Abstract
Background
Heart failure (HF) has become an increasingly significant public health problem, associated with repeated hospitalizations, high costs, low quality of life, and decreased survival rate. The progress of the disease may be slowed if treatment is administered in accordance with current guidelines.
Objectives
To compare the clinical profile of HF patients in a Romanian general hospital over a 3-year period.
Methods and results
We studied two cohorts of patients admitted in the cardiology department of a rehabilitation hospital with a diagnosis of chronic HF New York Heart Association class II–IV The first, in 2006, included 415 patients, 67.08 ± 10.59 years; the second, in 2009, included 500 patients, 67.31 ± 11.27 years. Considering all patients, the left ventricle ejection fraction (LVEF) was not statistically different in the two cohorts. Compared to the 2006 cohort, the 2009 female cohort had higher LVEF (60.49% ± 13.41% vs 64.42% ± 13.79%, P < 0.05), while males over 65 years of age had lower LVEF (52.75% ± 15.02% vs 54.37% ± 15.23%, P = NS). For females, the probability of having LVEF <45% was higher in 2006 (odds ratio = 1.573). HF with preserved LVEF was more common in females, both in 2006 (78.2% vs 54.2%) and 2009 (87.2% vs 57.3%). In the 2009 cohort, LVEF was higher both in young patients (59.08% ± 14.22% vs 55.35% ± 14.92%) and patients ≥ than 75 years of age (62.28% ± 13.81% vs 56.79% ± 14.81%) compared to the 2006 cohort. Ischemic heart disease was the main underlying cause for HF in both cohorts.
Conclusion
HF appeared to have the same clinical profile over a 3-year period. Females diagnosed with HF showed higher rates of preserved LVEF.
Keywords:
Introduction
The guidelines for the diagnosis and treatment of acute and chronic heart failure (HF) published by the European Society of Cardiology in 2008 mention a number of changes in the recommendations for diagnosis and treatment of HF, in both conventional and interventional therapyCitation1
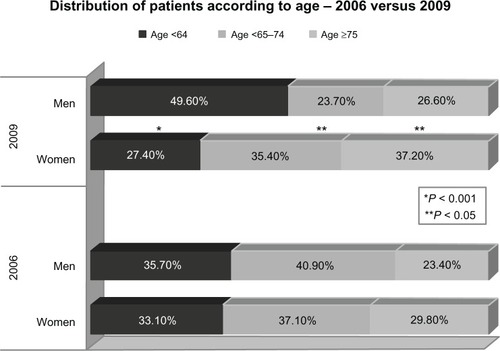
Figure 1 Distribution of patients according to age – 2006 vs 2009.
Besides HF symptoms and typical signs, the definition of HF comprises a functional or structural abnormality supported by reported cardiac murmurs, the third heart sound in objective examinations, cardiomegaly or other echocardiographic abnormalities, as well as increased plasmatic values of the natriuretic peptides. There is no left ventricle ejection fraction (LVEF) cut-off value for HF diagnosis, but LVEF does play an important role in the prognosis of HF.
In UK, HF is the cause of 5% of emergency hospitalizations, occurs in 10% of hospitalized patients and accounts for ~2% of the national health expenditure, mostly due to the costs of inpatient management.Citation2 There is substantial underreporting of HF occurrence, which is considered to be due to clinician preference for reporting other etiological diagnoses (eg, aortic stenosis) or the diagnosis of a major comorbidity (eg, diabetes), but not HF per se.
The objective of this study was to compare the clinical profile of HF patients over a 3-year period in a Romanian general hospital.
Methods
The study was retrospective and observational and took into consideration two cohorts admitted in the cardiology department of the Rehabilitation Hospital with a diagnosis of chronic HF New York Heart Association (NYHA) functional class II–IV. The first cohort (2006) included 415 patients, 67 ± 10.59 years, of whom 43.1% were female. The second (2009) included 500 patients, 67.31 ± 11.27 years, 45.2% being female.
Data were collected from patients’ charts and discharge records. HF was defined on the basis of the recommendations made by the guidelines for the diagnosis and treatment of HF published by the European Society for Cardiology in 2005 (symptoms, objective evidence of cardiac dysfunction detected by echocardiography, and response to treatment directed towards HF),Citation3 and 2008 (symptoms and signs typical of HF and objective evidence of a structural or functional abnormality of the heart at rest, eg, cardiomegaly, third heart sound, cardiac murmurs, abnormality on the echocardiogram, raised natriuretic peptide concentration, etc),Citation1 respectively. As far as HF etiology is concerned, patients were divided into ischemic and nonischemic (other etiologies). In most patients, ischemia was diagnosed only on the basis of typical electrocardiographic alterations.
Statistical analysis was carried out using SPSS for Windows (v 16.0; IBM Corporation, Armonk, NY, USA) and MedCalc (v 10.3.0.0; MedCalc Software, Ostend, Belgium) software programs. The analysis of the differences between qualitative variables was performed by using the χ2 test. The Kolmogorov–Smirnov test was used to check the normal distribution of continuous numerical variables. Mean differences among continuous qualitative variables were evaluated with the Student’s t-test (unpaired and paired), while nonparametric tests (Mann–Whitney U) were used to assess distribution variables that did not comply with normal conditions. A value of P < 0.05 was deemed statistically significant.
Results
In 2009, the number of HF patient admissions (500 patients) was much higher compared to 2006 (415 patients).
There was no significant difference between the mean ages of the patients included in the study when considering both sexes; however, the females admitted with a diagnosis of HF in 2009 were significantly older than those admitted in 2006 (P < 0.05). The LVEF mean value in all patients included in the study did not differ significantly in the two different years. The female patients admitted in 2009 with a diagnosis of HF had a significantly higher mean LVEF compared to those admitted in 2006. Odds ratio (OR) for LVEF <45% was higher in 2006 for women (OR = 1.573, 95% confidence interval [CI]: 0.946–2.617).
The comparative features of the patients in the two different years are presented in .
Table 1 Comparative features of patients investigated in 2006 and 2009
Most patients were classed as NYHA III, with no statistically significant differences between the NYHA classes in the two years. There were more females diagnosed with HF NYHA class IV in 2009 (22.10%) than in 2006 (14%) (P = 0.05). As for NYHA II and NYHA III functional classes, there was no significant difference between the two years. There were no differences in terms of NYHA class among the male patients.
When considering the patients’ age distribution in the two years, the proportion of females over 75 years of age increased, while the number of those less than 64 years decreased. The number of male patients younger than 64 years of age diagnosed with HF increased. These results are shown in .
Table 2 Age-group distribution of patients according to sex
When comparing the two types of HF (systolic and diastolic), the occurrence of HF with preserved ejection fraction (>45%) was higher in both years: 64.5% in 2006 and 69.8% in 2009.
HF with preserved ejection fraction was much more often diagnosed in females than in males, ratios were higher in.2009 than in 2006. Although the difference between the two years was not statistically significant (P = 0.09), the risk of LVEF <45% in females was higher in 2006 (OR = 1.573, 95% CI: 0.94–2.61). The findings were also valid for males yet the difference between patients with LVEF <45% and those with LVEF ≥45%, was not that obvious (see ).
Table 3 Chronic heart failure type according to sex
The comparative analysis of LVEF mean values by patient age revealed that, in 2009, the mean LVEF was higher in patients between 65–74 and ≥75 in comparison with <64 years, Furthermore, in 2009, mean LVEF values increased markedly with age, but, in 2006, we found no significant statistical difference by analysis of variance (ANOVA) testing in mean LVEF values according to patient age ().
Table 4 Mean LVEF values according to age group
summarizes the mean age of females versus males with preserved/nonpreserved LVEF in 2006 and 2009. In 2006, no significant differences were found between mean age in preserved versus nonpreserved LVEF cases for females, but the difference was almost statistically significant in 2009 (P = 0.09; 70.49 ± 9.66 vs 66.65 ± 11.12 years). No significant mean age difference was found among male patients in 2006, but the same difference was found in 2009 (63.06 ± 12.41 years for those with LVEF <45 vs 66.75 ± 11.19 years for ejection fraction ≥45%, P = 0.011).
Table 5 Comparative mean age of patients with low LVEF vs preserved LVEF, in 2006 vs 2009
No significant differences were found in 2006 versus 2009 regarding the left ventricle telediastolic volume (56.73 ± 12.79 mL vs 56.28 ± 14.02 mL, P = nonsignificant [NS]) and left ventricle telesystolic volume (LVTSV 42.06 ± 14.15 mL vs 41.03 ± 14.71 mL, P = NS). A significant difference was found in the left atrium’s diameter (47.43 ± 12.5 mm in 2006 vs 45.34 ± 13.81 mm in 2009, P = 0.018).
We deemed left ventricle dysfunction to be severe if the ejection fraction was less than 30%, moderate if the ejection fraction ranged between 30% and 40%, and discrete if the ejection fraction was higher than 40%.
In 2006, among the patients with systolic dysfunction, 45.6% suffered from discrete dysfunction, 46.9% from moderate dysfunction, and 7.5% from severe dysfunction. In 2006, discrete dysfunction was more often registered in females (61.5% vs 39.8%, P = 0.038), while moderate and severe dysfunction prevailed in men (moderate: 35.9% females vs 50.9% males, P = NS; severe: 2.6% females vs 9.3% males, P = NS). In 2009, 52.3% of the patients were found to suffer from discrete dysfunction, 37.7% from moderate dysfunction, and 9.9% from severe dysfunction. No significant differences were recorded between sexes regarding the percentage of patients with discrete (55.9% females vs 51.3% males, P = NS), moderate (38.2% females vs 37.6% males, P = NS), or severe dysfunction (5.9% females vs 11.1% males, P = NS).
We should also emphasize the fact that there were a large number of patients with hypertension in both years. Of those investigated in 2006, 235 (56.6%) were diagnosed with hypertension; mean LVEF was 58.69% ± 16.52%. Understandably, 73.2% of these patients had LVEF ≥45%. The distribution of the hypertension (HTA) patients according to NYHA class was as follows: NYHA II: 10.6%; NYHA III: 71.9%; and IV: 17.4%. In 2009, 57.8% (289 patients) were diagnosed with HTA: NYHA II: 8.7%; NYHA III: 72.7%; and NYHA IV: 18.7%. The mean LVFE in HTA patients was 64.01% ± 16.22%; 18.7% (54) of these had LVFE <45%, and 81.3% had preserved LVFE.
We found significant differences between the two years regarding the percentage of hypertensive patients with ejection fraction over 45% (73.2% in 2006 vs 81.3% in 2009, P = 0.03).
There were no statistically significant differences between the two time intervals regarding either the prevalence of diabetes mellitus (27.9% vs 31 %) or levels of creatinine (1.04 vs 1.09 mg/dL) and serum urea (45 vs 51 mg/dL).
At the same time, no statistically significant differences between the two years were noted regarding the ischemic etiology of the HF, ischemic etiology representing the main underlying cause of HF. In 2006, congestive heart failure etiology was ischemic in 330 patients (79.5%) and nonischemic in 85 patients (20.48%). In 2009, HF etiology was ischemic in 335 patients (70.6%) and nonischemic in 147 patients (29.4%).
Although no marked differences were registered in ischemic etiology between the two sexes (P = NS), it seemed that females were less affected by ischemia compared to males (OR = 0.448, 95% CI: 0.182–1.105 for 2006, and OR = 0.814, 95% CI: 0.398–1.666 for 2009).
In 2006, permanent atrial fibrillation was present in 209 patients (50.4%), being 92 (44%) females and 117 (56%) males, while in 2009 it was found in 239 patients (47.8%), being 108 (45.1%) females and 131 (54.8%) males.
Seventy-two patients (17.39%) admitted in 2006 suffered from ventricular arrhythmias, at 99 patients (9.8%), the percentage was higher in 2009.
In 2006, 69 patients, namely 16.6% of the total number of patients included in the study, were diagnosed with chronic obstructive pulmonary disease (COPD), bronchial asthma, or chronic bronchitis. The occurrence of pulmonary pathology was diagnosed in only 44 (8.8%) of the patients with HF admitted in 2009.
Discussion
As mentioned above, HF incidence is continually increasing, most likely as a consequence of population aging and increase in the survival of patients after myocardial infarction. The Study group on HF Awareness and Perception in Europe (SHAPE) study revealed alarming facts about HF mortality: only 25% of men and 38% of women survive more than 5 years after diagnosis.Citation4
HF affects about 2% of the Western population, with incidence increasing from 1% in 40-year-old individuals to 10% of those over the age of 75 years.Citation5 Among the younger population, HF prevails in men, being secondary mainly to ischemic heart disease. The mean age of patients diagnosed with HF in the general population of developing countries is 75 years overall.Citation1 HF admissions increased three times over the past 3 decades,Citation6 due to population aging and improved treatment of other cardiac conditions that generally lead to HF.Citation7 The age of the 415 patients included in our study in 2006 ranged from 32 to 92 years, the mean age being 67.08 ± 10.59 years. In 2009, data were somewhat similar: the 500 patients were between 27 and 94 years, with a mean age of 67.31 ± 11.27. Females were generally older than males in both years. The females included in the 2009 study were statistically significantly older than those included in the 2006 study, data that were different from those reported by other studies.Citation5–Citation8 Furthermore, 61% of HF deaths occurred in females.Citation9,Citation10 Females with HF were more frequently hospitalized than males,Citation8,Citation9 and the number of hospitalization days was also higher among females.Citation9 Females were less often diagnosed with HF and were generally older than males.Citation8,Citation10–Citation12 A notable difference was represented by the prevalence and severity of characteristic symptoms, which were more severe in females. Most often, the symptoms described by female patients were atypical, and did not in fact correspond to standard HF.Citation8,Citation11
Ischemic heart disease is by far the most common cause of myocardial damage, being the initiating cause in ~70% of HF patients. According to the literature in the field, etiology is ischemic in most HF cases.Citation1,Citation13–Citation17 In our study, the occurrence of ischemic etiology was also more than 70% in both 2006 and 2009.
Females seem to be less affected by ischemia compared to males, most likely due to hormonal differences in the two sexes.
In this study, all patients were classed as NYHA classes II–IV, males and females in nearly equal proportions, the great majority being classified as NYHA class III. In USA, HF represents a major public health problem affecting >5 million Americans, with an estimated 250,000 belonging to NYHA functional class IV.Citation5 More men than women belonged to NYHA class II in our study, while NYHA class IV comprised more females. The data were at variance with those presented by Baumhakel et al in 2009, who did not report any differences between the two sexes concerning NYHA classes.
As for diastolic HF or HF with preserved LVEF, the literature in the field suggests that it is present in approximately 50% of HF patients, being more frequent in females, the elderly, and patients diagnosed with diabetes mellitus and hypertension. The prognosis of diastolic HF is similar to that of systolic HF.Citation18,Citation19 The Euro Heart Failure survey reports an even higher mortality among patients with diastolic congestive heart failure.Citation20
The mean ejection fraction of the patients included in our study was over 45%. The incidence of this form of HF was very high in both years: 64.5% in 2006 and 69.8% in 2009. The reported incidence of preserved LVEF among patients with HF varied widely, from 13% to 74% in early studies, depending on inclusion criteria and clinical characteristics.Citation21 An accurate diagnosis of diastolic HF is often difficult to make due to lack of standardization in diagnostic criteria and misdiagnosis potential, especially in elderly, overweight, or deconditioned patients, whose conditions hinder a correct interpretation of the symptoms.Citation22
The occurrence of HF with preserved ejection fraction in the general population increases with advancing age, and is higher in women; the reported age- and sex-specific incidence has increased from 0% (men) and 1% (women) in the age group 25–49 years to about 4%–6% in men and 8%–10% in women for individuals 80 years of age and older.Citation23 In our study, irrespective of sex, the mean age of the patients was rather high, over 65 years. Furthermore, HF with preserved ejection fraction was much more often diagnosed in women. In 2009, the percentage of females with preserved LVEF was higher than in 2006, which could be explained by the larger number of females over 75 years of age included in the study. Additionally, one should keep in mind that the percentage of hypertensive patients with ejection fraction over 45% was very high in both years (>70%).
As concerns the presence of pulmonary diseases in HF cases, specialists believe that the association is much more common than currently acknowledged; however, diagnosis is difficult due to similar symptomatology.Citation24 Therefore, in the current study, paradoxically, the incidence of pulmonary pathology was much lower in 2009 than in 2006. Few clinical trials have reported the presence of concomitant COPD; where that has been the case, the low incidence of 7%–13% in the stable outpatient setting may suggest significant recruitment bias.Citation25
Conclusion
HF had the same clinical profile over a 3-year period, suggesting that there were no significant changes or improvements in the severity of the disease or the patients’ treatment. Our findings suggest that: HF is more severe in males over 65 years of age; females diagnosed with HF are usually older and have preserved LVEF; and ischemic heart disease represents the dominant etiology, but is less common in females.
Disclosure
The authors report no conflicts of interest in this work.
References
- DicksteinKCohen-SolalAFilippatosGESC Committee for Practice Guidelines (CPG)ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2008: the Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2008 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association of the ESC (HFA) and endorsed by the European Society of Intensive Care Medicine (ESICM)Eur Heart J2008292388244218799522
- StewartSJenkinsABuchanSThe current cost of heart failure to the National Health Service in the UKEur J Heart Fail20024336137112034163
- SwedbergKClelandJDargieHTask Force for the Diagnosis and Treatment of Chronic Heart Failure of the European Society of CardiologyGuidelines for the diagnosis and treatment of chronic heart failure: executive summary (update 2005): The Task Force for the Diagnosis and Treatment of Chronic Heart Failure of the European Society of CardiologyEur Heart J200526111115114015901669
- RemmeWJMcMurrayJJHobbsFDSHAPE Study GroupAwareness and perception of heart failure among European cardiologists, internists, geriatricians, and primary care physiciansEur Heart J2008291739175218506054
- AdamsonRMStahovichMChillcottSClinical strategies and outcomes in advanced heart failure patients older than 70 years of age receiving the HeartMate II left ventricular assist device: a community hospital experienceJ Am Coll Cardiol2011572487249521679851
- FangJMensahGACroftJBKeenanNLHeart failure-related hospitalization in the US, 1979 to 2004J Am Coll Cardiol20085242843418672162
- HuntSAAbrahamWTChinMHAmerican College of Cardiology FoundationAmerican Heart Association2009 Focused update incorporated into the ACC/AHA 2005 Guidelines for the Diagnosis and Management of Heart Failure in Adults A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines Developed in Collaboration With the International Society for Heart and Lung TransplantationJ Am Coll Cardiol200953e1e9019358937
- NewbyKLDouglasPSCardiovascular disease in womenBraunwald’s Heart Disease. A textbook of cardiovascular medicine8th EditionEd Saunders200819551983
- Stramba-BadialeMFoxKMPrioriSGCardiovascular diseases in women: a statement from the policy conference of the European Society of CardiologyEur Heart J200627994100516522654
- PiloteLDasguptaKGuruVA comprehensive view of sex-specific issues related to cardiovascular diseaseCMAJ20071766S1S4117353516
- AlfonsoFBermejoJSegoviaJCardiovascular disease in women. Why now?Rev Esp Cardiol2006593259263 Spanish16712750
- AzevedoAGender differences in heart failureHeart20089426426518276810
- LenzenMJRosengrenAScholte op ReimerWJManagement of patients with heart failure in clinical practice: differences between men and womenHeart200894e1017575332
- McMurrayJJAdamopoulosSAnkerSDESC Committee for Practice GuidelinesESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESCEur Heart J201233141787184722611136
- TenderaMEpidemiology, treatment, and guidelines for the treatment of heart failure in EuropeEur Heart J Suppl20057Supplement JJ5J9
- ZdrengheaDPopDPenciuODrug treatment of HF patients in a general Romanian hospitalRom J Intern Med200947322723320446437
- PopDZdrengheaDSitar-TǎutAParticularities of the cardiovascular risk in old women in an urban Romanian communityThe 2008 World Congress of Cardiology Abstracts, Buenos Aires, Argentina2008118e332
- YipGWFrenneauxMSandersonJEHeart failure with a normal ejection fraction: new developmentsHeart200995191549155219643767
- OwanTEHodgeDOHergesRMJacobsenSJRogerVLRedfieldMMTrends in prevalence and outcome of heart failure with preserved ejection fractionN Engl J Med200620355325125916855265
- KomajdaMFollathFSwedbergKStudy Group on Diagnosis of the Working Group on Heart Failure of the European Society of CardiologyThe EuroHeart Failure Survey programme – a survey on the quality of care among patients with heart failure in Europe. Part 2: treatmentEur Heart J20032446447412633547
- VasanRSBenjaminEJLevyDPrevalence, clinical features and prognosis of diastolic heart failure: an epidemiologic perspectiveJ Am Coll Cardiol199526156515747594087
- CeiaFFonsecaCMotaTEPICA InvestigatorsPrevalence of chronic heart failure in Southwestern Europe: the EPICA studyEur J Heart Fail2002453153912167394
- LamCSPDonalEKraigher-KrainerEVasanRSEpidemiology and clinical course of heart failure with preserved ejection fractionEur J Heart Fail2011131182820685685
- JabbourAMacdonaldPSKeoghAMDifferences between beta-blockers in patients with chronic heart failure and chronic obstructive pulmonary disease: a randomized crossover trialJ Am Coll Cardiol20102755171780178720413026
- HawkinsNMPetrieMCJhundPSChalmersGWDunnFGMcMurrayJJHeart failure and chronic obstructive pulmonary disease: diagnostic pitfalls and epidemiologyEur J Heart Fail20091113013919168510