
Abstract
Many patients with Alzheimer’s disease will develop agitation at later stages of the disease, which constitutes one of the most challenging and distressing aspects of dementia. Recently, nonpharmacological therapies have become increasingly popular and have been proven to be effective in managing the behavioral symptoms (including agitation) that are common in the middle or later stages of dementia. These therapies seem to be a good alternative to pharmacological treatment to avoid unpleasant side effects. We present a systematic review of randomized controlled trials (RCTs) focused on the nonpharmacological management of agitation in Alzheimer’s disease (AD) patients aged 65 years and above. Of the 754 studies found, eight met the inclusion criteria. This review suggests that music therapy is optimal for the management of agitation in institutionalized patients with moderately severe and severe AD, particularly when the intervention includes individualized and interactive music. Bright light therapy has little and possibly no clinically significant effects with respect to observational ratings of agitation but decreases caregiver ratings of physical and verbal agitation. Therapeutic touch is effective for reducing physical nonaggressive behaviors but is not superior to simulated therapeutic touch or usual care for reducing physically aggressive and verbally agitated behaviors. Melissa oil aromatherapy and behavioral management techniques are not superior to placebo or pharmacological therapies for managing agitation in AD. Further research in clinical trials is required to confirm the effectiveness and long-term effects of nonpharmacological interventions for managing agitation in AD. These types of studies may lead to the development of future intervention protocols to improve the well-being and daily functioning of these patients, thereby avoiding residential care placement.
Introduction
Dementia is one of the most prevalent diseases in older people and constitutes the largest global public health care challenge. According to the 2015 World Alzheimer Report data,Citation1 nearly 47 million people are living with dementia in 2015, a number that will nearly double every 20 years. Alzheimer’s disease (AD) is a specific form of dementia that causes as many as 50%–70% of all dementia cases.Citation2 Although cognitive impairment is the central symptom of AD, behavioral and psychological symptoms, such as agitation, often coexist and are a common cause of patient and caregiver distress, institutionalization, and impairment in quality of life.Citation3,Citation4 Frequencies of agitation between 13.0% and 50.4% have been reported across studies and settings,Citation5–Citation7 and these increase as the severity of dementia progresses. Agitation has been defined as “inappropriate verbal, vocal, or motor activity that is not explained by needs or confusion per se”.Citation8 Although there is no consensus regarding specific behaviors that integrate the concept,Citation4 clinicians have identified three subtypes of agitation as follows: physically nonaggressive behavior, aggressive behavior, and verbally agitated behavior.Citation9 Interestingly, there appears to be a relationship between agitation and unmet needs originated by a decreased ability to cope with environmental stimulation and to communicate these needs.Citation10
Pharmacological interventions have been traditionally used in the treatment of agitation, but many studies have documented adverse effects of sedative and antipsychotic drugs, such as worsening cognitive function, higher cerebrovascular side effects, longer hospitalizations, and increased mortality.Citation11 Thus, the use of a nonpharmacological approach as a first-line treatment for agitation in dementia patients has been increasingly recommended.Citation12,Citation13 Overall, well-conducted, evidence-based studies on nonpharmacological interventions are lacking. Nonpharmacological approaches address the contextual and/or psychosocial reasons for agitation and avoid the potentially negative side effects of pharmacological treatment. Interventions such as cognitive stimulation/training, behavioral interventions, physical exercise, therapeutic touch, aromatherapy, bright light therapy, music therapy, and multisensory stimulation have shown promising results in decreasing agitation and cognitive impairment in older adults with dementia.Citation14,Citation15
We performed a systematic review of randomized controlled trials (RCTs) focusing on the nonpharmacological management of agitation of AD patients, with the aim of making evidence-based recommendations about the use of specific intervention strategies. Previous systematic reviews on the topic have been published, including studies with dementia patients, but none of these studies analyzed their results according to dementia subtypes.Citation12,Citation14–Citation17 Because patients with different subtypes of dementia or different levels of cognitive impairment may present with different levels of agitation and respond differently to interventions, we specifically focused this review on AD patients aged 65 years and above.
This paper had three specific aims as follows: 1) to review the literature on nonpharmacological therapies used to manage agitation in older AD patients over the past 20 years, 2) to assess the specific effectiveness of each nonpharmacological therapy, and 3) to provide evidence-based recommendations about the use of specific therapies and future research on this topic. Exploring these aspects is clinically relevant and has important implications for health service planning.
Methods
Data sources and search strategy
A systematic review of the literature published during the past 20 years (January 1996 to June 2015) was performed. Four computerized electronic databases were searched, including PubMed, Web of Science, PsycINFO, and Scopus, using the following keywords for AD, agitation, and non-pharmacological therapy: randomized controlled trial, Alzheimer*, agitat*, agress*, non-pharmacological, non-drug therap*, acupuncture, aromatherapy, light therap*, massage, touch, music*, group exercise*, activities, snoezelen, multisensory stimulation, social contact*, environmental modification*, caregiver training, behavioral or behavioral management, psychosocial, reminiscence therap*, validation therap*, reality orientation, space retrieval, alternative therap*, intervention*, and staff training.
Two independent reviewers evaluated appropriateness of inclusion, and conflicts were discussed until a consensus was reached. In cases in which a consensus was not reached, a third reviewer was involved.
Inclusion and exclusion criteria
We included original scientific articles in English that met the following criteria: 1) Population: AD patients (65 years of age or older, or a mean age of at least 75 if no age ranges were provided). Studies were selected if they reported a validated or medical diagnosis of AD, and they were excluded if they included patients with other subtypes of dementia; 2) Intervention: nonpharmacological interventions aimed at managing agitated behaviors were included; 3) Type of experimental design: RCTs comparing agitation before and after interventions were included. In terms of the level of evidence, all studies were considered to be level 2 based on the Oxford Centre for Evidence-Based Medicine (CEBM) criteria;Citation18 4) Outcome: Only studies exploring nonpharmacological interventions for agitation as a primary outcome (measured quantitatively and with a validated scale) or studies including sufficient information to determine the effect of nonpharmacological intervention on agitation were included; 5) Type of study: Only original articles were included. Abstracts, reviews, descriptive studies, and studies based on the description of a protocol, as well as studies based on the perspective of the authors, books, short surveys, observational studies, comments on an article, and conference abstracts, were excluded.
Data extraction
Studies were synthesized according to the following characteristics: author and year, country, sample characteristics (age and sex), study design, level of cognitive impairment, type of intervention, agitation scale, and main findings. A narrative synthesis approach was performed to examine the results. Next, we made recommendations about the clinical use for each nonpharmacological intervention based on the main findings.
Results
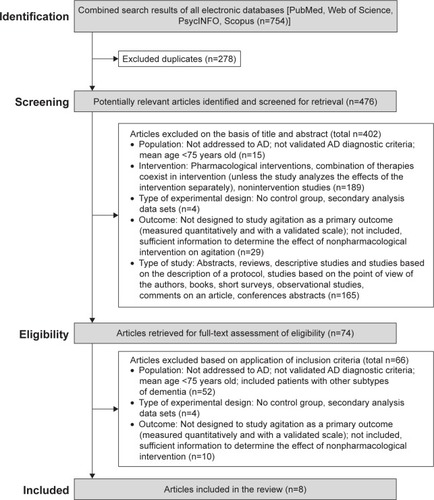
The review procedure is described in . As shown in the figure, a total of 754 studies were identified; after the removal of duplicates, 476 were considered potentially relevant and were screened for relevant content. From these studies, 402 were excluded on the basis of the title and abstract, and 74 were retrieved for full-text assessment. In the next phase, 66 were excluded based on the inclusion criteria. Finally, eight studies met the inclusion criteria for the review ().
Figure 1 Flowchart of systematic literature search.
Data synthesis
Studies’ characteristics
The characteristics of the studies are listed in . The eight studies that were included provided data on the effectiveness of music therapy (n=3),Citation19–Citation21 bright light therapy (n=2),Citation22,Citation23 aromatherapy (n=1),Citation24 therapeutic touch (n=1),Citation25 and psychological interventions with caregivers using behavioral management techniques (BMT) (n=1).Citation26
Table 1 Studies included in the review (n=8)
The sample size of the included studies ranged from 37Citation19 to 148Citation26 AD participants. Three studies were from Europe,Citation19,Citation21,Citation24 whereas three studies were from the United States,Citation22,Citation23,Citation26 one study was from Asia,Citation20 and one study was from Canada.Citation25 All studies except oneCitation26 included institutionalized AD patients in care homes. Two were multicenter studies.Citation24,Citation26
Of the eight included studies, four studiesCitation22–Citation24,Citation26 used the National Institute of Neurological and Communication Disorders and Stroke/Alzheimer’s Disease and Related Disorders Association (NINCDS/ADRDA) clinical criteria for AD,Citation27 whereas two studiesCitation19,Citation20 used the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) criteria for AD,Citation28 one studyCitation21 diagnosed AD according to International Classification of Diseases, Tenth Edition (ICD-10), and one studyCitation25 did not report to specific criteria, but the AD diagnosis was confirmed from the medical records of each patient.
Regarding the scales used to assess agitation, two studiesCitation19,Citation25 used the Cohen-Mansfield Agitation Inventory (CMAI),Citation9 which assesses the frequency of agitated behavior in a 7-point rating scale, with a higher score indicating more agitation. Two studiesCitation20,Citation21 used the Behavioral Pathology in Alzheimer’s Disease rating scale (BEHAVE-AD),Citation29 which covers behavioral symptoms in seven categories: paranoid and delusional ideations, hallucinations, activity disturbances, aggressiveness, diurnal rhythm disturbances, affective disturbances, and anxieties and phobias, with a higher score indicating more severity. One studyCitation23 used the Neuropsychiatric Inventory-Nursing Home (NPI-NH),Citation30 which assesses either ten or 12 behavioral disturbances common in dementia as follows: delusions, hallucinations, dysphoria, anxiety, agitation or aggression, euphoria, disinhibition, irritability or lability, apathy, aberrant motor activity, sleep and nighttime behavior disturbances, and appetite and eating changes, with a higher score indicating greater severity. In the study by Ancoli-Israel et al,Citation22 agitation was assessed both with the CMAICitation9 and the Agitated Behavior Rating Scale (ABRS).Citation31 The ABRS is a behavioral observation rating scale of the following five major behaviors: manual manipulation, restraint escape, searching or wandering, tapping or banging, and vocalization, with a higher score indicating more severity. In the study by Burns et al,Citation24 agitation was assessed using both the Pittsburg Agitation Scale (PAS)Citation32 and the NPI.Citation30 The PAS is a 16-item observational scale that rates the severity of agitation from 0 to 4 using the following four general behavior groups: aberrant vocalization, motor agitation, aggressiveness, and resisting, with a higher score indicating more agitation. In the study by Teri et al,Citation26 agitation was assessed with the CMAICitation9 and Agitated Behavior Inventory for Dementia (ABID).Citation33 The ABID consists of 16 items designed specifically to evaluate the frequency of common agitated behaviors and caregiver reactions in community-residing dementia patients. Most studiesCitation19,Citation22,Citation23,Citation25,Citation26 evaluated cognitive status by administering the Mini–Mental State Examination (MMSE).Citation34
Description of the studies
Studies were organized according to the types of nonpharmacological therapy, which are briefly described using Medical Subject Headings (MeSH) definitions.
Music therapy
Music therapy is the use of music as an adjunctive therapy in the treatment of neurological, mental, or behavioral disorders. Three studiesCitation19–Citation21 provided evidence of the effectiveness of music therapy for reducing agitation in institutionalized patients with moderately severe and severe AD. This result was particularly strong when the intervention included individualized (related to special positive memories of the participants) and interactive (including clapping, singing, and dancing) music.Citation20
One RCTCitation19 compared the short- and long-term effects of participative music and cooking interventions lasting 4 weeks and reported that both types of pleasant intervention decreased the severity of agitation measured using the CMAICitation9 and NPI.Citation30 The intervention group (n=18) received two 1-hour sessions a week of participatory music therapy (listening to music, singing, and playing percussion instruments), and the control group (n=19) received a cooking intervention (preparing a recipe). Importantly, in the music therapy group, the decrease in agitated behaviors was significant during the intervention (after the fourth session) but not at the end or at the follow-up evaluations (2 and 4 weeks after the intervention). Moreover, this study did not include a no-contact group to ensure that behavioral improvement did not result from increasing familiarity with the supervisor, who had no previous education in music therapy. Because the authors did not take into account individual music preferences, and the supervisor (psychologist) was not a qualified music therapist (and he/she was more comfortable in cooking), the benefit of music therapy observed in this study may have been reduced. Importantly, the improvement in agitation was stronger in the cooking intervention, suggesting that the observed benefits were not specific to musical interventions.
The other RCTCitation20 explored the long-term effects of passive (listening to music via a CD player) or interactive (including clapping, singing, and dancing) music therapy lasting 10 weeks using the BEHAVE-ADCitation29 and reported a higher, long-term reduction in behavioral symptoms in the interactive music group (n=13) compared with the passive music group (n=13) and no-music control group (n=13). Particularly, the scores of five items of the BEHAVE-AD were significantly reduced in the interactive group: paranoid and delusional ideations, activity disturbances, aggressiveness, affective disturbances, and anxieties and phobias; however, this effect disappeared 3 weeks after the music intervention, indicating the need for regularly conducted music interventions to maintain the beneficial effects. The music facilitators included two music therapists, four occupational therapists, and six nurses. Each intervention was performed once a week and lasted 30 minutes, and individualized music related to specific positive memories for each participant was selected.
In a case-control study,Citation21 a significant reduction was observed in activity disturbances, aggressiveness, and anxiety measured using the unpublished Icelandic version of the BEHAVE-ADCitation29 in a music therapy group during a 6-week period, although this effect had mostly disappeared 1 month later. In this study, the music intervention (n=20) was 30 minutes of music therapy delivered three times a week, whereas the control (n=18) was usual care. A qualified music therapist performed the intervention after the selection of a collection of songs familiar to the elderly. Each song was sung twice during the sessions, and every patient participated actively (singing, playing instruments, or dancing) or passively (holding the songbook and listening).
Bright light therapy
Light therapy is the exposure to light, particularly by variously concentrated light rays or specific wavelengths. Two studiesCitation22,Citation23 examined the efficacy of bright light therapy in decreasing agitated behaviors in AD patients, and these results showed that this therapy had little and possibly no clinically significant effects. One of the RCTsCitation22 including AD patients with significant agitation at baseline examined both caregiver perceptions of the agitated behavior using the CMAICitation9 and the direct observation of agitated behaviors using the ABRS.Citation31 The researchers found that increasing light exposure (2,500 lux) significantly decreased caregiver ratings of physical and verbal agitation after intervention, but caregiver ratings also decreased in the control group. They also reported that bright light had no significant effects on the observational ratings of agitation in any of the light-treatment groups, although morning bright light treatment delayed the timing (but not the strength) of agitation.Citation22 Importantly, they also observed a worsening of verbal agitation in the evening bright light group.
The other RCTCitation23 explored the effect of timed morning (n=29) or afternoon bright light (n=24) exposure at 2,500 lux for 1 hour daily compared with usual indoor light levels (n=17; 150–200 lux) in AD patients who experienced rest–activity disruption at baseline. They found a significant but clinically small worsening in agitation/aggression as measured with the NPI-NHCitation30 after 10 weeks of treatment, particularly in the morning-light group. Importantly, the nursing staff was not unaware of the experimental condition of the participants, and the effect of interrater variability on the observed results was impossible to determine in this study.
Aromatherapy
Aromatherapy is the use of fragrances and essences from plants to affect or alter a person’s mood or behavior and facilitate physical, mental, and emotional well-being. A multicenter, double-blind, placebo RCTCitation24 explored the effects of aromatherapy with Melissa officinalis oil in the treatment of agitation in institutionalized AD patients with a previous history of significant agitation, and found that intervention with Melissa oil (n=32) was not superior to placebo (n=31) or pharmacological therapy with donepezil (5 mg/day, n=31) after 4 or 12 weeks of treatment. Agitation was assessed by the PASCitation32 and NPI.Citation30 The application of Melissa oil occurred twice a day and involved massaging the oil into the hands and upper arms for 1–2 minutes. Given the substantial improvement in the placebo group, the authors emphasized the potential benefits of meeting regularly (touch and social interaction) with care staff in the management of agitation in AD patients.
Therapeutic touch
Therapeutic touch is an intentionally directed process during which the practitioner places his or her hands upon the person to be cured with the intent of spiritual energetic healing. One RCTCitation25 compared the effectiveness of therapeutic touch intervention (n=17), which was administered daily for 30–40 minutes for 5 consecutive days, with a simulated therapeutic touch intervention (n=16) and with usual care (n=18) in institutionalized AD patients with a previous history of agitated behaviors. The therapeutic touch intervention was conducted by nurses who had completed the advanced level of a therapeutic touch and healing program, and the simulated therapeutic touch intervention was conducted by nursing and health-related volunteer students. Agitation levels were measured at various times after treatment and then compared. Therapeutic touch was effective in reducing the frequency of physical nonaggressive behaviors (pacing, repetitious movements, and general restlessness) but was not superior to simulated therapeutic touch or usual care in reducing physically aggressive and verbally agitated behaviors. It is important to note, however, that a significant decrease in the number of all analyzed agitated behaviors was observed in the three groups from baseline to the end of intervention, although this reduction was significantly lower in the usual care group.
Psychological intervention with family caregivers
Psychological therapies imply the use of specific psychological techniques or approaches for the reduction of behavioral symptoms in dementia. One multicenter, placebo RCTCitation26 reported that a psychological intervention with family caregivers (spouses or adult relatives) by training in BMT (n=41) was not superior to pharmacological therapy with haloperidol (mean dose, 1.8 mg/d; n=34), trazodone (mean dose, 200 mg/d; n=37), or placebo (n=36) in reducing agitation in AD outpatients with a previous history of significant agitation and moderate-to-severe cognitive impairment, although it slightly reduced the incidence of adverse events such as bradykinesia and parkinsonian gait after 16 weeks of treatment. No long-term effects of the intervention were found at 3-, 6-, and 12-month follow-ups. In this study, the intervention was performed by expert therapists with master’s degrees and consisted of eleven structured sessions that provided information about AD strategies to decrease agitation, and structured in- and out-of-session assignments, including a videotaped training program. The treatment protocol was general due to the diversity of the participants, and the authors suggest that a more individualized BMT may have yielded better results.
Discussion
The purpose of this review was to identify and synthesize available research evidence on the efficacy of the nonpharmacological management of agitation in older adults with AD and to make evidence-based recommendations about the clinical use of different interventions in this population. The focus on AD is relevant, because the treatment effects on agitation may be different depending on the subtype and the severity of dementia. There is also evidence of more agitation in patients with AD than in patients with vascular dementia or other types of dementia.Citation35
Effective nonpharmacological therapies to manage agitation in AD
On the basis of the methodological quality of the three included studies exploring the effectiveness of music therapy in AD,Citation19–Citation21 we concluded that music therapy performed by qualified music therapists is an optimal intervention in institutionalized AD patients. The effectiveness of this type of therapy in reducing agitated behaviors has been reported in previous systematic reviews with dementia patients,Citation14,Citation15,Citation17,Citation36–Citation38 particularly when based on individual music choices and when complemented by group interventions. Thus, it appears that music therapy is effective for managing agitation in institutionalized dementia patients, potentially because it can engage interest and provides an opportunity for social interaction.
It is important to note that in the three studies, agitated behaviors returned to baseline levels at follow-up, suggesting that music therapy interventions must be implemented on a long-term basis to maintain their beneficial effects. Moreover, the long-term benefits of music therapy remain unclear and require further investigation.
One of the three studiesCitation19 included participants with some previous agitation, whereas the other two studiesCitation20,Citation21 did not clearly report the previous history of agitation. Thus, the effect of music therapy in AD patients with severe baseline agitation has not been specifically investigated.
Low number and variability among the included studies makes it difficult to identify the most effective duration and frequency of the music intervention. The researchers completed therapy over several weeks (4–10 weeks), with the sessions lasting 30–60 minutes and occurring 1, 2, or 3 times a week; thus, a minimum of 30 minutes of interactive and individualized music therapy twice a week appears reasonable in AD patients. The three trials were small; thus, to strengthen the above evidence, future studies should include larger samples. Finally, it is important to note that the sample was predominantly female, making it difficult to explore differences between the sexes with respect to the effectiveness of music therapy.
Nonpharmacological therapies requiring more research
The inconclusive results of the two studies exploring the effectiveness of bright light therapyCitation22,Citation23 and the fact that it may slightly worsen symptomatic agitation indicate that future research is necessary to examine the actual effect of bright light exposure on agitated behaviors in AD patients.
The study by Burns et alCitation24 provided strong evidence indicating that there is no benefit for aromatherapy with Melissa oil in the management of agitation in AD, at least over a 12-week period of intervention. Consistent with this finding, a recent systematic reviewCitation39 of RCTs including dementia patients of any type and severity reported equivocal benefits with aromatherapy.
Regarding the effectiveness of therapeutic touch, the results obtained by Hawranick et alCitation25 provided evidence of the modest potential for this therapy in treating agitated but not physically aggressive behaviors in AD patients with severe cognitive impairment, but additional research is required to obtain evidence about its long-term effects because it constitutes an inexpensive method that can be implemented by family caregivers or staff.
Regarding psychological interventions involving training of family caregivers to use BMT, the study by Teri et alCitation26 provides strong evidence of modest and comparable reductions in agitation with placebo and active treatments (both pharmacological and nonpharmacological), suggesting that training family caregivers with this technique is not an optimal clinical alternative for the management of agitation in AD outpatients.
Consistent with these findings, a recent systematic review found inconclusive evidence regarding the efficacy of these therapies in improving agitation in dementia and recommended further research on the topic.Citation15
Challenges and solutions
Optimal management of agitation in AD constitutes a major clinical challenge to avoid or delay institutionalization and to improve quality of life for patients and caregivers. On the basis of the present literature review, there are some questions that merit further investigation. First, there is insufficient evidence in the literature about the effectiveness of nonpharmacological therapies in noninstitutionalized AD patients and the long-term effects of these interventions. Future studies in home and community settings are particularly relevant to determine if nonpharmacological therapies can delay or avoid residential care placement. Second, all included studies implemented interventions in AD patients with significant cognitive impairment, but the benefits of nonpharmacological therapy on patients with milder forms of AD may be underestimated. Third, future studies should include a detailed description of the previous history of agitation to distinguish between spontaneous or reactive agitation. Indeed, in our opinion, the identification of the underlying causes (and biological mechanisms) and the severity of agitation in AD patients is crucial and may assist clinicians and researchers in designing effective nonpharmacological interventions. AD patients usually present multiple comorbidities that may act as behavioral risk factors, and these can have an important impact on the effectiveness of the nonpharmacological therapies. Evaluating for their presence and addressing them is equally important to implement personalized interventions for agitation management.
Given the limited evidence currently available regarding the efficacy of nonpharmacological therapies to manage agitation in AD, there is a strong need for further and more rigorous research. In recent years, multisensory stimulation (MSS) has become a commonly used approach to manage behavioral disturbances and to promote positive mood in dementia patients. MSS actively stimulates the senses of hearing, touch, vision, and smell in an individual-oriented, nonthreatening environment. It is intended to provide individualized, sensory stimulation without the need for higher intellectual activity to achieve or maintain a state of well-being and may be useful in the management of agitation in AD. In previous studies and reviews, it has been demonstrated that MSS produces immediate or short-term positive effects on behavior and mood.Citation38,Citation40–Citation46 Future studies are required to assess its effectiveness in this dementia subtype.
Importantly, in the present study, we included only RCTs; it was recently suggested that this likely excludes potent interventions in dementia patients, which limits conclusions.Citation36 Finally, we would like to highlight that although we have made some recommendations providing valuable practical information about the optimal management of agitation in AD patients based on the level of evidence of the reviewed studies, these recommendations are not definitive because clinicians should take into consideration the specific characteristics of their patients or alternative/complementary treatments before using a specific intervention.Citation47
Conclusion
This review found that music therapy is an effective nonpharmacological intervention for reducing agitation in institutionalized AD patients, particularly when the intervention implies individualized and interactive music. However, more evidence regarding the long-term effects of this therapy is needed. Bright light therapy has little and potentially no clinically significant effects on agitation levels. Therapeutic touch is effective for reducing physical nonaggressive behaviors but is not superior to simulated therapeutic touch or usual care in reducing physically aggressive and verbally agitated behaviors. Melissa aromatherapy and BMT do not appear to be superior to pharmacological therapies or placebo in managing agitation in AD patients; more evidence about their effects on agitation is needed to make definitive clinical recommendations. In general, there is a severe paucity of research into the effects of nonpharmacological therapies in managing agitation in older AD patients.
Author contributions
JCM made the conception of the study and design. CD and BA developed the search strategies, independently screened the title and abstracts of the 754 articles extracted from the literature search, applied the inclusion/exclusion criteria, and retrieved the full electronic text of the eight selected articles. LL and BA extracted the relevant data from the selected articles (independently). LL, BA, and JCM drafted the manuscript. AM and IG provided feedback on the protocol during its development and edited the manuscript. All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work. All authors read and approved the final version of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
- Alzheimer’s Disease International (AZ)World Alzheimer Report 2015London, UKAlzheimer’s Disease International2015 Available from: http://www.alz.co.uk/research/WorldAlzheimerReport2015.pdfAccessed September 28, 2015
- QuiuCKivipeltoMStraussEEpidemiology of Alzheimer’s disease: occurrence, determinants, and strategies toward interventionDialogues Clin Neurosci20091111112819585947
- HayDPKleinTTHayLKGrossbergGTKennedyJSAgitation in Patients with Dementia: A Practical Guide to Diagnosis and Management1st edWashington, DCAmerican Psychiatric Publishing2003
- KongEAgitation in dementia: concept clarificationJ Adv Nurs20055252653616268859
- KvernoKSRabinsPVBlassDMHicksKBlackBSPrevalence and treatment of neuropsychiatric symptoms in hospice-eligible nursing home residents with advanced dementiaJ Gerontol Nurs20083481719112999
- OkuraTPlassmanBLSteffensDCLlewellynDJPotterGGLangaKMPrevalence of neuropsychiatric symptoms and their association with functional limitations in older adults in the United States: the aging, demographics, and memory studyJ Am Geriatr Soc20105833033720374406
- SteinbergMShaoHZandiPPoint and 5-year period prevalence of neuropsychiatric symptoms in dementia: the Cache County studyInt J Geriatr Psychiatry20082317017717607801
- Cohen-MansfieldJBillingNAgitated behaviors in the elderly. I. A conceptual reviewJ Am Geriatr Soc1986347117213531296
- Cohen-MansfieldJMarxMSRosenthalASA description of agitation in a nursing homeJ Gerontol198944M77M842715584
- Cohen-MansfieldJDakheel-AliMMarxMSTheinKRegierNGWhich unmet needs contribute to behavior problems in persons with advanced dementia?Psychiatry Res2015228596425933478
- SchneiderLSDagermanKInselPSEfficacy and adverse effects of atypical antipsychotics for dementia: meta-analysis of randomized, placebo-controlled trialsAm J Geriatr Psychiatry20061419121016505124
- OlazaránJReisbergBClareLNonpharmacological therapies in Alzheimer’s disease: a systematic review of efficacyDement Geriatr Cogn Disord20103016117820838046
- PanzaFSolfrizziVSeripaDProgresses in treating agitation: a major clinical challenge in Alzheimer’s diseaseExpert Opin Pharmacother2015161825387541
- LivingstonGKellyLLewis-HolmesEA systematic review of the clinical effectiveness and cost-effectiveness of sensory, psychological and behavioural interventions for managing agitation in older adults with dementiaHealth Technol Assess201418391226
- LivingstonGKellyLLewis-HolmesENon-pharmacological interventions for agitation in dementia: systematic review of randomised controlled trialsBr J Psychiatry201420543644225452601
- KongEEvansLKGuevaraJPNonpharmacological intervention for agitation in dementia: a systematic review and meta-analysisAging Ment Health20091351252019629775
- StaedtlerAVNunezDNonpharmacological therapy for the management of neuropsychiatric symptoms of Alzheimer’s disease: linking evidence to practiceWorldviews Evid Based Nurs20151210811525809879
- OCEBM Levels of Evidence Working GroupThe Oxford 2011 Levels of EvidenceOxford Centre for Evidence-Based Medicine Available from: http://www.cebm.net/index.aspx?o=5653Accessed September 28, 2015
- NarmePClémentSEhrléNEfficacy of musical interventions in dementia: evidence from a randomized controlled trialJ Alzheimers Dis20143835936923969994
- SakamotoMAndoHTsutouAComparing the effects of different individualized music interventions for elderly individuals with severe dementiaInt Psychogeriatr20132577578423298693
- SvansdottirHBSnaedalJMusic therapy in moderate and severe dementia of Alzheimer’s type: a case-control studyInt Psychogeriatr20061861362116618375
- Ancoli-IsraelSMartinJLGehrmanPEffect of light on agitation in institutionalized patients with severe Alzheimer diseaseAm J Geriatr Psychiatry20031119420312611749
- DowlingGAGrafCLHubbardEMLuxenbergJSLight treatment for neuropsychiatric behaviors in Alzheimer’s diseaseWest J Nurs Res20072996197517596638
- BurnsAPerryEHolmesCA double-blind placebo-controlled randomized trial of Melissa officinalis oil and donepezil for the treatment of agitation in Alzheimer’s diseaseDement Geriatr Cogn Disord20113115816421335973
- HawranikPJohnstonPDeatrichJTherapeutic touch and agitation in individuals with Alzheimer’s diseaseWest J Nurs Res20083041743418272750
- TeriLLogsdonRGPeskindETreatment of agitation in AD: a randomized, placebo-controlled clinical trialNeurology2000551271127811087767
- McKhannGDrachmanDFolsteinMKatzmanRPriceDStadlanEMClinical diagnosis of Alzheimer’s disease: report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer’s DiseaseNeurology1984349399446610841
- American Psychiatric AssociationDiagnostic and Statistical Manual of Mental Disorders, (DSM-IV)4th edWashington, DCAmerican Psychiatric Association1994
- ReisbergBBorensteinBSalobSPFerrisSHFranssenEGeorgotasABehavioral symptoms in Alzheimer’s disease: phenomenology and treatmentJ Clin Psychiatry1987489153553166
- CummingsJLMegaMGrayKRosenberg-ThompsonSCarusiDAGombeinJThe neuropsychiatric inventory: comprehensive assessment of psychopathology in dementiaNeurology199444230823147991117
- BliwiseDLLeeKADevelopment of an agitated behavior rating scale for discrete temporal observationsJ Nurs Meas199311151247850494
- RosenJBurgioLKollarMThe Pittsburg Agitation Scale: a user friendly instrument for rating agitation in dementia patientsAm J Geriatr Psychiatry19942525921629007
- LogsdonRGTeriLWeinerMFAssessment of agitation in Alzheimer’s disease: the agitated behavior in dementia scale. Alzheimer’s disease cooperative studyJ Am Geriatr Soc1999471354135810573447
- FolsteinMFolsteinSEMcHughPRMini-mental state: a practical method for grading the cognitive state of patients for the clinicianJ Psychiatr Res1975121891981202204
- ZuidemaSKoopmansRVerheyFPrevalence and predictors of neuropsychiatric symptoms in cognitively impaired nursing home patientsJ Geriatr Psychiatry Neurol200720414917341770
- Cohen-MansfieldJNon-pharmacological interventions for agitation in dementia: various strategies demonstrate effectiveness for care home residents; further research in home settings is neededEvid Based Nurs20161913125990080
- ForbesDAPeacockSMorganDNonpharmacological management of agitated behaviours associated with DementiaGeriatr Aging2005842630
- LivingstonGJohnstonKKatonaCPatonJLyketsosCGOld Age Task Force of the World Federation of Biological PsychiatrySystematic review of psychological approaches to the management of neuropsychiatric symptoms of dementiaAm J Psychiatry20051621996202116263837
- ForresterLTMaayanNOrrellMSpectorAEBuchanLDSoares-WeiserKAromatherapy for dementiaCochrane Database Syst Rev20142CD00315024569873
- BakerRHollowayJHoltkampCCEffects of multi-sensory stimulation for people with dementiaJ Adv Nurs20034346547712919265
- CollierLMcPhersonKEllis-HillCStaalJBucksRMultisensory stimulation to improve functional performance in moderate to severe dementia-interim resultsAm J Alzheimers Dis Other Demen20102569870321131677
- MasedaASánchezAMaranteMPGonzález-AbraldesIBujánAMillán-CalentiJCEffects of multisensory stimulation on a sample of institutionalized elderly people with dementia diagnosis: a controlled longitudinal trialAm J Alzheimers Dis Other Demen20142946347324604894
- MasedaASánchezAMaranteMPGonzález-AbraldesIde LabraCMillán-CalentiJCMultisensory stimulation on mood, behavior, and biomedical parameters in people with dementia: is it more effective than conventional one-to-one stimulation?Am J Alzheimers Dis Other Demen20142963764724792708
- SánchezAMillán-CalentiJCLorenzo-LópezLMasedaAMultisensory stimulation for people with dementia: a review of the literatureAm J Alzheimers Dis Other Demen20122871423221029
- SánchezAMarante-MoarMPSarabiaCMultisensory stimulation as an intervention strategy for elderly with severe dementia: a pilot randomized controlled trialAm J Alzheimers Dis Other Demen Epub1212015
- StaalJASacksAMatheisRThe effects of Snoezelen (multi-sensory behavior therapy) and psychiatric care on agitation, apathy, and activities of daily living in dementia patients on a short term geriatric psychiatric inpatient unitInt J Psychiatry Med20073735737018441625
- HowickJChalmersIGlasziouPThe 2011 Oxford CEBM Evidence Levels of Evidence (Introductory Document)Oxford Centre for Evidence-Based Medicine Available from: http://www.cebm.net/index.aspx?o=5653Accessed September 28, 2015