
Abstract
Background
The number of elderly patients with asthma has been increasing in Japan. Treatment for these patients should be provided based on the condition of individual patients. This study was performed to clarify the relationship between inhalation procedure and sex difference in elderly patients with asthma.
Methods
The inhalation procedure was examined in 155 elderly patients with asthma (male: n=66, average age ± standard deviation: 75.5±5.65 years old; female: n=89, average age ± standard deviation: 78.7±6.87 years old) during a medical examination.
Results
For the three items that were common to all devices, the percentages of the 155 patients who could/could not perform the actions were examined by separate Fisher’s exact tests for males and females. A statistically significant difference (P=0.007) was observed for “breath holding”, and more females than males were not able to hold their breath. Although no significant difference was seen in the “accurate number of times of inhalation”, females tended to not be able to inhale accurately compared to males (P=0.072).
Conclusion
Our results suggest that elderly female patients with asthma have less understanding of inhaled steroid therapy, compared to elderly male patients. Therefore, it is particularly important to confirm that the correct inhalation procedure is used by elderly female patients with asthma.
Keywords:
Introduction
The number of deaths in patients with bronchial asthma in Japan has decreased after introduction of the Guidelines for Prevention and Management of Asthma and with increased use of anti-inflammatory drugs.Citation1 The number of deaths due to asthma in Japan in 2011 was 2,060, which is approximately 33% of the mortality rate 10 years ago. However, the number of elderly patients with asthma has increased with aging of society and treatment of these patients can be difficult due to conditions such as COPD. Bronchial asthma is mainly treated with anti-inflammatory inhaled steroids, but this therapy may be difficult to administer in elderly patients. Therefore, different approaches to treatment of asthma are required for these patients, while confirmation of appropriate inhalation is needed for those who can receive treatment with inhalants. In this context, a recent report suggested the presence of more severe asthma and a lower rate of correct inhalation in female patients.Citation2 Here, we report the results of a study in elderly patients with asthma who were outpatients at our hospital, in which the aim was to clarify the reasons for the sex difference in the inhalation procedure.
Methods
The subjects were 155 adults patients with bronchial asthma who made regular visits to Banbuntane Hotokukai Hospital at Fujita Health University and to related medical institutions from September 2010 to March 2011 and gave informed consent for the study. The patients included 66 males (average age ± standard deviation: 75.5±5.65 years old) and 89 females (average age ± standard deviation: 78.7±6.87 years old), who did not have dementia, neurological disorders, or muscular disorders. We performed an investigation of the inhalation procedure during a medical examination. The severity of the asthma was mild and persistent or severe and persistent, and the duration of the disease ranged from 1 to 43 years.
The diagnosis of asthma was made by physicians according to JGL2012,Citation1 and the instructions on the inhalation of steroids were given by physicians or pharmacists. The patients who had been treated with inhaled corticosteroids for at least 3 months were selected. Four patients with severe persistent asthma were concomitantly taking an oral corticosteroid (prednisolone), and other patients were taking oral corticosteroids as needed at the time of attacks. However, these patients were not being treated with antibiotics.
A test of respiratory function was conducted together with an inspection of the inhalation procedure.
For this study, items on the instructions that were given to maximize the effects of the inhalation therapy and to keep the device clean during routine medical care were inspected. The patients were required to record the “correct number of inhalations”, which was an item that was common to all devices, in the asthma diary and whether the patients complied with the required times of inhalation was checked at hospital visits. In patients using more than one device, the use of each device was inspected, and the results were added to the data.
Code of ethics
The study was approved by the Institutional Review Boards of Fujita Health University (IRB no 14-037). Written informed consent was obtained from all participants.
Results
The results of the respiratory function tests are shown in . Statistically significant differences were observed between males and females for vital capacity and forced vital capacity (P<0.0001) and forced expiratory volume in 1 second (P=0.007, Student’s t-test).
Table 1 Results of the respiratory function tests
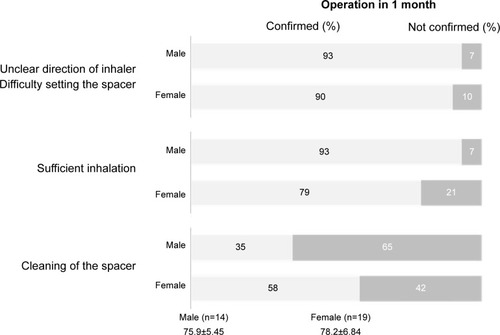
For the three items that were common to all devices, the percentages of the 155 patients who could/could not perform the actions were examined by separate Fisher’s exact tests for males and females (). A statistically significant difference (P=0.007) was observed for “breath holding”, and more females than males were not able to hold their breath. Although no significant difference was seen in the “accurate number of times of inhalation”, females tended to not be able to inhale accurately compared to males (P=0.072). Next, we examined specific items for individual devices. For 33 patients (male: 14, female: 19) who used a pressurized metered-dose inhaler with spacers, “direction of the inhaler and setting of the spacer” were correctly performed by 93% of males and 90% of females, with no significant difference. However, there was a difference of 14% in “sufficient inhalation”, which was observed in 93% of males and 79% of females. Cleaning of the spacer was correctly performed by 35% of males and 58% of females, showing a much higher rate in female patients ().
Figure 1 Results for items common to all inhalation devices.
Notes: *P=0.007. Average age ± standard deviation.
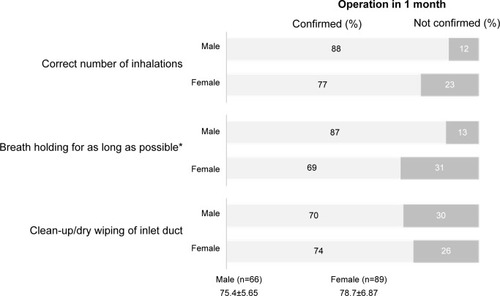
Figure 2 Results for use of a pressurized metered-dose inhaler (pMDI) with spacers.
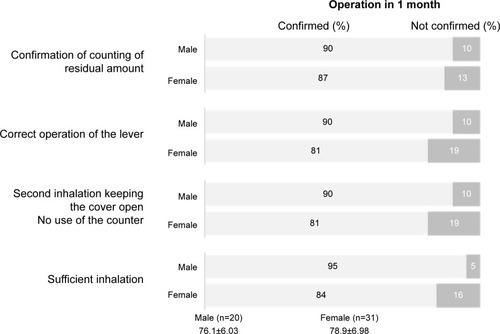
Among 51 patients (male: 20, female: 31) using a Diskus (fluticasone propionate, salmeterol/fluticasone combination) “confirmation of counting of residual amount” was performed by 90% of males and 87% of females, while “correct operation of the lever” occurred for 90% of males and 81% of females, with no significant difference between the sexes. Sufficient inhalation occurred in 95% of males and 84% of females ().
Figure 3 Results for use of a Diskus.
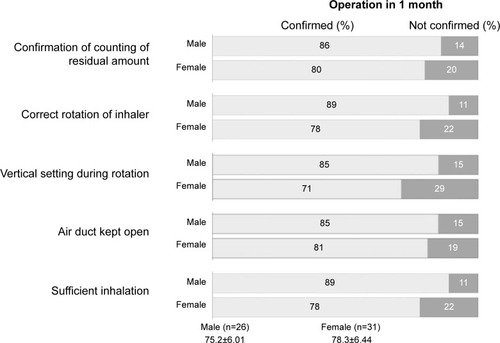
For patients using a Turbuhaler (male: 26, female: 31), an “open air duct” was found in 85% of males and 81% of females, with no significant difference. However, the rates of three other items (“correct rotation of the inhaler”, “vertical setting during rotation”, and “sufficient inhalation”) were 89%, 85%, and 89% in males and 78%, 71%, and 78% in females, respectively, with each item having approximately a 10% lower rate in females (). The “confirmation of counting of residual amount” was 86% in males and 80% in females, which were almost the same percentages.
Figure 4 Results for use of a Turbuhaler.
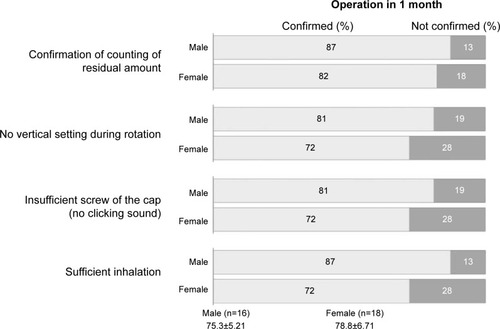
Among patients using a Twisthaler (male: 16, female: 18) “no vertical setting during rotation” and “insufficient screw of the cap” occurred in 81% of males and 72% of females, while “sufficient inhalation” was found in 87% of males and 72% of females, indicating a difference of 15% (). The “confirmation of counting of residual amount” was 87% in males and 82% in females, which were almost the same percentages.
Figure 5 Results for use of a Twisthaler.
Discussion
In Japan, anti-inflammatory treatment with inhaled steroids is widely used in line with the Guidelines for Prevention and Management of Asthma,Citation1 and this approach has resulted in an annual decrease in mortality due to asthma. However, most patients who die from asthma are aged 65 years or older, and thus long-term management of asthma in elderly patients has become increasingly important.
According to our previous survey on the preference for drugs for long-term control of asthma, patients who preferred not to use an inhaler were mainly elderly, with 36% of this group aged 65–74 years and 43% aged 75–84 years.Citation3 This seemed to be attributable to the observation that the use of inhalers is not very common among Japanese people and suggests that understanding of inhalation devices and of inhaled steroids may be insufficient, and that it may not be easy for elderly patients to perform the inhalation procedure. However, respiratory function has been found to be significantly improved after providing elderly asthma patients with training in inhalation.Citation4 Thus, correct treatment for individual patients can make a major contribution to improvement of asthma control.
In this study, we examined possible sex differences in the inhalation procedure in elderly patients with asthma who were treated with inhaled steroids. This sex difference in elderly asthma patients could be due to the complication of COPD, and muscle strength of hands and fingers, but these factors were not investigated in the current study.
The results showed that the percentage of males who were able to perform “breath holding” was significantly larger than the percentage of females, and a similar result was observed for the “correct number of inhalations” which is the item that checks the adherence of inhaled corticosteroids (ICS). These findings suggest that men have a deeper understanding of the dosing procedure and the importance of inhaled steroids, while the understanding of them was low in female patients. The possible reasons for this include that Japanese people have a smaller body size than American and European people; the body size of elderly women is even smaller; age-related changes, such as kyphoscoliosis, are common; abdominal breathing is mainly used; and breath holding and inhalation speed are not sufficient in a large percentage of people. No significant differences were observed for the individual devices, the percentage of patients who met the criteria for all items except those related to cleaning the device were higher in males. In particular, the rate of “sufficient inhalation” was approximately 10% higher in males for all devices. This result is similar to the finding of Goodman et alCitation2 that the rate of correct inhalation in females was significantly lower than that in male patients.
Concerning the items related to washing, it was considered likely that females are more familiar with cleaning and washing than males because it is customary in Japan that males work outside their homes, such as at companies, while women work at home. Moreover, a study on the differences in compliance with short-acting beta-agonists (SABA), which is a drug that is used to treat asthma attacks, recently reported a correlation between inhalation compliance and severity.Citation5 Our present report was on the use of inhaled steroids that need not to be carried around and that can be used at home for the long-term management of asthma, rather than a drug like SABA, which is used at the time of an attack. Thus, the purpose of the use of inhalants might have been different.
Inhaled steroids are also the first-line drugs for elderly asthma patients, but there may be problems with the inhalation procedure when a physician provides this treatment without clear instructions. In some cases, this may result in reduced effects of the inhalant. The results of this study suggest that provision of clear information on the inhalation procedure is particularly important for elderly female patients. If limited effects of inhaled steroids are likely even after repeated training for inhalation, use of oral anti-inflammatory agents such as leukotriene receptor antagonists and transdermal preparations should be considered.
Conclusion
In conclusion, in this study we examined potential sex differences in the inhalation procedure in elderly asthma patients. Many female patients used an incorrect inhalation procedure, compared to male patients, and thus more training in inhalation is required for female patients. Confirmation of the correct inhalation procedure will be increasingly important for elderly asthma patients with the continuing aging of society.
Disclosure
The authors report no conflict of interest in this work.
References
- Japanese Society of AllergologyAsthma Prevention and Management Guidelines (JGL)JapanKyowa Kikaku2012
- GoodmanDEIsraelERosenbergMJohnstonRWeissSTDrazenJMThe influence of age, diagnosis, and gender on proper use of metered-dose inhalersAm J Respir Crit Care Med19941505 Pt 1125612617952549
- HoriguchiTKondoRBanNSurvey of type of administration in treatment of asthma in adults in different age groups: problems of asthma in elderly patientsProg Med20113124692471 Japanese
- HoriguchiTKondoRBanNTherapeutic approach based on characteristics of asthma in elderly patients: procedure and level of understanding of inhalant drugsAllergy Immunity20101710861093 Japanese
- LinderPSLinderAJGender differences in asthma inhalerConn Med201478420721024830116