
Abstract
Background and purpose
Musculoskeletal system deterioration among the aging is a major reason for loss of autonomy and directly affects the quality of life of the elderly. Articular evaluation is part of physiotherapeutic assessment and helps in establishing a precise diagnosis and deciding appropriate therapy. Reference instruments are valid but not easy to use for some joints. The main goal of our study was to determine reliability and intertester reproducibility of the MP-BV, an inertial sensor (the MotionPod® [MP]) combined with specific software (BioVal [BV]), for elbow passive range-of-motion measurements in geriatrics.
Methods
This open, monocentric, randomized study compared inertial sensor to inclinometer in patients hospitalized in an acute, post-acute, and long-term-care gerontology unit.
Results
Seventy-seven patients (mean age 83.5±6.4 years, sex ratio 1.08 [male/female]) were analyzed. The MP-BV was reliable for each of the three measurements (flexion, pronation, and supination) for 24.3% (CI 95% 13.9–32.8) of the patients. Separately, the percentages of reliable measures were 59.7% (49.2–70.5) for flexion, 68.8% (58.4–79.5) for pronation, and 62.3% (51.2–73.1) for supination. The intraclass correlation coefficients were 0.15 (0.07–0.73), 0.46 (0.27–0.98), and 0.50 (0.31–40 0.98) for flexion, pronation, and supination, respectively.
Conclusion
This study shows the convenience of the MP-BV in terms of ease of use and of export of measured data. However, this instrument seems less reliable and valuable compared to the reference instruments used to measure elbow range of motion in gerontology.
Introduction
Musculoskeletal system deterioration among the aging is a major reason for loss of autonomy and directly affects the quality of life of the elderly.Citation1–Citation3 In this context, physiotherapeutic assessment helps in evaluating elderly patient deficiencies and thus in planning an appropriate rehabilitation program. Articular evaluation is part of this assessment and allows joint deviation quantification, identification of orthopedic deformities, observation of painful events, and follow-up of progress made by patients. It also helps in establishing a precise diagnosis and deciding appropriate therapy.Citation4
An essential stage of this evaluation is the measurement of joint angles. Within a clinical setting, physiotherapists do have technical references: the goniometer and inclinometer are valid instruments;Citation5–Citation7 however, positioning of these tools is not easy with some joints.Citation8–Citation10 Other techniques are also used in tests: the meter ribbon (easy use for estimating improvement in range of motion [ROM] but not adapted to a unique assessment) and visual assessment (often practiced in clinical tests but subjective and not entirely replicable).Citation11,Citation12 It seemed necessary to find an instrument that would allow a combination of all the assets of those reference techniques – that is, an instrument that is reliable and replicable but also simple, fast, and easy to use.
Actigraphy is a technique for measuring locomotive activity. Traditionally, actimeters were composed of single piezoelectric accelerometers worn on the waist.Citation13 With the improvement of technology in the past 30 years, actimeters have become more precise (with multiple piezoelectric accelerometers) and the position of wear has been diversified (wrist, chest, hip) in response to new applications.Citation14 Several practical applications of actigraphy have been proposed, such as assessment of hyperactivity in childrenCitation15,Citation16 and behavioral disorders among patients suffering from dementia;Citation17,Citation18 ecological assessment of daily living activities;Citation19 assessment of sedative effects of some drugs;Citation20 and screening for certain sleep problems.Citation21–Citation23 However, the actigraph can also be used for measurement of articular ROM. Indeed, the actigraph, in combination with specific software, is used as an inertial sensor for measurement of lower limb articulationsCitation24–Citation27 but also for cervical spine.Citation28
The main goal of the present study was to determine reliability, with an inclinometer as reference, and intertester reproducibility of an actigraph that uses an inertial sensor (the MotionPod®; Movea SA, Grenoble, France) associated with specific software (BioVal; RM Ingénieurie, Groupe Cegedim, Rodez, France) for obtaining elbow passive ROM measurements in geriatrics. In this study, we also evaluated the duration of examination and the acceptability of the instrument according to the patient and the physiotherapist. From this point onward, we shall use the term “MP-BV” to define the actigraph/software coupling.
Methods
Location and subjects
This open, monocentric, randomized study (NCT1462760) took place from October 1, 2011 to May 1, 2012. Patients were recruited within the acute, post-acute, and long-term-care gerontology unit of University Hospital of Nice (Nice, France). The study was approved by the South Mediterranean V Ethical Review Board (Comité de Protection des Personnes Sud Méditérrannée V), as well as by the French Agency for the Safety of Health Products (ANSM). Patients who agreed to participate gave their written informed consent.
Included patients were 65 years or older and had received a physiotherapy prescription from the physiotherapists of Department of Geriatrics mentioning the need for a passive joint assessment. Patients who agreed to participate had to be covered by social insurance. Exclusion criteria were: patients suffering from a pathology for which heating of joints was contraindicated; patients wearing a pacemaker, a metallic prosthesis, or osteosynthesis equipment located less than 10 cm from the captor; patients incapable of maintaining a straight wrist position and/or a neutral shoulder position; and patients having a joint deviation in flexion, extension, pronation or supination of less than 20°.
Recruitment and randomization
Patients were pre-recruited during weekly physiotherapy sessions at the Department of Geriatrics. Due to organizational constraints, a maximum of six patients per week were included. An explanation of the study and an associated pamphlet were given to the patients by the physician responsible for the study, with a 7-day retraction delay. The inclusion visit began with signing of consent and was led by the physician after those 7 days.
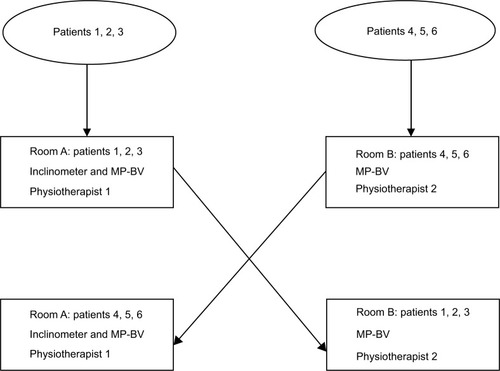
At the end of the inclusion visit, an inclusion form was completed by the physician. This form included the first and last name of the patient and the confirmation of all inclusion and non-inclusion criteria. Then, this form was forwarded to a clinical research assistant of the Clinical Research and Innovation Department (DRCI), who randomly assigned the patients. The randomization was centralized at the methodological center and done in a 1:1 ratio. The generation of the allocation sequence was made with number permutation tables in block sizes of six. Consequently, among six patients, three were allocated to room A and three were allocated to room B, and so on. All patients were examined successively in both rooms. Furthermore, in room A, the running order on both instruments (MP-BV and inclinimeter) was also randomized. Physiotherapists were also randomly assigned to room A or B ().
Figure 1 Randomization process.
Materials used for the measures
The MotionPod is a patented hardware solution for motion sensing that features a state-of-the-art miniaturized motion-sensing microelectromechanical system. It contains three-axis accelerometers, three-axis magnetometers, and three-axis gyroscopes in a compelling form factor the size of a standard wristwatch (33×21×15 mm [1.3×0.8×0.6″]) and weighs 14 g (0.5 oz). The battery was a 150 mAh Li-ion polymer technology battery with a battery life of 6 hours and a charging duration of 2–3 hours (500 charging cycles). The device is worn by a patient by way of a bracelet attached to the mechanical interface. The sampling rate for accelerometers, gyroscopes, and magnetometers was adjustable between 25 and 200 Hz with 12-bit resolution. The information from the MotionPod was transferred via radio waves to the MotionPod controller, which was linked to a computer with a USB cable. The wireless band ranged from 10 m (30 feet) to 30 m (100 feet), depending on the environment, with a frequency band of 2.4 Ghz. The measurement range was a full 360°. The fusion of data from accelerometers, magnetometers, and gyroscopes was done with an application programming interface developed by Movea. Then, data were delivered by the BioVal software to the practitioner as yaw, pitch, roll, quaternion, or rotation matrix. The resolution was 0.5° for static accuracy and 1° for dynamic accuracy.
The inclinometer used as reference was the Baseline® Bubble inclinometer (Fabrication Enterprises, Withe Plains, NY, USA), the dimensions of which were 101.6×5.08×101.6 mm (4×0.2×4″) for 90.72 g (0.2 lbs). For the measure, the inclinometer was placed near the elbow. The physiotherapist turned the dial until the scale read 0, then took the elbow through its range of motion. Finally, the range was read directly from the dial.
Experimentation process
Experimentation was performed in the Physiotherapy Unit of the Gerontology Department over one half-day per week. A training session on both instruments used in this study was held by physiotherapists before the study began so that all four investigators had the same level of knowledge regarding the use of the MP-BV. No physiotherapist had had any experience with any inertial sensor before the training sessions.
Measurements were made on the elbow joint, as it allows good validity and intertester reproducibility.Citation5 Physiotherapists successively measured flexion, pronation, and supination. In room A, experimentation included measurement with the MP-BV as well as with the inclinometer. The screen displaying the result was hidden from the physiotherapist so as not to influence the inclinometer measurement. In room B, the experiment included a measurement with the MP-BV, in order to assess intertester reliability. Considering that inclinometer was the instrument of reference, only one measure was taken. For MP-BV two measures were taken for each patient to assess intertester reliability, which were performed by different physiotherapists for each measure.
When the passive elbow flexion was measured, the arm was placed vertically and the forearm was placed in supination in the same straight line as that formed by the arm. The inclinometer was placed on the longitudinal axis of the mobile segment, on the dorsal surface, and on the middle of the forearm. For this measurement, we used two MotionPod devices; the first one, fixed on the wrist, measured the joint angle, and the second one, on the arm, was used as reference positioning ().
Figure 2 Positioning of the actimeters.
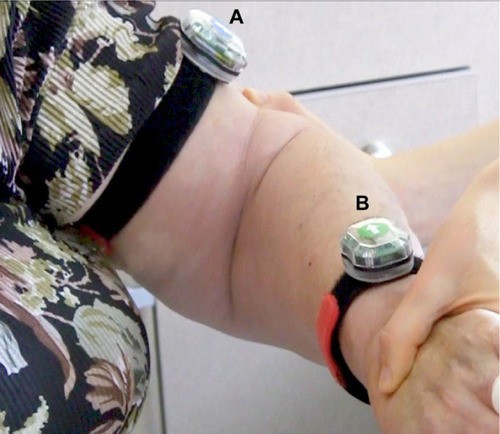
Regarding pronosupination, the arm was placed vertically; the forearm was placed horizontally with the palm of the hand up, the thumb upward, and the longitudinal axis of the third metacarpus in the same axis as the forearm. The inclinometer was positioned on the dorsal face of the wrist and the MotionPod the motion pod was positioned on the external face of the wrist.
Variables studied
Measurement reliability
Passive elbow ROM measurements expressed in degrees and obtained with the MP-BV were compared to those obtained with an inclinometer for all three of the movements (flexion, pronation, and supination). We excluded elbow extension because the articular deviation of this joint is inferior to 10°, which is inferior to the variability accepted between the two techniques. A 10° scope of error is acceptable for goniometric measurements.Citation29 Consequently, we considered as reliable a measure with the MP-BV with a difference of less than 10° of the measure obtained with the inclinometer. The percentage of reliable measure was calculated in this way for each movement.
Intertester reproducibility
Intertester reproducibility was assessed through two series of passive ROM measurements conducted with the MP-BV by two researchers. For each of the three movements, intertester reproducibility of MP-BV measurement was evaluated by calculating the intraclass correlation coefficient (ICC).Citation30 Reproducibility was also evaluated through the rates of concordant measures with both techniques (less than 10° difference between the measures) for each movement.
Duration of examination
The durations of examination (in seconds) obtained with both instruments were compared. Duration was defined as the time at which the patient was ready for examination until the time at which the data were recorded in the patient’s file.
Acceptability
The patient rated the comfort of the measurement process for both instruments using a ten-point visual analog scale (VAS). Meanwhile, each physiotherapist rated his acceptance of the instruments using a 10-point VAS, as well as the ease of use and of data exporting of both instruments.
Statistical analysis
It was decided a priori that MP-BV would be considered a reliable measurement technique if the three joint angles from at least 90% of patients had less than 10° error when compared to the inclinometer. Considering the assumption that 95% of patients would have a valid measure, it was necessary to include 73 patients so that the lower limit of the 95% confidence interval (CI) would be above 90%. To account for potential measurement failures, the decision was made to include 84 patients.
First, a descriptive analysis was made by the biostatistician from the DRCI of Nice University Hospital. Results were presented as mean ± standard deviation for quantitative variables and percentage for qualitative variables. The percentage of patients with a valid global assessment was calculated and presented with the corresponding 95% CI as well as percentages of reliable measurements for each movement (flexion, pronation, supination). An ICC value <0.40 was considered poor, 0.40–0.50 moderate, 0.50–0.70 good, and 0.70–1.0 excellent.Citation31 Examination duration was compared between the two techniques using the Student’s t-test for paired data. For this analysis, only data recorded in room A were used, as examinations were performed there with both techniques and by the same physiotherapist. Finally, for acceptability analyses, VAS scores (recorded in room A) were compared using the Student’s t-test for paired data. All the tests were two-sided and the significance level was set to 5%. Statistical analyses were performed using SAS Enterprise Guide (v 4.1; SAS Institute Inc., Cary, NC, USA).
Results
Three hundred and fifteen patients were screened during weekly physiotherapy sessions. Of these, 84 patients were deemed eligible for inclusion in the study, and 77 of these 84 (91.7%) were eventually included in the validation study ().
Figure 3 Consort flow diagram.
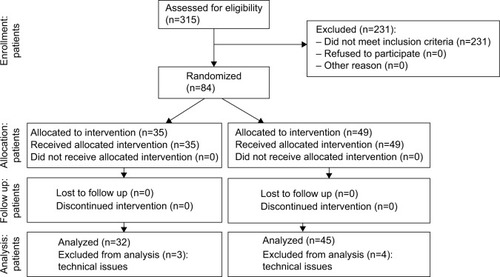
Characteristics of the patients with missing data for analyses did not differ significantly from analyzable patients. For these 77 patients, the mean age was 83.5±6.4 (range 68–101) years; 40 (52.0%) were women and 37 (48.0%) men, resulting in a sex ratio of 1.08.
Measuring reliability
The MP-BV was reliable on each of the three measurements (flexion, pronation, and supination) for 24.3% (13.9–32.8) of the patients. Separately, the percentages of reliable measures were 59.7% (49.2–70.5) for flexion, 68.8% (58.4–79.5) for pronation, and 62.3% (51.2–73.1) for supination ().
Table 1 Proportion of valid measures for each movement
Intertester reproducibility
The ICCs were 0.15 (0.07–0.73) for flexion, 0.46 (0.27–0.98) for pronation, and 0.50 (0.31–0.98) for supination. For the same movements, respectively, the concordant measures percentages were 53.2% (42.1–64.4), 57.1% (46.1–68.2), and 53.2% (42.1–64.4).
Duration of examination
Mean examination duration was significantly longer with the MP-BV than with the inclinometer, at 117.4 (±26.9) seconds and 104.4 (±34.0) seconds, respectively (P<0.0001).
Acceptability
There was no significant difference between the two instruments regarding patient comfort, with a mean VAS score for the MP-BV of 9.21 (±1.10) versus 9.26 (±0.99) for the inclinometer (P=0.49, DF =76, t=0.69). Results were the same regarding the physiotherapist’s acceptance of the instruments, with a mean VAS score of 7.88 (±1.97) for the MP-BV and 7.70 (±1.70) for the inclinometer (P>0.05, DF =76, t=1.43).
Regarding the ease of use, the mean VAS score was 8.55 (±1.21) for the MP-BV versus 7.13 (±2.54) for the inclinometer (P<0.0001, DF =76, t=6.07). Results were similar regarding the data exportation, with a mean VAS score of 8.76 (±1.44) for the MP-BV and 7.24 (±2.7) for the inclinometer (P<0.0001, DF =76, t=4.75).
Adverse events
No adverse events were recorded during the study.
Discussion
Measuring articular ROM requires the use of various instruments. However, even those instruments provide reliable and replicable measures, they present difficulties in the use and the use of reference instruments (like inclinometer or goniometer) required that the user was very rigorous in positioning the instrument before using it.Citation10 The purpose of this study was to determine the reliability and the intertester reproducibility of the MP-BV as a new measurement instrument for ROM, which may be simpler to use than other instruments.
The results of this study show the convenience of the MP-BV in terms of ease of use and of export of measured data. However, this instrument seems less reliable and useful compared to the reference instruments used to measure elbow ROM in gerontology.
The choice of measurement instrument in clinical practice is not consensual, and study results differ between authors.Citation8,Citation32 For this reason, van de Pol et alCitation33 concluded in their literature review that more research regarding these instruments was necessary. In our study, we chose the inclinometer as a reference instrument due to its validity, but also because of its higher intertester reproducibility compared to a classical goniometer on the elbow joint.Citation34 Moreover, the inclinometer is a fast and easy-to-use instrument with which physiotherapists from the Nice University Hospital are familiar. Finally, an important physiological valgus could hamper common goniometer implementation on the elbow joint. Chapleau et alCitation29 highlighted in their study the need for using radiological measurement in clinical protocols. However, radiological measurement was difficult to apply in our study.
Remarkably, this study analyzed 77 patients, which represents a significant number of patients compared to similar studies which have validated reference instruments.Citation5,Citation11 Within the context of the study, a double-blind experiment for measurements was not achievable.
We experienced some difficulties in measurement that could explain the differences between the two instruments’ outcomes. Elbow flexion measurement is usually done by placing the shoulder in a neutral position, and the choice of using two inertial sensors was made to avoid subject compensation while performing this measure (shoulder protraction). Unlike the inclinometer, the MP-BV was attached to the skin; however, skin elasticity decreases with age,Citation35,Citation36 and, as a result, there was a low adjustment of the sensor in regard to the underlying bony landmark, creating a measurement difference higher than 10°. This particularity could also explain measurement differences when pronation and supination movements were performed.
Contrary to what was expected, the importance of a rigorous marked of reference point proved to be extremely important. Indeed, the positioning of the sensor on the joint by both physiotherapists was not exactly the same and may have been responsible for the different outcomes. Moreover, a clamping system was not provided with the MotionPod, and it was necessary to use a skin guard to protect the elderly patients’ skin, which is often fragile, increasing tracking difficulties.
Regarding examination duration, it is important to note that this not only included examination duration, but also the setting-up of the skin guard, thus increasing the total measuring time with the MP-BV compared to the inclinometer.
Conclusion
With the continuing development of new technologies, we shall witness more and more new instruments that will require assessment using similar protocols to those used for medications. Based on this study, the MP-BV seems less reliable and to give less reproducible measures than one of the reference instruments used to assess elbow ROM in the elderly. Taking into account its limitations as well as its ease of both use and data exportation, it could be interesting to compare MP-BV measurements to radiographic measurements in a younger population.
Acknowledgments
The authors wish to thank Eric Fontas for his methodological support and Mathilde Demory for reviewing the English. We thank Marie Geronimi from RM Ingénieurie and Yanis Caritus from MOVEA for the technical informations. We also wish to thank the physiotherapists from the Gerontology Department (Damian Argini, Urko Larranaga, and Jérôme Danfali) and the rehabilitation health care manager Valérie Victor, as well as Professor Alain Franco and Mr Patrick Malléa.
Disclosure
This study benefited from Ministry of Industry funding within the Centre for Innovation and Health Usage (Centre d’Innovation et d’Usage en Santé [CIU-S]). MP-BV developers were part of the initial CIU-S project consortium. The statistical outcomes analysis was independently realized by the DRCI and the data interpretation was performed by physicians from the public hospital. Participants for this study (physicians, physiotherapists) who were involved in this research protocol and in the interpretation of the outcomes did not receive any specific compensation. The authors report no other conflicts of interest in this work.
References
- CallahanLFRaoJBoutaughMArthritis and women’s health: prevalence, impact, and preventionAm J Prev Med19961254014098909652
- KelseyJLWhiteAA3rdPastidesHBisbeeGEJrThe impact of musculoskeletal disorders on the population of the United StatesJ Bone Joint Surg Am1979617959964158597
- JanssenIHeymsfieldSBRossRLow relative skeletal muscle mass (sarcopenia) in older persons is associated with functional impairment and physical disabilityJ Am Geriatr Soc200250588989612028177
- KolberMJHanneyWJThe reliability and concurrent validity of shoulder mobility measurements using a digital inclinometer and goniometer: a technical reportInt J Sports Phys Ther20127330631322666645
- GogiaPPBraatzJHRoseSJNortonBJReliability and validity of goniometric measurements at the kneePhys Ther19876721921953809242
- BovensAMvan BaakMAVrenckenJGWijnenJAVerstappenFTVariability and reliability of joint measurementsAm J Sports Med199018158632405721
- PoichotteEInclinomètre et standardisation des mesures d’amplitude articulaire [Inclinometer and standardization of range of motion measurements]Kinésithérapie Scientifique20054603743 French.
- ArmstrongADMacDermidJCChinchalkarSStevensRSKingGJReliability of range-of-motion measurement in the elbow and forearmJ Shoulder Elbow Surg1998765735809883416
- GajdosikRLBohannonRWClinical measurement of range of motion. Review of goniometry emphasizing reliability and validityPhys Ther19876712186718723685114
- FishDRWingateLSources of goniometric error at the elbowPhys Ther19856511166616704059329
- WatkinsMARiddleDLLambRLPersoniusWJReliability of goniometric measurements and visual estimates of knee range of motion obtained in a clinical settingPhys Ther199171290961989012
- BrutonAEllisBGoddardJComparison of visual estimation and goniometry for assessment of metacarpophalangeal joint anglePhysiotherapy1999854201208
- MontoyeHJWashburnRServaisSErtlAWebsterJGNagleFJEstimation of energy expenditure by a portable accelerometerMed Sci Sports Exerc19831554034076645869
- ChenKYBassettDRJrThe technology of accelerometry-based activity monitors: current and futureMed Sci Sports Exerc20053711 SupplS490S50016294112
- DaneAVSchacharRJTannockRDoes actigraphy differentiate ADHD subtypes in a clinical research setting?J Am Acad Child Adolesc Psychiatry200039675276010846310
- WiggsLMontgomeryPStoresGActigraphic and parent reports of sleep patterns and sleep disorders in children with subtypes of attention-deficit hyperactivity disorderSleep200528111437144516335331
- NagelsGEngelborghsSVloeberghsEVan DamDPickutBADe DeynPPActigraphic measurement of agitated behaviour in dementiaInt J Geriatr Psychiatry200621438839316534768
- NagelsGEngelborghsSVloeberghsELemmensWPickutBADe DeynPPCorrelation between actigraphy and nurses’ observation of activity in dementiaInt J Geriatr Psychiatry2007221848617171751
- SaccoGJoumierVDarmonNDetection of activities of daily living impairment in Alzheimer’s disease and mild cognitive impairment using information and communication technologyClin Interv Aging2012753954923271900
- StanleyNActigraphy in human psychopharmacology: a reviewHum Psychopharmacol2003181394912532314
- BrooksJO3rdFriedmanLBliwiseDLYesavageJAUse of the wrist actigraph to study insomnia in older adultsSleep19931621511558446835
- YesavageJAFriedmanLKraemerHCA follow-up study of actigraphic measures in home-residing Alzheimer’s disease patientsJ Geriatr Psychiatry Neurol19981117109686746
- FriedmanLBensonKNodaAAn actigraphic comparison of sleep restriction and sleep hygiene treatments for insomnia in older adultsJ Geriatr Psychiatry Neurol2000131172710753003
- ZhangJTNovakACBrouwerBLiQConcurrent validation of Xsens MVN measurement of lower limb joint angular kinematicsPhysiol Meas2013348N63N6923893094
- WatanabeTSaitoHTests of wireless wearable sensor system in joint angle measurement of lower limbsConf Proc IEEE Eng Med Biol Soc201120115469547222255575
- WatanabeTSaitoHKoikeENittaKA preliminary test of measurement of joint angles and stride length with wireless inertial sensors for wearable gait evaluation systemComput Intell Neurosci2011201197519321941531
- CooperGSheretIMcMillanLInertial sensor-based knee flexion/extension angle estimationJ Biomech200942162678268519782986
- TheobaldPSJonesMDWilliamsJMDo inertial sensors represent a viable method to reliably measure cervical spine range of motion?Man Ther2012171929621784696
- ChapleauJCanetFPetitYLaflammeGYRouleauDMValidity of goniometric elbow measurements: comparative study with a radiographic methodClin Orthop Relat Res2011469113134314021779866
- LinLHedayatASSinhaBYangMStatistical methods in assessing agreement: models, issues, and toolsJ Am Stat Assoc200297457257270
- FleissJLThe Design and Analysis of Clinical ExperimentsNew York, NYJohn Wiley & Sons1986
- GoodwinJClarkCDeakesJBurdonDLawrenceCClinical methods of goniometry: a comparative studyDisabil Rehabil199214110151586755
- van de PolRJvan TrijffelELucasCInter-rater reliability for measurement of passive physiological range of motion of upper extremity joints is better if instruments are used: a systematic reviewJ Physiother201056171720500132
- PetherickMRheaultWKimbleSLechnerCSenearVConcurrent validity and intertester reliability of universal and fluid-based goniometers for active elbow range of motionPhys Ther19886869669693375320
- FiroozASadrBBabakoohiSVariation of biophysical parameters of the skin with age, gender, and body regionScientific World Journal2012201238693622536139
- LevakovAVuckovićNDolaiMKaćanskiMMBozanićSAge-related skin changesMed Pregl2012655–619119522730701