Abstract
Adrenal incidentaloma (AI) is a term applied to an accidentally discovered adrenal mass on imaging performed for reasons unrelated to adrenal pathology. The widespread application of abdominal imaging procedure has resulted in an increased frequency of clinically silent adrenal masses. Although most AIs are nonfunctioning benign adenomas, a multidisciplinary approach with biochemical and radiological evaluation is needed to characterize these lesions and identify patients who are at high risk for hormonal or malignant evolution. Herein, we describe a case of a 69-year-old man with a pain at the base of right chest. On the basis of clinical evaluation, biochemical analysis, as well as imaging procedures, a diagnosis of right adrenocortical carcinoma was made. The patient underwent medical treatment.
Introduction
The widespread use of imaging, particularly computed tomography (CT) and magnetic resonance imaging (MRI), during diagnostic testing or treatment for many clinical conditions, has resulted in the identification of previously unsuspected adrenal lesions defined as adrenal incidentalomas (AIs).Citation1,Citation2 The assessment of AIs is aimed at deciding whether or not the tumor should be surgically removed,Citation3 adrenalectomy being indicated in hormonal hypersecretory states (such as pheocromocytoma) and in potentially malignant lesions.Citation4
Adrenal cortical carcinoma (ACC) is a rare and heterogeneous malignancy with incompletely understood pathogenesis and poor prognosis.Citation5 ACC can be functional or nonfunctional with regard to hormone synthesis and clinical features.
We report the case of a 69-year-old man who was investigated for chest pain, with a right adrenal carcinoma identified by total body CT-scan and adrenal scintigraphy.
Case report
A 69-year-old male was admitted to the Geriatric Unit of Catanzaro Hospital due to the onset of chest pain since few days, without other symptoms. Clinical examination and review of systems as well as family medical history were unremarkable. On clinical examination we found only a mild hepatomegaly and a reduction of vesicular murmur. In the past medical history, he reported a moderate increase of systolic and diastolic blood pressure which was controlled by weight reduction, salt restriction, and pharmacological therapy (ramipril plus hydrochlorothiazide 5/25 mg one tablet/day). In the present admission, blood pressure was 140/80 mmHg and heart rate 110 beats per min (bpm); patient’s body mass index was 36.36 Kg/m2. Chest X-ray was negative and electrocardiogram (ECG) recorded a sinus tachycardia. Biochemical analyses were normal () as well as hormonal evaluation (). We found only high levels of fibrinogen (697 mg/dL), lactate dehydrogenase (LDH; 758 U/L), α2-globulins (8.2%) ().
Table 1 Biochemical evaluation
Table 2 Endocrine work-up
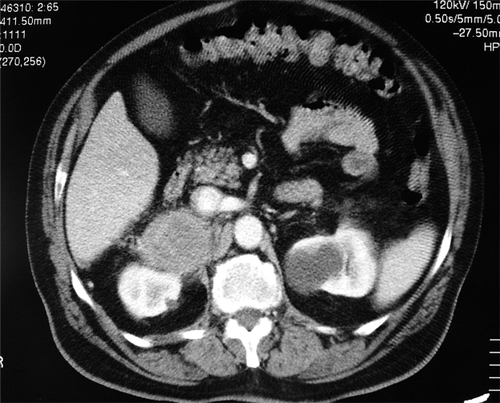
Following an abdominal ultrasound imaging (US), a 10-cm right adrenal lesion was identified ( and ). For this reason the patient underwent a total body CT-scan that revealed a 10-cm round, dense, heterogeneous enhancing lesion with irregular margins and inhomogeneous contrast enhancement of solid component after intravenous (iv) contrast medium. Local invasion (right liver lobe, renal hilus, and right diaphragm) and tumor extension into the inferior vena cava, as well as a tumor thrombus in the inferior vena cava and in the pulmonary arteries, were found. After 5 and 7 days, adrenal scintigraphy with iodocholesterol analogs showed a discordant pattern with absence of radiotracer uptake by the adrenal mass.
Figure 1 Abdominal computed tomography shows a 10-cm right adrenal lesion.
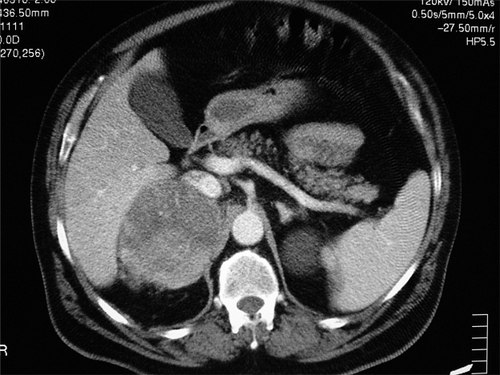
Figure 2 Abdominal computed tomography shows a 10-cm right adrenal lesion.
On the basis of these findings a diagnosis of “right adrenocortical carcinoma hormonally inactive” was made. Due to the invasive nature of the tumor we chose to put the patient on single agent mitotane.
Discussion
Incidentally discovered adrenal masses are found more frequently, so that all clinicians need to be aware of their etiology since each case needs to be treated individually. Patient age, general conditions, and tumor extension have to be taken into account; they may suggest avoiding combination therapy with other cytotoxic drugs and surgical treatment.
The true prevalence of AIs is unknown. Much of the information quoted is derived from autopsy series, in which the prevalence of undiagnosed adrenal masses ranges from 1.4% to 3%–6%.Citation6 These results resemble those emerging from imaging studies, in fact, the prevalence of AIs in daily radiological practice is up to 5% of CT examination performed for various reasons.Citation7
However, the prevalence of incidentally discovered adrenal masses increases with age, accounting for less than 1% in patients aged younger than 30 years, approximately 7% between the fifth and the seventh decades, and showing peak incidence in the sixth decade.Citation8
AI is not a single pathological entity. A recent studyCitation9 on the prevalence of incidental adrenal mass confirmed histologically, shows that adenomas and myelolipomas are the most common lesions, whereas adrenocortical carcinoma is about 0.1%.
ACC is a rare malignancy (incidence 1–2 per million people) and radiologic prevalence is clearly related to the size of the tumor, accounting for 2% of tumors that are 4 cm or less, 6% of tumors that are 4.1 to 6 cm, and 25% of tumors that are greater than 6 cm.Citation10 Clinical presentation is heterogeneous and prognosis is variable but generally poor,Citation11 in fact, overall, this neoplasia accounts for 0.02% to 0.2% of all cancer-related deaths, with a median survival of 18 months.
Women are more often affected than men (ratio 1:5);Citation12 this gender difference could be partly explained by the higher rate of diagnostic abdominal procedures recommended for women than men. The age distribution has two peaks: the first in childhood and the second in the fourth and fifth decade.Citation13
Pathogenesis was incompletely understood, mutation at the 17p13 locus, including the p53 tumor suppressor gene, is observed in about 25% of cases;Citation14 furthermore, alterations of the 11p15 locus, leading to IGF-II overexpression are frequently observedCitation15 compared to adenomas or normal adrenal cortex.
Patients present hormonal excess (virilization in women and gynecomastia and testis atrophy in men),Citation16 Cushing’s syndrome, or local effect mass in hormonally inactive ACC (nausea, vomiting, abdominal and back pain).Citation17
Biochemical screening for tumor hypersecretion as well as imaging evaluation is mandatory in all adrenocortical carcinomas to define the most correct approach. In fact, in stages I–II (localized or locally invasive tumor) complete tumor removal offers the best chance for cure by far,Citation16 in particular a complete resection.Citation18 In ACC sized more than 10 cm or with invasion of adjacent organs, local recurrence after surgery occurs in 40% of patients.Citation19
Our patient had an advanced tumor and diagnosis was belated due to the absence of hormonal excess symptoms. Considering our patient’s age, general conditions (hypertension, sinus tachycardia, obesity), invasivity and prognosis of the neoplasm, and the possibility of intraoperative complications, even after the negativity of biochemical work up (), we considered a medical therapy with mitotane.
Although adrenalectomy is the method of choice for the management of patients with ACC, being also compatible with a complete tumor resection in the presence of a tumor thrombus in the inferior vena cava,Citation20 medical treatment should be considered as an alternative to adrenalectomy in elderly patients, in those unwilling to undergo surgery, and in patients with comorbid conditions that preclude surgery.Citation21 In fact, while the presence of tumor thrombus may necessitate cardiac bypass technique, the prognosis of ACC still remains poor even after surgery with an overall five-year survival rate ranging between 16% and 38% in different series.Citation22 Moreover, survival is clearly related to the extent of disease.Citation23
Mitotane is the only adrenal-specific agent available for treatment of ACC, it exerts a specific cytotoxic effect on adrenocortical cells producing focal degeneration. In the first study on the efficacy of this therapy by Lim and colleagues,Citation24 seven of 18 patients with ACC showed significant tumor regression; even more favorable was the report by Lubitz and colleagues,Citation25 which described tumor regression in 61% of patients. A recent clinical review by Allolio and colleaguesCitation5 that analyzed the efficacy of mitotane treatment in advanced ACC, concluded that mitotane leads to an objective tumor regression in about 25% of cases.
Although a complete response (or even cure) in patients with advanced ACC is extremely rare, long-term survival has been reported;Citation26 in fact our patient is alive and in good clinical conditions six months after surgery.
Disclosure
The authors report no conflicts of interest in this work.
References
- AlexandrakiKIGrossmanABAdrenal incidentalomas: the “rule of four”Clin Med2008820120418478872
- PrinzRABrooksMHChurchillRIncidental asymptomatic adrenal masses detected by computed tomographic scanning. Is operation required?JAMA19822487017047097921
- SinghPKBuchHNAdrenal incidentaloma: evaluation and managmentJ Clin Pathol2008611168117318955573
- GrumbachMMBillerBMBrownsteinGDManagement of the clinically in apparent adrenal mass (incidentaloma)Ann Intern Med200313842442912614096
- AllolioBFassnachtMClinical review: adrenocortical carcinoma: clinical updateJ Clin Endocrinol Metab2006912027203716551738
- MansmannGLauJBalkERothbergMMiyachiYBornsteinSRThe clinically inapparent adrenal mass: update in the diagnosis and managementEndocr Rev20042530934015082524
- KloosRTGrossMDFrancisIRKorobkinMShapiroBIncidentally discovered adrenal massesEndocr Rev1995164604848521790
- BarzonLBoscaroMDiagnosis and management of adrenal incidentalomasJ Urol200016339840710647642
- SongJHChaudryFSMayo-SmithWWThe incidental adrenal mass on CT: prevalence of adrenal disease in 1,049 consecutive adrenal masses in patients with no known malignancyAJR Am J Roentgenol20081901163116818430826
- VierhapperHHeinzeGGesslAExnerMAdrenocortical tumors; prevalence of impaired glucose tolerance and of “Paradoxical Rise” of cortisol during an oral glucose tolerance testExp Clin Endocrinol Diabetes200311141542014614648
- StratakisCAChrousosGPAdrenal cancerEndocrinol Metab Clin North Am200029152510732261
- Del GaudioADDel GaudioGAVirilizing adrenocortical tumors in adult woman. Report of 10 patients, 2 of whom each had a tumor secreting only testosteroneCancer199372199720038364880
- WootenMDKingDKAdrenal cortical carcinoma. Epidemiology and treatment with mitotane and a review of the literatureCancer199372314531558242539
- ReinckeMKarlMTravisWHP53 mutations in human adrenocortical neoplasms: Immunohistochemical and molecoular studiesJ Clin Endocrinol Metab1994787907948126158
- HeppnerCReinckeMAgarwalSKMEN1 gene analysis in sporadic adrenocortical neoplasmsJ Clin Endocrinol Metab1999842162199920087
- Vassilopoulou-SellinRSchultzPNAdrenocortical carcinoma. Clinical outcome at the end of the 20th centuryCancer2001921113112111571723
- CrucittiFBellantoneRFerranteABischeriniMCrucittiPThe italian registry for adrenal cortical carcinoma: analysis of a multiinstitutional series of 129 patients. The ACC Italian registry study groupSurgery19961191611708571201
- BodieBNovickACPontesJEThe Cleveland clinic experience with adrenal cortical carcinomaJ Urol19891412572602913342
- PorteHSiatJGuibertBResection of adrenal metastases from non-small cell lung cancer: a multicenter studyAnn Thorac Surg20017198198511269485
- ManteroFTerzoloMArnaldiGA survey on adrenal incidentaloma in ItalyClin Endocr Metab2000852637644
- HaakHOHermansJvan de VeldeCJOptimal treatment of adrenocortical carcinoma with mitotane: results in a consecutive series of 96 patientsBr J Cancer1994699479518180029
- IcardPGoudetPCharpenayCAdrenocortical carcinoma: surgical trends and results of a 253-patient series from the French Association of Endocrine Surgeons Study GroupWorld J Surg20012589189711572030
- WajchenbergBAlbergariaPMMedoncaBAdrenocortical carcinoma: clinical and laboratory observationsCancer20008871173610679640
- LimMCTanYOChongPYCheahJSTreatment of adrenal cortical carcinoma with mitotane: outcome and complicationsAnn Acad Med Singapore1990195405442171414
- LubitzJAFreemanLOkunRMitotane use in inoperable adrenal cortical carcinomaJAMA1973223110911124739370
- AllolioBHahnerSWeismannDFassnachtMManagement of adrenocortical carcinomaClin Endocrinol (Oxf)20046027328715008991