Abstract
Aim
The aim of our study was to retrospectively evaluate the effectiveness and safety of cataract surgery and intraocular lens implantation (IOL) for patients aged 90 years or older, whom we define as “very elderly.”
Methods
The study involved a total number of 122 patients (122 eyes) with senile cataracts. The mean age of patients was 91.2 ± 2.3 years (range 90–100 years old). Phacoemulsification (phaco) was done on 113 of 122 eyes, and 9 of 122 eyes had extracapsular cataract extraction (ECCE). Postoperative visual acuity and intraocular pressure (IOP) were analyzed on the first postoperative day, 3 months after surgery, and 6 months after surgery.
Results
Best corrected visual acuity (BCVA) improved in 100 of 122 eyes (82.0%). BCVA remained the same in 20 of 122 eyes (16.4%) and decreased in 2 of 122 eyes (1.6%), mainly because of coexisting age-related macular degeneration (AMD). The BCVA 3 months after surgery was ≥0.8 in 23 of 122 eyes (18.9%), between 0.5 and 0.7 in 28 of 122 eyes (22.3%), and between 0.2 and 0.4 in 33 of 122 eyes (27.1%). We found significant implications of cataract surgery on decreasing IOP in the studied group of patients suffering from glaucoma compared to the patients without glaucoma.
Conclusion
Advanced age is not a contraindication for cataract surgery. The results of the study showed that when systemic conditions are stable, both phaco and ECCE with IOL for very elderly patients are effective and safe.
Introduction
Age-related ocular diseases such as cataracts will assume increasing importance in the public health of the Polish nation. Cataracts are a common cause of visual acuity (VA) loss and reduced quality of life in the elderly population.Citation1
Over the last few years, life expectancy in Poland has been increasing steadily, and forecasts for the future are optimistic. For men, this rate is predicted to grow from the current 70.4 years to 77.6 years by 2035, while for women, we can expect an increase from 78.8 years to 83.3 years (compared with 56.0 and 61.6 years, respectively, in 1950).Citation2
The occurrence of cataracts is strongly related to aging; however, there is little information in the literature on the final visual results and safety of cataract surgery and intraocular lens (IOL) implantation in the group defined as “very elderly.”Citation3,Citation4
In a study of 802 consecutive cataract operations, Berler found that patients >88 years of age were at increased risk of complications compared with those under 88.Citation5 Syam et al also found a higher incidence of complications, in a retrospective study of perioperative complications of cataract surgery in a group of very elderly patients, although the studied group was small (34 eyes from 21 patients).Citation6
The number of patients eligible for cataract surgery is predicted to increase as a result of greater surgical safety and an increase in the proportion of elderly people in the population.Citation7 Furthermore, visual impairment leads to reduced quality of life, poorer general health, and increased mortality.Citation8,Citation9
Cataracts are one of the conditions responsible for impaired vision in the very elderly. The decrease of vision is a serious risk factor for loss of balance, perhaps leading to falls and injury. Many risk factors for falling among elderly people have been identified in epidemiological studies, including poor vision.Citation10 Hip fractures in the elderly are commonly caused by falls. The authors established that cataract surgery is an effective intervention to reduce the risk of falls in elderly patients with cataract-related visual impairment.Citation11–Citation13
The aim of our study was to retrospectively evaluate the effectiveness and safety of cataract surgery and IOL implantation in patients aged 90 years or older, whom we define as “very elderly.” Visual outcomes and their relation to the coexisting disorders and to the complications were analyzed.
Methods
The study was retrospectively conducted between 2008 and 2010 at University Hospital No 5 of the Medical University of Silesia. The study involved a total of 122 patients (122 eyes) with senile cataracts. All operations were performed by surgeons from the Special Cataract Clinic, who are all highly experienced in phacoemulsification (phaco).
In this study we included patients >90 years old, who had significant bilateral cataracts causing impairment of visual functions not correctable by glasses (best corrected visual acuity [BCVA] worse than 0.7), or with unacceptable glare, polyopia, or reduced quality of vision attributable to cataracts. The exclusion criteria were age under 90 years, a preoperative BCVA of 0.7 or better, a baseline endothelial cell density of less than 1500 cells/mm2, uncontrolled glaucoma, and physical or mental disability that would make it difficult to perform the surgery. The mean age of the patients was 91.2 ± 2.3 years (range 90–100 years old). Surgery was performed on 43 men (mean age 90.4 years) and 79 women (mean age 91.5 years). Phaco was done on 113 of 122 eyes and 9 of 122 eyes had extracapsular cataract extraction (ECCE).
Surgical techniques
Phaco was developed in 1967 by Charles D Kelman and is now the most common technique used in developed countries.Citation14 It involves the use of ultrasounds to emulsify the cataractous lens through a small incision (1.8–3.2 mm). The artificial IOL is inserted directly to the lens capsule.
ECCE involves the removal of the cataractous lens while the posterior capsule is left intact to allow implantation of an intraocular lens. The lens is removed through a large (usually 10–12 mm) incision. This method may be indicated for patients with very hard cataracts.
The type of anesthesia used depended on the preference of the surgeon and general condition of the patient. These included topical drop anesthesia in 110 of 122 patients, sub-Tenon’s and peribulbar anesthesia in 10 of 122 patients, and general anesthesia only in two cases because of inability to understand verbal commands.
During the clinical examination on the day of surgery, visual and clinical data were collected prospectively. Ocular comorbidity was defined as: coexisting ocular disease identified preoperatively that was likely to limit the final VA outcome. The Snellen VA was converted to decimal values for statistical calculations.
The primary outcome measures were postoperative BCVA, intraocular pressure (IOP) using Goldmann Applanation Tonometry, and intraoperative and postoperative complications. Postoperative VA and IOP were analyzed on the first postoperative day, 3 months, and 6 months after surgery.
The statistical analysis was carried out using the Statistica 10.0 PL (StatSoft, Inc., Tulsa, OK, USA) with Student’s t-test performed for normal distribution (preoperative IOP between patients with and without coexisting glaucoma, pre- and postoperative IOP in both groups) of the results in the study groups, or the Mann–Whitney U test in non-normal distribution (postoperative IOP between patients with and without coexisting glaucoma). Analysis of variance (ANOVA) with Tukey’s HSD post-hoc test was applied to compare the first day, 3 months, and 6 months after surgery. For all statistical tests, a P-value of <0.05 was considered to indicate statistical significance.
All subjects gave an informed consent before participating in the study, and research followed the tenets of the Declaration of Helsinki.
Results
In the group of 122 eyes, 41 (33.6%) had no ocular comorbidity identified before surgery. The 81 eyes (66.4%) with ocular comorbidity included 54 (44.3%) with age-related macular degeneration, 26 (21.3%) with glaucoma, 15 (12.3%) with pseudoexfoliation syndrome, 8 (6.6%) with corneal opacity, 15 (12.3%) with hypertensive retinopathy, and 9 (7.4%) with diabetic retinopathy.
Mean postoperative scores were significantly better compared to the preoperative level. The BCVA was ≤0.1 in 94 of 122 eyes (77.1%), between 0.2–0.4 in 24 of 122 eyes (19.7%), and between 0.5–0.7 in four of 122 eyes (3.3%). The postoperative BCVA 3 months after surgery was ≥0.8 in 23 of 122 eyes (18.9%), between 0.5–0.7 in 28 of 122 eyes (22.3%), and between 0.2–0.4 in 33 of 122 eyes (27.1%).
VA improved in 100 of 122 eyes (82.0%), remained the same in 20 of 122 eyes (16.4%), and decreased in two of 122 eyes (1.6%), mainly because of coexisting age-related macular degeneration (AMD).
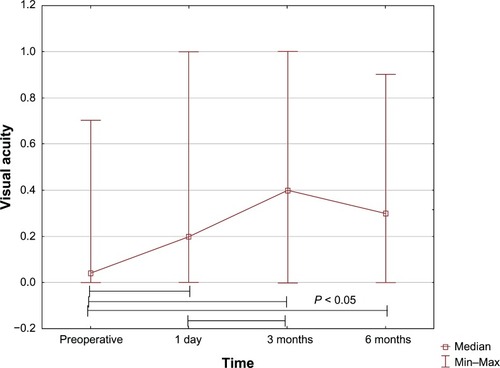
We found significant difference between pre- and postoperative VA on the first day, 3 months, and 6 months after cataract surgery. We also found significant difference between VA measured on the first day and 3 months after surgery, but there was no difference between the 3-month and 6-month postoperative VA. We did not observe significant differences in VA between patients operated on with phaco and ECCE between 3 months and 6 months after surgery. The results are presented in and .
Table 1 Details of follow-up and visual outcomes in very elderly patients following cataract surgery
Figure 1 Visual acuity in the studied group (n = 122) of very elderly patients before and after cataract surgery (ANOVA).
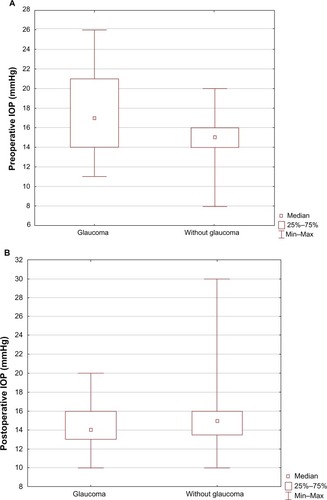
We found significant difference in preoperative IOP between patients with and without coexisting glaucoma (17.7 ± 3.4 mmHg versus 14.8 ± 2.4 mmHg, P = 0.002).
On the first postoperative day we observed a decrease of IOP in the group of glaucoma patients (14.2 ± 2.4 mmHg), but there was no difference in IOP compared to patients without glaucoma (14.5 ± 2.5 mmHg). Postoperative IOP had significantly decreased in glaucoma patients compared to the preoperative period (17.7 ± 3.4 mmHg versus 14.2 ± 2.4 mmHg, P = 0.002). We found no difference in IOP on the first day, 3 months, and 6 months after surgery. Results are presented in .
Figure 2 IOP in patients before (A) and after (B) cataract surgery.
Abbreviations: IOP, intraocular pressure; Min–Max, minimum to maximum.
The most frequent complications following cataract surgery in very elderly patients in our study were posterior capsule tear without vitreous loss and corneal decompensation. Both were found in three patients (2.5%). A dropped nucleus and vitreous loss were found in only one eye (0.8%). Postoperative uveitis occurred in two eyes (1.6%). The overall complications rate in the studied group of very elderly patients was 8.2%.
Discussion
Cataracts are one of the most frequent reasons for visual impairment around the world. Cataracts in very elderly patients can cause progressively painless vision loss. Because of the demographic shift in developed countries toward older age, the prevalence of cataracts in the population as a whole has increased. It is difficult to perform cataract surgery on an elderly patient owing to additional difficulties like coexisting systemic disorders, the difficulty of patient cooperation during surgery, higher incidence of hard nucleus, smaller pupil size and high rate of pseudoexfoliation syndrome. We found little evidence to support the hypothesis that age alone is a risk factor for the intraoperative complications of phaco cataract surgery.
The lack of data on very elderly patients may be due to the relatively few patients of this age who have undergone cataract surgery. Guzek et al had only 84 patients >80 years of age in a group of 1000 cases of cataract surgery;Citation15 Davison conducted a study of 2839 patients wherein only 1.3% of the patients were aged ≥90 years.Citation16
Many elderly people have ocular and systemic comorbidities. In a UK National Cataract Surgery Survey, one in three participants had a pre-existing ocular condition that could significantly affect cataract surgery outcomes.Citation17 In that study, AMD was present in 15% of the participants, glaucoma in 10%, and diabetic retinopathy in 3%. The prevalence of these conditions, as expected, increased with age.
In the Medical Research Council Assessment and management of older people in the community trial, the authors found that in both men and women aged ≥90 years, AMD is the most important cause of visual loss (55.6% and 53.7%), and cataracts were the cause of visual loss in 33.3% and 24.1%, respectively.Citation1
Berler found that in patients under 88 years, 90.5% of eyes with complicated cataract surgery achieved a VA >6/12, compared with only 40% of complicated cataract cases when patients were >88 years old.Citation5 In a previous study, Westcott et al found that age is a significant determinant of visual outcome, with the odds of a patient with no comorbidity achieving acuity VA of >6/12 being 4.6 times higher in the 60–69 year old age group than in those >80 years old.Citation18
Our study supports these observations and others. Lundström et al have shown improvement in VA in 84.3% of patients >85 years.Citation19 Similarly, a study carried out by Applegate et al has shown improved VA in a majority of the patients (88%) above 70 years old following cataract surgery.Citation20 Our study showed that postoperative VA improved in 84% of cases. VA remained the same in 16.4% and deteriorated in 1.6% of the cases; this deterioration was attributed in 62.2% of the cases to the underlying advanced AMD.
The incidence of early postoperative IOP increase is reported to be 2.3%–8.9% in all cataract extractions.Citation21 In another study, Kim et al found more frequent (22.0%) increased IOP on the first postoperative day following cataract surgery.Citation22 The extent of such an early IOP increase was reported to be related to anterior chamber inflammation and prostaglandin release, capsulorhexis size, or residual viscoelastic material in the anterior chamber.Citation23 In contrast to the results of that study, in our study’s group of elderly patients we did not find that cataract surgery resulted in an increase of the IOP on the first postoperative day, 3 months, and 6 months after surgery; we also found significant decrease of the IOP in patients with preoperatively existing glaucoma.
It is not surprising that AMD was the primary cause of visual impairment in the studied group of patients after cataract surgery – that is consistent with results presented by other authors.Citation5 In the newest study, Owen et al report the prevalence of late AMD standardized to the UK population aged 50 years or older was 2.4%, increasing to 4.8% in those aged 65 years or older, and 12.2% in those aged 80 years or older.Citation24
In another study, Jonasson et al found a higher prevalence of AMD in the studied group.Citation25 The prevalence of early AMD was 12.4% for those aged 66–74 years and 36% for those aged ≥85 years. This is consistent with the results of our study. The authors concluded that persons aged ≥85 years have a 10-fold higher prevalence of late AMD than those aged 70–74 years.Citation25 Surgery is an effective treatment for age-related cataract-induced visual loss, though some clinicians suspect that such an intervention may increase the risk of worsening underlying AMD, and thus may have deleterious effects on vision.
Casparis et al found no significant difference in the development of AMD between groups in the immediate cataract surgery group versus patients in the delayed surgery group.Citation26 The authors suggested that the immediate surgery group fared better with quality of life outcomes than the delayed surgery group;Citation26 however, even in patients with AMD, where central vision is lost, the peripheral visual field necessary for confident navigation can be improved by cataract surgery, and can improve quality of life for very elderly patients. In a series of studies, it was found that reduced contrast sensitivity and visual field size, rather than VA, were more strongly associated with falls and fractures in elderly people.Citation27,Citation28 Although 27.7% of the AMD patients have not obtained a significant improvement of BCVA, in contrast to some previous studies we also have not observed a deterioration of VA in an observation period of 6 months.Citation29,Citation30
Conclusion
The results of the study showed that when systemic conditions are stable both phaco and ECCE with IOL implantation for very elderly patients are effective and safe. Advanced age is not a contraindication for cataract surgery. Restoration of visual function, especially in people with severe VA reduction, has a positive impact on the psychological state of patients.
Disclosure
The authors have no financial or proprietary interest in any of the products or techniques mentioned in this presentation. This work was not supported by any organization.
References
- EvansJRFletcherAEWormaldRPMRC Trial of Assessment and Management of Older People in the CommunityCauses of visual impairment in people aged 75 years and older in Britain: an add-on study to the MRC Trial of Assessment and Management of Older People in the CommunityBr J Ophthalmol200488336537014977771
- Glowny Urzad Statystyczny [webpage on the Internet]Life expectancy tables of PolandCentral Statistical Office2011 Available from: http://www.stat.gov.pl/cps/rde/xbcr/gus/POP_life_expectancy_in_2011.pdfAccessed July 10, 2013
- LeskeMCSperdutoRDThe epidemiology of senile cataracts: a reviewAm J Epidemiol198311821521656349331
- RobbieSJMuhtasebMQureshiKBunceCXingWIonidesAIntraoperative complications of cataract surgery in the very oldBr J Ophthalmol200690121516151816899530
- BerlerDKIntraoperative complications during cataract surgery in the very oldTrans Am Ophthalmol Soc20009812713011190016
- SyamPPEleftheriadisHCasswellAGBrittainGPMcLeodBKLiuCSClinical outcome following cataract surgery in very elderly patientsEye (Lond)2004181596214707968
- MinassianDCReidyADesaiPFarrowSVafidisGMinassianAThe deficit in cataract surgery in England and Wales and the escalating problem of visual impairment: epidemiological modelling of the population dynamics of cataractBr J Ophthalmol20008414810611089
- FingerRPKupitzDGHolzFGThe impact of the severity of vision loss on vision-related quality of life in India: an evaluation of the IND-VFQ-33Invest Ophthalmol Vis Sci20115296081608821693607
- LamoureuxELFenwickEPesudovosKTanDThe impact of cataract surgery on quality of lifeCurr Opin Ophthalmol2011221192721088580
- HarwoodRHVisual problems and fallsAge Ageing200130Suppl 4131811769782
- BrannanSDewarCSenJClarkeDMarshallTMurrayPIA prospective study of the rate of falls before and after cataract surgeryBr J Ophthalmol200387556056212714392
- FossAJHarwoodRHOsbornFGregsonRMZarnanAMasudTFalls and health status in elderly women following second eye cataract surgery: a randomised controlled trialAge Ageing2006351667116364936
- KulmalaJViljanenASipiläSPoor vision accompanied with other sensory impairments as a predictor of falls in older womenAge Ageing200938216216719008307
- KelmanCDPhaco-emulsification and aspiration. A new technique of cataract removal. A preliminary reportAm J Ophthalmol19676423356028631
- GuzekJPHolmMCotterJBRisk factors for intraoperative complications in 1000 extracapsular cataract casesOphthalmol1987945461466
- DavisonJAAcute intraoperative suprachoroidal hemorrhage in extracapsular surgeryJ Cataract Refract Surg19861266066223491206
- GrayCSCrabtreeHLO’ConnellJEAllenEDWaiting in the dark: cataract surgery in older peopleBMJ199931871951367136810334727
- WestcottMCTuftSJMinassianDCEffect of age on visual outcome following cataract extractionBr J Ophthalmol200084121380138211090477
- LundströmMSteneviUThorburnWCataract surgery in the very elderlyJ Cataract Refract Surg200026340841410713238
- ApplegateWBMillerSTElamJTFreemanJMWoodTOGettlefingerTCImpact of cataract surgery with lens implantation on vision and physical function in elderly patientsJAMA19872578106410663806895
- McKellarMJElderMJThe early complications of cataract surgery: is routine review of patients 1 week after cataract extraction necessary?Ophthalmology2001108593093511320024
- KimJYJoMWBraunerSCIncreased intraocular pressure on the first postoperative day following resident performed cataract surgeryEye (Lond)201125792993621527959
- O’BrienPDHoSLFitzpatrickPPowerWRisk factors for a postoperative intraocular pressure spike after phacoemulsificationCan J Ophthalmol2007421515517361241
- OwenCGJarrarZWormaldRCookDGFletcherAERudnickaARThe estimated prevalence and incidence of late stage age related macular degeneration in the UKBr J Ophthalmol201296575275622329913
- JonassonFArnarssonAEriksdottirGPrevalence of age-related macular degeneration in old persons: Age, Gene/environment Susceptibility Reykjavik StudyOphthalmology2011118582583021126770
- CasparisHLindsleyKKuoICSikderSBresslerNBSurgery for cataracts in people with age-related macular degenerationCochrane Database Syst Rev20126CD00675722696359
- de BoerMRPluijmSMLipsPDifferent aspects of visual impairment as risk factors for falls and fractures in older men and womenJ Bone Miner Res20041991539154715312256
- LordSRVisual risk factors for falls in older peopleAge Ageing200635Suppl 2ii42ii4516926203
- Fraser-BellSChoudhuryFKleinRAzenSVarmaRLos Angeles Latino Eye Study GroupOcular risk factors for age-related macular degeneration: the Los Angeles Latino Eye StudyAm J Ophthalmol2010149573574020138605
- HoLBoekhoornSSLianaCataract surgery and the risk of aging macula disorder: the Rotterdam studyInvest Ophthalmol Vis Sci200849114795480018599571