
Abstract
The purpose of this study was to measure kinesthetic accuracy in healthy older adults by using arm position and motion matching tests. We investigated the effect of task type, joint angle, and matching arm results on kinesthetic accuracy in the upper extremities of 17 healthy right-handed older adults. Blinded subjects were asked to match positions and motions at four reference joint angles: 1) shoulder flexion, 0°–60°; 2) elbow flexion, 90°–135°; 3) wrist extension, 0°–50° in the sagittal plane; and 4) shoulder abduction, 0°–60° in the frontal plane. The absolute difference in angular displacement between the reference and matching arms was calculated to determine kinesthetic accuracy. Results showed that subjects were more accurate at matching motion than position tasks (P=0.03). Shoulder and elbow joints were more sensitive than wrist joints in perceiving passive positions and motions (P<0.05). The effect of the matching arm was found only when matching the joint angles of shoulder abduction and wrist extension (P<0.01). These results are comparable to findings of other studies that used machine-generated kinesthetic stimuli. The manual measurement of kinesthetic accuracy could be effective as a preliminary screening tool for therapists in clinical settings.
Introduction
Proprioception has been defined as awareness of and ability to sense the position of limbs, trunk (position sense), and kinesthesia as the awareness of motion of the human body (motion sense).Citation1 Awareness and ability are essential for optimal muscular control, coordination, and stability when planning movements for the performance of daily activities.Citation2–Citation5
In a rehabilitation setting, therapists often rely on proprioceptive and kinesthetic accuracy to determine intervention programs and evaluate treatment effectiveness.Citation6 A comprehensive sensory evaluation can provide useful information for determining clinical treatment. However, results from Lincoln et al showed that inter-rater reliability of sensory assessment for stroke survivors was poor due to variability between assessors and subjects.Citation7 A reliable and standardized assessment is needed to increase the reliability of assessment and minimize physical and mental demands on subjects. Although the validity and reliability of the arm matching test has been little researched,Citation8 the magnitude of end-position errors has been thought to be a good indicator of acuity for motion and position sense.Citation9
The arm position matching test, a common proprioceptive measurement, is used to measure the ability of a subject to perceive limb position by moving a single joint on one side and matching its exact position on the other.Citation10–Citation12 During the test, subjects are required to move the testing joint to match the reference joint at the desired position. At the end of each trial, examiners visually determine proprioceptive accuracy. Using an ordinal scale, accuracy is noted as absent (no appreciation), impaired (inaccurate detection), or intact (precise awareness).Citation6,Citation13
Although previous studies have reported on the accuracy of position and motion sense for various populations,Citation14–Citation22 the experimental paradigms used in those studies are difficult for clinical practitioners to apply on patients due to the following reasons. First, researchers used their own customized apparatuses to measure accuracy of position and motion sense because uniform commercial apparatuses were unavailable. Second, lack of a standardized test protocol made it difficult to compare results across studies. Finally, some experimental paradigms involved the use of memory issues, applications that were impractical when patients suffered from central nervous system (CNS) impairments.
As a result, the current study examined the most widely used clinical position and motion sense assessments, the arm position and motion matching tests, to investigate their suitability for screening proprioceptive and kinesthetic ability in a clinical setting. When performing the tests during assessments, therapists did not move the subject’s reference arm back to the starting position. Furthermore, subjects were not required to memorize arm positions or motions during the tests; therefore, memory issues were excluded. The tests were simple and easy to administer to patients in a clinical setting. This study investigated whether the arm position matching test could be a useful screening test for measuring passive position sense of the upper limbs by manually imposing passive movements on the upper extremities. Subjects were required to mirror the position while blinded to the tests.
This study measured proprioceptive and kinesthetic accuracy in healthy older adults by using the arm matching position and motion tests. We investigated the effects of task types (position matching vs motion matching), joint angles (shoulder flexion 0°–60°, shoulder abduction 0°–60°, elbow flexion 90°–135°, and wrist extension 0°–50°), and matching arm (preferred vs non-preferred hand) on the accuracy of position and motion sense of the joints in the upper extremities. The main purpose of this study was to investigate whether arm matching position and motion tests can provide clinical results compatible with those of previous studies that used a custom-made apparatus as an initial screening tool.
Methods
Subjects
Seventeen healthy right-handed older adults (7 males, 10 females) participated in this study. Mean age was 62.59±4.60 years (mean ± SD) and ranges between 56–70 years. Mini Mental State Examination (MMSE) results were 28.65±1.00 (mean ± SD). All subjects signed an informed consent form approved by the Institutional Review Board of Chang Gung Memorial Hospital. Inclusion criteria were: 1) Right-handedness. Only right-handed subjects were included according to the Edinburgh Handedness Inventory;Citation23 b) No cognitive impairment. Subjects with a score <24 on the MMSE were excluded;Citation24 and c) No presence of neurological disease such as stroke or diabetes that could interfere with kinesthesia. A medical history interview was performed to exclude subjects with past severe arm injuries.
Kinematic measurements
We used a seven-camera Vicon MX motion analysis system (Oxford Metrics Inc., Oxford, UK) with a sampling rate of 120 Hz to capture the movement of subjects during arm position and motion matching tests. A total of nine spherical markers each with a diameter of 5 mm were used (four markers on each arm and one on the sternum). Bony landmarks were the sternum, acromion process, lateral epicondyle, styloid process of the ulna, and dorsal surface of the third metacarpophalangeal joint. Similar marker placements have been used in previous studies.Citation25–Citation27 Prior to data collection, the system was reconfigured, calibrated, and test data were collected. This initial process required approximately 40 minutes. For each individual testing session, the experimenters spent 10 to 15 minutes preparing the system for testing.
Shoulder flexion was determined by the angle between the vector joining the ipsilateral acromion-lateral epicondyle markers and the vector from the acromion process towards the hip in the sagittal plane. Shoulder abduction was calculated using the angle between the vector joining the ipsilateral acromion-lateral epicondyle markers and the vector from the acromion process towards the hip in the frontal plane. Elbow flexion was determined by the angle between the vector formed by the ipsilateral acromion-lateral epicondyle markers and a vector defined by the lateral epicondyle and styloid process of the ulna in the sagittal plane. Wrist extension was determined by the angle between the vectors formed by the ipsilateral lateral epicondyle and styloid process of the ulna and a vector defined by the styloid process of the ulna and third metacarpophalangeal joint in the sagittal plane.
Procedure
Due to a lack of standardized testing protocols for clinics, we based the evaluation procedure on previous research and current clinical practice.Citation6,Citation14,Citation28 Measuring accuracy of position and motion sense in the upper extremities normally includes the major joints, and excludes the end position, which can generate extra cues other than proprioceptive information.Citation8,Citation29 In general, the evaluation was performed from the proximal to the distal joint, and was simple for clinical practitioners to administer. Four joint angles were selected for the arm position and motion matching tests: 1) shoulder flexion (SF), 0°–60°; 2) elbow flexion (EF), 90°–135°; 3) wrist extension (WE), 0°–50° in the sagittal plane; and 4) shoulder abduction (SA), 0°–60° in the frontal plane. A detailed graphical representation of the joint angles is shown in .
Figure 1 Tested joint angles and marker placement.
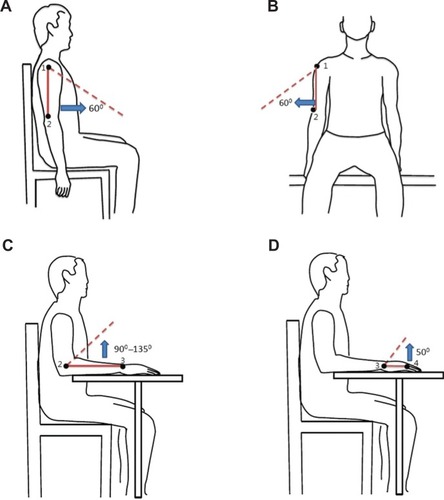
Each subject was seated in a chair adjusted to the subject’s height. The subject’s forearm rested with an elbow flexion of 90° for the starting position. Vision was then blocked by opaque glasses, to ensure that the subject relied exclusively on kinesthesia to perform the required tasks. Each subject visited the laboratory once and both arms were tested. Each joint angle was measured three times, and one joint was moved each time. Before data recording, practice trials were performed without the use of opaque glasses to familiarize subjects with the experimental tasks. To ensure consistency of angular displacement imposed by the experimenter, three goniometers were placed on the table and the back of the subject’s chair so that the experimenter could visualize the desired reference joint angles to enhance accuracy. The experimental setup is shown in .
Figure 2 Experimental setup.

The order of the experiment was balanced by a Latin square design to prevent a potential order effect. Therefore, each subject was randomly assigned to the following four blocks: 1) position matching task with the non-preferred side as the matching arm; 2) position matching task with the preferred side as the matching arm; 3) motion matching task with the non-preferred side as the matching arm; and 4) motion matching task with the preferred side as the matching arm. Each block contained 12 trials; in total 48 trials were conducted, administered by a certified occupational therapist. To ensure the reliability of the imposed displacement and movement, the occupational therapist was trained to follow the experimental protocol and to move the individual joint to the desired angles using the goniometers attached to the chair. To prevent possible extra cues during arm matching tasks, the therapist was instructed to hold the neighboring joints instead of the muscle belly at the desired angles.
In the arm position matching test, the examiner moved the reference arm to the testing joint angles. To mimic the actual measuring procedures used in clinics, the experimenter moved each joint angle for 2 to 4 seconds and maintained the position while subjects moved the matching arm to mirror the joint angle. During the arm motion matching test, the examiner moved the reference arm and asked the subject to concurrently mirror the motion with the matching arm. Subjects were instructed to match the imposed velocity with the matching arm as soon as they were aware of the limb motion. The experimenter isolated the tested joint and attempted to maintain a steady speed for each trial. In both the arm position and motion matching tests, each joint angle measurement was repeated until three correct matching trials were recorded. At the end of each trial, subjects were required to verbally confirm that both joint angles were identical and at symmetrical positions. For the motion sense task, subjects were further required to verbally confirm whether the motion at both joint occurred at the same speed.
Data analyses
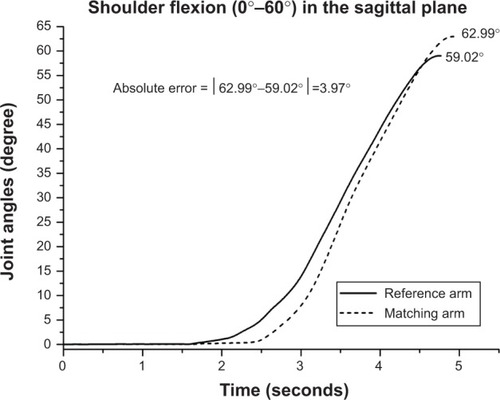
We used a customized algorithm based on MATLAB® (The MathWorks, Inc., Natick, MA, USA) to calculate angular displacement for each trial. All kinematic data were filtered by a low pass Butterworth fourth-order filter with a cut-off frequency of 5 Hz. The outcome measure was the difference in angular displacement (absolute error) between the reference and matching arms. The absolute error was computed in degrees by subtracting the angular displacement of the reference arm from that of the matching arm. As the most widely used measure of proprioceptive and kinesthetic accuracy, the absolute error can distinguish differences among various populations.Citation13–Citation15,Citation30,Citation31 An example calculation of absolute error is shown in . For position sense tasks, random and constant errors were calculated to show directional information.
Figure 3 Example calculation of absolute error.
A three-way repeated measure analysis of variance (ANOVA) was performed to determine differences in within-subject factors for position and motion sense accuracy followed by post hoc analysis. The three within-subject factors were tasks (position matching vs motion matching), joint angles (SF vs SA vs EF vs WE), and matching arms (preferred arm vs non-preferred arm). The significance level was P<0.05.
Results
Because passive position and motion were imposed manually by the experimenter, we examined the intraclass correlation coefficient (ICC) of angular displacement for each joint angle to ensure reliability. The ICC for each joint angle was between 0.6 and 0.8, which has been defined as an acceptable agreement.Citation32 The average velocity of joint angle movement imposed manually by the therapist was 20.24±3.95 (°/s). The mean absolute error for each joint angle and task are presented in and .
Table 1 Absolute error (mean ± SD) for each condition in degrees
Table 2 Constant error and random error for position sense in degrees
The results from the repeat ANOVA did not yield a significant task × joint angle × matching arm interaction effect for kinesthetic accuracy (F2.27,111.27=0.69, P=0.52); however, the joint angle matching arm interaction effect was significant (F2.51,122.97= 8.28, P<0.05). The simple main effect was further analyzed and a post hoc analysis using least significant difference was performed for a significant effect.
Effect of task type
The absolute error was 9.91°±0.35° (mean ± SD) for the position matching test and 8.90°±0.40° (mean ± SD) for the motion matching test. A statistically significant difference was found between position and motion matching tests (F1,49=4.82, P=0.03), and results showed that subjects performed more accurately in the arm motion matching test than in the arm position matching test.
Effect of joint angles
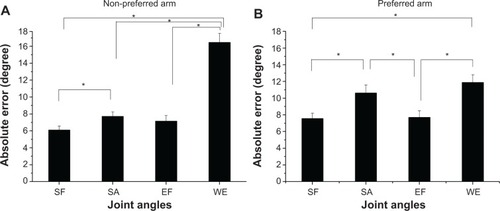
Further analysis found significant differences in absolute error for joint angles in the preferred (F3,147=8.02, P<0.001) and non-preferred arms (F2.3,112.5=39.63, P<0.001). Post hoc analyses showed that subjects were least accurate in matching wrist extension 0°–50° compared to shoulder flexion 0°–60°, shoulder abduction 0°–60°, and elbow flexion 90°–135° (all P<0.05; ).
Figure 4 The effect of joint angle on the (A) non-preferred arm and (B) preferred arm.
Abbreviations: SF, shoulder flexion 0°–60°; SA, shoulder abduction 0°–60°; EF, elbow flexion 90°–135°; WE, wrist extension 0°–50°.
Effect of matching arm (using preferred arm vs non-preferred arm)
Absolute error was 9.45°±0.50° for the preferred arm and 9.37°±0.27° for the non-preferred arm. Further analysis showed that a significant simple main effect was found in shoulder abduction (F1,50=9.55, P=0.003) and wrist extension (F1,50=8.88, P=0.004). For shoulder and elbow flexion, no significant difference was found in absolute error for using the preferred or non-preferred arm. However, using the non-preferred arm to match shoulder abduction (0°–60°) and the preferred arm to match wrist extension (0°–50°) resulted in greater accuracy than using the other arms.
Discussion
We examined proprioceptive and kinesthetic accuracy in healthy older adults using arm matching position and motion tests. Based on our results, the subjects demonstrated greater accuracy in the motion matching tasks; wrist joint was less sensitive than proximal joint. The difference between preferred and non-preferred arms was inconsistent among joint angles.
Current findings indicate that the mean absolute error was reduced in the motion matching test compared to the position matching test, consistent with a previous study.Citation33 The discrepancy in proprioceptive accuracy between task types could be due to the proprioceptive information used by each task. However, the method by which proprioceptive information was used during movement has yet been fully understood.Citation34 Previous research has shown that the CNS uses all available cues to complete a task.Citation34 One possible explanation is that the reference arm provided proprioceptive information to the CNS in both tasks but used it differently in position and motion matching tasks. Several studies have suggested that the right hemisphere is dominant in processing proprioception and kinesthesia and responsible for processing input from muscle spindles, especially in the primary motor area.Citation35,Citation36
In the position matching test, the proprioceptive inputs signaled the velocity and end position but subjects did not move the matching arm until the reference arm was placed at the given angle. However, in the motion matching test, the proprioceptive information signals served as “on-line” feedback in providing current status to the CNS to estimate the next state of the limb. By comparing current and predictive forthcoming status, an individual can monitor the performance during the trial and immediately adjust velocity and end position; therefore, proprioceptive accuracy can be elevated in the motion matching test.
Another possible explanation is that position and motion sense are two separate senses, generated from separate processing but having the same receptors.Citation37 Evidence from a muscle fatigue study suggests that significantly elevated errors occur only in the elbow position matching test and not in the motion matching test.Citation33 In another experiment, blindfolded subjects were required to repeat movements 70 times between two targets. Results showed that the hand position deviated but direction and distance did not.Citation38 These findings indicate that position and motion sense can be processed separately, and that position sense is affected more easily by muscle status (fatigue) and nature of the task (repeated movements) than motion sense. As a result, these findings could also explain why subjects in this study performed more accurately in the motion matching task than the position matching task.
Accuracy of the arm matching test at the shoulder and elbow joints was greater than that at the wrist joints in both position and motion matching tests; however, the difference in accuracy between the shoulder and elbow joints remains unclear. This finding concurs with that of Hall and McCloskey who measured the detection threshold of passive movements in shoulder, elbow, and finger joints.Citation28 An explanation for this discrepancy is that change in fascicle length per degree was greater in the proximal than distal portion of the muscle.Citation28 The joint was considered to be more sensitive in perceiving positions and motions, with more change in the muscle length per degree. Another explanation is that the CNS processed proprioceptive information from multiple joints and integrated interjoint dynamics when performing distal joint movements.Citation5 In the current study, we moved only one joint at a time. The group of muscles surrounding the proximal joint also sensed change at the distal portion and provided a stabilizing function. When moving the wrist joint, the subject must stabilize the proximal segment of the limbs to manipulate objects with the hands or fingers.
Furthermore, results from the computational study of Scott and Loeb showed a descending gradient from proximal to distal joints for position sense accuracy.Citation39 The authors proposed that the distribution of muscle spindles around each joint could explain differences in perception of position sense and commented on the relative importance of proximal joints in localizing the endpoint. The effect of gravity and sense of effort were unlikely explanations for the discrepancy in proprioceptive sensitivity, since most joint angles were measured in the sagittal plane under the influence of gravity and we attempted to minimize the influence of gravity to the greatest possible extent with our methodology. Additionally, each joint angle was passively moved by the experimenter, who minimized the sense of effort with the controlled and slow nature of the tested movements. Given these conditions, muscle spindles would be the primary proprioceptor to provide information for all joint angles. Our findings indicate that matching wrist extension 0°–50° was the least accurate joint angle in both position matching and motion matching tasks.
Detailed analyses showed that the difference between the preferred and non-preferred arm was intriguing in the arm position and motion matching tests. Previous research has found the non-preferred arm to be more accurate at performing target-matching tasks than the preferred arm when tasks require both memory and hemisphere transfer.Citation30,Citation40–Citation42 Our results did not show systematic limb asymmetry in proprioceptive and kinesthetic accuracy because we employed contralateral matching tasks without reliance on memory. In addition, most studies measured the upper extremity in the elbow and thumb joints; and, we did not have the results from shoulder and wrist joints to compare.Citation30,Citation40–Citation42 By contrast, results from vibration studies suggest that proprioceptive asymmetry in upper extremities is dependent on sex, matching hand, and handedness.Citation14 For right-handed subjects, studies have found that only males demonstrate significant proprioceptive asymmetry in motion matching tasks. In summary, asymmetric proprioceptive accuracy across limbs was task-dependent and findings were inconsistent and difficult to compare across different experimental protocols.
The accuracy of limb position sense is affected by many factors. First, the issued motor command has been shown to contribute to the ability to sense limb position.Citation43–Citation46 Gandevia et al first reported that the level of effort used in generation of the motor command is graded with the amount of position illusion of wrist displacement during hand paralysis.Citation43 In the current study, subjects actively moved the matching arm in the vertical plane during the position matching test to match the reference arm; therefore, the source of the position signal in the matching arm was a combination of inflow and outflow signals. Second, the effect of muscle history of the reference arm, such as muscle fatigue and conditioning might have generated a position matching error because of the initial status of the muscle spindles.Citation33,Citation45,Citation47 Previous studies have found that position matching errors increased when arms are supported by the experimenter, as in the current study;Citation45,Citation48 thus, the accuracy of our subjects might have been affected to a greater extent than subjects in other studies using unsupported tasks. Third, the status of the matching arm can influence the position matching error.Citation44,Citation49 Previous studies have focused on the effect of the reference arm for position matching tasks.Citation33,Citation43,Citation47 However, recent studies have suggested that the condition of the matching arm, such as arm stiffness and conditioning of the muscles, affects the error pattern in the proprioceptive tasks.Citation44,Citation49 Finally, the effect of gravity could result in a proprioceptive illusion.Citation50 Ansems et al reported that performing position matching tasks with a relaxed arm in the horizontal plane leads to similar results as performing the task in the vertical plane with the arm supported.Citation47 Current protocols combined position matching tasks in the horizontal plane with relaxed arms, and in the vertical plane with the arms supported; therefore, the major proprioceptive signal is from the muscle spindles and measurements from the four selected joint angles are comparable.Citation47
To ensure the reliability and reproducibility of these results, proper training is required for clinical practitioners to perform the assessment. This is primarily because previous research has shown poor inter-rater reliability for sensory assessment.Citation7 Although standardized machine-based assessments have been developed to examine limb position quantitatively and have shown good inter-rater and test-retest reliability in stroke patients, they are not widely available in clinics.Citation19,Citation20 Moreover, proprioception has been reported as the main type of somatosensory assessment applied in clinical practice and upper extremities were the most tested body areas.Citation51 Therefore, combining training for clinical practitioners and assistance from a standardized device could minimize the measurement bias to obtain reliable results for clinical practice.
Conclusion
To the best of our knowledge, this is the first study to examine the suitability of using arm matching position and motion tests performed manually by a therapist. Because these tests are commonly used to measure position and motion sense accuracy in clinics, establishing standardized protocols is necessary for evidence-based practice. The results of this study are comparable to those of previous studies that used machine-generated kinesthetic stimuli. The manual measurement of accuracy of position and motion sense in clinical settings can be an effective screening tool; however, therapists must be properly trained. Although previous studies have examined detection thresholds for the upper extremities, they used customized machines to provide consistent stimuli. Most studies measured only the accuracy in perceived elbow angular displacement in the transverse plane. The machines, which are expensive and not available in every clinical setting, may be unsuitable for clinical use. Furthermore, measuring proprioceptive accuracy in the elbow joint only does not provide sufficient information to therapists for development of a treatment plan. Future studies are necessary to establish standardized testing procedures and to verify the reliability and validity of the arm position and motion matching tests for evidence-based practice in clinics.
Clinical implications
During movement planning and execution, proprioception that provides movement and position information of needed segments is essential to the CNS for taking into account all body segments involved in the desired task.Citation52 An adequate assessment of proprioceptive and kinesthetic accuracy can provide further insights into implementing a treatment plan. After proper training, clinical practitioners can gather preliminary information on an individual’s accuracy of position and motion sense by manually performing the test, which is inexpensive and easily administered in a clinical setting. We hope that the results of the current study will add more evidence to enhance evidence-based practice.
Limitations
There are several limitations to our study. First, the ratio of men to women was uneven and this may have influenced results. Although there is no clear evidence to suggest that sex has an effect on proprioceptive accuracy, it should be investigated in future studies. Second, we applied testing protocols only to healthy adults. Potential applications for patients with neurological disorders should be further explored. Third, most joint angles were tested in the sagittal plane (the exception was shoulder abduction). Determining whether horizontal plane motion can generate similar findings requires further investigation. Finally, we only recruited right-handed subjects. Previous studies have reported that left-handed individuals do not display uniform brain activation patterns during execution of movement and processing of language.Citation53,Citation54 Determining the effect of handedness on arm matching position and motion tests warrants further examination.
Acknowledgments
This project was supported in part by grants from the National Science Council of Taiwan (NSC100-2410-H-182-015-MY2 and NSC102-2314-B-182-009-MY3) and the Healthy Aging Research Center at Chang Gung University (EMRPD1D0291, CMRPD1B0331).
Disclosure
The authors report no conflicts of interest in this work.
References
- SherringtonCSOn the proprio-ceptive system, especially in its reflex aspectBrain190729467482
- GentilucciMNegrottiADissociation between perception and visuomotor transformation during reproduction of remembered distancesJ Neurophysiol1994724202620307823116
- GentilucciMToniIChieffiSPavesiGThe role of proprioception in the control of prehension movements: a kinematic study in a peripherally deafferented patient and in normal subjectsExp Brain Res19949934835007957728
- SainburgRLGhilardiMFPoiznerHGhezCControl of limb dynamics in normal subjects and patients without proprioceptionJ Neurophysiol19957328208357760137
- SainburgRLPoiznerHGhezCLoss of proprioception produces deficits in interjoint coordinationJ Neurophysiol1993705213621478294975
- BentzelKAssessing abilities and capacities: sensationRadomskiMVTromblyLCALathamCATOccupational therapy for physical dysfunction6th edBaltimore, MarylandLippincott Williams & Wilkins2008212233
- LincolnNBCrowJLJacksonJMWatersGRAdamsSAHodgsonPThe unreliability of sensory assessmentsClinical Rehabilitation19915273282
- Juul-KristensenBLundHHansenKChristensenHDanneskiold-SamsoeBBliddalHTest-retest reliability of joint position and kinesthetic sense in the elbow of healthy subjectsPhysiother Theory Pract2008241657218300109
- GobleDJProprioceptive acuity assessment via joint position matching: from basic science to general practicePhys Ther20109081176118420522675
- GobleDJCoxonJPWenderothNVan ImpeASwinnenSPProprioceptive sensibility in the elderly: degeneration, functional consequences and plastic-adaptive processesNeurosci Biobehav Rev200933327127818793668
- O’SuilleabhainPBullardJDeweyRBProprioception in Parkinson’s disease is acutely depressed by dopaminergic medicationsJ Neurol Neurosurg Psychiatry200171560761011606670
- AdamoDEAlexanderNBBrownSHThe influence of age and physical activity on upper limb proprioceptive abilityJ Aging Phys Act200917327229319799100
- KaplanFSNixonJEReitzMRindfleishLTuckerJAge-related changes in proprioception and sensation of joint positionActa Orthop Scand198556172743984706
- AdamoDEMartinBJBrownSHAge-related differences in upper limb proprioceptive acuityPercept Mot Skills20071043 Pt 21297130917879664
- BarrackRLSkinnerHBCookSDHaddadRJJrEffect of articular disease and total knee arthroplasty on knee joint-position senseJ Neurophysiol19835036846876619913
- KonczakJLiKYTuitePJPoiznerHHaptic perception of object curvature in Parkinson’s diseasePLoS One200837e262518612466
- MaschkeMGomezCMTuitePJKonczakJDysfunction of the basal ganglia, but not the cerebellum, impairs kinaesthesiaBrain2003126Pt 102312232212821507
- PutzkiNStudePKonczakJGrafKDienerHCMaschkeMKinesthesia is impaired in focal dystoniaMov Disord200621675476016482525
- DukelowSPHerterTMMooreKDQuantitative assessment of limb position sense following strokeNeurorehabil Neural Repair201024217818719794134
- CareyLMOkeLEMatyasTAImpaired limb position sense after stroke: a quantitative test for clinical useArch Phys Med Rehabil19967712127112788976311
- SullivanJEHedmanLDSensory dysfunction following stroke: incidence, significance, examination, and interventionTop Stroke Rehabil200815320021718647725
- SemrauJAHerterTMScottSHDukelowSPRobotic identification of kinesthetic deficits after strokeStroke201344123414342124193800
- OldfieldRCThe assessment and analysis of handedness: the Edinburgh inventoryNeuropsychologia197191971135146491
- FolsteinMFFolsteinSEMcHughPR“Mini-mental state”. A practical method for grading the cognitive state of patients for the clinicianJ Psychiatr Res19751231891981202204
- Alt MurphyMSunnerhagenKSJohnelsBWillenCThree-dimensional kinematic motion analysis of a daily activity drinking from a glass: a pilot studyJ Neuroeng Rehabil200631816914057
- CirsteaMCLevinMFCompensatory strategies for reaching in strokeBrain2000123Pt 594095310775539
- MichaelsenSMLutaARoby-BramiALevinMFEffect of trunk restraint on the recovery of reaching movements in hemiparetic patientsStroke20013281875188311486120
- HallLAMcCloskeyDIDetections of movements imposed on finger, elbow and shoulder jointsJ Physiol19833355195336875893
- GobleDJBrownSHUpper limb asymmetries in the matching of proprioceptive versus visual targetsJ Neurophysiol20089963063307418436632
- GobleDJLewisCAHurvitzEABrownSHDevelopment of upper limb proprioceptive accuracy in children and adolescentsHum Mov Sci200524215517016043248
- WestlakeKPCulhamEGSensory-specific balance training in older adults: effect on proprioceptive reintegration and cognitive demandsPhys Ther200787101274128317636154
- ChinnSStatistics in respiratory medicine. 2. Repeatability and method comparisonThorax19914664544561858087
- AllenTJProskeUEffect of muscle fatigue on the sense of limb position and movementExp Brain Res20061701303816328298
- KerrGKWorringhamCJVelocity perception and proprioceptionAdv Exp Med Biol2002508798612171154
- HaguraNOouchidaYAramakiYVisuokinesthetic perception of hand movement is mediated by cerebro-cerebellar interaction between the left cerebellum and right parietal cortexCereb Cortex200919117618618453537
- NaitoERolandPEGrefkesCDominance of the right hemisphere and role of area 2 in human kinesthesiaJ Neurophysiol20059321020103415385595
- ProskeUGandeviaSCThe kinaesthetic sensesJ Physiol2009587Pt 174139414619581378
- BrownLERosenbaumDASainburgRLLimb position drift: implications for control of posture and movementJ Neurophysiol20039053105311814615428
- ScottSHLoebGEThe computation of position sense from spindles in mono- and multiarticular musclesJ Neurosci19941412752975407996193
- GobleDJBrownSHTask-dependent asymmetries in the utilization of proprioceptive feedback for goal-directed movementExp Brain Res2007180469370417297548
- GobleDJBrownSHDynamic proprioceptive target-matching behavior in the upper limb: effects of speed, task difficulty and arm/hemisphere asymmetriesBehav Brain Res2009200171419073219
- Riolo-QuinnLRelationship of hand preference to accuracy on a thumb-positioning taskPercept Mot Skills19917312672731945704
- GandeviaSCSmithJLCrawfordMProskeUTaylorJLMotor commands contribute to human position senseJ Physiol2006571Pt 370371016439427
- AllenTJAnsemsGEProskeUEffects of muscle conditioning on position sense at the human forearm during loading or fatigue of elbow flexors and the role of the sense of effortJ Physiol2007580Pt 242343417255167
- WinterJAAllenTJProskeUMuscle spindle signals combine with the sense of effort to indicate limb positionJ Physiol2005568Pt 31035104616109730
- GritsenkoVKrouchevNIKalaskaJFAfferent input, efference copy, signal noise, and biases in perception of joint angle during active versus passive elbow movementsJ Neurophysiol20079831140115417615137
- AnsemsGEAllenTJProskeUPosition sense at the human forearm in the horizontal plane during loading and vibration of elbow musclesJ Physiol2006576Pt 244545516873408
- ItaguchiYFukuzawaKEffects of arm stiffness and muscle effort on position reproduction error in the horizontal planePercept Mot Skills2012114375777322913018
- ItaguchiYFukuzawaKThe influence of the indicator arm on end point distribution in proprioceptive localization with multi-joint armsExp Brain Res20122221–2778822842910
- LacknerJRDiZioPAAspects of body self-calibrationTrends Cogn Sci20004727928810859572
- WinwardCEHalliganPWWadeDTCurrent practice and clinical relevance of somatosensory assessment after strokeClin Rehabil1999131485510327097
- HasanZStuartDGAnimal solutions to problems of movement control: the role of proprioceptorsAnnu Rev Neurosci1988111992233284440
- PujolJDeusJLosillaJMCapdevilaACerebral lateralization of language in normal left-handed people studied by functional MRINeurology19995251038104310102425
- VerstynenTDiedrichsenJAlbertNAparicioPIvryRBIpsilateral motor cortex activity during unimanual hand movements relates to task complexityJ Neurophysiol20059331209122215525809