
Abstract
Background
Knee osteoarthritis (OA) is largely attributable to chronic excessive and aberrant joint loading. The purpose of this pilot study was to quantify radiographic changes in subchondral bone after treatment with a minimally invasive joint unloading implant (KineSpring® Knee Implant System).
Methods
Nine patients with unilateral medial knee OA resistant to nonsurgical therapy were treated with the KineSpring System and followed for 2 years. Main outcomes included Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pain, function, and stiffness subscores and independent core laboratory determinations of joint space width and fractal signature of the tibial cortex.
Results
WOMAC scores, on average, improved by 92% for pain, 91% for function, and 79% for stiffness over the 2-year follow-up period. Joint space width in the medial compartment of the treated knee significantly increased from 0.9 mm at baseline to 3.1 mm at 2 years; joint space width in the medial compartment of the untreated knee was unchanged. Fractal signatures of the vertically oriented trabeculae in the medial compartment decreased by 2.8% in the treated knee and increased by 2.1% in the untreated knee over 2 years. No statistically significant fractal signature changes were observed in the horizontally oriented trabeculae in the medial compartment or in the horizontal or vertical trabeculae of the lateral compartment in the treated knee.
Conclusion
Preliminary evidence suggests that the KineSpring System may modify knee OA disease progression by increasing joint space width and improving subchondral bone trabecular integrity, thereby reducing pain and improving joint function.
Introduction
Osteoarthritis (OA) of the knee is a leading cause of disability in adults that is attributed, in large part, to chronic excessive and aberrant joint loading.Citation1 Despite the recent concerted effort to develop disease modifying OA drugs, none have been shown to alter the natural history of knee OA in human clinical trials. According to the Osteoarthritis Research Society International/Outcome Measures in Rheumatology Initiative,Citation2 pain, functional impairment, and radiographic progression should comprise the key endpoints in trials intended to evaluate potential disease-modifying therapies. To date, there is no known treatment for knee OA that has consistently reported benefit for each of these disease modification characteristics.Citation2
Mounting evidence suggests that minimally invasive joint unloading implants have clinical utility in patients who have unsuccessfully exhausted nonsurgical knee OA therapies, but who are ineligible or unwilling to undergo arthroplasty. Data from several clinical studies have reported that these implants provide durable and clinically meaningful improvements in knee pain and function.Citation3–Citation7 However, none of these studies have reported longitudinal radiographic changes in the knee following implant. While disease progression is frequently assessed by quantifying intraarticular cartilage loss, changes in subchondral bone also play a key role in the pathogenesis of knee OA.Citation8 In fact, subchondral bone trabecular integrity has been shown to be a strong predictor of disease progression.Citation9 Fractal signature analysis (FSA) assesses the complexity of detail in a two-dimensional image (ie, radiograph) to yield a value representative of trabecular number, spacing, and cross-connectivity.Citation10 The purpose of this pilot study was to quantify clinical outcomes and radiographic changes occurring in the knee joint 2 years following treatment with a joint unloading implant, with special emphasis on subchondral bone characteristics quantified by FSA.
Methods
The COAST clinical study prospectively enrolled 40 patients at five European centers who received the KineSpring® Knee Implant System (Moximed, Inc., Hayward, CA, USA) for treatment of unilateral medial compartment knee OA (ISRCTN63048529). The study was approved by local hospital ethics committees and all subjects provided written informed consent before participation. Interim results from the COAST study have been reported elsewhere.Citation3 This report describes a post hoc assessment of subchondral trabecular integrity using fractal signature methods in a randomly selected subgroup of nine patients from the COAST study with available 2-year follow-up data and adequate imaging.
Patients
Inclusion criteria for the COAST study included patients were aged 25 years and older with radiographically confirmed medial knee OA, diagnosed according to the American College of Rheumatology Clinical and Radiographic or Clinical Classification criteria.Citation11 All eligible patients had previously failed at least 3 months of nonoperative care. Exclusion criteria included symptomatic OA in the lateral or patellofemoral compartment, varus or valgus malalignment >10 degrees, inflammatory joint disease, moderate to severe osteoporosis, recent surgery or previous prosthesis at the target knee, ligamentous or meniscal instability, active infection, and clinically significant comorbidity (eg, uncontrolled diabetes mellitus).
Procedures
Baseline assessments included inclusion/exclusion criteria evaluation, a complete clinical and orthopedic examination, and medical history. At baseline and at 2 years follow-up, standing X-rays (anteroposterior, lateral, and sunrise views) were performed on all patients. The Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC, version 3.1) was used to quantify changes in knee pain, function, and stiffness.Citation12
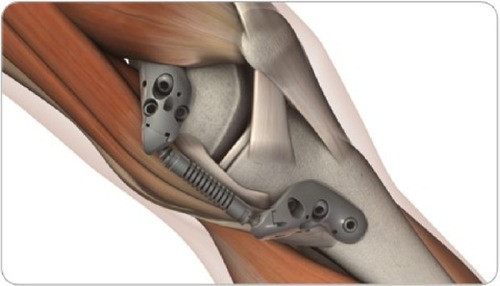
All patients were treated with the KineSpring System (), a minimally invasive implant that reduces loading at the diseased medial compartment during the stance phase of gait. The KineSpring System absorbs a maximum load of 13 kg in the medial compartment without transferring additional loads to the lateral knee compartment.Citation13 The magnitude of medial joint unloading provided by the KineSpring System is comparable to the amount of body weight loss that improves joint function and alleviates knee pain in OA patients.Citation14 A detailed description of the surgical procedure for KineSpring System implant has been reported elsewhere.Citation15
Figure 1 KineSpring® Knee Implant System.
Radiographic imaging
An imaging core laboratory (SYNARC, Newark, CA, USA) independently reviewed pretreatment and 2-year radiographs in patients treated with the joint unloading implant. Radiographs of the treated and untreated knee were digitally acquired with a mean resolution of 0.12±0.024 microns/pixel. Image analysis was performed using dedicated software (KneeAnalyzer; Optasia Medical, Cheadle, UK) that incorporates computer-aided detection methods () using statistical modeling to provide quantitative measurements of subchondral trabecular integrity in the medial and lateral compartments of each knee ().Citation9 The software also automatically calculated the minimum joint space width (JSW) of the medial and lateral compartments in each knee.
Figure 2 Semiautomated regions of interest by KneeAnalyzer.
Notes: Joint space boundary profiles for femur (blue); Joint space boundary profiles for tibial plateau at both the lateral compartment (red) and the medial (green) compartments; Regions for fractal signature analysis in the medial and lateral subchondral bone (light green boxes); Minimum joint width at the lateral compartment and the medial compartments (black).
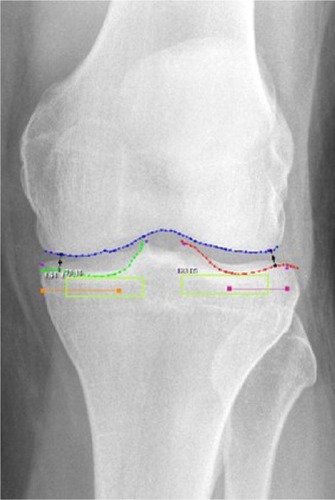
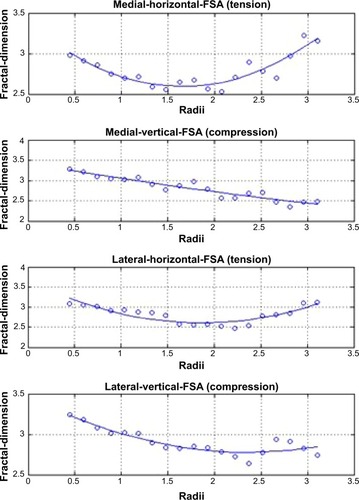
Figure 3 Representative fractal signature curves, demonstrating fractal dimensions at the tibial cortex over a range of trabecular widths from 0.4 to 3.0 mm.
Abbreviation: FSA, fractal signature analysis.
Data analysis
Continuous data were reported as median (interquartile range [IQR]), and categorical data were reported as frequencies. Longitudinal changes in clinical outcomes were assessed with the Wilcoxon signed rank test. Fractal signature data were analyzed using the methods of Kraus et al.Citation9,Citation16 Briefly, morphology of vertically and horizontally aligned trabeculae was assessed by quantifying the fractal dimension across a range of radii, representing trabeculae from 0.4 to 3.0 mm in thickness. Quadratic multiple regression using a noncentered polynomial was applied to model data for each patient, which accounted for differences in pixel width among radiographs. Pretreatment and 2-year radiographs were analyzed using area under the curve methodology.Citation17 Due to the pilot nature of this study, a one-sided P-value <0.1 was considered statistically significant.Citation18 The sample size was selected to provide 80% power to detect a minimum standardized pre–post effect size ≥0.80 (PASS 2013, Kaysville, UT, USA). Data were analyzed using IBM SPSS Statistics (version 22; IBM Corp., Armonk, NY, USA).
Results
Of the 40 patients enrolled in the COAST study, nine patients (five males) with complete clinical and radiographic data at 2 years were randomly selected for inclusion in this pilot study. Median patient age was 53 years (IQR: 48 to 58 years) with body mass index of 30 kg/m2 (IQR: 28 to 33 kg/m2) (). Clinical and radiographic disease severity of these patients were comparable to patients undergoing total knee arthroplasty.Citation19,Citation20
Table 1 Baseline patient characteristics
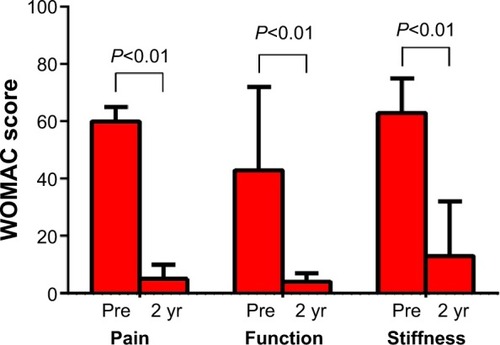
Statistically significant improvements were observed in all WOMAC scores 2 years following implant with the KineSpring® System. Median WOMAC scores improved 92% for pain, 91% for function, and 79% for stiffness (all P<0.01) over the 2-year follow-up period (). All patients exceeded the threshold for clinical success in each WOMAC domain, defined as a ≥20% improvement from baseline.Citation21
Figure 4 Change in WOMAC subscores over 2 years following joint unloading implant.
Abbreviations: WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index; yr, years.
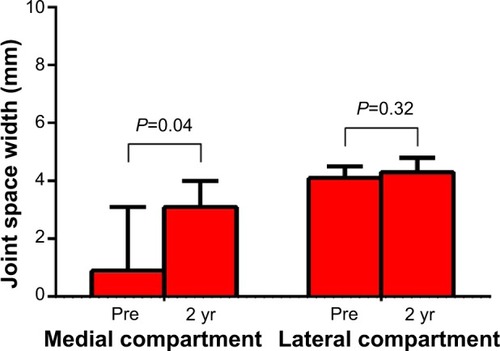
Minimum JSW in the medial compartment of the treated knee significantly increased from a median of 0.9 mm at baseline to 3.1 mm at 2 years (P=0.04); JSW in the medial compartment of the untreated knee was unchanged (P=0.32) (). No significant differences in JSW were observed in the lateral compartment of either knee.
Figure 5 Change in joint space width over 2 years following joint unloading implant.
Abbreviation: yr, years.
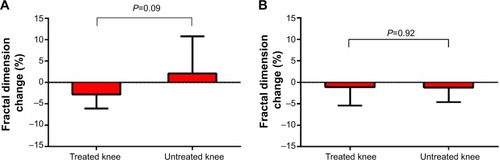
Fractal signatures of the vertically oriented trabeculae in the medial compartment decreased by 2.8% in the treated knee and increased by 2.1% in the untreated knee over 2 years postimplant (). The differences in these FSA values between knees were statistically significant (P=0.09) and, from a clinical perspective, was suggestive of OA modification in the treated knee. No statistically significant FSA changes were observed in the horizontally oriented trabeculae in the medial compartment () or in the horizontal or vertical trabeculae of the lateral compartment in the treated knee.
Figure 6 Change in subchondral tibial fractal signatures for (A) vertical and (B) horizontal oriented trabeculae over 2 years following joint unloading implant.
Discussion
The results of this pilot study suggest that a joint unloading implant may modify knee OA disease progression by increasing JSW and improving subchondral bone trabecular integrity, thereby reducing pain and improving joint function. This is the first report demonstrating radiographic evidence of knee OA disease modification with the KineSpring System.
OA progression is largely mediated through failed attempts at subchondral bone and cartilage repair secondary to excessive mechanical loading at the knee joint. Over time, repetitive impulse loading causes microfractures to develop in the subchondral endplate, resulting in local osteoporosis, subchondral sclerosis, and subsequent cartilage degeneration.Citation22–Citation24 OA progression can be visualized and quantified as thinning and fenestration of vertical trabeculae due to stress shielding and hypomineralization.Citation16
In this study, we observed the opposite phenomenon; that is, medial compartment unloading over 2 years with a minimally invasive implant modified subchondral sclerosis in vertically oriented trabeculae with concomitant increases in JSW in the medial knee compartment. The observed decrease in FSA area under the curve over 2 years is indicative of a less complex radiographic image, with reversal of thinning and fenestration of vertically oriented trabeculae. Fractal signatures of the horizontally oriented trabeculae were unchanged in the current study. This observation was not unexpected; vertical trabecular integrity has a strong relationship with OA progression while the relationship with horizontal trabecular morphometry is inconsistent.Citation9,Citation16,Citation25,Citation26
Interestingly, over 2 years, JSW in the medial compartment of the treated knee increased to approach the baseline JSW of the unaffected knee. These data further support the concept that knee OA progression may be modified when chronic biomechanical overloading forces are reduced.Citation1 Regarding therapies intended to unload the knee joint, Waller et al state:
[…] if the pathological stress pattern across the joint is normalized, it has been hypothesized that extrinsic cells can induce repair by forming fibrocartilage, remodeling of the subchondral plate so a typical trabeculated pattern will ensue, regaining its shock absorption quality and joint space width will be reestablished.Citation1
Studies of surgical joint distraction in patients with knee OA have reported similar findings, with sustained improvements in clinical outcomes, JSW, and cartilage thickness.Citation27,Citation28 The observation of decreased vertical FSA values, increased JSW, and clinically meaningful improvements in patient symptoms with the KineSpring System is supportive of these previous findings.
This pilot study was limited by a small sample size, which limits generalizability of results to the general population with knee OA. Therefore, the results are indeed promising but should not be considered conclusive. A matched control group that did not receive the joint unloading implant would provide more definitive evidence that the observed results were not attributable to confounding factors. Another limitation of this study was that a standardized imaging protocol was not used across study sites, which may introduce additional variability to the radiographic measures. A final limitation of this study was that only patients with available 2-year follow-up were selected for inclusion, which may introduce bias in the study outcomes. A notable strength of the study was use of semiautomated software to determine FSA values, which was used to reduce measurement variability compared to other fractal signature methods.Citation29,Citation30 Additional studies with larger sample sizes are needed to confirm the impact of the KineSpring System on radiographic indexes of knee OA progression.
Conclusion
Preliminary evidence suggests that in patients with knee OA, the KineSpring System may modify knee OA disease progression by increasing JSW and improving subchondral bone trabecular integrity, thereby reducing pain and improving joint function.
Acknowledgments
This research was supported by Moximed, Inc.
Disclosure
The authors report no conflicts of interest in this work.
References
- WallerCHayesDBlockJELondonNJUnload it: the key to the treatment of knee osteoarthritisKnee Surg Sports Traumatol Arthrosc201119111823182921298256
- MannoRLBinghamCOPaternotteSOARSI-OMERACT initiative: defining thresholds for symptomatic severity and structural changes in disease modifying osteoarthritis drug (DMOAD) clinical trialsOsteoarthritis Cartilage20122029310122178465
- LondonNJSmithJMillerLEBlockJEMidterm outcomes and predictors of clinical success with the KineSpring Knee Implant SystemClin Med Insights Arthritis Musculoskelet Disord20136192823761985
- LiCSSeegerTAuhuberTCBhandariMCost-effectiveness and economic impact of the KineSpring® Knee Implant System in the treatment for knee osteoarthritisKnee Surg Sports Traumatol Arthrosc201321112629263723397420
- FarrJCrawfordDCDiduchDRArendtEAMaCBLiCSProspective, multi-center, pilot study to evaluate symptom relief in patients with medial knee osteoarthritis (OA) treated with the KineSpring® knee implant for load reduction – the SOAR protocolJ Long Term Eff Med Implants2013232–316117324579856
- LiCSAyeniORSpragueSTruongVBhandariMConservative treatments, surgical treatments, and the KineSpring® Knee Implant system for knee osteoarthritis: a systematic reviewJ Long Term Eff Med Implants2013232–310514924579854
- GabrielSMCliffordAGMaloneyWJO’ConnellMKTornettaPUnloading the osteoarthritic knee with a novel implant systemJ Appl Biomech201329664765423271045
- Kwan TatSLajeunesseDPelletierJPMartel-PelletierJTargeting subchondral bone for treating osteoarthritis: what is the evidence?Best Pract Res Clin Rheumatol2010241517020129200
- KrausVBFengSWangSTrabecular morphometry by fractal signature analysis is a novel marker of osteoarthritis progressionArthritis Rheum200960123711372219950282
- MessentEABuckland-WrightJCBlakeGMFractal analysis of trabecular bone in knee osteoarthritis (OA) is a more sensitive marker of disease status than bone mineral density (BMD)Calcif Tissue Int200576641942515834503
- AltmanRAschEBlochDDevelopment of criteria for the classification and reporting of osteoarthritis. Classification of osteoarthritis of the knee. Diagnostic and Therapeutic Criteria Committee of the American Rheumatism AssociationArthritis Rheum1986298103910493741515
- BellamyNBuchananWWGoldsmithCHCampbellJStittLWValidation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or kneeJ Rheumatol19881512183318403068365
- CliffordAGGabrielSMO’ConnellMLoweDMillerLEBlockJEThe KineSpring(®) Knee Implant System: an implantable joint-unloading prosthesis for treatment of medial knee osteoarthritisMed Devices (Auckl)20136697623717052
- ZhaoDBanksSAMitchellKHD’LimaDDColwellCWJrFreglyBJCorrelation between the knee adduction torque and medial contact force for a variety of gait patternsJ Orthop Res200725678979717343285
- CliffordAO’ConnellMGabrielSMillerLEBlockJEThe KineSpring load absorber implant: rationale, design and biomechanical characterizationJ Med Eng Technol2011351657121142591
- KrausVBFengSWangSSubchondral bone trabecular integrity predicts and changes concurrently with radiographic and magnetic resonance imaging-determined knee osteoarthritis progressionArthritis Rheum20136571812182123576116
- MatthewsJNAltmanDGCampbellMJRoystonPAnalysis of serial measurements in medical researchBMJ199030067192302352106931
- LeeECWhiteheadALJacquesRMJuliousSAThe statistical interpretation of pilot trials: should significance thresholds be reconsidered?BMC Med Res Methodol2014144124650044
- BachmeierCJMarchLMCrossMJArthritis Cost and Outcome Project GroupA comparison of outcomes in osteoarthritis patients undergoing total hip and knee replacement surgeryOsteoarthritis Cartilage20019213714611330253
- BeckerRDöringCDeneckeABroszMExpectation, satisfaction and clinical outcome of patients after total knee arthroplastyKnee Surg Sports Traumatol Arthrosc20111991433144121811857
- BarrSBellamyNBuchananWWA comparative study of signal versus aggregate methods of outcome measurement based on the WOMAC Osteoarthritis Index. Western Ontario and McMas-ter Universities Osteoarthritis IndexJ Rheumatol19942111210621127869318
- BurrDBRadinELMicrofractures and microcracks in subchondral bone: are they relevant to osteoarthrosis?Rheum Dis Clin North Am200329467568514603577
- LindseyCTNarasimhanAAdolfoJMMagnetic resonance evaluation of the interrelationship between articular cartilage and trabecular bone of the osteoarthritic kneeOsteoarthritis Cartilage2004122869614723868
- RadinELRoseRMRole of subchondral bone in the initiation and progression of cartilage damageClin Orthop Relat Res198621334403780104
- MessentEAWardRJTonkinCJBuckland-WrightCTibial cancellous bone changes in patients with knee osteoarthritis. A short-term longitudinal study using Fractal Signature AnalysisOsteoarthritis Cartilage200513646347015922180
- Buckland-WrightJCMessentEABinghamCOWardRJTonkinCA 2 yr longitudinal radiographic study examining the effect of a bisphosphonate (risedronate) upon subchondral bone loss in osteoarthritic knee patientsRheumatology (Oxford)200746225726416837470
- WiegantKvan RoermundPMIntemaFSustained clinical and structural benefit after joint distraction in the treatment of severe knee osteoarthritisOsteoarthritis Cartilage201321111660166723954704
- IntemaFVan RoermundPMMarijnissenACTissue structure modification in knee osteoarthritis by use of joint distraction: an open 1-year pilot studyAnn Rheum Dis20117081441144621565898
- WolskiMPodsiadloPStachowiakGWLohmanderLSEnglundMDifferences in trabecular bone texture between knees with and without radiographic osteoarthritis detected by directional fractal signature methodOsteoarthritis Cartilage201018568469020175970
- PodsiadloPDahlLEnglundMLohmanderLSStachowiakGWDifferences in trabecular bone texture between knees with and without radiographic osteoarthritis detected by fractal methodsOsteoarthritis Cartilage200816332332917825585