
Abstract
Purpose
There is a limited availability of multidomain interventions that target cognitive frailty. Thus, the aim of the present study was to develop and evaluate the content validity and acceptance of the multidomain intervention module to reverse cognitive frailty among older adults (iAGELESS).
Patients and Methods
This study was conducted in two phases: Phase I included the development of the multidomain intervention module iAGELESS and evaluation of content validity, while Phase II consisted of evaluating the acceptance of the module among 18 healthcare and social care providers, 13 older adults with cognitive frailty, and 13 caregivers. Content validity index (CVI) was used to quantify the content validity. Respondents completed a questionnaire which consisted of information on sociodemographic, followed by module acceptance evaluation with respect to content, terminologies, and graphics. The data was then analyzed descriptively.
Results
A multidomain intervention module, iAGELESS was developed. The module was found to have appropriate content validity (overall CVI = 0.83). All the caregivers, 92% of older adults with cognitive frailty and 83% of healthcare and social care providers were satisfied with the overall content of the module. More than 50% of those who accepted the module had satisfactory consensus on the ease of the terminologies, length of sentences, pictures, information, color, and font size included in the module.
Conclusion
The iAGELESS module demonstrated good content validity and was well accepted, thus warranting its utilization in future studies to determine its effectiveness in reversing cognitive frailty among older adults.
Introduction
The global older population is growing at a rapid pace, with older adults defined as persons aged 60 years and over. In 2020, there were 1 billion older adults worldwide, and this figure is expected to increase to 2.1 billion by 2050.Citation1 Similarly, it is anticipated that the number of older adults in Malaysia will rise to 5.8 million in 2030 from 2.3 million in 2020. With this, the demand for healthcare and expenses to manage older adults who are usually at a greater health risk will increase accordingly.Citation2 Both cognitive impairment and physical frailty are important indicators of the ageing process and linked to adverse health outcomes such as disability, hospitalization and death.Citation1,Citation2
Mild cognitive impairment (MCI) is defined as a period of transition between normal cognitive aging and dementia.Citation3 In Malaysia, the prevalence of MCI is reported to be 16%.Citation2 Physical frailty is defined as a clinical syndrome that involves having at least three of the following characteristics: unintentional loss of 5 kg weight, exhaustion, weakness, slowness, and low physical activity level.Citation1 In the Malaysian community dwelling older population, the prevalence of frailty was reported to be 8.9%.Citation4 Cognitive frailty (CF) is defined as a heterogeneous clinical manifestation characterized by the simultaneous presence of physical frailty and cognitive impairment.Citation5 Prevalence of cognitive frailty among the Malaysian community dwelling older population was reported at 2.2%. Several risk factors for CF have been established which include increased age, low niacin intake, lack of social support, depression, and lower functional status. Additionally, CF is associated with increased risk of dementia, disability and mortality.Citation6
Preventive intervention strategies for physical frailty, MCI and CF are important for the prevention of physical impairments, disabilities and dementia in older adults.Citation5 Previous reviews by Toman et alCitation7 and Hafdi et alCitation8 suggested that multidomain interventions (diet, physical exercise, cognitive training, social activities, and vascular risk management) might be beneficial in maintaining cognitive health. Another recent systematic review also reported that multidomain interventions focusing on cognitive training, dietary improvement, and physical activity could help prevent cognitive decline among older adults, including those at risk of developing dementia.Citation9 Dedeyne et alCitation10 found that multidomain interventions (diet and physical exercise) were more effective than monodomain interventions at improving frailty status and physical functioning.
Furthermore, in a feasibility study, it has been demonstrated that there is potential to reverse CF with multidomain intervention (physical, cognitive, nutritional, and psychosocial) among older adults from lower socioeconomic background.Citation11 A multidomain approach comprised nutritional (a daily dose of Fortisip Multi Fibre, iron, folate, vitamin B6, vitamin B12, calcium, and vitamin D supplements over 24 weeks), physical training (twice a week for resistance and balance exercises) and cognitive interventions (2 hours per week for cognitive-enhancing activities),Citation12 as well as additional modalities, namely social stimulation (group meetings) and monitoring metabolic and vascular risk factors (which include 3 nurse visits and 3 physician visits)Citation13 demonstrated an improved cognition and reduced frailty. The primary outcomes for these studies were frailty scoreCitation12 and changes in cognition.Citation13 Both studies emphasized the need to incorporate several domains of interventions, such as diet, exercise, cognitive training, social stimulation, and vascular risk monitoring, rather than a singular intervention for the most effective results. However, in these studies, the assessment of the effectiveness of the multidomain intervention was conducted either among older adults with frailty or those at increased risk of cognitive decline but not among individuals experiencing both conditions simultaneously. Additionally, some multidomain interventions missed either psychosocial or vascular risk management components,Citation12 resulting in a less holistic approach. Furthermore, multidomain intervention for older adults with CF is limited to a feasibility study and focuses solely on older adults from lower socioeconomic backgrounds.Citation11 Thus, we designed a study to determine the effectiveness of an all-inclusive multidomain intervention module (nutrition, psychosocial, physical activity, cognitive training, and vascular risk management) in older adults with cognitive frailty.Citation14 It is noted that most intervention studies did not report the development process of the intervention module. Thus, the aim of this article is to report the development and evaluation of the content validity and acceptance of the module.
Materials and Methods
Study Design
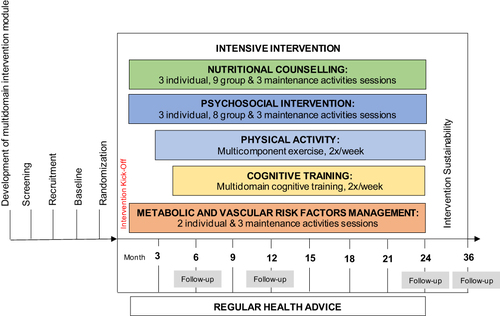
The study was conducted from October 2020 until December 2021 and consisted of two phases. In Phase I, a multidomain intervention module was developed, covering areas such as nutrition, psychosocial, physical activity, cognitive training, and vascular risk management, alongside an evaluation of the content validity. Phase II involved the evaluation of acceptance. The multidomain intervention module was designed and adapted based on the Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability (FINGER) trial protocolCitation15 (). The study was conducted under the Declaration of Helsinki.
Figure 1 Multidomain intervention module (iAGELESS) timeframe.
Phase I: Part 1: Development of Multidomain Intervention Module
Nutrition Intervention Module
To develop this component, a thorough literature review on recommendations for optimal dietary nutrient intake in older adultsCitation16–18 was conducted. The gathered data were extensively reviewed to develop the content based on the suitability of dietary habits of Malaysian older adults. Food photos were taken, and a professional artist was hired to design illustrations to be included in the module. The content of the nutrition intervention module was finalized through a series of meetings, with the research members consisting of dietitians and nutritionists.
Psychosocial Intervention Module
A comprehensive review of available literature and international guidelines for psychosocial education packagesCitation19 was conducted, followed by its adaptation to develop a psychosocial intervention module. The module was designed using a transtheoretical model to promote positive behavioral changes among participants. The information gathered was extensively reviewed through face-to-face or online meetings with a panel of three psychologists to develop the content of the package based on local contexts.
Physical Activity Intervention Module
The development of the physical activity intervention module involved a literature review on multidomain interventions for the potential reversal of MCI and frailty which was performed for the WE-RISE trial (Warga Emas-Resilient mInd and muScle Exercise).Citation20 The WE-RISE module was adapted and updated for the iAGELESS module to be performed to suit for a longer duration of implementation. This module was then reviewed through a series of face-to-face/online meetings, with content experts comprising physiotherapists, geriatricians, and an exercise physiologist to finalize the contents and graphics of the current module.
Cognitive Training Intervention Module
Similarly, iAGELESS cognitive training intervention module was developed as the physical activity module. This module was reviewed by the research team led by a clinical psychologist.
Metabolic and Vascular Risk Factors Management Intervention Module
Metabolic and vascular risk factors management intervention module was developed based on the national evidence-based guidelines.Citation21 The contents of the module were finalized through a series of meetings, with the research team members consisting of geriatricians.
Phase I: Part 2: Evaluation of Content Validity
The purposive sampling method was employed to recruit participants for content validity evaluation. Sample size calculation was determined according to Lynn (1986)Citation22 with at least three individuals required for content validation of each component. Regarding the healthcare experts included in the study, the subjects were chosen from diverse interdisciplinary areas comprising four physicians (two geriatricians and two family health physicians), three academicians in medicine, geriatric medicine and dietetic and six healthcare professionals (two clinical psychologists, two physiotherapists, and one nutritionist and dietician, respectively). The inclusion criteria of the expert panels included those involved in research focusing on nutrition, psychosociology, vascular health, physical activity, cognition, and wellness.
The validation tool was adapted from Clayton’s (2009) proposed questionnaire, the Tool to Evaluate Materials Used in Patient Education (TEMPtED).Citation23 The multidomain intervention module was evaluated based on five criteria: content, motivational principal, literature, arrangement and typography, and graphic.Citation23 Content validity index (CVI) is most often used for content validity determination, and in this study, expert panels were invited to examine each item and rate it on a scale of 1 to 4 (with 1 being “not relevant”, 2 being “some revision required”, 3 being “relevant but needs minor revision”, and 4 being “extremely relevant”).Citation22 The number of expert panels rating an item as relevant (with a rating of 3 or 4) was calculated by dividing it by the total number of expert panels to produce the CVI for relevancy of each item. An index of 0.80 or above for each item was considered acceptable.Citation24 The expert panels were given 2 weeks to review the module followed by video conferencing for roundtable discussion.
Phase II: Acceptance Test
The evaluation of acceptance was carried out using purposive sampling. The sample size was calculated using OpenEpi Software Version 3.01 with hypothesized 2.2% prevalence of cognitive frailtyCitation6 at 95% confidence level. Thus, the total sample size suggested was 34. After considering 10% dropout, the total sample size needed was 38 subjects. A total of 44 subjects participated in the acceptance test that consisted of 18 healthcare and social care providers, 13 older adults with cognitive frailty, and 13 caregivers.
Inclusion criteria for healthcare and social care providers included those involved in the health care of older adults at hospitals, health clinics and senior citizen centers for the past 6 months. The inclusion criteria for older adults with cognitive frailty were individuals aged 60 to 80 years, community dwellers from the Klang Valley, Malaysia, and meet the following criterion; ie, Mini-Mental State Examination (MMSE) score ≥19 and <26 points, Clinical Dementia Rating Scale (CDR) = 0.5 and fulfilled at least three of Fried’s frailty criteria.Citation14 The selection criteria for caregivers included those who were living or meeting with cognitive frailty, older adults at least once daily and were responsible for managing their food and drink, clothing or shelter. Informal caregivers such as spouses, children, son-in-law, grandsons, close friends and neighbors were also included in the study.
The questionnaire used for this study was adapted from Vanoh et al (2018)Citation18 which comprised of questions regarding participants’ sociodemographic information and assessed the module’s acceptability in terms of its content, terminologies, length of sentences, pictures, information, color, font size and elements that required improvement. The evaluation of acceptance was administered through virtual sessions. Data were analyzed descriptively using SPSS version 21.0.
Results
Multidomain Intervention Module
Based on the extensive literature review and FINGER trial protocol, the multidomain intervention module comprised five components, namely nutrition, psychosocial, exercise, cognitive training, and metabolic and vascular risk factors management. The module was prepared in the form of PowerPoint slides accompanied by a manual book, both produced in the Malay language. The module utilized Arial font with of size of font ranging from 30 to 40 points for title of content and 20–25 points for content, and the font color was set to black over a white background. The topics, activities, learning time and mode of delivery of multidomain intervention module are summarized in .
Table 1 Topics, Activities, Learning Time and Mode of Delivery of the Multidomain Intervention Module
Nutrition Intervention Module
The nutrition intervention module contained 12 series that included three individual nutritional counseling sessions, nine group sessions and three maintenance activity sessions conducted within 30 to 60 minutes over a period of 24 months. Individualized nutritional counseling consisted of personalization of the participant’s diet and their compliance to the sessions through assessments and monitoring (). Meanwhile, group counseling sessions consisted of talks on various topics such as the Malaysian Healthy Plate, fasting, the importance of nutrient intake on the brain and muscles, menu planning, food safety, and how to read nutritional information. Each session included interactive activities such as online games, video presentations, gardening sessions, and cooking demonstrations. Health maintenance of similar activities as additional sessions was scheduled for month 16th, 20th and 24th.
Figure 2 Personalization of the participant’s diet with clinical dietician.

Psychosocial Intervention Module
The psychosocial intervention module comprised 11 series, consisting of both individual and group sessions. Individual sessions included an evaluation of motivational level of the participants, and counseling session using the Stages of Change model (). Meanwhile, group sessions included multiple psychosocial dimensions such as social support, resilience, self-efficacy, and coping strategies that were conducted through various methods: sharing session, kindergarten visit, talks from professionals, as well as games and reward sessions to support and maintain new healthy behavior. Three health maintenance activities are recommended to be given after one year of intervention that consist of talks, games, and potluck.
Figure 3 Individual counseling session using the Stages of Change model with clinical psychologist.

Physical Activity Intervention Module
The physical activity intervention module consisted of five components, namely warm-up, aerobic, strengthening, postural balance, and cooling exercise (). It is recommended for the intervention to be performed two to three times per week over a period of 21 weeks. Three health maintenance activity sessions consisting of multicomponent exercise sessions and talks on the importance of physical activity are suggested for implementation.
Figure 4 Multicomponent exercise session with physiotherapist.

Cognitive Training Intervention Module
The cognitive training intervention module comprised 16 series of both individual and group sessions. These sessions should be carried out two to three times a week over a period of 20 months. Cognitive exercises included activities such as crossword puzzles, memory games, word search, maze, and spot the differences (). Three booster sessions are to be administered which include cognitive exercises and a talk on cognitive health.
Figure 5 Cognitive training games such as maze and spot the differences.

Metabolic and Vascular Risk Factors Management Intervention Module
The metabolic and vascular risk factors management intervention module comprised two series of individual counseling with a physician (). These sessions were aimed to identify the need for initiation or modification of medication, physical activity status and other necessary recommendations for the participants. Medication compliance and body weight were also assessed and monitored. A booster dose was delivered which included a healthy lifestyle talk with reading materials provided.
Figure 6 Individual counseling with physician.

Content Validity by Expert Panels
The average mean age of the expert panels was 48.0 ± 8.4 years, comprising physicians (30.8%, n = 4) and academicians (23.1%, n = 3) and healthcare professionals (46.2%, n = 6) (). As shown in , all components were subjected to good content validity. The CVI values were 0.82, 0.83, 0.80, 0.86, 0.83 and 0.83 for nutrition, psychosocial, exercise, cognitive, vascular and multidomain intervention module, respectively. In terms of graphics, layout and typography for the multidomain intervention module, the CVI were 1.00 and 0.90, respectively. Other categories of evaluation such as content, motivating principles and literacy showed positive feedback from the expert panel members.
Table 2 Sociodemographic Characteristics of Expert Panels for Content Validity [Presented as Mean ± SD or n (%)]
Table 3 Content Validity Index for the Multidomain Intervention Module by Expert Panel Members
Acceptance by Health and Social Care Providers, Older Adults with Cognitive Frailty and Caregivers
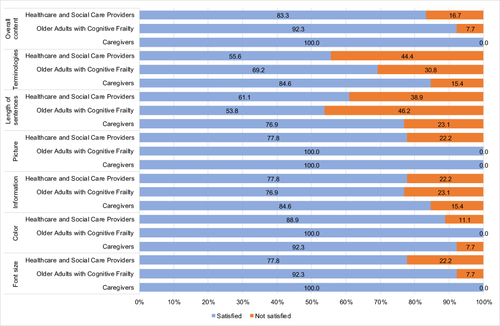
As shown in , the average mean age of health and social care providers, older adults with CF and caregivers were 39.3 ± 10.5, 66.0 ± 4.7 and 52.0 ± 17.8 years, respectively. Most of the health and social care providers (83.3%, n = 15) had tertiary education. Most of the older adults with CF (53.8%, n = 7) and caregivers (61.5%, n = 8) had secondary education. All the caregivers, 92% (n = 12) of older adults with CF and 83% (n = 15) of health and social care providers were satisfied with the overall content of the multidomain intervention module. A total of 55.6% (n = 10) of health and social care providers were satisfied with the terminologies used in the module in comparison to 69.2% (n = 9) of older people and 84.6% (n = 11) of the caregivers. Overall, 76.9% (n = 10) of the caregivers approved the length of sentences included in the module. All the caregivers were satisfied with the font size used in the module; however, 7.7% (n = 1) of the older adults with CF had expressed their disapproval. Majority of the older adults with CF and caregivers who participated in this study approved the pictures incorporated in the module ().
Table 4 Sociodemographic Characteristics of Health and Social Care Providers, Older Adults with Cognitive Frailty and Caregivers for Acceptance Evaluation [Presented as Mean ± SD or n (%)]
Figure 7 Satisfaction with the multidomain intervention module by health and social care providers, older adults with cognitive frailty and caregivers.
Discussion
In the present study, we successfully developed a validated multidomain intervention module for the reversal of cognitive frailty among older adults. The module was also well accepted. Due to the COVID-19 pandemic, the intervention was administered using a hybrid approach whereby both face-to-face and online sessions were employed. Face-to-face counseling was conducted to address the specific needs of older adults in individual and personalized nutrition, psychosocial support, exercise and cardiovascular health. Personalized nutrition through face-to-face dietary counseling nutrition interventions has been found to be effective in facilitating dietary changes.Citation25 Meanwhile, interactive methods such as online games, video presentation, gardening, cooking demonstrations, and visit to a kindergarten were utilized to conduct group sessions. Interactive cognitive-motor interventions have been found to improve physical and cognitive fall risk factors in older people.Citation26 The module was also equipped with photos to facilitate the participants in understanding health messages as this approach has been reported to be effective.Citation27 Health maintenance activities were incorporated to reinforce the health messages delivered, hence necessitating the repetition of information for optimal learning in older adults.Citation28
The determination of relevance and quality of an educational material is crucial.Citation29 The overall CVI for the current multidomain intervention module was 0.83, thus, indicating good content validity. The same approach was used in another study to validate educational materials by using CVI.Citation24 However, content validation of this module required some corrections, including revisions to the content, language, and activity examples. After discussions with the expert panels in this study, we had improved the content of the module, rephrased medical jargon with layman’s terms and incorporated more activities that were more relatable to real life. The contents that had been improved were “maintain body weight and muscle strength”, “social activities” such as organizing a trip and potluck session with the participants and “benefits of exercise”. The process of adapting educational materials to the suggestions and evaluation of experts is an essential step to ensure that the module is more scientifically rigorous and effective for health education activities.Citation29 Besides that, more activities related to real life were incorporated in the module such as cooking, gardening, potluck, problem-solving, multitasking, chair-based activities and obstacle walking. Activities such as cooking, exercise, and problem solving related to real life have been shown to be suitable tools in educating older people about lifestyle modification strategies that can slow down cognitive impairment.Citation30
In view of the evaluation of acceptance of the content module, majority of health and social care providers, older adults with CF, and caregivers in this study expressed overall satisfaction. Similar findings were reported in our team’s earlier study.Citation18 The acceptance test enables the targeted population to provide their input.Citation31 This step assists in the improvement of educational materials that can accommodate their needs. In this study, the participants suggested maximizing font size, using simpler words, and incorporating more visuals to replace words. Furthermore, in response to participants’ input, the initial font size 10 of the module content was increased to size 20. Previous studies have highlighted the preference of older adults for larger font sizes in educational materials and M-HealthCitation32 due to the high prevalence of eyesight problems. In terms of the language used, the module initially contained scientific terms, which were subsequently replaced with simpler and accessible terms. Furthermore, suggestions by participants to incorporate more pictures aligned with the findings of previous studies,Citation33 which reported that the use of pictures can increase attention and recall of health-related educational content.
The strength of this study is the appropriate process to develop the intervention module.Citation34 Nevertheless, this study has a few limitations, including the potential lack of representativeness of the samples with participants consisting of older adults and caregivers from the Klang Valley area. Their perspectives may not represent the views of older adults from other regions in Malaysia. The multidomain intervention module was developed in one language, ie, Malay which is the national language. Thus, future study should consider translating it to other languages such as English and Mandarin to increase its outreach among other ethnic groups in Malaysia.
Conclusion
In conclusion, the contents of the newly developed multidomain intervention were successfully validated among healthcare experts and well accepted by all the older adults with cognitive frailty, and caregivers, particularly for picture and color used in the module. The multidomain intervention module is ready to be tested for its effectiveness. With further testing, this comprehensive module has the potential to be used as a tool kit in efforts to prevent cognitive frailty among older adults, particularly from those in low middle income countries.
Abbreviations
CDR, Clinical Dementia Rating Scale; CF, Cognitive Frailty; CVI, Content Validity Index; FINGER, Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability; iAGELESS, Multidomain Intervention Module to Reverse Cognitive Frailty Among Older Adults; MCI, Mild cognitive impairment; MMSE, Mini-Mental State Examination; TEMPtED, Tool to Evaluate Materials Used in Patient Education; WE-RISE, Warga Emas-Resilient mInd and muScle Exercise.
Ethics Approval and Informed Consent
The study was reviewed and approved by Research Ethics Committee of Universiti Kebangsaan Malaysia (UKM PPI/111/8/JEP-2020-347). The participants provided their written informed consent to participate in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest in this work.
Acknowledgments
The authors would like to acknowledge and thank the participation of subjects, healthcare and social care providers, caregivers, and experts in health promotion. We are also grateful to the local authorities for their cooperation, time, and effort. The MMSE is reproduced by special permission of the Publisher, Psychological Assessment Resources, Inc., 16204 North Florida Avenue, Lutz, Florida 33549, from the Mini Mental State Examination, by Marshal Folstein and Susan Folstein, Copyright 1975, 1998, 2001 by Mini Mental LLC, Inc. Published 2001 by Psychological Assessment Resources, Inc. Further reproduction is prohibited without permission of PAR, Inc. The MMSE can be purchased from PAR, Inc. by calling (800) 331-8378 or (813) 968-3003.
Data Sharing Statement
Data available on request from the authors.
Additional information
Funding
References
- Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. Journals Gerontol - Ser a Biol Sci Med Sci. 2001;56(3):146–157. doi:10.1093/gerona/56.3.m146
- Vanoh D, Shahar S, Din NC, et al. Predictors of poor cognitive status among older Malaysian adults: baseline findings from the LRGS TUA cohort study. Aging Clin Exp Res. 2017;29(2):173–182. doi:10.1007/s40520-016-0553-2
- Olazarán J, Torrero P, Cruz I, et al. Mild cognitive impairment and dementia in primary care: the value of medical history. Fam Pract. 2011;28(4):385–392. doi:10.1093/fampra/cmr005
- Badrasawi M, Shahar S, Kaur Ajit Singh D. Risk factors of frailty among multi-ethnic Malaysian older adults. Int J Gerontol. 2017;11(3):154–160. doi:10.1016/j.ijge.2016.07.006
- Kelaiditi E, Cesari M, Canevelli M, et al. Cognitive frailty: rational and definition from an (I.A.N.A./I.A.G.G.) International Consensus Group. J Nutr Health Aging. 2013;17(9):726–734. doi:10.1007/s12603-013-0367-2
- Rivan NFM, Shahar S, Rajab NF, et al. Cognitive frailty among Malaysian older adults: baseline findings from the LRGS TUA cohort study. Clin Interv Aging. 2019;14:1343–1352. doi:10.2147/CIA.S211027
- Toman J, Klímová B, Vališ M. Multidomain lifestyle intervention strategies for the delay of cognitive impairment in healthy aging. Nutrients. 2018;10(10):1–10. doi:10.3390/nu10101560
- Hafdi M, Hoevenaar-Blom MP, Richard E. Multi-domain interventions for the prevention of dementia and cognitive decline. Cochrane Database Syst Rev. 2021;2021(11). doi:10.1002/14651858.CD013572.pub2
- Castro CB, Costa LM, Dias CB, et al. Multi-domain interventions for dementia prevention–a systematic review. J Nutr Heal Aging. 2023;27(12):1271–1280. doi:10.1007/s12603-023-2046-2
- Dedeyne L, Deschodt M, Verschueren S, Tournoy J, Gielen E. Effects of multi-domain interventions in (pre)frail elderly on frailty, functional, and cognitive status: a systematic review. Clin Interv Aging. 2017;12:873–896. doi:10.2147/CIA.S130794
- Murukesu RR, Shahar S, Subramaniam P, Rasdi HFM, Nur AM, Singh DKA. The WE-RISE TM multidomain intervention: a feasibility study for the potential reversal of cognitive frailty in Malaysian older persons from lower socioeconomic status (pre-print). Res Sq. 2023:1–37. doi:10.21203/rs.3.rs-3134012/v1.
- Ng TP, Feng L, Nyunt MSZ, et al. Nutritional, physical, cognitive, and combination interventions and frailty reversal among older adults: a randomized controlled trial. Am J Med. 2015;128(11):1225–1236.e1. doi:10.1016/j.amjmed.2015.06.017
- Ngandu T, Lehtisalo J, Solomon A, et al. A 2 year multidomain intervention of diet, exercise, cognitive training, and vascular risk monitoring versus. A 2 year multidomain intervention of diet, exercise, cognitive training, and vascular risk monitoring versus control to prevent cognitive. Lancet. 2015:15(July):1–9. doi: 10.1016/S0140-6736(15)60461-5.
- Ponvel P, Shahar S, Kaur D, Singh A, Fitri A, Ludin M. Multidomain Intervention for Reversal of Cognitive Frailty, Towards a Personalized Approach (AGELESS Trial. Study Design. 2021;82:673–687. doi:10.3233/JAD-201607
- Kivipelto M, Solomon A, Ahtiluoto S, et al. The Finnish geriatric intervention study to prevent cognitive impairment and disability (FINGER): study design and progress. Alzheimer’s Dement. 2013;9(6):657–665. doi:10.1016/j.jalz.2012.09.012
- Ministry of Health Malaysia. Malaysian Dietary Guidelines 2010. Putrajaya: Ministry of Health; 2018.
- National Coordinating Committee on Food and Nutrition (NCCFN). Recommended Nutrient Intakes for Malaysia. Putrajaya: Ministry of Health; 2017.
- Vanoh D, Ishak IH, Shahar S, Manaf ZA, Ali NM, Noah SAM. Development and assessment of a web-based intervention for educating older people on strategies promoting healthy cognition. Clin Interv Aging. 2018;13:1787–1798. doi:10.2147/CIA.S157324
- Substance Abuse and Mental Health Services Administration (SAMHSA). Enhancing Motivation for Change in Substance Use Disorder Treatment. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2019.
- Murukesu RR, Kaur D, Singh A, Shahar S. A multi-domain intervention protocol for the potential reversal of cognitive frailty: ” WE-RISE “. Randomized Controlled Trial. 2020;8(September):1–11. doi:10.3389/fpubh.2020.00471
- Ministry of Health Malaysia. Clinical Practice Guidelines on Primary & Secondary Prevention of Cardiovascular Disease. Putrajaya:Kementerian Kesihatan Malaysia. Available from: https://www.moh.gov.my/moh/resources/Penerbitan/CPG/CARDIOVASCULAR/3.pdf. Accessed July 4, 2022.
- LYNN MR; Lynn. Determination and quantification of content validity. Nurs Res. 1986;35(6):382–386. doi:10.1097/00006199-198611000-00017
- Clayton LH. TEMPtEd: development and psychometric properties of a tool to evaluate material used in patient education. J Adv Nurs. 2009;65(10):2229–2238. doi:10.1111/j.1365-2648.2009.05049.x
- Lau XC, Wong YL, Wong JE, et al. Development and validation of a physical activity educational module for overweight and obese adolescents: CERGAS programme. Int J Environ Res Public Health. 2019;16(9):1–16. doi:10.3390/ijerph16091506
- Al-Awadhi B, Fallaize R, Zenun Franco R, Hwang F, Lovegrove JA. Insights Into the Delivery of Personalized Nutrition: evidence From Face-To-Face and Web-Based Dietary Interventions. Front Nutr. 2021;7(January):1–10. doi:10.3389/fnut.2020.570531
- Schoene D, Valenzuela T, Lord SR, De Bruin ED. The effect of interactive cognitive-motor training in reducing fall risk in older people: a systematic review. BMC Geriatr. 2014;14(1). doi:10.1186/1471-2318-14-107
- Shahar S, Nur S, Adznam A, et al. Development and analysis of acceptance of a nutrition education package among a rural elderly population: an action research study. BMC Geriatr. 2012;12(24):1–9. doi:10.1186/1471-2318-12-24
- Lauridsen B. Health education for the elderly. Can Nurse. 1989;85(11):16–18. doi:10.5772/33472
- Denise A. Focus on research methods is the CVI an acceptable indicator of content validity? appraisal and recommendations. Res Nurs Health. 2007;30(459–467):488–495. doi:10.1002/nur
- Vanoh D, Shahar S, Rosdinom R, Din NC, Yahya HM, Omar A. Development of TUA-WELLNESS screening tool for screening risk of mild cognitive impairment among community-dwelling older adults. Clin Interv Aging. 2016;11:579–587. doi:10.2147/CIA.S102925
- de Oliveira SC, de Oliveira Lopes MV, Fernandes AFC, Oliveira SCD, Lopes AFC. Development and validation of an educational booklet for healthy eating during pregnancy. Rev Lat Am Enfermagem. 2014;22(4):611–620. doi:10.1590/0104-1169.3313.2459
- Singh DKA, Goh JW, Shaharudin MISS. A mobile app (FallSA) to identify fall risk among Malaysian community-dwelling older persons: development and validation study. 2021;9(10). doi:10.2196/23663
- Houts PS, Doak CC, Doak LG, Loscalzo MJ. The role of pictures in improving health communication: a review of research on attention, comprehension, recall, and adherence. Patient Educ Couns. 2006;61(2):173–190. doi:10.1016/j.pec.2005.05.004
- Robert Maribe Branch.Instructional Design: The ADDIE Approach.New York: Springer.2009.