
Abstract
Objective
To investigate the associations among uncontrolled hypertension, orthostatic hypotension (OH), and standing balance impairment in the elderly hypertensive patients referred to comprehensive geriatric assessment (CGA).
Methods
In a cross-sectional study, a total of 176 elderly hypertensive patients who underwent CGA were divided into OH group (n=36) and non-OH group (n=140) according to blood pressure measurement in the supine position, after immediate standing up, and after 1 minute and 3 minutes of standing position. Uncontrolled hypertension was defined as blood pressure of ≥140/90 mmHg if accompanied by diabetes mellitus (DM) or chronic kidney disease (CKD), or ≥150/90 mmHg if no DM and no CKD. Standing balance, including immediate standing balance and prolonged standing balance, was assessed in side-by-side and tandem stance.
Results
Neither uncontrolled hypertension nor OH was associated with prolonged standing balance impairment in elderly hypertensive patients (P>0.05). Blood pressure decrease after postural change was significantly associated with immediate standing balance impairment in side-by-side and tandem stance (P<0.05). Patients with OH were at greater risk of immediate standing balance impairment in both side-by-side and tandem stance than those without OH (odds ratio [OR] 3.44, 95% confidence interval [CI] 1.26–9.33, P<0.05; OR 3.14, 95% CI 1.14–8.64, P<0.01). Furthermore, uncontrolled hypertension was associated with immediate standing balance impairment in side-by-side stance (OR 2.96, 95% CI 1.31–6.68, P<0.05).
Conclusion
Uncontrolled hypertension, OH, and blood pressure decrease after postural change were associated with immediate standing balance impairment, and therefore, a better understanding of the underlying associations might have major clinical value.
Introduction
Orthostatic hypotension (OH) is a common clinical phenomenon in the elderly population and has been thought to be an independent risk factor for falls, cardiovascular events, frailty, and mortality.Citation1–Citation6 As reported, more than half of the elderly suffer from hypertension, and the prevalence of OH in this population ranges from 6% to 30%.Citation1,Citation7–Citation10 Due to aging blood vessels, blood pressure regulation declines with advancing age, and both OH and hypertension indicate impaired blood pressure regulation.Citation11–Citation13 Hypertension itself increases the incidence of OH,Citation14 especially uncontrolled hypertension in the elderly patients, who often refuse antihypertensive medication.Citation15–Citation17 Compared with participants with controlled hypertension and without OH, those with uncontrolled hypertension and systolic OH at 1 minute were at greater fall risk.Citation15 Moreover, previous studies showed that standing balance impairment may be a predisposing risk factor of falls and increase this risk threefold.Citation18–Citation20 The relationship between the presence of OH and reduced ability to maintain standing balance has been recently reported,Citation5,Citation21–Citation24 but few studies focus on the association between blood pressure regulation, including uncontrolled hypertension and OH, and standing balance.
It was hypothesized that impaired blood pressure regulation, mainly uncontrolled hypertension and OH, would increase the risk of standing balance impairment, including immediate standing balance and prolonged standing balance impairment. Accordingly, this study assessed the association of uncontrolled hypertension and orthostatic blood pressure change from the supine to standing position with two measurements of standing balance: side-by-side stance and tandem stance.
Methods
Study design and patients
This cross-sectional study included 407 elderly hypertension patients who were from the geriatric ward in Zhejiang Hospital for a comprehensive geriatric assessment (CGA) between September 2013 and September 2014. A complete CGA including a general questionnaire, physical, cognitive, and function assessments lasted approximately 1 hour. The CGA was performed by a trained geriatric nurse and a specialized geriatric physician. Approval for the study was granted by Zhejiang Hospital committees and written informed consent was obtained from each study patient.
All participants with hypertension were diagnosed by experienced cardiovascular physicians according to the 2010 Chinese Guidelines for Management of Hypertension.Citation25 Hypertension was defined as systolic blood pressure (SBP) of ≥140 mmHg and/or diastolic blood pressure (DBP) of ≥90 mmHg or currently taking antihypertension medications no matter how high blood pressure was. The inclusion criteria were aged 65 years and older, ability to understand and communicate in Chinese, ability to walk without personal assistance (walking aids permitted), and hearing and vision sufficient for compliance with assessment. Participants with acute infection, malignant tumor, Parkinson’s disease, cerebellum diseases, acute cerebrovascular diseases, delirium, terminal illness, severe vision or hearing deficits, or severe cognitive impairment (mini-mental state examination [MMSE] score ≤10) were excluded from the study.
A total of 407 potential cases were identified and eventually 353 participants agreed to participate in the study. Of these 353 cases, three patients were not included because of their age; seven patients were excluded due to severe cognitive decline; 13 patients were excluded by reason of acute infection; and 16 patients were repeatedly assessed. Forty-four patients for whom the data of the orthostatic test were unavailable were excluded, as were 94 other patients due to missing data on standing balance. All the remaining 176 cases were used for analysis. shows the procedure of selecting patients.
Figure 1 The procedure of patient selection.
Data collection
Socio-demographic data including age, sex, marital status, living arrangement, cigarette smoking, and alcohol use were collected. The body mass index (BMI) was calculated by measuring body weight (kilogram) and body height (meter). Information about concomitant diseases and the usage of medication was recorded by reviewing the hospital medical records. Multiple comorbidities were defined as no less than five kinds of diseases. Patients who took five or more oral prescription drugs were regarded as experiencing polypharmacy.Citation26 The MMSE was used to evaluate cognitive functioning.Citation27 Depression symptoms were detected by using 15-item geriatric depression scale (GDS-15); a score greater than five indicated the presence of depression symptoms.Citation28 By using a grip dynamometer, grip strength was measured every 5 minutes when the patients sat straight. The average of the repeated three trials was used for final analysis. Patients walked back and forth once a distance of 4 meters, and the shorter time was recorded to indicate current physical performance. The abilities of balance and gait were similarly considered to assess physical functioning. Venous blood samples were obtained early in the morning from resting fasting patients. Serum 25-hydroxyvitamin D (25-OH D) and serum calcium were tested at the Zhejiang Hospital laboratory.
Standing balance assessment
The balance subscale of the Tinetti performance-oriented mobility assessment (B-POMA) and the tandem test were used for assessing the ability of standing balance. All patients, wearing nonslip shoes, were asked to walk as briskly as possible with or without walking aids during the assessment. The B-POMA test contained nine static and dynamic tasks for a maximum score of 16, with a higher score indicating better balance performance; two tasks of B-POMA named immediate standing balance in which the patient was asked to keep side-by-side stance in the first 5 seconds after getting up, and prolonged standing balance reflecting how well to maintain the balance with his/her feet together in the following 10 seconds, were administered.Citation29 The patients who had marked staggering, moved feet, marked trunk sway, grabbed object for support or used walker or cane, or mild staggering but manages to stand without grabbing objects, or unable to put feet together, were considered to have standing balance impairment; and otherwise not.
The tandem test was timed in seconds while the patients were keeping their feet in line as still as possible, with the heel of the front foot touching the toes of the rear foot. Cutoff points for the tandem test were selected as 3 seconds and 10 seconds,Citation30 which were, respectively, defined as immediate standing balance impairment, prolonged standing balance impairment, and stable standing balance. The individuals who were unable to stand with one foot in front of other or start to fall or hold for less than the appointed time were regarded as having standing balance impairment; otherwise, the patients were considered as having stable standing balance. Besides, the participants were asked to recall the history of falls during the past 12 months. Fear of falling, gait problems, and use of any walking aids were self-reported.
OH measurement
Supine and standing blood pressure were measured on the left arm by a trained nurse, using an automated sphygmomanometer. SBP and DBP were recorded after at least 5 minutes in the supine position, after immediate standing up, and after 1 minute and 3 minutes of standing position. Either a decline of at least 20 mmHg in SBP and/or at least 10 mmHg in DBP within 3 minutes of standing position in the orthostatic test was considered as OH.Citation31 According to 2014 evidence-based guideline for the management of high blood pressure in adults,Citation32 the definition of uncontrolled hypertension was SBP greater than 150 mmHg and/or DBP greater than 90 mmHg in elderly hypertension patients without diabetes mellitus (DM) or chronic kidney disease (CKD), and SBP greater than 140 mmHg and/or DBP greater than 90 mmHg in those with DM or CKD.
Statistical analysis
The variables were analyzed by using the SPSS 18.0 software (SPSS, Chicago, IL, USA). Conforming to the normal distribution, continuous variables were presented as the mean and standard deviation (SD); conforming to the abnormal distribution, continuous variables were presented as the median and interquartile range (IQR). Categorical variables were presented as a percentage or constituent ratio. The unpaired t-test (for normally distributed continuous data), the chi-square test or Fisher’s exact test (for categorical data), and the Mann–Whitney U-test (for abnormally distributed continuous data) were used to compare the statistical difference between non-OH group and OH group. Furthermore, by adjustment for confounding factors, the association between standing balance, blood pressure decrease, and uncontrolled hypertension was analyzed using the logistic regression model, which was expressed in odds ratios (ORs) and 95% confidence intervals (CIs). All signifi-cance tests were two-tailed, and statistical significance was assumed as P<0.05.
Results
Characteristics of patients
The clinical characteristics of all patients are tabulated in . The mean SBP and DBP after postural change are summarized in . The mean age of all patients was 76.7 years (SD =6.6, range 65–91 years), and 101 (57.4%) of them was male. According to the definition of OH, 20.5% patients were diagnosed with OH, and the rest were classified as non-OH.
Table 1 Comparison of clinical data between the non-OH group and OH group (n=176)
Table 2 Hypertension correlated characteristics of the non-OH and OH groups (n=176)
Comparison of clinical characteristics of non-OH and OH groups
shows that the patients in the OH group were older and with a higher percentage of cerebrovascular disease, mainly cerebral infarction remission without obvious limb disorder, compared with the non-OH group (P<0.05). No significant differences were shown in the comorbidities, polypharmacy, GDS score, MMSE score, and grip strength between the two groups (P>0.05). In terms of fall history, using of walk aids, fear of falling and gait, results showed no statistical differences between the two groups, as well as in the level of calcium and 25-OH D (P>0.05); adjustments for age, sex, osteoarticular diseases, calcium supplement, and vitamin D supplement did not influence the result among the groups regarding the level of serum calcium and 25-OH D.
As for the hypertension duration, stage, and antihypertension therapy, no differences were found between patients with or without OH (P>0.05). The percentage of uncontrolled hypertension in the OH group was higher than in the non-OH group (P<0.01). In orthostatic test, compared OH group with non-OH group, supine SBP was higher, DBP after immediate standing up and standing SBP/DBP after 3 minutes were lower (P<0.05), but there was no significant difference in other assessment time points (P>0.05). Details are presented in .
Comparison of standing balance function of non-OH and OH groups
shows that the median score of the B-POMA in the OH group was lower than in the non-OH group (14 vs 15, P=0.003). In side-by-side stance, 30.6% of the patients reported impaired immediate standing balance in the OH group compared to 7.9% of the patients in the non-OH group (P<0.01). Statistical difference was observed in the percentage of prolonged standing balance impairment between the OH group and the non-OH group (61.1% vs 38.1%, P<0.05). After adjustment for age, the results remained the same, except for impaired prolonged standing balance ().
Figure 2 Comparison of standing balance between non-OH group and OH group.
Abbreviations: B-POMA, the balance subscale of the Tinetti performance-oriented mobility assessment; OH, orthostatic hypotension.
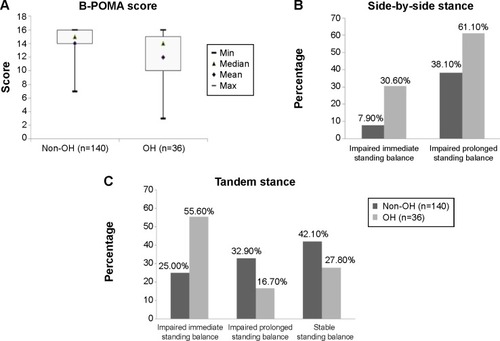
In the tandem test, compared with the non-OH group, the percentage of immediate standing balance impairment was respectively higher than prolonged standing balance impairment and stable standing balance in the OH group ([55.6% vs 16.7% vs 27.8%] vs [25.0% vs 32.9% vs 42.1%], all P<0.01), while there was no statistical significance between the latter two parameters (P>0.05). Furthermore, the results were consistent with the above after adjustment for age (), indicating that patients with OH had standing balance impairment from immediate standing up.
Association of blood pressure measurement with standing balance function
As shown in , after adjustment for age, sex, and concomitant cerebrovascular disease, partial correlations analysis found that the B-POMA score was not only associated with SBP decrease at 3 minutes after postural change (r=−0.180, P=0.019), but also negatively related with DBP decrease at 1 minute or 3 minutes after changing the position from supine to standing (r=−0.185, P=0.016; r=−0.237, P=0.002).
Table 3 Association between blood pressure decrease and B-POMA score in all elderly patients with hypertension (n=176)
shows that the decrease in SBP and DBP at 3 minutes after postural change were both associated with impaired immediate standing balance in side-by-side stance adjusted for the same confounders ([OR 3.91, 95% CI 1.27–12.03]; [OR 3.26, 95% CI 1.02–9.33]); however, this relationship disappeared between blood pressure decrease and prolonged standing balance impairment among elderly hypertensive patients. In tandem stance, patients with a higher decrease in DBP immediately, or at 1 minute and 3 minutes after postural change were significantly correlated with impaired standing balance ([OR 2.61, 95% CI 1.01–6.73]; [OR 3.85, 95% CI 1.33–11.14]; [OR 3.41, 95% CI 1.25–9.32]), but similar correlations in SBP decrease were not found. Supine blood pressure was not associated with standing balance function in side-by-side stance or tandem stance adjusted for age, sex, and concomitant disease. Patients with OH were correlated with impaired immediate standing balance in both side-by-side stance and tandem stance ([OR 3.44, 95% CI 1.26–9.33]; [OR 2.96, 95% CI 1.31–6.68]). Moreover, compared with controlled hypertension patients, patients with uncontrolled hypertension were more likely to have impairment of immediate standing balance in side-by-side stance (OR 3.14, 95% CI 1.14–8.64).
Table 4 Association between blood pressure decrease and impaired standing balance in all elderly patients with hypertension (n=176)
Discussion
This study aimed to explore the association between uncontrolled hypertension, OH, and impaired standing balance in elderly patients with hypertension. Patients with OH were more likely to have impairment of the ability of immediate standing balance in the positions of side-by-side stance and tandem stance, compared with patients without OH. Blood pressure decrease after postural change was significantly associated with immediate standing balance impairment in the above two positions, similar relationship was found between blood pressure decrease after postural change and B-POMA score. Patients with uncontrolled hypertension were correlated with a higher risk of impairment of immediate standing balance in the side-by-side position than those with controlled hypertension. In addition, no associations were found between serum 25-OH D levels, OH, and standing balance.
Blood pressure decrease, OH, and standing balance
In previous studies, the close association between OH and standing balance impairment was found not only in healthy elderlyCitation21 and older outpatientsCitation5 but also in the elderly with specific disease, including DMCitation22 or Parkinson’s disease.Citation23,Citation24 In accordance with those studies, we did find this association in elderly hypertensive patients. A cross-sectional cohort study, involving 197 elderly outpatients, indicated that elderly patients with either OH or greater blood pressure decrease after postural change had an increased risk of reduced ability of maintaining standing balance just in semi-stance with eye closed, but not in side-by-side stance or tandem stance whether eyes of the patients were open or closed.Citation5 That is not in line with this study, which showed that both OH and blood pressure decrease after changing posture were correlated with immediate standing balance impairment in both side-by-side stance (in the first 5 seconds) and tandem stance (in the first 3 seconds), even if measured with the patients’ eyes open. The discrepancy in the results may have arisen from the differences in the assessment criteria of standing imbalance and the difference in the characters of study sample.
Upon standing up from the supine position, approximately 500–1,000 mL blood accumulates in the legs and splanchnic venous vessels, resulting in reduced venous blood return to the heart, and then a transient decline in blood pressure.Citation33 In general, this situation can be normally compensated by the arterial baroreceptor reflex.Citation34 Once this baroreflex is activated, sympathetic activity will be subsequently enhanced and parasympathetic activity will be lessened, increasing the heart rate and vascular resistance in order to maintain sufficient perfusion of vital organs.Citation35 However, as for the patients with OH, these regulation mechanisms might be partly impaired, resulting in a rapid drop in blood pressure after postural change, and as a consequence of failure to timely compensation for recovering and maintaining adequate blood pressure and cerebral perfusion.Citation34,Citation36 Moreover, the dynamic cerebral autoregulation plays an important role in maintaining cerebral blood flow (CBF) relatively stable within a few seconds.Citation37–Citation40 Therefore, the researchers of some studies regarded the first few seconds of standing as a critical period of cerebral hypoperfusion,Citation41–Citation43 which would potentially increase a risk of serious outcomes, such as falls, fall-related injuries, frailty, or even mortality.Citation3,Citation4 The hypoperfusion pressure and its consequences might not be manifested in the time following standing, probably because other compensatory mechanisms, such as neurovascular compensation, the skeletal muscle pump, and neurohumoral regulation, are responsible for orthostatic blood redistribution.Citation44 Under the circumstances, the body might adapt to the state of hypoperfusion so that it can maintain standing balance in the following time. These results indirectly reflect that the ability of standing balance of the frail body has a time lag in the face of the orthostatic change. Based on aforementioned mechanisms, it can be explained why a decline in blood pressure within 5 seconds of posture change was significantly associated with immediate standing balance impairment, but not prolonged standing balance impairment.
Uncontrolled hypertension, OH, and standing balance
Some clinical studies had shown that compared with controlled hypertension, OH was more often present in the elderly with uncontrolled hypertension,Citation16 while increased blood pressure was negatively associated with the balance impairment in the elderly with hypertension, and that mediated the physical function and the risk of fall.Citation45 A recent study indicated that the patients with uncontrolled hypertension (blood pressure of $140/90 mmHg) and systolic OH at 1 minute were at a greater risk of fall.Citation15 Using 2014 evidence-based guidelines for the management of high blood pressure in adults, the results in this study were similar to the above. In this study, elderly hypertensive patients with OH represented a higher percentage of uncontrolled hypertension, and increased about three times the risk of immediate standing balance. In those uncontrolled hypertensive patients, blood pressure variability, including orthostatic blood pressure variability, is impaired,Citation46 leading to decreased CBF, and further causing deep white matter lesions detected by brain magnetic resonance imaging (MRI).Citation47–Citation49 Meanwhile, white matter lesions might be associated with standing balance impairment,Citation50,Citation51 and probably increased the fall risk.Citation18 In addition, another possible explanation is that the levels of basic blood pressure in elderly patients with uncontrolled hypertension were comparatively higher, and the differences in blood pressure after postural change were greater, corresponding increasing the risk of standing balance impairment as a consequence of the combined effect, including blood pressure regulation failure, cerebral autoregulation, neurodegeneration, and deteriorated sensory systems.
Serum 25-OH D, OH, and standing balance
In the present study, serum 25-OH D levels were not associated with OH and standing balance impairment, respectively, after adjusting for some potential confounders. Our study was in accordance with the result of another Italian population-based cohort study which included 2,640 elderly people with a mean age of 74 years.Citation52 Nevertheless, previous studies showed that a negative association was observed between serum 25-OH D levels and OH in elderly patients.Citation53,Citation54 In elderly women with a mean age of 83 years, 25-OH D deficiency was more likely to present in the participants with diastolic OH,Citation55 and simultaneously increased the risk of fall.Citation56,Citation57 It had been reported that except bone health, 25-OH D deficiency might play a role on the dysfunction of the arterial wall, finally resulting in arterial stiffness and the dysfunction of the baroreflex neural arc with a consequence of short-term maladaptive response to standing up.Citation58–Citation60 The discrepancy of the results may attribute to difference in age and the definition of 25-OH D deficiency. Therefore, further studies need large samples in order to focus on different age groups and serum 25-OH D levels to add more clinical value.
Strengths and limitations
The strength of this present study was a considerable large group of elderly patients with specific diseases who underwent CGA in the geriatric ward. A CGA was done to systematically appraise the function status of the elderly that has not been effectively applied to elderly Chinese patients on a large scale. In addition, this study divided standing balance into two parts, namely, immediate standing balance and prolonged standing balance, measured by side-by-side and tandem positions. Accordingly, additional clinical information about the associations among standing balance, OH, and uncontrolled hypertension was obtained. Moreover, this study also had several limitations. Firstly, blood pressure measurement was confined to 3 minutes after posture change, and therefore delayed OH that occurs beyond 3 minutes, even 10 minutes or more after standing,Citation61,Citation62 may be ignored. Secondly, it is possible that there is a bias about different antihypertensive medications in the elderly with hypertension at a risk of standing balance impairment. The study sample with OH was too small to detect the possible association. Finally, due to the feature of the cross-sectional study, a causal association among the three variables, namely, standing balance, OH, and uncontrolled hypertension, could not be directly concluded. Further studies with larger sample sizes will be required to investigate the possible causal relationships by longitudinal studies, and add the nonhypertension group for reference in order to make results more comprehensive.
Conclusion
In conclusion, using CGA, the prevalence of uncontrolled hypertension and standing balance impairment are observed to be higher in elderly hypertensive patients with OH than in those without OH. The risk of immediate standing balance impairment is approximately three times more in elderly hypertensive patients with OH or uncontrolled hypertension than in those with no OH or controlled hypertension, but not in prolonged standing balance impairment.
Acknowledgments
This work was supported by grants from National Health and Family Planning Commission of Scientific Research Fund of People’s Republic of China (WKJ2013-2-001) to X Chen and from Science Technology Department of Zhejiang Province (2014C33241) to X Chen.
Disclosure
The authors report no conflicts of interest in this work.
References
- BenvenutoLJKrakoffLRMorbidity and mortality of orthostatic hypotension: implications for management of cardiovascular diseaseAm J Hypertens201124213514420814408
- FanXHWangYSunKDisorders of orthostatic blood pressure response are associated with cardiovascular disease and target organ damage in hypertensive patientsAm J Hypertens201023882983720414196
- Romero-OrtunoRCoganLO’SheaDLawlorBAKennyRAOrthostatic haemodynamics may be impaired in frailtyAge Ageing201140557658321749997
- XinWLinZMiSOrthostatic hypotension and mortality risk: a meta-analysis of cohort studiesHeart2014100540641323878177
- PasmaJHBijlsmaAYKlipJMBlood pressure associates with standing balance in elderly outpatientsPLoS One201499e10680825222275
- BaeHJLimJHCheonSMOrthostatic hypotension and cognitive impairment in de novo patients with Parkinson’s diseaseJ Mov Disord20147210210425360236
- McDowellAEngelAMasseyJTMaurerKPlan and operation of the Second National Health and Nutrition Examination Survey, 1976–1980Vital Health Stat 119811511447344293
- Wolf-MaierKCooperRSBanegasJRHypertension prevalence and blood pressure levels in 6 European countries, Canada, and the United StatesJAMA2003289182363236912746359
- BeckettNSPetersRFletcherAETreatment of hypertension in patients 80 years of age or olderN Engl J Med2008358181887189818378519
- ApplegateWBDavisBRBlackHRSmithWMMillerSTBurlandoAJPrevalence of postural hypotension at baseline in the Systolic Hypertension in the Elderly Program (SHEP) cohortJ Am Geriatr Soc19913911105710641753042
- Rubio-RuizMEPerez-TorresISotoMEPastelinGGuarner-LansVAging in blood vessels. Medicinal agents FOR systemic arterial hypertension in the elderlyAgeing Res Rev201418C13214725311590
- LipsitzLAOrthostatic hypotension in the elderlyN Engl J Med1989321149529572674714
- JamesMAPotterJFOrthostatic blood pressure changes and arterial baroreflex sensitivity in elderly subjectsAge Ageing199928652253010604503
- GoldsteinDSPechnikSHolmesCEldadahBSharabiYAssociation between supine hypertension and orthostatic hypotension in autonomic failureHypertension200342213614212835329
- GangavatiAHajjarIQuachLHypertension, orthostatic hypotension, and the risk of falls in a community-dwelling elderly population: the maintenance of balance, independent living, intellect, and zest in the elderly of Boston studyJ Am Geriatr Soc201159338338921391928
- LeeTDoneganCMooreACombined hypertension and orthostatic hypotension in older patients: a treatment dilemma for cliniciansExpert Rev Cardiovasc Ther20053343344015889971
- FotherbyMDPotterJFOrthostatic hypotension and anti-hypertensive therapy in the elderlyPostgrad Med J1994708308788817870633
- MuirSWBergKChesworthBKlarNSpeechleyMQuantifying the magnitude of risk for balance impairment on falls in community-dwelling older adults: a systematic review and meta-analysisJ Clin Epidemiol201063438940619744824
- GanzDABaoYShekellePGRubensteinLZWill my patient fall?JAMA20072971778617200478
- RubensteinLZFalls in older people: epidemiology, risk factors and strategies for preventionAge Ageing200635suppl 2ii37ii4116926202
- OverstallPWExton-SmithANImmsFJJohnsonALFalls in the elderly related to postural imbalanceBr Med J197716056261264837061
- CordeiroRCJardimJRPerraciniMRRamosLRFactors associated with functional balance and mobility among elderly diabetic outpatientsArq Bras Endocrinol Metabol200953783484319942985
- HohlerADZuzuarreguiJRKatzDIDifferences in motor and cognitive function in patients with Parkinson’s disease with and without orthostatic hypotensionInt J Neurosci2012122523323622191544
- MatinolliMKorpelainenJTKorpelainenRSotaniemiKAMyllylaVVOrthostatic hypotension, balance and falls in Parkinson’s diseaseMov Disord200924574575119133666
- LiuLSWriting Group of Chinese Guidelines for the Management of H. 2010 Chinese guidelines for the management of hypertensionChin Med J2011397579615
- ViktilKKBlixHSMogerTAReikvamAPolypharmacy as commonly defined is an indicator of limited value in the assessment of drug-related problemsBr J Clin Pharmacol200763218719516939529
- FolsteinMFFolsteinSEMcHughPR“Mini-mental state”. A practical method for grading the cognitive state of patients for the clinicianJ Psychiatr Res19751231891981202204
- DennisMKadriACoffeyJDepression in older people in the general hospital: a systematic review of screening instrumentsAge Ageing201241214815422236655
- TinettiMEPerformance-oriented assessment of mobility problems in elderly patientsJ Am Geriatr Soc19863421191263944402
- GuralnikJMSimonsickEMFerrucciLA short physical performance battery assessing lower extremity function: association with self-reported disability and prediction of mortality and nursing home admissionJ Gerontol1994492M85M948126356
- The Consensus Com mittee of the American Autonomic Society and the American Academy of NeurologyConsensus statement on the definition of orthostatic hypotension, pure autonomic failure, and multiple system atrophyNeurology199646514708628505
- ArmstrongCJNC8 Guidelines for the Management of Hypertension in AdultsAm Fam Physician201490750350425369633
- MukaiSLipsitzLAOrthostatic hypotensionClin Geriatr Med200218225326812180246
- WielingWKredietCTvan DijkNLinzerMTschakovskyMEInitial orthostatic hypotension: review of a forgotten conditionClin Sci2007112315716517199559
- GoldsteinDSRobertsonDEslerMStrausSEEisenhoferGDysautonomias: clinical disorders of the autonomic nervous systemAnn Intern Med2002137975376312416949
- ThomasKNCotterJDGalvinSDWilliamsMJWillieCKAinsliePNInitial orthostatic hypotension is unrelated to orthostatic tolerance in healthy young subjectsJ Appl Physiol2009107250651719541730
- TiecksFPLamAMAaslidRNewellDWComparison of static and dynamic cerebral autoregulation measurementsStroke1995266101410197762016
- KurthCDUherBCerebral hemoglobin and optical pathlength influence near-infrared spectroscopy measurement of cerebral oxygen saturationAnesth Analg1997846129713059174310
- HamnerJWTanCOLeeKCohenMATaylorJASympathetic control of the cerebral vasculature in humansStroke201041110210920007920
- OgohSBrothersRMEubankWLRavenPBAutonomic neural control of the cerebral vasculature: acute hypotensionStroke20083971979198718451346
- ImminkRVSecherNHRoosCMPottFMadsenPLvan LieshoutJJThe postural reduction in middle cerebral artery blood velocity is not explained by PaCO2Eur J Appl Physiol200696560961416470413
- OlufsenMSOttesenJTTranHTEllweinLMLipsitzLANovakVBlood pressure and blood flow variation during postural change from sitting to standing: model development and validationJ Appl Physiol20059941523153715860687
- RickardsCACohenKDBergeronLLCerebral blood flow response and its association with symptoms during orthostatic hypotensionAviat Space Environ Med200778765365817679561
- PerlmuterLCSardaGCasavantVMosnaimADA review of the etiology, associated comorbidities, and treatment of orthostatic hypotensionAm J Ther201320327929123656967
- HausdorffJMHermanTBaltadjievaRGurevichTGiladiNBalance and gait in older adults with systemic hypertensionAm J Cardiol200391564364512615286
- KarioKEguchiKHoshideSU-curve relationship between orthostatic blood pressure change and silent cerebrovascular disease in elderly hypertensives: orthostatic hypertension as a new cardiovascular risk factorJ Am Coll Cardiol200240113314112103267
- KarioKPickeringTGBlood pressure variability in elderly patientsLancet200035592151645164610821389
- GodinOTzourioCMaillardPMazoyerBDufouilCAntihypertensive treatment and change in blood pressure are associated with the progression of white matter lesion volumes: the Three-City (3C)-Dijon Magnetic Resonance Imaging StudyCirculation2011123326627321220733
- DufouilCChalmersJCoskunOPROGRESS MRI Substudy InvestigatorsEffects of blood pressure lowering on cerebral white matter hyperintensities in patients with stroke: the PROGRESS (Perin-dopril Protection Against Recurrent Stroke Study) Magnetic Resonance Imaging SubstudyCirculation2005112111644165016145004
- TellGSLefkowitzDSDiehrPElsterADRelationship between balance and abnormalities in cerebral magnetic resonance imaging in older adultsArch Neurol199855173799443713
- StarrJMLeaperSAMurrayADBrain white matter lesions detected by magnetic resonance [correction of resonance] imaging are associated with balance and gait speedJ Neurol Neurosurg Psychiatry2003741949812486275
- VeroneseNBolzettaFDe RuiMSerum 25-hydroxyvitamin D and orthostatic hypotension in old people: the Pro.V.A. studyHypertension201464348148624914191
- SoysalPYayAIsikATDoes vitamin D deficiency increase orthostatic hypotension risk in the elderly patients?Arch Gerontol Geriatr2014591747724742775
- McCarrollKGRobinsonDJCoughlanAHealyMKennyRACunninghamCVitamin D and orthostatic hypotensionAge Ageing201241681081322789765
- AnnweilerCSchottAMRollandYBeauchetOVitamin D deficiency is associated with orthostatic hypotension in oldest-old womenJ Intern Med2014276328529524444004
- Bischoff-FerrariHADawson-HughesBStaehelinHBFall prevention with supplemental and active forms of vitamin D: a meta-analysis of randomised controlled trialsBMJ2009339b369219797342
- AnnweilerCMontero-OdassoMSchottAMBerrutGFantinoBBeauchetOFall prevention and vitamin D in the elderly: an overview of the key role of the non-bone effectsJ Neuroeng Rehabil201075020937091
- BraamLAHoeksAPBrounsFHamulyakKGerichhausenMJVermeerCBeneficial effects of vitamins D and K on the elastic properties of the vessel wall in postmenopausal women: a follow-up studyThromb Haemost200491237338014961167
- KalueffAVTuohimaaPNeurosteroid hormone vitamin D and its utility in clinical nutritionCurr Opin Clin Nutr Metab Care2007101121917143049
- AnnweilerCSchottAMBerrutGVitamin D and ageing: neurological issuesNeuropsychobiology201062313915020628264
- StreetenDHAndersonGHJrDelayed orthostatic intoleranceArch Intern Med19921525106610721580710
- GibbonsCHFreemanRDelayed orthostatic hypotension: a frequent cause of orthostatic intoleranceNeurology2006671283216832073