
Abstract
Purpose
Prostate-specific antigen (PSA) is the most important marker in the diagnosis and follow-up of patients with prostate cancer. The primary objective of this study was to evaluate the effect of various urologic procedures in prostatic area on serum free and total PSA levels.
Subjects and methods
A series of 62 patients (8 after digital rectal examination [DRE], 12 after transrectal ultrasonography [TRUS], 11 after rigid cystoscopy, 13 after prostatic massage, 8 after TRUS-guided prostate biopsy, and 10 after transurethral resection of prostate [TURP]) were enrolled in the study. Blood samples were taken from each patient before procedure and at 10, 30, 60, and 120 minutes after procedures.
Results
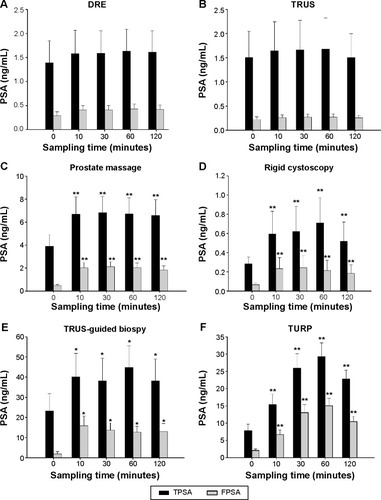
Prostate massage, rigid cystoscopy, TURP, and TRUS-guided prostate biopsy caused statistically significant rise in total and free PSA levels in the serum. There was no significant increase in total and free PSA levels in the serum after DRE and TRUS. The mean differences were greater for free PSA level in the serum for TURP, TRUS-guided prostate biopsy, prostate massage, and rigid cystoscopy.
Conclusion
Total and free PSA levels in the serum are altered by prostate massage, rigid cystoscopy, TRUS-guided prostate biopsy, and TURP. The PSA rises were related to the stimulation strength of the procedures. The total and free PSA levels were increased significantly from 10 minutes after procedures, except DRE and TRUS, and were increased to maximal level at 60 minutes after procedures.
Introduction
What’s known?
Serum prostate specific antigen (PSA) has become the most useful marker for diagnosis, staging, monitoring, and predicting prognosis of prostate cancer.
Serum PSA level may be elevated in patients with prostate cancer, benign prostate hyperplasia (BPH), infection, abscess or infarction, transurethral resection of prostate.
What’s new?
The PSA rises were related to the stimulation strength of the procedures.
After prostate massage, rigid cystoscopy, transrectal ultrasono guided prostate biopsy and transurethral resection of prostate, the total and free PSA levels were increased significantly from 10 min after procedures and increased to maximal level at 60 min after procedures.
What is the factor to affect prostate-specific antigen?
Prostate-specific antigen (PSA) is a kallikrein-like serine protease produced exclusively by prostatic epithelial cells. Serum PSA has become the most useful marker for diagnosis, staging, monitoring, and predicting prognosis of prostate cancer. Current screening recommendation by the American Urological Association and the American Cancer Society includes yearly serum PSA determination in low-risk groups, starting at 50 years of age. High-risk men are encouraged to obtain yearly PSA measurements, starting at 40 years of age.Citation1,Citation2 Elevated serum PSA levels are probably a product of disruption of cellular architecture within the prostatic gland. The loss of the barrier afforded by the basal layer and basement membranes within the normal gland is a likely site for the egress of PSA into the circulation. Serum PSA level may be elevated in patients with prostate cancer,Citation3,Citation4 benign prostate hyperplasia (BPH),Citation5,Citation6 infection, abscess, or infarction.Citation7,Citation8 Transurethral resection of prostate (TURP),Citation9 transrectal ultrasonography (TRUS)-guided prostate biopsy,Citation10,Citation11 ejaculation,Citation12 cystoscopy,Citation10 colonoscopy,Citation13 and coronary artery stent implantationCitation14 can cause serum PSA rises. Serum PSA levels can decrease after prostatectomy, treatment with 5α-reductase inhibitor, luteinizing hormone-releasing hormone analog and antiandrogen, and radiation.Citation15–Citation19
For the patients with lower urinary tract symptoms (BPH/LUTS), serum PSA, DRE and TRUS were evaluated in the same urologic clinic. The cystoscopy or expressed prostatic secretion by prostatic massage was added to routine practice for evaluation of BPH/LUTS when patients had hematuria or pelvic pain. These procedures seem to affect the cutoff level of serum PSA for decision of prostate biopsy, especially between 2.5 and 10 ng/mL of serum PSA. Thus, we conducted a prospective study of serum PSA levels consecutively in the same patients undergoing procedures in the prostatic area within 120 minutes of the procedure.
Patients and methods
We conducted a prospective study on the effect of various urologic procedures in prostatic area for the change of total and free PSA levels in the serum. After Chonbuk National University Hospital Institutional Review Board’s approval, 62 men were enrolled in the study. All patients provided informed consent after a candid discussion. We excluded patients who had prostatic biopsy, cystoscopy, or urinary tract infection in the preceding 30 days. The half-life of total serum PSA has been reported to be between 2.2 and 3.2 days;Citation20,Citation21 thus, 30 days might be enough time to return to normal range of PSA after prostatic biopsy, cystoscopy, or urinary tract infection. We also excluded patients with a history of prostate cancer, prostatic surgery, luteinizing hormone-releasing hormone analog or antiandrogen use, and 5α-reductase inhibitor use.
The patients underwent TRUS, DRE, and prostate massage for the evaluation of their BPH/LUTS. The patients underwent rigid cystoscopy for the evaluation of microscopic or gross hematuria. The patients underwent TRUS-guided prostate biopsy because of abnormal DRE or serum PSA levels over 4.0 ng/mL. All DREs were performed by same physician, with the patient in the lateral position. All prostate massages were performed by same physician. TRUS was performed with a 7.5 MHz transducer (B&K 2102, Bruel and Kjær, Nærum, Denmark), and 12 core biopsies were taken in all cases with an 18G Tru-cut needle (Pro-Mag™ biopsy needle, Medical device technologies, Inc., Gainesville, FL, USA). Rigid cystoscopies were performed with a 20-French cystoscope after lubricating the urethra with 10 mL of lidocaine gel in our outpatient department. The TURP was performed using a 17-French resectoscope as an inpatient procedure.
Venipuncture was performed, and 5 mL of blood was collected immediately before procedures. Venipuncture was performed by a urologic resident, and it was maintained with a plastic cannula (Venflon, Viggo, Helsingborg, Sweden). The blood samples were collected again at 10, 30, 60, and 120 minutes. The serum was immediately centrifuged and was kept frozen at −80°C until assay. Total and free PSA were measured using an immunoradiometric assay (CIS bio international, Gif-Sur-Yvette Cedex, France).
For multiple comparisons in a small number of patients, we used the Wilcoxon signed-rank test. The Wilcoxon signed-rank test is a nonparametric statistical hypothesis test used when comparing two related samples, matched samples, or repeated measurements on a single sample to assess whether their population mean ranks differ. The mean total and free PSA levels in the serum at baseline were compared with the mean total and free PSA levels in the serum at 10 minutes. In the same way, the mean total and free PSA levels in the serum at baseline were compared with the mean total and free PSA levels in the serum at 30, 60, and 120 minutes, respectively. The results were considered significant at P<0.05. All statistical analyses were performed using SPSS version 13.0 (SPSS, Chicago, IL, USA).
Results
A total of 8, 12, 13, 11, 8, and 10 patients who underwent DRE, TRUS, prostatic massage, rigid cystoscopy, TRUS-guided prostate biopsy, and TURP were enrolled this study, respectively (). The mean age was 63.95 years (35–83 years). The mean ages were 60.34±11.31, 57.02±12.45, 58.8±14.78, 66.14±15.26, 72.93±14.91, and 71.45±16.28 years in patients who underwent DRE, TRUS, prostate massage, rigid cystoscopy, TRUS-guided prostate biopsy, and TURP, respectively (). The mean prostate volumes were 23.95±15.28, 25.33±18.29, 32.86±17.55, 31.35±22.35, 46.1±21.95, and 52.7±18.48 mL in patients who underwent DRE, TRUS, prostate massage, rigid cystoscopy, TRUS-guided prostate biopsy, and TURP in TRUS measurement, respectively ().
Table 1 Baseline characteristics of patients enrolled in the study
After prostate massage, rigid cystoscopy, and TURP, the total and free PSA levels increased significantly from 10 minutes after procedures (P<0.01; and , ). And TRUS-guided prostate biopsy also caused the total and free PSA to rise significantly from 10 minutes after procedure (P<0.05; and , ). The total and free PSA levels increased to a maximal level at 60 minutes after procedures ( and , ). Interestingly, the mean changes were greater for free PSA than total PSA rises (P<0.05). This was most apparent following TURP and TRUS-guided prostate biopsy. But there was no statistically significant change in total and free PSA levels in the serum before and after DRE and TRUS.
Table 2 The mean changes in total PSA level in the serum before and after procedures according to time
Table 3 The mean changes in free PSA level in the serum before and after procedures according to time
Figure 1 The changes in total and free PSA levels in the serum before and after procedures.
Abbreviations: DRE, digital rectal examination; PSA, prostate-specific antigen; TRUS, transrectal ultrasonography; TURP, transurethral resection of the prostate; TPSA, total prostate-specific antigen; FPSA, free prostate-specific antigen.
Discussion
PSA has become the most useful marker for diagnosis, staging, monitoring, and predicting prognosis of prostate cancer. However, some forms of urologic procedure increase PSA level.Citation9,Citation10,Citation20,Citation22 These unpredictable factors usually require the urologist to repeat previously performed PSA tests. Thus, it is important to know what kind of urologic procedure is affecting PSA level. In our study, after prostate massage, rigid cystoscopy, TRUS-guided prostate biopsy, and TURP, the total and free PSA levels were increased significantly from 10 minutes after procedures and increased to a maximal level at 60 minutes after procedures. The PSA rises were related to the stimulation strength of the procedures.
First of all, DRE is an important examination for screening prostate cancer together with PSA. Long et alCitation9 demonstrated that serum total and complexed PSA, which were statistically significant, increased at 20 minutes after DRE in 34 patients. Ornstein et alCitation20 also showed that a DRE caused a modest rise in total PSA level in the serum. But, Lynn et al,Citation11 showed that there was no significant increase in total PSA level in the serum levels after DRE. The results of our study are similar to the existing findings in that no significant increase in serum total and free PSA at 10, 30, 60, and 120 minutes after DRE. These results suggested that DRE did not disrupt cellular architecture within the prostate gland.
Urethrocystoscopy is the standard procedure for endoscopic evaluation of the lower urinary tract. Collins et alCitation10 noted a change in the mean total PSA level in the serum level of 2.48–2.50 ng/mL (P=0.841) and in free PSA level in the serum of 0.40–0.49 ng/mL (P=0.019) in 26 patients at 30 minutes after flexible cystoscopy. Long et alCitation9 showed changes in the mean total PSA level in the serum of 0.68 ng/mL (P=0.0006) in 28 patients at 20 minutes after flexible cystoscopy and 0.13 ng/mL (P=0.0199) in 17 patients at 20 minutes after rigid cystoscopy. DeCastro et alCitation22 found a small increase in the total and free PSA levels in the serum after flexible cystoscopy. They suggested that although statistically significant, the increase in mean total PSA level in the serum of 0.113 ng/mL was not clinically relevant. They concluded that flexible cystoscopy does not adversely affect the serum PSA values in men with total serum PSA values <4 ng/mL. Lynn et alCitation11 also showed that there was no significant increase in serum PSA level after flexible cystoscopy. In our study, the mean changes in total PSA level in the serum levels were 0.31, 0.34, 0.43, and 0.24 ng/mL at 10, 30, 60, and 120 minutes after procedures, respectively (P<0.01). No volunteer had a total PSA >2.5 ng/mL on the initial serum PSA measurement. One volunteer had a total PSA level in the serum increase from 0.564 ng/mL before cystoscopy to 2.84 ng/mL at 10 minutes after cystoscopy and 3.11 ng/mL at 30 minutes after cystoscopy. Although the effect of cystoscopy on serum PSA was clinically minimal, serum PSA should be checked before performing cystoscopy.
Prostatic massage and DRE are commonly performed at the same urologic visit, as is serum PSA measurement. Several studies have investigated the effect of prostatic massage on total PSA level in the serum levels, with different conclusions. Tarhan et alCitation23 showed that the total and free PSA levels in the serum increased significantly after prostate massage and that no significant increase occurred in the mean total PSA level in the serum after prostatic massage in patients with prostate cancer. In our study, the total and free PSA levels in the serum significantly increased after prostatic massage, and the rise in free PSA level in the serum after prostatic massage was greater.
TRUS is a useful tool for evaluation of prostate volume and architecture as well as for prostate biopsy. Long et alCitation9 and Lynn et alCitation11 suggested that TURP and TRUS-guided prostate biopsy significantly increased total PSA level in the serum. And they demonstrated that serum complexed PSA is less prone to variations compared to total PSA level in the serum. In our study, TRUS alone had no effect on total and free PSA levels in the serum. But TRUS guided prostate biopsy and TURP had significant effect on total and free PSA levels in the serum. The change of free PSA level in the serum was greater than total PSA level in the serum. The results of our study are consistent with results of Long et alCitation9 and Lynn et al.Citation11 Elevated serum PSAs are probably a product of disruption of cellular architecture within the prostate gland. This can occur in the setting of prostate disease (prostate cancer, prostatitis) and with prostatic manipulation (TURP, prostatic massage, prostate biopsy). Although TURP and TRUS-guided prostate biopsy increased serum total and free PSA levels, it is unlikely to be of clinical relevance as these changes in level were minimal.
A limitation of our study is a very small cohort of patients for each urological procedure. However, to our knowledge, this study represents the first prospective investigation of the change of total and free PSA levels in the serum at baseline, 10, 30, 60, and 120 minutes after each procedure. It is clinically important because most urologic procedures are taken within 120 minute for evaluation. This study gives valuable information about change of PSA after various urological procedures as time passes.
Conclusion
This study found increased total and free PSA levels in the serum after prostatic massage, rigid cystoscopy, TRUS-guided prostate biopsy, and TURP. But DRE and TRUS had no effect on total and free PSA levels in the serum. Prostate manipulation has minimal effect on total and free PSA when patients visit urologic clinic for their BPH/LUTS. But, serum PSA measurement must precede prostatic massage and rigid cystoscopy when prostate massage and rigid cystoscopy are added to routine checkup.
Author contributions
Seung Chol Park, Yu Seob Shin, Dal Sik Kim, Sung Zoo Kim, Nam Cheol Park, and Jong Kwan Park were involved in the laboratory procedures, data collection, and analysis. Seung Chol Park, Yu Seob Shin, Nam Cheol Park, and Jong Kwan Park were involved in the preparation and the review of the article. All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Acknowledgments
This study was supported by grants of the Korea Healthcare technology R&D Project, Ministry of Health, Welfare and Family Affairs, Republic of Korea (HI13C0104).
Disclosure
The authors report no conflicts of interest in this work.
References
- American Urological AssociationEarly Detection of Prostate Cancer: Policy StatementBoard of Directors MinutesLinthicum, MDAmerican Urological Association1992
- MettlinCJonesGAveretteHGusberbSBMurphyGPDefining and updating the American Cancer Society guidelines for the cancer-related checkup of prostate and endometrial cancersCA Cancer J Clin19934342468422604
- CatalonaWJSmithDSRatliffTLManagement of prostate-specific antigen in serum as a screening test for prostate cancerN Engl J Med1991324115611611707140
- CrawfordEDDeAntoniEPEtzieriRSchaeferVCOlsonRMRossCASerum prostate-specific antigen and digital rectal examination for early detection of prostate cancer in a national community-based programUrology1996478638698677578
- MochtarCAKiemeneyLAvan RiemsdijkMMProstate-specific antigen as an estimator of prostate volume in the management of patients with symptomatic benign prostate hyperplasiaEur Urol20034469570014644122
- YuDWParkSCSeoIYRimJSCan serum PSA predict prostate volume in men with benign prostate hyperplasia?Korean J Urol200546574578
- AgnihotriSMittalRDKapoorRMandhaniAAsymptomatic prostatic inflammation in men with clinical BPH and erectile dysfunction affects the positive predictive value of prostate-specific antigenUrol Oncol20143294695124996777
- TchetgenMBOesterlingJEThe effect of prostatitis, urinary retention, ejaculation and ambulation on the serum prostate-specific antigen concentrationUrol Clin N Am199724283291
- LongRGiriSDiverSDuddyLMcKeownDMoranKEffect of prostate manipulation on the serum levels of complexed prostate-specific antigen and total prostate-specific antigenInt J Urol20061394795016882060
- CollinsGNMartinPJWynn-DaviesABroomanPJO’ReillyPHThe effect of digital rectal examination, flexible cystoscopy and prostatic biopsy on free and total prostate specific antigen, and the free-to total prostate specific antigen ratio in clinical practiceJ Urol1997157174417479112518
- LynnNNKCollinsGNO’ReillyPHProstatic manipulation has a minimal effect on complexed prostate-specific antigen levelsBJU Int200086656710886085
- LimJHKimSDChoiKSChoiSBKimDWParkJKThe changes of serum prostate-specific antigen after ejaculationKorean J Urol20074812471250
- SchwartzBFFaughtJJeziorJRThe effect of colonoscopy on serum prostate antigen levelsBJU Int19998430230410468726
- OzcanTBozluMMusluNGozukardKHSeyisSAkcayBElevation of the serum total and free prostate specific antigen levels after stent implantation in patients with coronary artery diseaseSwiss Med Wkly200913967267519950034
- LangePHErcoleCJThe value of serum prostate specific antigen determinations before and after radical prostatectomyJ Urol19891418738792467013
- StameyTAKabalinJNFerrariMProstate specific antigen in the diagnosis and treatment of adenocarcinoma of the prostate. III. Radiation treated patientsJ Urol1989141108410872468796
- StameyTAKabalinJNFerrariMYangNProstate specific antigen in the diagnosis and treatment of adenocarcinoma of the prostate. IV. Anti-androgen treated patientsJ Urol1989141108810902468797
- MorganWRZinckeHRainwaterLMMyersRPKleeGGProstate specific antigen value after radical prostatectomy for adenocarcinoma of the prostate. Impact of adjuvant treatment (hormonal and radiation)J Urol19911453193231703241
- EtzioniRDHowladerNShawPALong-term effects of finasteride on prostate specific antigen level: results from the prostate cancer prevention trialJ Urol200517487788116093979
- OrnsteinDKRaoGSSmithDSRatliffTLBaslerJWCatalonaWJEffect of digital rectal examination and needle biopsy on serum total and percent of free prostate specific antigen levelsJ Urol19971571951988976249
- OesterlingJEChanDWEpsteinJIProstate specific antigen in the preoperative and postoperative evaluation of localized prostatic cancer treated with radical prostatectomyJ Urol19881397667722451037
- DeCastroBJBakerKCEffect of flexible cystoscopy on serum prostate-specific antigen valuesUrology20097323724019041123
- TarhanFOrcunAKucukercanICamursoyNKuyumcuogluUEffect of prostatic massage on serum prostate-specific antigen levelsUrology2005661234123816360449