
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Background
Executive function impairment (in particular, mental flexibility) in the elderly, and in patients with mild cognitive impairment (MCI), is strongly correlated with difficulties in performing complex walking tasks. The aim of this study was to determine if the adaptation of a neuropsychological test (the Trail-Making Test), to evaluate executive functions during walking, can be an early detection tool for cognitive impairment.
Methods
Fifty subjects (15 young, 20 older, presumably healthy, and 15 MCI) were first evaluated for cognitive functions (Mini-Mental State Examination, Frontal Assessment Battery, and Trail-Making Test) and motor functions (10-meter walking test). All subjects then performed a spatial navigation, or a complex walking test (the Walking Trail-Making Test: [WTMT]), and their spatiotemporal walking variables were analyzed using cluster analysis.
Results
Following evaluation of WTMT locomotor performance, cluster analysis revealed three groups that were distinctly different in age and cognitive abilities: a group of young subjects, a group of healthy older subjects, MCI subjects with amnestic impairment, and a group of MCI subjects with executive function impairment. The WTMT enabled early detection, (ie, borderline MCI) of dysexecutive impairment, with 78% sensitivity and 90% specificity.
Conclusion
The WTMT is of interest in that it can help provide early detection of dysexecutive cognitive impairment.
Introduction
The concept of mild cognitive impairment (MCI) is classified, in older subjects, as a more deficient state than expected for their age and sociocultural level, but not severe enough to define it as dementia. This state is often characterized as the prodromal phase of several dementia pathologies;Citation1 and so, its early diagnosis is of major importance in the implementation of adapted care.
Executive functions (EF) are among cognitive functions that are rapidly altered in MCI subjects.Citation2,Citation3 Several studies have reported that an early EF deficit in subjects with MCI can predict the occurrence of dementia pathologies.Citation4,Citation5 EF includes a group of cognitive processes (mental inhibition, planning, mental flexibility, updating, control abilities) that enable a subject to adapt to a new and/or complex situation.Citation6 Mental flexibility, a dominant cognitive function in most cognitive models,Citation7 is defined as the ability to go from one cognitive task to another. Among the neuropsychological tests that evaluate this cognitive function, the Trail-Making Test (TMT)Citation8 is the most-used clinically, because it can be administered quickly and it evaluates several aspects: visual conception, visuospatial abilities, visuomotor coordination, divided attention, and alternation tasks.Citation9 TMT also has good power to predict the development of dementia,Citation4 which justifies its use for the detection of cognitive impairment in older subjects.
Many other neuropsychological tests that evaluate EF are used in the diagnosis of MCI.Citation10,Citation11 However, most of these tests have numerous limitations (the problem of novelty, lack of sensitivity and specificity, patient cognitive reserve, etc).Citation12,Citation13 This recent observation underscores the need to find new detection indicators for cognitive impairment.
With this in perspective, a new approach associates walking performance of older subjects with the presence and/or appearance of cognitive impairment. In fact, numerous longitudinal studies have reported that a reduction in walking speed is associated with the occurrence of negative events, such as cognitive declineCitation14 and dementia – of the Alzheimer typeCitation15 or non-Alzheimer type.Citation16,Citation17 Gait and cognition, long studied separately, appear to be closely linked, beginning in the early stages of dementia.Citation18 Indeed, the association of motor and cognitive impairment in subjects with MCI is strongly associated with a high risk of developing subsequent dementia.Citation19,Citation20
This new approach supposes the existence of a direct link between EF performances (mental inhibition, working memory, etc) and single- and dual-task walking abilities. This relationship has been shown in healthy older subjectsCitation21,Citation22 and in subjects with dementia.Citation23 Moreover, several studies have revealed that TMT score is strongly correlated with overall physical abilities,Citation24 as measured in functional testsCitation24,Citation25 and walking performance in complex situations.Citation26–Citation29
At the same time, studies in the literature have reported several adaptations of TMT to locomotion, creating original and complex walking tasks.Citation30–Citation32 In 2008, Persad et al showed, through one of these tests, called the Walking Trail-Making Test (WTMT), that subjects with dementia and MCI with dysexecutive syndrome differentiated themselves from other older subjects by locomotor performance that was significantly more altered.Citation31 In this context, new walking tests that included spatial navigation were developed for early detection of cognitive impairment in an ageing population.Citation33 We demonstrated that an adaptation of the Stroop Test to walking, by analysis of dual-task locomotor performances, made early detection of dysexecutive-type cognitive impairment possible in patients who no longer had diagnoses of MCI, but were considered as blMCI.Citation33
The aim of this study was to determine if the analysis of walking variables during an adaptation of TMT to locomotion (WTMT) is an effective means to detect cognitive impairment.
Materials and methods
Subjects
Our study population was made up of 15 young subjects (mean age: 21.1±2.2 years [20–30 years]) and 35 older adults (mean age: 75.3±6.8 years [65–85 years]). This population included young adults, healthy older subjects, and subjects with MCI from high socioprofessional categories; all subjects had college graduate education levels. The healthy older subjects were recruited from cultural associations; the young subjects were students. MCI patients were evaluated by a geriatrician or a neurologist (in memory centers) and fulfilled the criteria established by Petersen (2004).Citation1 These subjects presented a memory complaint or had cognitive impairment, identified by neuropsychological tests. They also had an absence of functional impairment and, of course, an absence of dementia.Citation1 The cognitive work-up used to determine cognitive performance enabled us to identify a group of 26 healthy subjects: 15 young healthy (YH) subjects, 11 older healthy (OH) subjects, and 15 MCI subjects, divided into subgroups according to Petersen’s criteria (six subjects with isolated impairment of MCI amnestic functions [aMCI]; three subjects with non-amnestic MCI, with isolated impairment of executive functions [naMCI]; and six subjects with multiple domain MCI cognitive impairment with dysexecutive symptoms [mdMCI]). We noted and differentiated nine subjects who were not diagnosed with MCI, but whose EF test performances were consistently at the threshold of pathologic levels. These subjects formed another group, which we described in a previous study as “borderline MCI” (blMCI).Citation33
Inclusion criteria were: to be willing to actively participate in the study, live in a non-institutional environment, and be able to get around on an everyday basis without technical assistance. Exclusion criteria were: uncorrected visual impairment, a neurologic pathology (Parkinson’s disease, stroke, etc), orthopedic surgery of the lower limbs, depression, and the taking of medications that could influence posture and/or gait. All subjects consulted with a doctor, to verify inclusion and exclusion criteria. Prior to inclusion in the study, each subject signed informed consent forms, in order to participate.
Evaluation of cognitive and motor abilities
The subjects first underwent an evaluation of cognitive functions by a neuropsychologist, using the Mini-Mental State ExaminationCitation34 and the Frontal Assessment Battery.Citation35 Each subject was assessed using the Stroop Color-Word test, the Wechsler Adult Intelligence Scale (WAIS) III, the Clock-Drawing Test, and the Corsi Block-Tapping Test.
The dominant cognitive function in our study was mental flexibility, which was tested using the TMT.Citation8 The TMT is a paper and pencil test that consists of linking targets as quickly as possible, in numeric order in Part A, (ie, 1–25), and alternating between numbers and letters in Part B (ie, 1–A–2–B–3–C).Citation8 It evaluates visual perception abilities, perceptual/motor speed, and speed processing in Part A, and mental flexibility in Part B. Delta TMT (ΔTMT) (TMT B–TMT A) is considered the best indicator of EF performance.Citation9
Finally, we performed a motor evaluation of single-task, spontaneous walking for 10 minutes, in a normal environment on a pressure-sensitive, portable walkway (Length: 793 cm; Width: 61 cm; Height: 0.6 cm) (GAITRite®, CIR Systems Inc, Sparta, NJ, USA). In order to derive a value representative of single-task locomotor abilities, subjects were asked to walk five times, at a spontaneous pace, from which walking speed, frequency, cycle time, and time in double support were calculated.
Complex walking task: the Walking Trail-Making Test
The WTMT is an adaptation to walking of a traditional neuropsychological test, the TMT. We used an experimental protocol similar to that of Persad,Citation31 by reproducing the different stages proposed by those authors (). In the WTMT-N part, the walking circuit is always performed in the same order. First, the subject is asked to walk on 20 numeric targets, in increasing order (ie, 1–20). In the WTMT-A part, the WTMT-N includes 20 other, associated targets, considered as distraction targets. These targets, which the subject must avoid during the test, have been added to provide an attentional aspect to the walking test. Finally, the third part, called WTMT-B, evaluates mental flexibility abilities. For this test, subjects are asked to walk on targets, alternating between numbers and letters, while avoiding the 20 distraction targets (ie, 1–A–2–B–3–C). Each target is eight centimeters in diameter.
Figure 1 Illustration of WTMT experimental conditions.
Abbreviation: WTMT, Walking Trail-Making Test.
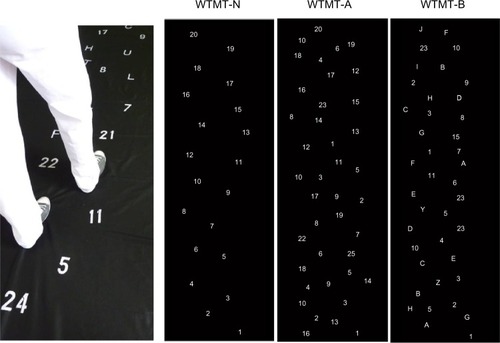
The main modification of the TMT, relative to the 2008 study by Persad et al, is that our targets were drawn on a removable cloth support of five-meter length, which covered the eight-meter electronic walkway. This device, therefore, provided a recording of all of the WTMT walking variables. In order to study locomotor performances, we selected four spatiotemporal walking variables: speed, frequency, double support time, and cycle time.
In this circumstance, the carpet is black and the targets are white, in order to increase contrast and reduce the risk of instability that is linked to the treatment of information. Indeed, in 1991, Lord et al demonstrated that reduction of ability to distinguish characters with low contrast was a strong predictor of the risk of falling.Citation36
The subjects received the following instruction, to perform the two tasks as best they could: “Walk as fast as possible and do the WTMT exercise without making any mistakes.” However, no priority was given to one domain or the other. Each condition had a familiarization and learning phase (over a distance of 2 meters), which was repeated until the subject understood the task to be accomplished (a maximum of three repetitions were allowed). During the test, the result was considered to be positive when the subject touched the correct targets with his or her foot. Each condition was filmed using a webcam (640 × 480 pixel resolution) that was synchronized with the electronic walkway, in order to detect errors accurately. Indeed, we used video recording only for error analysis. This video camera was placed in front of the electronic walkway, in line with the anteroposterior axis of travel. We noted the number of errors the subjects made on the test (expressed in percentages of subjects who made the fewest errors).
Statistics
Our aim was to detect the possible existence of executive function impairment from WTMT walking characteristics only. The ascendant hierarchic classification method, or cluster analysis (Ward’s method,Citation37 Euclidean distance), makes it possible to regroup subjects, according to their functional similarities, from the spatiotemporal parameters of walking.
The differences between groups formed by the cluster analysis method, be it WTMT or cognitive and functional tests, were studied using analysis of variance (ANOVA), followed by a post hoc Tukey’s test. The correlation coefficient between ΔTMT and single-task walking speed and the correlation coefficient between ΔTMT and WTMT were studied using Pearson’s R coefficient. Statistical analysis was performed using Statistica Version 9 software (StatSoft Inc, Tulsa, OK, USA). Results were considered significant at P<0.05.
Finally, when one attempts to detect a syndrome from a test, one determines the sensitivity and specificity values for this test. For our experimental conditions, sensitivity and specificity values for the detection of the MCI syndrome by WTMT were calculated using the following formulas:
Low performance refers to the motor performance of the group with the largest deficit in the WTMT, and high performance refers to the group with the best gait parameters in navigational tasks.Citation33
Results
WTMT cluster analysis
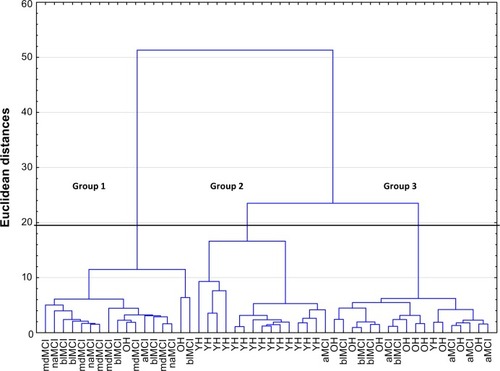
WTMT cluster analysis () includes the subjects’ locomotor performances for the entire test. Classification by the ascendant hierarchic method revealed three distinct branches, with a Euclidean distance of <20 and a reunification at 50 (). The R ratio calculationCitation38 distinguished three, apparently different, walking abilities for the entire test.
Figure 2 Dendrogram of spatio-temporal walking variables during WTMT.
Abbreviations: YH, young healthy; OH, older healthy; blMCI, borderline MCI; naMCI, non-amnestic MCI – executive impairment only; aMCI, amnestic MCI; mdMCI, multiple domain amnestic MCI; WTMT, Walking Trail-Making Test.
MCI detection
We studied the morphological and psychobehavioral characteristics (age, cognitive ability) of the subjects in each group (). Overall, the subjects in Group 2 were much younger than those in Groups 1 and 3, and the subjects in Group 1 had significantly more EF deterioration (Frontal Assessment Battery; ΔTMT) than the subjects in Groups 2 and 3 (). More precisely, Group 1 mainly included older subjects presenting a decline in EF (naMCI, mdMCI), or cognitive fragility of the dysexecutive type (blMCI), including 17 older subjects (five older, 12 very elderly): two healthy, six mdMCI, five blMCI, three naMCI, and one aMCI, whereas Group 2 was made up of 15 subjects (14 young, one older): 14 young and healthy, and one aMCI. Finally, Group 3 was more heterogeneous. It was made up of 18 subjects (one young, 12 older, five very elderly): ten healthy, four blMCI, and four aMCI.
Table 1 Demographic, clinical, and locomotor characteristics of the different groups formed by cluster analysis
Figure 3 Breakdown by circular diagram of the cognitive profiles of the subjects in each group from the cluster analysis.
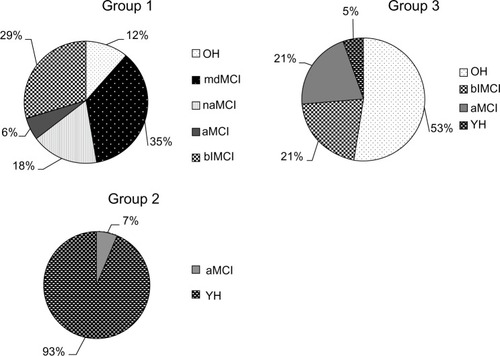
The WTMT detected dysexecutive syndrome (naMCI and mdMCI) with 100% sensitivity and 80% specificity. This test also made it possible to detect EF fragility, beginning at the blMCI stage, with 78% sensitivity and 90% specificity.
Gait characteristics
We studied the functional abilities of these three cluster analysis groups. We first observed that the subjects in Group 1 walked more slowly than the subjects in Group 2 during the single-task walking test, and that there was not a significant difference between the subjects in Groups 2 and 3 (). On the other hand, during the WTMT, the locomotor performances of Group 1 subjects were significantly worse than those of Group 3, whose performances were worse than those of Group 2 (). This impairment in locomotor abilities during WTMT was observed by reductions in walking speed (F=78.7; P<0.001) and walking frequency (F=76.4; P<0.001), and by increases in cycle time (F=113.3; P<0.001) and percentage in double support (F=47.6; P<0.001) (). Lastly, the number of subjects making errors was higher in Group 1 than in the other groups (P=0.009) ().
Finally, as for the link between cognitive and motor abilities, performance in ΔTMT was significantly correlated with WTMT walking speed (R=0.54, P<0.05), but not with single-task walking speed (R=0.10).
Discussion
The aim of this study was to determine if the WTMT could detect people with early-stage EF impairment. Cluster analysis broke down the subjects into groups according to the similarities of the different walking variables. We noted that the groups were differentiated at both locomotor and cognitive levels.
In this study, we did not note any walking variables to analyze subjects’ locomotor performances, but we did study the locomotor abilities of each subject during the WTMT. In the literature, one can observe that several walking variables, and not one alone, can reveal an alteration in dual-task locomotor performance.Citation23,Citation39 Moreover, some authors have associated an alteration in cognitive functions with a reduction in walking speed.Citation21,Citation22,Citation40,Citation41 Therefore, we think that integrating several walking variables in the statistical analysis reinforces the results.
The WTMT is characterized as a complex walking task, requiring the subject to plan his/her walking in a defined space, according to a goal. The aim is to use walking tests that are more related to spatial navigation than to stereotyped walking in a straight line, in which the subject is able to pace his/her walking frequency depending on the cognitive task.Citation42
Detection of cognitive impairment in the elderly by analysis of locomotor performances during WTMT
Detailed study of the spatiotemporal variables of walking during the WTMT revealed three distinct groups. Group 1 subjects had the lowest performances in the WTMT and walked with cautious gaits during the test (ie, they greatly reduced their walking speeds, significantly increasing their times in double support). Group 3 subjects had intermediate locomotor performances that were between those of Groups 1 and 2, but were significantly different from each. Error analysis showed that, on average, one out of two older subjects committed at least one error during the WTMT (). Therefore, Group 1 subjects had the lowest performances in both domains (physical and cognitive).
In the literature, several authors have studied the performance of the elderly on the WTMT.Citation30,Citation31 Alexander et al observed that the locomotor performances of WTMT subjects depended on their age. We agree with their first results because, in this study, the subjects who had the best WTMT performances were in Group 2, which was essentially made up of young adults (14 out of 15 subjects), whereas Groups 1 and 3 were composed of older subjects (>65 years old). These results are different from those of another test that we recently developed (the Walking Stroop Carpet); in this study, healthy older subjects were grouped with young subjects.Citation33
The WTMT has been identified in the literature as a test that is sensitive to the alteration of cognitive functions.Citation31 In order to study the relationship between gait and cognition in this population, we analyzed the cognitive profiles of the subjects in Groups 1 and 3. Analysis of the different MCI subgroups, according to Petersen’s classification (2004), revealed that all of the MCI subjects with a dysexecutive-type syndrome (naMCI or mdMCI) were in Group 1 (nine out of nine subjects), whereas the aMCI subjects were mainly in Group 3 (four aMCI subjects out of six). In our study population, the WTMT was able to detect the dysexecutive syndrome with 100% sensitivity and 80% specificity. Persad et al (2008) reported similar results, since the group with EF alteration (naMCI and Alzheimer patients) had WTMT-B performances that were significantly more altered than the group of subjects without EF alteration (aMCI and healthy subjects).Citation31
This strong relationship between EF impairment and reduction in walking abilities can be found in the literature, in particular, in studies of TMT performance. First of all, many authors have reported that low TMT performances are associated with a reduction in the overall physical abilities of older subjects,Citation25 of subjects with MCI,Citation43 and even as a predictor of early morbidity.Citation24 Moreover, analysis of walking abilities has revealed that older subjects whose TMT performances were the poorest also presented a reduction in complex walking exercises, such as the Figure-of-Eight Walk test,Citation28 a seven-meter walk, with obstacles.Citation26,Citation27 In the present study, we found the same relationship, since the ΔTMT score was significantly correlated with walking speed during the WTMT, but not with single-task walking speed.
This relationship between cognitive and locomotor abilities does not appear to be linked with amnestic abilities.Citation21,Citation31,Citation44 In this study, the aMCI and healthy older subjects were classified into the same groups according to their locomotor performances. One can suppose, therefore, that amnestic abilities do not have an impact on WTMT performance.
Early detection of cognitive impairment that was not revealed in traditional neuropsychological tests
Thorough clinical analysis of the older population revealed the presence of blMCI: subjects who presented neuropsychological test performances that were consistently on the verge of the pathological threshold.Citation33 We noted that some blMCI subjects were classified by their WTMT locomotor performances (five out of nine subjects) in the same group (Group 1) as the MCI subjects with EF impairment (). We can suppose that a complex walking exercise, such as the WTMT, makes it possible to detect subjects who were not diagnosed as MCI by traditional neuropsychological tests, but who, nevertheless, presented common impairments (alterations of locomotor abilities during complex walking, and reduction in EF performances). The WTMT has the ability to detect early EF (ie, the blMCI stage) with 78% sensitivity and 90% specificity. These values are slightly inferior to those obtained with the Walking Stroop Carpet.Citation33
We suppose that blMCI subjects who present a major modification in walking variables during WTMT are more at risk to evolve towards an MCI state, even to dementia. Indeed, several authors have reported that subjects with MCI who have an abnormal gait during dual-task or complex walking situations are more at risk of developing dementia.Citation18–Citation20,Citation45 These hypotheses suggest, once again, that walking impairment could play an important role in the diagnosis of dementia and that, even before the MCI stage, we can detect, through complex walking tests, older subjects who are likely to deteriorate at a cognitive level.
These differences in detection abilities, between our tests and those currently used, can be explained by the numerous limitations presented by traditional neuropsychological tests. Indeed, the performances of neuropsychological tests to evaluate EF vary according to numerous parameters, such as a lack of novelty, diagnostic variations dependent on threshold values,Citation46 and the taking of medications.Citation13 Moreover, the older subjects who participated in our study had high levels of education and were from high socioprofessional categories. Therefore, it is probable that these subjects had sufficient cognitive reserve to respond to traditional neuropsychological tests. On the other hand, we can suppose that this cognitive reserve would be negatively affected in a complex walking situation or when great attention is required.Citation47
Limitations
Our study showed that this test provides early detection of cognitive impairment, but did not give us values for clinical diagnostic use. It would be of interest to define a threshold value that would enable a clinician to decide on the presence of cognitive impairment and to make a diagnosis. Such a decision value, with confidence intervals, defined according to walking speed, could be studied in a broader population, in order to improve clinical diagnosis.
Our population is small, with regard to statistical treatment, because this study was based on only 36 older subjects and 15 young subjects. In addition, 27 out of the 32 subjects in Groups 1 and 2 were women.
Moreover, these tests should be performed on a larger population that includes Alzheimer patients, in order to determine whether they present the same motor performances as dysexecutive-type MCI subjects, or if they make up a new group in the cluster analysis. The monitoring of this population within the framework of a longitudinal study would make it possible to increase statistical power and to confirm previously developed clinical hypotheses.
Conclusion
New walking tests, such as the WTMT, come close to everyday acts, in which walking situations are navigational situations, punctuated with sensory conflicts and interferences provoked by mental operations. The WTMT also detects older people with cognitive fragility (blMCI), who are likely to deteriorate. The WTMT is a test that is noninvasive and easily and quickly performed. This test requires low-cost equipment, which makes it possible to test a large proportion of a population.
Disclosure
The authors have no conflicts of interest to declare.
References
- PetersenRCMild cognitive impairment as a diagnostic entityJ Intern Med2004256318319415324362
- TraykovLRaouxNLatourFExecutive functions deficit in mild cognitive impairmentCogn Behav Neurol200720421922418091070
- ReinvangIGrambaiteREspesethTExecutive dysfunction in MCI: subtype or early symptomInt J Alzheimers Dis2012201293627222693679
- ChapmanRMMapstoneMMcCraryJWPredicting conversion from mild cognitive impairment to Alzheimer’s disease using neuropsychological tests and multivariate methodsJ Clin Exp Neuropsychol201133218719920711906
- ClarkLRSchiehserDMWeissbergerGHSalmonDPDelisDCBondiMWSpecific measures of executive function predict cognitive decline in older adultsJ Int Neuropsychol Soc201218111812722115028
- GodefroyOFrontal syndrome and disorders of executive functionsJ Neurol1200325011612527984
- MiyakeAFriedmanNPEmersonMJWitzkiAHHowerterAWagerTDThe unity and diversity of executive functions and their contributions to complex “Frontal Lobe” tasks: a latent variable analysisCogn Psychol20004114910010945922
- ReitanRMTarshesELDifferential effects of lateralized brain lesions on the trail making testJ Nerv Ment Dis195912925726214437233
- Sanchez-CubilloIPerianezJAAdrover-RoigDConstruct validity of the Trail Making Test: role of task-switching, working memory, inhibition/interference control, and visuomotor abilitiesJ Int Neuropsychol Soc200915343845019402930
- TabertMHManlyJJLiuXNeuropsychological prediction of conversion to Alzheimer disease in patients with mild cognitive impairmentArch Gen Psychiatry200663891692416894068
- LopezOLBeckerJTJagustWJNeuropsychological characteristics of mild cognitive impairment subgroupsJ Neurol Neurosurg Psychiatry200677215916516103044
- BrooksBLStraussEShermanEMSIversonGLSlickDJDevelopments in neuropsychological assessment: Refining psychometric and clinical interpretive methodsCanadian Psychology2009503196209
- WestonALWeinsteinAMBartonCYaffeKPotentially inappropriate medication use in older adults with mild cognitive impairmentJ Gerontol A Biol Sci Med Sci201065331832119843646
- Abellan van KanGRollandYAndrieuSGait speed at usual pace as a predictor of adverse outcomes in community-dwelling older people an International Academy on Nutrition and Aging (IANA) Task ForceJ Nutr Health Aging2009131088188919924348
- WaiteLMGraysonDAPiguetOCreaseyHBennettHPBroeGAGait slowing as a predictor of incident dementia: 6-year longitudinal data from the Sydney Older Persons StudyJ Neurol Sci20052292308993
- VergheseJLiptonRBHallCBKuslanskyGKatzMJBuschkeHAbnormality of gait as a predictor of non-Alzheimer’s dementiaN Engl J Med2002347221761176812456852
- VergheseJDerbyCKatzMJLiptonRBHigh risk neurological gait syndrome and vascular dementiaJ Neural Transm2007114101249125217541695
- HausdorffJMBuchmanASWhat links gait speed and MCI with dementia? A fresh look at the association between motor and cognitive functionJ Gerontol A Biol Sci Med Sci201368440941123401565
- VergheseJWangCLiptonRBHoltzerRMotoric cognitive risk syndrome and the risk of dementiaJ Gerontol A Biol Sci Med Sci201368441241822987797
- Montero-OdassoMBergmanHPhillipsNAWongCHSourialNChertkowHDual-tasking and gait in people with mild cognitive impairment. The effect of working memoryBMC Geriatr200994119723315
- van IerselMBKesselsRPBloemBRVerbeekALOlde RikkertMGExecutive functions are associated with gait and balance in community-living elderly peopleJ Gerontol A Biol Sci Med Sci200863121344134919126847
- BeauchetOAnnweilerCMontero-OdassoMFantinoBHerrmannFRAllaliGGait control: a specific subdomain of executive function?J Neuroeng Rehabil201291222321772
- Yogev-SeligmannGHausdorffJMGiladiNThe role of executive function and attention in gaitMov Disord2008233329342 quiz 47218058946
- HirotaCWatanabeMSunWAssociation between the Trail Making Test and physical performance in elderly JapaneseGeriatr Gerontol Int2010101404720102381
- VazzanaRBandinelliSLauretaniFTrail Making Test predicts physical impairment and mortality in older personsJ Am Geriatr Soc201058471972320398153
- BleAVolpatoSZulianiGExecutive function correlates with walking speed in older persons: the InCHIANTI studyJ Am Geriatr Soc200553341041515743282
- CoppinAKShumway-CookASaczynskiJSAssociation of executive function and performance of dual-task physical tests among older adults: analyses from the InChianti studyAge Ageing11200635661962417047008
- HessRJBrachJSPivaSRVanSwearingenJMWalking skill can be assessed in older adults: validity of the Figure-of-8 Walk TestPhys Ther2010901899919959654
- HobertMANieblerRMeyerSIPoor trail making test performance is directly associated with altered dual task prioritization in the elderly – baseline results from the TREND studyPLoS One2011611e2783122114705
- AlexanderNBAshton-MillerJAGiordaniBGuireKSchultzABAge differences in timed accurate stepping with increasing cognitive and visual demand: a walking trail making testJ Gerontol A Biol Sci Med Sci200560121558156216424288
- PersadCCJonesJLAshton-MillerJAAlexanderNBGiordaniBExecutive function and gait in older adults with cognitive impairmentJ Gerontol A Biol Sci Med Sci12200863121350135519126848
- YamadaMIchihashiNPredicting the probability of falls in community-dwelling elderly individuals using the trail-walking testEnviron Health Prev Med201015638639121432571
- PerrochonAKemounGWatelainEBerthozAWalking Stroop carpet: an innovative dual-task concept for detecting cognitive impairmentClin Interv Aging2013831732823682211
- FolsteinMFFolsteinSEMcHughPR“Mini-mental state”. A practical method for grading the cognitive state of patients for the clinicianJ Psychiatr Res1119751231891981202204
- DuboisBSlachevskyALitvanIPillonBThe FAB: a Frontal Assessment Battery at bedsideNeurology200055111621162611113214
- LordSRClarkRDWebsterIWVisual acuity and contrast sensitivity in relation to falls in an elderly populationAge Ageing19912031751811853790
- WardJHHierarchical grouping to optimize an objective functionJ Am Stat Assoc196358236244
- HartiganJAClustering Algorithms (Probability and Mathematical Statistics)Hoboken, NJJohn Wiley and Sons1975
- Al-YahyaEDawesHSmithLDennisAHowellsKCockburnJCognitive motor interference while walking: a systematic review and meta-analysisNeurosci Biobehav Rev201135371572820833198
- SheridanPLSolomontJKowallNHausdorffJMInfluence of executive function on locomotor function: divided attention increases gait variability in Alzheimer’s diseaseJ Am Geriatr Soc200351111633163714687395
- AllaliGAssalFKressigRWDubostVHerrmannFRBeauchetOImpact of impaired executive function on gait stabilityDement Geriatr Cogn Disord200826436436918852489
- BeauchetOAllaliGPoujolLBarthelemyJCRocheFAnnweilerCDecrease in gait variability while counting backward: a marker of “magnet effect”?J Neural Transm2010117101171117620809070
- McGoughELKellyVELogsdonRGAssociations between physical performance and executive function in older adults with mild cognitive impairment: gait speed and the timed “up and go” testPhys Ther20119181198120721616934
- HausdorffJMYogevGSpringerSSimonESGiladiNWalking is more like catching than tapping: gait in the elderly as a complex cognitive taskExp Brain Res2005164454154815864565
- Montero-OdassoMVergheseJBeauchetOHausdorffJMGait and cognition: a complementary approach to understanding brain function and the risk of fallingJ Am Geriatr Soc201260112127213623110433
- KochanNASlavinMJBrodatyHEffect of different impairment criteria on prevalence of “objective” mild cognitive impairment in a community sampleAm J Geriatr Psychiatry201018871172221491632
- HoltzerRWangCLiptonRVergheseJThe protective effects of executive functions and episodic memory on gait speed decline in aging defined in the context of cognitive reserveJ Am Geriatr Soc201260112093209823039200