoonstraAMSchiphorst PreuperHRRenemanMFPosthumusJBStewartREReliability and validity of the visual analogue scale for disability in patients with chronic musculoskeletal painInt J Rehabil Res20083116516918467932
- LauferYElboimMEffect of burst frequency and duration of kilohertz-frequency alternating currents and of low-frequency pulsed currents on strength of contraction, muscle fatigue, and perceived discomfortPhys Ther2008881167117618703676
- BergerMJMcKenzieCAChessDGGoelaADohertyTJQuadriceps neuromuscular function and self-reported functional ability in knee osteoarthritisJ Appl Physiol201211325526222604883
- MachnerAPapGAwiszusFEvaluation of quadriceps strength and voluntary activation after unicompartmental arthroplasty for medial osteoarthritis of the kneeJ Orthop Res20022010811111853077
- StevensJEMiznerRLSnyder-MacklerLQuadriceps strength and volitional activation before and after total knee arthroplasty for osteoarthritisJ Orthop Res20032177577912919862
- LyonsCLRobbJBIrrgangJJFitzgeraldGKDifferences in quadriceps femoris muscle torque when using a clinical electrical stimulator versus a portable electrical stimulatorPhys Ther200585445115623361
- McDonnellMKDelittoASinacoreDRRoseSJElectrically elicited fatigue test of the quadriceps femoris muscle. Description and reliabilityPhysical Ther198767941945
- DuganSAFronteraWRMuscle fatigue and muscle injuryPhys Med Rehabil Clin N Am20001138540310810767
- FinkBEglMSingerJFuerstMBubenheimMNeuen-JacobEMorphologic changes in the vastus medialis muscle in patients with osteoarthritis of the kneeArthritis Rheum2007563626363317968889
- EimreMPuhkeRAlevKAltered mitochondrial apparent affinity for ADP and impaired function of mitochondrial creatine kinase in gluteus medius of patients with hip osteoarthritisAm J Physiol Integr Comp Physiol2006290R1271R1275
- TallonMJHarrisRCMaffulliNTarnopolskyMACarnosine, taurine and enzyme activities of human skeletal muscle fibres from elderly subjects with osteoarthritis and young moderately active subjectsBiogerontology2007812913716967207
- GlasbergMRGlasbergJRJonesREMuscle pathology in total knee replacement for severe osteoarthritis: a histochemical and morphometric studyHenry Ford Hosp Med J19863437403700127
- NakamuraTSuzukiKMuscular changes in osteoarthritis of the hip and kneeNihon Seikeigeka Gakkai Zasshi1992664674751387155
- LinssenWHStegemanDFJoostenEMForce and fatigue in human type I muscle fibres. A surface EMG study in patients with congenital myopathy and type I fibre predominanceBrain1991114Pt 5212321321933237
- BergerMJMcKenzieCAChessDGGoelaADohertyTJSex differences in quadriceps strength in OAInt J Sports Med20123392693322706942
- StaronRSHagermanFCHikidaRSFiber type composition of the vastus lateralis muscle of young men and womenJ Histochem Cytochem20004862362910769046
- WüstRCMorseCIde HaanAJonesDADegensHSex differences in contractile properties and fatigue resistance of human skeletal muscleExp Physiol20089384385018296492
- CairnsSPKnickerAJThompsonMWSjøgaardGEvaluation of models used to study neuromuscular fatigueExerc Sport Sci Rev20053391615640715
- MaïsettiOGuévelALegrosPHogrelJYSEMG power spectrum changes during a sustained 50% maximum voluntary isometric torque do not depend upon the prior knowledge of the exercise durationJ Electromyogr Kinesiol20021210310911955982