
Abstract
Aim
The aim of this study is to determine the reliability of panoramic radiograph (PR) as a screening tool for the detection of calcified carotid atheroma (CCA) by comparing it with Doppler ultrasonography (DU) examination. A second aim was to evaluate the relationship among CCA, systemic diseases, smoking, and body mass index in an older population.
Materials and methods
A total of 1,650 PRs of patients aged over 45 years (736 males and 914 females) were randomly selected. All the patients had been referred to the Faculty of Dentistry, Afyon Kocatepe University, Afyonkarahisar, Turkey, during 2013–2014 for routine PR screening. Medical data were collected from the archival records of the dental school. The patients were divided into two groups: Group A (study group), CCA findings were confirmed by DU (n=59); and Group B (control group), CCA findings were not confirmed by DU (n=34).
Results
Of the 1,650 individuals, 93 (5.63%) were detected to have CCA on PR. The population consisted of 43 males and 50 females with mean age of 59.84±10.92 years. No difference was determined in respect of CCA between the sexes (P=0.745). There was a significant difference between Group A and Group B in respect of hypertension (P=0.004). But there was no difference between Group A and Group B in respect of age (P=0.495), BMI (P=0.756), diabetes (P=0.168), and smoking (P=0.482) distribution.
Conclusion
Although PR cannot be used as an initial diagnostic method when searching for CCA, dentists should be aware of CCA on a routine PR, particularly in older patients who may also have the risk factors of obesity, diabetes mellitus, hypertension, and smoking. Recognizing of CCA especially in hypertensive patients could potentially increase the length and quality of life for individuals.
Introduction
Stroke remains one of the most leading causes of death and a main cause of long-time disability in most countries.Citation1 Stroke is generally the result of embolus or thrombus delivered from a carotid atheromatous plaque, or more rarely due to hemodynamic changes arising from the considerable contraction of the carotid lumen.Citation2 Calcified carotid atheroma (CCA) consists of a calcification plaque of cholesterol and fat within the carotid artery, and known risk factors include diabetes mellitus, hypertension, hyperlipidemia, obesity, and smoking.Citation3
Although stroke can be avoided, a major challenge is to discover efficient methods to detect stroke-prone patients. Most noncardiogenic strokes happen as a result of atheroma plaques in the internal carotid artery, calcification of which can be detected on panoramic radiograph (PR).Citation4 Cohen et alCitation5 thought PRs to be significant markers for following vascular events, and recommended that patients with CCA be referred for cerebrovascular and cardiovascular evaluation. On a routine PR, CCA can be detected primarily by the oral practitioner. Almost 5% of PRs of patients aged over 30 years show feasible CCA.Citation6 This calcification may appear in the form of nodular, or a verticolinear radiopacity inferior to the angulus mandible, adjacent to the C3–C4 intervertebral junction.Citation7–Citation9 However, PR is restricted to the diagnosis of the atheroma and cannot identify its exact location or degree of occlusion. Diagnosis may be made by means of ultrasonography, as a noninvasive and comparatively cheap technique.Citation6,Citation10
Many studies report the usefulness of the PR for identifying stroke patients by relationship with systemic diseases, cervical radiographs, or ultrasonography analysis.Citation5,Citation11,Citation12 But some studies were limited either by small sample sizes, or by not analyzing whether the carotid artery was actually calcified.Citation12,Citation13 There are not yet enough data confirming the relationship between the CCA shown on the PR and systemic diseases or smoking. Therefore, the present study was made to determine the reliability and prevalence of CCAs on PRs and relationship among systemic diseases, smoking, BMI and CCA in a group of patients aged over 45 years. As a result, careful evaluation of PRs could be lifesaving.
Materials and methods
Study population
In this study, a total of 1,650 PRs of patients aged over 45 years (736 males and 914 females) were retrospectively, randomly selected. All the patients had been referred to the Faculty of Dentistry, Afyon Kocatepe University, Afyonkarahisar, Turkey, during 2013–2014 for routine PR screening, and had recent, complete, medical records. The patients were contacted and informed consent was obtained from all the participants. The PRs had originally been taken for routine patient clinical examination and not for the investigation of CCAs. Approval for the study was granted by the Afyon Kocatepe University Faculty of Medicine Ethics Committee.
Patients were excluded if they had cancer or other serious comorbidities (and were thus not suitable for study), a previous stroke, or transient ischemic attack, since the aim was to study patients without any previous cerebrovascular event. When atheromatous plaque was detected, certain information (age, sex, smoking habits, weight, height, medical history, and uni/bilateral CCA appearance) was recorded. A total of 93 patients (43 male and 50 female, age range 45–84 years) with CCA on PR were included for evaluation in the study ( and ). CCA was checked via Doppler ultrasonography (DU) in 93 patients ( and ).
Figure 1 A panoramic radiograph of a 76-year-old female. There were bilateral multiple radiopacities of suspected calcified carotid atheromas (white circles) (Group A, study group).

Figure 2 A panoramic radiograph of a 56-year-old female. There was unilateral radiopacity of suspected calcified carotid atheroma (white circle) (Group B, control group).

Figure 3 A Doppler ultrasound image of a 76-year-old female. There was an evident calcified carotid atheroma (Group A, study group).
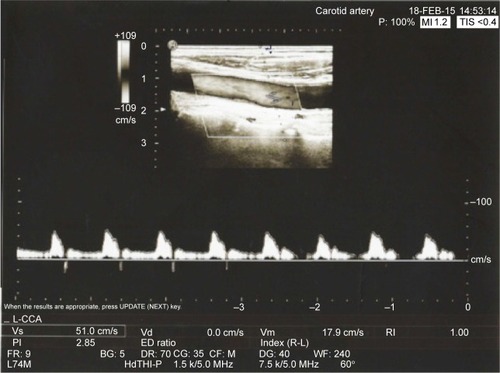
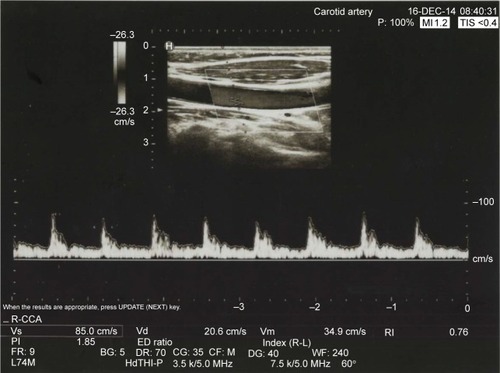
Figure 4 A Doppler ultrasound image of a 56-year-old female. There was no calcified carotid atheroma (Group B, control group).
The patients were divided into two groups as follows:
Group A (study group): CCA findings were tested by DU and CCA was confirmed (n=59).
Group B (control group): CCA findings were tested by DU but presence of CCA was not confirmed (n=34).
Hypertension was defined as current use of antihypertensive medication or systolic blood pressure of >140 mmHg and/or a diastolic blood pressure of >90 mmHg. Diagnosis of patients with diabetes was made from fasting plasma glucose >125 mg/dL. Body mass index (BMI) was classified according to WHO criteria with normal weight: 18–25 kg/m2; over weight, 25–30 kg/m2; obese class 1 (moderate obese), 30–35 kg/m2.Citation14
Panoramic radiography
PRs were taken at the Faculty of Dentistry, Afyon Kocatepe University, Afyonkarahisar, Turkey, using the Morita Vera-view IC-5 HD (Morita, Tokyo, Japan) panoramic X-ray systems. The range of exposure value was 1–7.5 mA and 60–70 kV depending on the patient’s size. The PRs were examined by one of the authors. Using the differential diagnosis of CCA described by FriedlanderCitation15 when there was a radiopaque nodular mass independent of the hyoid bone adjacent to the cervical vertebrae at or below the C3–C4 intervertebral disc level, or the retromandibular area, generally at an angle of about 45° from the angle of mandible, it was regarded as CCA. To minimize the discrepancy of observations, all PRs were evaluated by the same author.
Doppler ultrasonography
DU imaging studies of the carotid artery were performed at the Department of Radiology, Faculty of Medicine, Afyon Kocatepe University, Afyonkarahisar, Turkey, for all subjects to confirm the presence of CCA. All the ultrasound examinations were performed by the same radiologist, who was blinded to the findings on PR. Bilateral common carotid and proximal internal carotid arteries were examined with DU using a 7.5 MHz linear array transducer (Hitachi, Tokyo, Japan).
Statistical analysis
The prevalence and accuracy of CCA was calculated as the percentage of the total number of subjects. In the group comparisons of quantitative variables such as age and BMI, the Mann–Whitney U-test was used. In the evaluations of categorical data, the Pearson chi-square and the Fischer’s exact tests were applied in the comparisons between groups. A value of P<0.05 was accepted as statistically significant. All analyses were conducted using the SPSS version 14.0 statistical program.
Results
The screened population consisted of 736 (44.60%) males and 914 (55.40%) females with an age range of 45–84 years at the time the PRs were taken. Of the 1,650 individuals, 93 (5.63%) were detected to have CCA on PR. The population consisted of 43 males and 50 females with mean age of 59.84±10.92 years (male: 58±10.15 years, female: 61.12±11.49 years). No difference was determined in respect of CCA between the sexes (P=0.745).
In Group A, these CCA findings were confirmed by DU imaging as hyperechoic signals with distal acoustic shadow. This examination showed 63.44% accuracy for the detection of CCA using PR. The validated Group A comprised 59 patients: 28 males and 31 females with a mean age of 60.46±11.01 years (male: 59.07±10.85 years, female: 61.71±11.19 years). No statistically significant difference was determined in respect of CCA between the sexes (P=0.756).
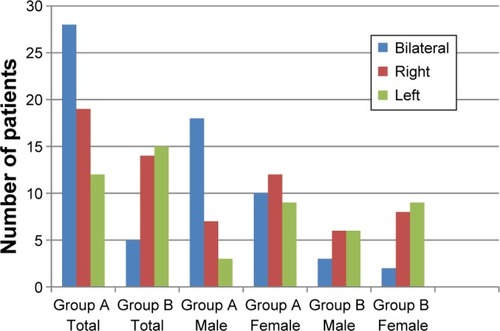
In Group A, CCA was identified as bilateral in 18 males and ten females and unilateral in ten males (seven right side, three left side) and 21 females (12 right side, nine left side) (, ). No significant difference was found between right and left side CCA (P=0.209). No statistically significant difference was determined in respect of left and right side CCA in both males and females (male, P=0.206; female, P=0.513).
Table 1 The demographic and medical records of Group A
Figure 5 Numerical distribution of radiographic findings of CCA according to sex and side.
Abbreviation: CCA, calcified carotid atheroma.
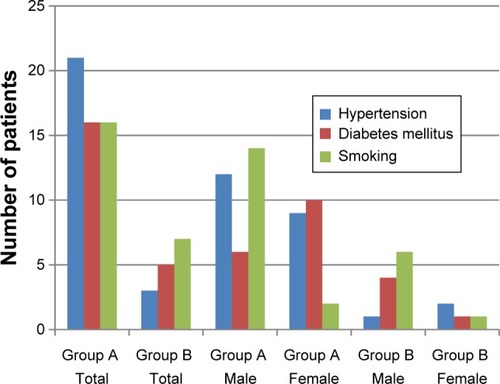
The systemic records of 59 patients in Group A were analyzed for the risk factors associated with CCA. shows the relationship between medical history, smoking, BMI, and CCA. In Group A, 21 (12 male, nine female) subjects (35.59%) reported hypertension, 16 (six male, ten female) subjects (27.11%) reported diabetes mellitus, and 16 (14 male, two female) subjects (27.11%) reported smoking (). Of these 59 patients, 12 (20.33%) were normal weight (BMI =18.5–25), 34 (57.62%) were overweight (BMI =25–30), and ten (16.94%) were moderately obese (BMI =30–35).
Figure 6 Numerical distribution of hypertension, diabetes mellitus, and smoking in Group A (study group) and Group B (control group) according to sex.
In Group B, verification of CCAs was tested by DU but no CCA was found. The 34 patients comprised 15 males and 19 females with a mean age of 58.76±10.84 years (male: 57±8.9 years, female: 60.16±12.21 years). No statistically significant difference was determined in respect of CCA between the sexes (P=0.493).
In Group B, CCA was identified as bilateral in three males and two females and unilateral in 12 males (six right side, six left side) and 17 females (eight right side, nine left side) (, ). No significant difference was determined between the right and the left sides of CCA (P=0.853). No statistically significant difference was determined in respect of left and right side CCA in both males and females (male, P=1.000; female, P=0.808).
Table 2 The demographic and medical records of Group B
The systemic records of 34 patients in Group B were analyzed for the risk factors associated with CCA. The correlations between medical history, smoking, BMI, and CCAs are shown in . In Group B, three (one male, two female) subjects (8.82%) reported hypertension, five (four male, one female) subjects (14.7%) reported diabetes mellitus, and seven (six male, one female) subjects (20.58%) reported smoking (). Of these 34 patients, eleven (three male, eight female) (32.35%) were normal weight (BMI =18.5–25 kg/m2), 19 (eight male, eleven female) (55.88%) were overweight (BMI =25–30 kg/m2), and four (four male, zero female) (11.76%) were moderately obese (BMI =30–35 kg/m2).
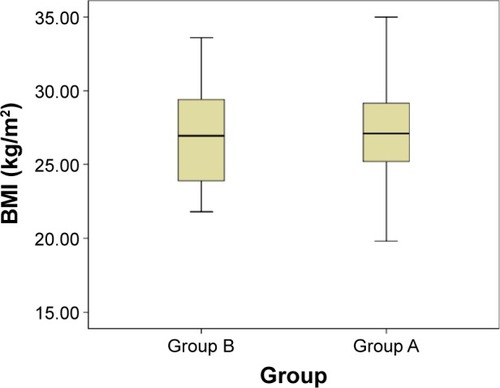
A statistically significant difference was determined between Group A and Group B in respect of hypertension rates (P=0.004). But there was no statistically significant difference between Group A and Group B in respect of age (P=0.495), BMI (P=0.756), diabetes (P=0.168), and smoking (P=0.482) distribution ( and ).
Figure 7 Comparison of BMI between Group A and Group B.
Abbreviation: BMI, body mass index.
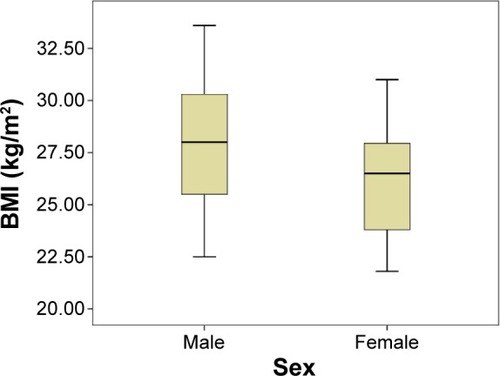
A statistically significant difference was determined between the males and females in Group A and Group B in respect of BMI rates (P=0.017, P=0.046) and smoking rates. (P=0.001, P=0.013) (, , and ). But there was no statistically significant difference between the males and females in Group A and Group B in respect of age distribution (P=0.327, P=0.444) and hypertension rates (P=0.291, P=0.691).
Figure 8 Comparison of BMI in Group A according to sex.
Note: Group A (study group).
Abbreviation: BMI, body mass index.
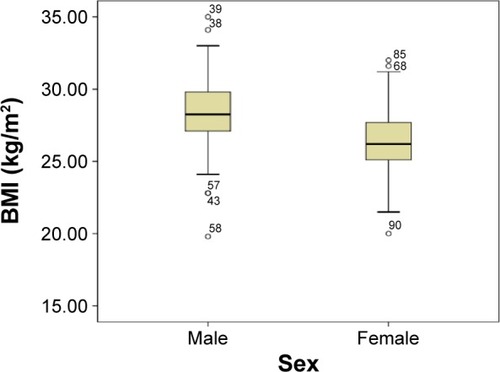
Figure 9 Comparison of BMI in Group B according to sex.
Abbreviation: BMI, body mass index.
A statistically significant difference was determined between the males and females in Group B in respect of diabetes rates (P=0.08). No statistically significant difference was determined between the males and females in Group A in respect of diabetes rates (P=0.35) ().
Discussion
Our aim was to determine the reliability of PR as a screening tool for the detection of CCA by comparing it with DU examination. A second aim was to evaluate the relationship among CCA, systemic diseases, smoking, and BMI in an older population. Group A was defined as the study group with findings confirmed by DU and Group B as the control group with findings were not confirmed by DU.
Friedlander and LandeCitation7 first found the incidence of CCA on PRs and suggested that the panoramic image may be a helpful in detecting patients at risk of stroke. Since the first report, many studies have been carried out to determine the incidence of CCA on PRsCitation5,Citation8,Citation16–Citation22 and to verify the useful ness of the PR in the identification of stoke-prone patients through correlation with medical history and Doppler spectral analysis.Citation5,Citation11,Citation12,Citation16–Citation18
DU is a method of examining vascular structures with sound waves. It provides hemodynamic information about the carotid and vertebral arteries. Despite sensitivity of 92.6% and specificity of 97%, angiography is accepted as the gold standard.Citation23 In the current study, DU was used for confirmation of CCA determined on PRs as it is a noninvasive method.
In our study, the diagnostic accuracy of PR for the detection of CCA was evaluated using DU. The results of this study showed 63.44% accuracy for the detection of CCA using PR. In a study by Yoon et alCitation24 similar accuracy was observed at 62.3%. In other studies, Baumann-Bhalla et alCitation25 and Almog et alCitation26 found the calcification rate with sonographic examination in atherosclerotic patients to be 81.5% and 65%, respectively. In the general population, the prevalence of CCA detected on PRs varies from 0.43% to 5% depending on age, sex, ethnicity, and lifestyle.Citation9,Citation16,Citation17,Citation26–Citation29 In the current study, a similar result of 5.63% CCA was determined in the general population. CCAs rates were not significantly different between males and females (P=0.756). The same finding of no difference in the male–female rates was reported by Ohba et al,Citation29 Bayram et al.Citation30 However, Tamura et alCitation31 identified a significant difference on PRs between the male and female rates. We thought that all these different CCA prevalences in female and male populations were probably due to ethnicity, eating habits, or social life.
In the present study in Group A and Group B, presumed CCA was identified on the left or right side, and no significant statistical differences were determined between the two sides. This finding differs from other studies, as in the majority of previous reports of normal populations,Citation8,Citation16,Citation31 CCA has been observed to be unilateral and located on the left side rather than the right side. However, Şişman et alCitation32 and Ohba et alCitation29 demonstrated CCA to be generally located on the right side. These differences in CCA localizations in the reports may be related to the study samples.
Studies showed that atherosclerotic lesions should be verified radiologically by a further diagnostic tool.Citation33,Citation34 It is thought that the reason for large differences in the CCA prevalence rates determined on PRs could be attributed to not making a differential diagnosis of the anatomic formations in the evaluation of the panoramic films. Several formations can appear as radiopacities in this region of the PR, including salivary calculi, calcified lymphoid tissue, tonsilloliths, the stylohyoid complex, and the triticeous cartilage.Citation35 False negatives may also be associated with the detection of CCA on PRs as the CCA may be inferior to the area covered by the PR or, if it is within this area, may not be visible because the degree of calcification is insufficient to be seen.Citation36
The sorting of obesity and overweight according to BMI by WHO is intended for international utilization. They show risk for type 2 diabetes and cardiovascular diseases, which are quickly becoming main reasons of death in adults.Citation14 In the present study, in the comparisons of Group A with Group B, no correlation was determined between CCA and BMI. This is consistent with the results of Irace et alCitation37 and Ertas and SismanCitation38 who reported that an increase in body weight is not associated with prevalence or degree of CCA. However, Carter et al found that obesity was most strongly related to the occurrence of CCA.Citation16 People with type 2 diabetes mellitus are disproportionately at risk of experiencing stroke, because hyperglycemia and other risk factors associated with diabetes accelerate the development of CCA. In a study by Friedlander, individuals with type 2 diabetes were determined to have high rates of atheroma visualized on PRs.Citation22,Citation39 The current study showed conflicting results with studies mentioned earlier, and there was no significant difference between Groups A and B in respect of diabetes mellitus. Especially, hypertension is one of the most important factors in atheroma formation and is crucial in patients with CCA.Citation40 In a study by Johansson et alCitation34 there was no significant difference between the group with stenosis and the group without stenosis in hypertensive patients. Pornprasertsuk-Damrongsri and ThanakunCitation8 found that patients with CCA were associated with hypertension (52.9%). Cohen et alCitation5 revealed that 53.5% of patients with CCA had a history of hypertension. In the current study, hypertension rates were found to be four times higher in Group A (35.59%) than in Group B (8.82%), and also was statistically significant. These conflicting results regarding CCA and systemic findings may be partly related to the size of samples in the studies or may be due to regional differences, lifestyle, and dietary factors.
In many epidemiological studies reported in literatures, smoking has been noted to be a major risk factor of cerebral infarction.Citation41–Citation43 The current study found that CCA was not affected by smoking, although in both groups, a significant difference was determined between the male and female population. We considered that decreased CCA prevalence in smoker persons are probably due to the amount of daily smoking or due to the less number of smoker individuals who participated in our study.
There were some limitations to the present study. Further study might be needed to clarify the clinical significance between PR and DU. No analysis was made of the appearance (intensity, size, and/or shape) of the calcification in the area of the carotid arteries on the panoramic images. These factors might be useful to select individuals for further carotid screening. Another limitation of the present study was the small number of subjects. Hypercholesterolemia could have been analyzed but that would have involved the invasive procedure of blood sampling and the associated ethical restrictions. The PRs in this study could have been evaluated by an oral and maxillofacial radiologist. However, as PRs are now found in nearly all dental clinics, the images are evaluated by dental practitioners. Therefore, it was aimed to provide an evaluation by physicians, not oral and maxillofacial radiologists.
Conclusion
Almost all patients undergo PR as part of their routine dental examinations and treatments.Citation44–Citation46 Although PR cannot be used as an initial diagnostic method when searching for CCA, dentists should be aware of CCA on routine PR, particularly in older patients who may also have the risk factors of obesity, diabetes mellitus, hypertension, and smoking. Recognition of CCA, especially in hypertensive patients, could potentially increase the length and quality of life for individuals. Proper findings of CCA and early referral for investigation could potentially decrease morbidity and mortality in the population. A medical consultation should be requested for all patients who present with CCA on PRs.
Acknowledgments
We would like to thank Dr Ismet Dogan for his support in statistical analyses.
Disclosure
The authors report no conflicts of interest in this work.
References
- WilliamsGRJiangJGMatcharDBSamsaGPIncidence and occurrence of total (first-ever and recurrent) strokeStroke1999302523252810582972
- WakhlooAKLieberBBSeongJHemodynamics of carotid artery atherosclerotic occlusive diseaseJ Vasc Interv Radiol200415S111S12115101520
- LevyCMandelLCalcified carotid artery imaged by computed tomographyInt J Oral Maxillofac Surg201068218220
- CarterLCTsimidisKFabianoJCarotid calcifications on panoramic radiography identify an asymptomatic male patient at risk for stroke: a case reportOral Surg Oral Med Oral Pathol Oral Radiol Endod1998851191229474626
- CohenSNFriedlanderAHJollyDADateLCarotid calcification on panoramic radiographs: an important marker for vascular riskOral Surg Oral Med Oral Pathol Oral Radiol Endod20029451051412374929
- BayerSHelfgenE-HBösCKrausDEnklingNMuesSPrevalence of findings compatible with carotid artery calcifications on dental panoramic radiographsClin Oral Investig201115563569
- FriedlanderAHLandeAPanoramic radiographic identification of carotid arterial plaquesOral Surg Oral Med Oral Pathol Oral Radiol Endod198152102104
- Pornprasertsuk-DamrongsriSThanakunSCarotid artery calcification detected on panoramic radiographs in a group of Thai populationSurg Oral Med Oral Pathol Oral Radiol Endod2006101110115
- KumagaiMYamagishiTFukuiNChibaMCarotid artery calcification seen on panoramic dental radiographs in the Asian population in JapanDentomaxillofac Radiol200736929617403886
- ManziFRBóscoloFNAlmeidaSMDNetoFHPanoramic radiography as an auxiliary in detecting patients at risk for cerebrovascular accident (CVA): a case reportJ Oral Rehabil200345177180
- FriedlanderAHGrattBMPanoramic dental radiography as an aid in detecting patients at risk for strokeJ Oral Maxillofac Surg199452125712627965328
- FriedlanderAIdentification of stroke-prone patients by panoramic and cervical spine radiographyDentomaxillofacial Radiol199524160164
- ChristouPLeemannBSchimmelMKiliaridisSMüllerFCarotid artery calcification in ischemic stroke patients detected in standard dental panoramic radiographs–a preliminary studyAdv Med Sci201055263120513642
- TanKAppropriate body-mass index for Asian populations and its implications for policy and intervention strategiesThe Lancet2004363157163
- FriedlanderAHPanoramic radiography: the differential diagnosis of carotid artery atheromasSpec Care Dentist1995152232279002923
- CarterLCHallerADNadarajahVCalamelADAguirreAUse of panoramic radiography among an ambulatory dental population to detect patients at risk of strokeJ Am Dent Assoc19971289779849231602
- FriedlanderAHBakerJDPanoramic radiography: an aid in detecting patients at risk of cerebrovascular accidentJ Am Dent Assoc1994125159816037798479
- FriedlanderAHManeshFWasterlainCGPrevalence of detectable carotid artery calcifications on panoramic radiographs of recent stroke victimsOral Surg Oral Med Oral Pathol Oral Radiol Endod199477669673
- FriedlanderAHFriedlanderIKYuehRLittnerMRThe prevalence of carotid atheromas seen on panoramic radiographs of patients with obstructive sleep apnea and their relation to risk factors for atherosclerosisJ Oral Maxillofac Surg19995751652110319824
- FreymillerESungEFriedlanderADetection of radiation-induced cervical atheromas by panoramic radiographyOral Oncol20003617517910745169
- SungECFriedlanderAHKobashigawaJAThe prevalence of calcified carotid atheromas on the panoramic radiographs of patients with dilated cardiomyopathyOral Surg Oral Med Oral Pathol Oral Radiol Endod20049740440715024368
- FriedlanderAHMaederLAThe prevalence of calcified carotid artery atheromas on the panoramic radiographs of patients with type 2 diabetes mellitusOral Surg Oral Med Oral Pathol Oral Radiol Endod20008942042410760724
- YurdakulSAytekinSDoppler ultrasound imaging of the carotid and vertebral arteriesTurk Kardiyol Dern Ars20113950851721918325
- YoonSYoonWKimOLeeJKangBDiagnostic accuracy of panoramic radiography in the detection of calcified carotid arteryDentomaxillofac Radiol200837210410818239037
- Baumann-BhallaSMeierRBurowARecognizing calcifications of the carotid artery on panoramic radiographs to prevent strokesSchweiz Monatsschr Zahnmed2012122111016102923184365
- AlmogDMHorevTIlligKAGreenRMCarterLCCorrelating carotid artery stenosis detected by panoramic radiography with clinically relevant carotid artery stenosis determined by duplex ultrasoundOral Surg Oral Med Oral Pathol Oral Radiol Endod20029476877312464905
- LewisDBrooksSCartoid artery calcification in a general dental population: a retrospective study of panoramic radiographsGen Dent1998479810310321159
- HubarJCarotid artery calcification in the black population: a retrospective study on panoramic radiographsDentomaxillofac Radiol19992834835010578188
- OhbaTTakataYAnsaiTEvaluation of calcified carotid artery atheromas detected by panoramic radiograph among 80-year-oldsOral Surg Oral Med Oral Pathol Oral Radiol Endod20039664765014600703
- BayramBUckanSAcikgozAMüderrisoğluHAydinalpADigital panoramic radiography: a reliable method to diagnose carotid artery atheromas?Dento maxillo facial radiology200635426627016798924
- TamuraTInuiMNakaseMNakamuraSOkumuraKTagawaTClinicostatistical study of carotid calcification on panoramic radiographsOral Dis20051131431716120119
- SismanYErtasETGokceCMenkuAUlkerMAkgunluFThe prevalence of carotid artery calcification on the panoramic radiographs in Cappadocia Region populationEur J Dent2007113219212556
- DamaskosSGriniatsosJTsekourasNReliability of panoramic radiograph for carotid atheroma detection: a study in patients who fulfill the criteria for carotid endarterectomyOral Surg Oral Med Oral Pathol Oral Radiol Endod200810673674218602315
- JohanssonEPAhlqvistJGaroffMKarpKJäghagenELWesterPUltrasound screening for asymptomatic carotid stenosis in subjects with calcifications in the area of the carotid arteries on panoramic radiographs: a cross-sectional studyBMC Cardiovasc Disord2011114421752238
- MacDonaldDOral and Maxillofacial Radiology: A Diagnostic ApproachAmes, IAWiley–Blackwell2011
- FriedlanderAHOdd practiceBr Dent J200920746446519942870
- IraceCScavelliFCaralloCSerraRCorteseCGnassoABody mass index, metabolic syndrome and carotid atherosclerosisCoron Artery Dis200920949919293666
- ErtasETSismanYDetection of incidental carotid artery calcifications during dental examinations: panoramic radiography as an important aid in dentistryOral Surg Oral Med Oral Pathol Oral Radiol Endod2011112e11e1721664149
- FriedlanderAHGarrettNRNormanDCThe prevalence of calcified carotid artery atheromas on the panoramic radiographs of patients with type 2 diabetes mellitusJ Am Dent Assoc20021331516152312462696
- MacDonaldDChanAHarrisAVertinskyTFarmanAGScarfeWCDiagnosis and management of calcified carotid artery atheroma: dental perspectivesOral Surg Oral Med Oral Pathol Oral Radiol201211453354722986250
- UeshimaHChoudhurySROkayamaACigarette smoking as a risk factor for stroke death in Japan NIPPON DATA80Stroke2004351836184115166389
- AbbottRDYinYReedDMYanoKRisk of stroke in male cigarette smokersN Engl J Med19863157177203748080
- NakayamaTDateCYokoyamaTYoshiikeNYamaguchiMTanakaHA 15. 5-year follow-up study of stroke in a Japanese Provincial City The Shibata StudyStroke19972845528996487
- Council on Dental Materials I, EquipmentRecommendations in radiographic practices: an update, 1988J Am Dent Assoc19891181151172913097
- KogonSBohayRStephensRA survey of the radiographic practices of general dentists for edentulous patientsOral Surg Oral Med Oral Pathol Oral Radiol Endod1995803653687489282
- ScandrettFRTeboHGMillerJTQuigleyMBRadiographic examination of the edentulous patient: Part I. Review of the literature and preliminary report comparing three methodsOral Surg Oral Med Oral Pathol1973352662744576432