Abstract
Coronary artery anomalies (CAAs) are present at birth, but are usually asymptomatic and are found during coronary angiography or multi-slice computed tomography (MSCT) detection. The most common coronary anomaly is the separating origin of left anterior descending coronary artery (LAD) and left circumflex artery (LCX) from the left sinus of Valsalva, and this variant is benign. Herein, we present three extremely rare cases of anomalous right coronary artery (RCA) detected incidentally during routine coronary angiography and confirmed by multi-slice computed tomography (MSCT) technique. All the anomalous right coronary artery coursed between the pulmonary artery and aorta. We discuss how to make an accurate diagnosis for appropriate management.
Introduction
Coronary artery anomalies (CAAs) are present at birth, but are usually asymptomatic and are found during coronary angiography or multi-slice computed tomography (MSCT) detection. Their prevalence is less than 1.3% based on a published series.Citation1–Citation4 The most common coronary anomaly is the separating origin of the left anterior descending coronary artery (LAD) and left circumflex coronary artery (LCX) from the left sinus of Valsalva. The second most common anomaly is origination of the LCX artery from the right coronary artery (RCA) or right sinus of Valsalva. Herein, we present three extremely rare cases of anomalous right coronary artery (RCA) detected incidentally during routine coronary angiography. The anomalous RCA originates from the left sinus of Valsalva, and a 64-slice MSCT detection of the heart was performed to distinguish the origin and course of the anomalous RCA. The results showed that the anomalous right coronary artery originated from the left sinus of Valsalva and coursing between the pulmonary artery and aorta; these are extremely rare. We discuss how to make an accurate diagnosis for appropriate management.
Case one
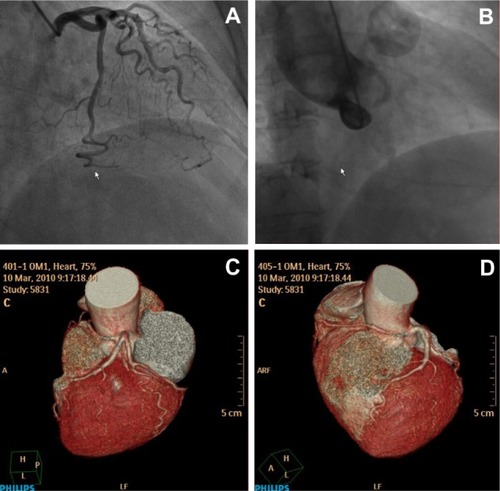
A 64-year-old woman complained of gradually progressive exertional angina pectoris for 3 months. Electrocardiogram was normal. Coronary angiogram was performed through a trans-radial approach. Coronary angiogram demonstrated the left main coronary artery (LMCA) and LAD were normal, but there was mild stenosis in the middle of the LCX segment (). Repeated attempts to cannulate the RCA were not successful (). A nonselective injection into the left coronary sinus with a pigtail catheter demonstrated an anomalous RCA arising from the left sinus. In order to confirm the anomalous origin and course of RCA, a 64-slice MSCT detection of the heart was performed on a 64-slice machine (Philips 64 Slice, Philips, Amsterdam, The Netherlands). The results showed the anomalous RCA originating from the left sinus of Valsalva, anteriorly, then taking an acute bend to course between the aorta and pulmonary artery trunk. The anomalous RCA was classified as type L-II B subtype (). The patient was treated medically.
Figure 1 (A) RAO caudal view shows a mild lesion in the middle of the LCX artery and (B) LAO view demonstrates no RCA in the right sinus of Valsalva. (C) Reconstructed three-dimensional image obtained by the volume-rendering technique shows the anomalous RCA with an interarterial course. (D) Similarly, the anomalous RCA between the aorta and pulmonary trunk can be seen.
Case two
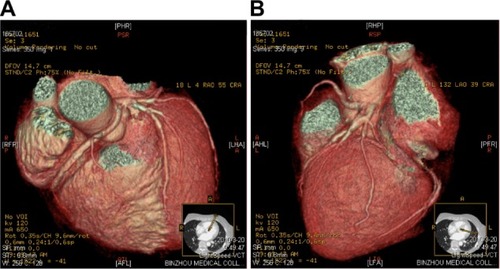
A 60-year-old woman presented with dyspnea after physical exertion for more than 2 months. Electrocardiogram showed ST depression in inferior leads II, III, aVF. Coronary angiogram was performed through trans-femoral approach. Coronary angiogram demonstrated the LMCA was normal, there was borderline narrowing in the proximal segment of LAD, and the LCX was small and patent. Repeated attempts to cannulate the RCA were successful and the result showed that the anomalous RCA originated from the left sinus of Valsalva and there was severe narrowing in the posterior descending coronary artery (PDA). Reconstructed three-dimensional images were performed to verify the course of the anomalous RCA. The results showed the anomalous RCA originating from the left sinus anterior to the left coronary artery ostium, then taking an acute bend to course between the aorta and pulmonary artery. The right coronary artery anomaly was classified as type L-II B subtype (). Neither percutaneous coronary intervention (PCI) nor coronary artery bypass grafting (CABG) was performed, and the patient was only treated medically.
Figure 2 (A) Reconstructed three-dimensional image obtained using the volume-rendering technique shows the anomalous RCA with an interarterial course. (B) The origin of the anomalous RCA is evident.
Case three
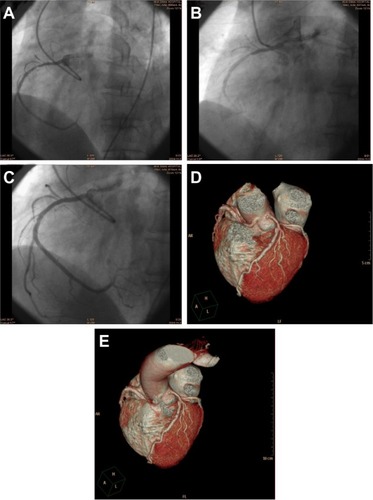
A 66-year-old man presented with an acute anterior myocardial infarction and had reperfusion therapy with thrombolytic agent. Electrocardiograms showed ST segment elevation in precordial leads V1–3 with normal creatininase values and troponin T concentration of 0.02 μg/L. The patient underwent cardiac catheterization because of post-infarct unstable angina. Angiography demonstrated that the right coronary artery and left main coronary arteries were originating from the same ostium of the left sinus (). The left main stem was patent, the LAD artery had 90% stenosis in the proximal segment, and the LCX artery was patent and non-dominant. The anomalous RCA had a high-grade 90% stenosis in the proximal (). A 6-F left Amplatz 1.5 guiding catheter was used to engage the left coronary system to perform PCI to the anomalous RCA and LAD, one stent was implanted at the proximal of the RCA segment and another stent deployed in the proximal of the LAD segment. The final angiographic result was excellent (). In order to confirm the origin and course of anomalous RCA, a 64-slice MSCT detection of the heart was performed on a 64-slice machine (Philips). The results showed the anomalous RCA originating from the left sinus of Valsalva, anteriorly, then taking an acute bend to course between the aorta and pulmonary artery trunk. The anomalous coronary artery was classified as type L-II B subtype.
Figure 3 (A) LAO cranial view shows an anomalous RCA arising from the left sinus of Valsalva. (B) LAO cranial view shows a high-grade 90% stenosis in the proximal RCA. (C) LAO cranial view shows a final good angiographic result after PCI procedure. (D) Reconstructed three-dimensional image obtained by the volume-rendering technique shows the anomalous RCA with an interarterial course. (E) The anomalous RCA originates from the left sinus of Valsalva.
Discussion
CAAs are present at birth, but are usually asymptomatic and are found during coronary angiography or MSCT detection. Their prevalence is less than 1.3% based on a published series.Citation1–Citation4 The most common coronary anomaly is the separating origin of the LAD and LCX from the left sinus of Valsalva. The second most common anomaly is the origination of the LCX artery from the RCA or right sinus of Valsalva. Anomalous right coronary artery deriving from the left coronary sinus of Valsalva is rare; its prevalence is about 0.17%.Citation1,Citation2 The three cases we reported herein all have anomalous RCA originating from the left sinus of Valsalva. The anomalous RCA arises from an orifice located anterior to the left main ostium in the left sinus of Valsalva and may course between the aorta and pulmonary artery before reaching the right atrioventricular (AV) groove (). This anomaly is suspected when the RCA ostium is unable to be located in the right sinus of Valsalva and collateral vessels are absent. The ectopic RCA is difficult to cannulate because of its slit-like orifice and odd angulation. Ostial occlusion due to aortic expansion during exercise may result in myocardial ischemia.Citation2 Clinical sequelae are rare, although angina pectoris, myocardial infarction, ventricular tachycardia, syncope, and sudden cardiac death in the absence of coronary atherosclerosis have been reported.Citation3,Citation4
In order to confirm the anomalous origin and course of the anomalous RCA, a MSCT detection of the heart was performed using a 64-slice machine (Philips). The results showed the anomalous RCA originating from the left sinus, posteriorly, then taking an acute bend to course between the aorta and pulmonary artery. There are four subtypes based on the anatomic course of the aortic artery: the aberrant vessel may course posterior to the aorta (retroaorta), or between the ascending aorta and pulmonary artery (interarterial), prepulmonary artery (prepulmonic), or septal (subpulmonic).Citation3,Citation6,Citation7 Although the interarterial subtype is extremely rare, this subtype of patient may present with symptoms of angina pectoris, myocardial infarction, ventricular tachycardia, syncope, and sudden cardiac death. Currently, these patients are submitted to cardiac surgery treatment, according to 2008 American College of Cardiology (ACC)/American Heart Association (AHA) guidelines for the management of adults with congenital heart disease.Citation5 The three cases of anomalous RCA we reported were classified as type L-II B subtype (, and ) and finally results were confirmed by 64-slice computed tomography of the heart. The first two cases were treated with oral medications, while on the third one PCI was performed; all patients are free of ischemic symptoms during follow-up.
We present these cases in an attempt to highlight their significance. These anomalies are considered to be an independent risk factor for adverse cardiovascular events including sudden cardiac death and dealing with these lesions is a challenge to cardiologists or cardiac surgeons.
Conclusion
We report three extremely rare cases of anomalous RCA that originates from the left sinus of Valsalva, and it courses between the pulmonary artery and aorta. These coronary anomalies are considered to be independent risk factors for adverse cardiovascular events, so we present these cases in an attempt to highlight their significance.
Disclosure
The authors report no conflicts of interest in this work.
References
- YamanakaOHobbsRECoronary artery anomalies in 126,595 patients undergoing coronary arteriographyCathet Cardiovasc Diagn199021128402208265
- RobertsWCSiegelRJZipesDPOrigin of the right coronary artery from the left sinus of valsalva and its functional consequences: analysis of 10 necropsy patientsAm J Cardiol19824948638687064835
- BarthCWBrayMRobertsWCSudden death in infancy associated with origin of both left main and right coronary arteries from a common ostium above the left sinus of ValsalvaAm J Cardiol19865743653663946238
- TaylorAJRoganKMVirmaniRSudden cardiac death associated with isolated congenital coronary artery anomaliesJ Am Coll Cardiol19922036406471512344
- WarnesCAWilliamsRGBashoreTMAmerican College of CardiologyAmerican Heart Association Task Force on Practice Guidelines (Writing Committee to Develop Guidelines on the Management of Adults With Congenital Heart Disease)American Society of EchocardiographyHeart Rhythm Society; International Society for Adult Congenital Heart DiseaseSociety for Cardiovascular Angiography and InterventionsSociety of Thoracic SurgeonsACC/AHA 2008 guidelines for the management of adults with congenital heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Develop Guidelines on the Management of Adults With Congenital Heart Disease). Developed in Collaboration With the American Society of Echocardiography, Heart Rhythm Society, International Society for Adult Congenital Heart Disease, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic SurgeonsJ Am Coll Cardiol20085223e143e26319038677
- AngeliniPVelascoJAFlammSCoronary anomalies: incidence, pathophysiology, and clinical relevanceCirculation2002105202449245412021235
- AngeliniPCoronary artery anomalies: an entity in search of an identityCirculation2007115101296130517353457