
Abstract
Background
Although sarcopenia represents a challenging burden for health care systems around the world, its prevalence in the elderly population varies widely. The primary aim of the study was to determine the prevalence of sarcopenia in community-dwelling (CD) German women aged 70 years and older; the secondary aim was to assess the effect of osteoarthritis (OA) on sarcopenia prevalence in this cohort.
Methods
A total of 689 Caucasian females 18–35 years old and 1,325 CD females 70 years+ living in Northern Bavaria, Germany, were assessed during the initial phase of the FORMoSA research project. Anthropometry, total and regional muscle mass, were assessed by segmental multifrequency Bioelectrical Impedance Analysis. Further 10 m walking speed and handgrip strength were evaluated to apply the European Working Group on Sarcopenia in Older People definition of sarcopenia. Covariates were determined by questionnaires and interviews.
Results
Applying the algorithm of the European Working Group on Sarcopenia in Older People of two standard deviations below the mean value for appendicular skeletal muscle mass of a reference cohort of the young cohort (5.66 kg/m2), low gait speed (≤0.8 m/s), and low grip strength (<20 kg), the prevalence of sarcopenia in CD German females 70 years and older was 4.5% (70–79 years: 2.8% vs ≥80 years: 9.9%; P<0.001). Participants with OA at the hip and lower limbs (n=252) exhibited significantly higher rates of sarcopenia (OA: 9.1 vs non-OA: 3.5%). Of importance, anthropometric, demographic, health, and lifestyle parameters (except exercise participation) of our cohorts corresponded with Bavarian or German data for CD women 70 years+.
Conclusion
The prevalence of sarcopenia in CD German females 70 years+ is relatively low. However, participants with OA at the hip or lower limbs were at increased risk for sarcopenia.
Introduction
Sarcopenia, defined as an age-related loss of muscle mass and low muscle function, may be the most prominent component of frailty, disability, and morbidity in older people.Citation1,Citation2 Although this relatively new geriatric syndromeCitation3 represents a challenging burden for health care systems not only, but particularly, in developed countries,Citation4 its prevalence in the elderly population was reported to vary widely.Citation5 For example, for comparable European industrial nations (Belgium, Denmark, Finland, France, Holland, and Northern Italy), the prevalence of sarcopenia for female cohorts 70 years+ ranges from 0.9%Citation6 to 52.9%.Citation7 This finding was related to different definitions of sarcopenia with varying methods, cutoffs, and algorithms.Citation8,Citation9 Additionally, the specific national situation with its social background and health resources may affect the transition from independence to institutionCitation10 and thus the prevalence of sarcopenia in the older community-dwelling (CD) cohort.
In Germany, the prevalence of sarcopenia in CD older people is unknown. However, to generate tailored interventions, it would be important to identify the prevalence of this geriatric syndrome in this cohort. Thus, the primary aim of this article was to determine the prevalence of sarcopenia in Germany according to the European Working Group on Sarcopenia in Older People (EWGSOP) definitionCitation8 that may be the most accepted protocol in this area. Our second and subordinated research question addressed a more clinical issue and evaluates whether and to which degree osteoarthritis (OA) of the hip and lower limbs, which is rather common in older people, was related to higher sarcopenia prevalence rates.
Our main hypothesis was that the prevalence of sarcopenia according to the EWGSOP-proposal is relatively low (<5%) in CD German females 70 years and older. The secondary hypothesis was that the prevalence of sarcopenia is significantly higher in participants with OA at the hip and lower limbs compared with nonarthritic peers.
Methods
The FORMoSA project (Bavarian Research Association – Sarcopenia and Osteoporosis) was implemented by a Bavarian research network that addresses sarcopenia and osteoporosis under several research aspects. Our research group focuses on the prevalence and nonpharmacologic therapy of sarcopenia and sarcopenic obesity in older females. This article is based on screening data (July–November 2014) from the project. The study was initiated by the Institute of Medical Physics and the Institute of Biomedicine of Aging, University of Erlangen-Nuremberg, Germany and approved by the University Ethics committee (Ethikantrag 905, 4209, 4914 B). All study participants gave written informed consent. FORMoSA was registered under www.clinicaltrials.gov (NCT2356016).
Primary endpoint
Sarcopenia as defined by the EWGSOP.Citation8
Participants
Using citizen registration records, the entire population of 7,908 female participants 70 years and older, living independently in the area of Erlangen, Germany, were contacted by personal letters with detailed study information including the most relevant eligibility criteria for the study. Of the 1,401 women who replied, 1,343 were included in the screening process after application of our eligibility criteria: 1) females, 70 years and older and 2) living independently (autonomous at home, in the community) in the area of Erlangen. Participants were assessed independent of their race; however, only white (Caucasian) participants were included in the analysis (n=1,325). shows the characteristics of the eligible participants.
Table 1 Characteristics of CD female participants 70 years and older living (n=1,325)
Assessment of sarcopenia
Sarcopenia was defined per the algorithm of the EWGSOPCitation8 (). Correspondingly, we applied a gait speed of ≤0.8 m/s and a handgrip strength of <20 kgCitation11 to determine cutoff values for our female cohort. Following Baumgartner,Citation12 low muscle mass was defined as a relative appendicular skeletal muscle mass (ASMM; kg/m2) of two standard deviations (SDs) below the mean value of a reference cohort of 689 Caucasian females 18–35 years old (Teschler scoreCitation13). The sample was collected between February and August 2014 in seven different locations of northern Bavaria. With respect to anthropometric (eg, body mass index and body fat) and demographic (eg, family and educational status and lifestyle) parameters, this cohort can be considered as representative for young BavarianCitation14 and German females.Citation15 shows the characteristic of this cohort.
Table 2 Characteristics of young (Caucasian) female adults 18–35 years old (n=689) living in northern Bavaria
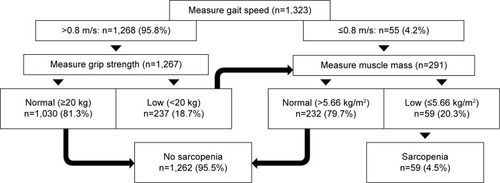
Figure 1 Flowchart when applying the EWGSOP algorithm on 1,325 community-dwelling females 70 years and older living in northern Bavaria, Germany.
Assessment of anthropometry and body composition parameter
Height was assessed using a Harpenden stadiometer (Holtain Ltd, Crymych, Pembs, UK), body mass, and composition (total and regional fat and fat-free body mass) were determined using segmental multifrequency Bioelectrical Impedance Analysis (BIA; Inbody 770, Biospace Co., Ltd., Seoul, Korea). This device was used to measure impedance of the trunk, arms, and legs separately with a tetrapolar eight-point tactile electrode system that applied six frequencies (1, 5, 50, 250, 500, and 1,000 kHz).
Total ASMM was based on the sum of the lean body mass (LBM) of the extremities (upper and lower limbs). Relative ASMM was calculated by dividing the total muscle mass (kg) by the height squared (m2). Using the relative ASMM mean value of −2 SDs of the young reference sample (), the cutoff value for sarcopenia for our cohort was ≤5.66 kg/m2.
Assessment of functional sarcopenia parameters
Muscle strength
Handgrip strength was measured using a Jamar hand dynamometer (Sammons Preston Inc, Bollington, USA). The width of the dynamometers grip was individually adjusted to the hand size of the participant. Tests were performed in an upright standing position, arms down by the side. Two test trials were performed, both for the dominant and nondominant hand; the best trial was included in the analysis.
Gait speed
Gait speed was assessed according to the 10 m test protocol of Fritz and Lusardi.Citation16 Tests were performed twice without any walking aims. Participants were asked to walk 14 m in their usual gait speed using their regular shoes. Participants started in a standing position 2 m before the first photo sensors (HL 2–31, TagHeuer, La Chaux-de-Fonds, Switzerland) and stopped 2 m after the second photo sensors, resulting in a steady-state measurement over 10 m.
Assessment of OA
Questionnaires, personal interviews, and medical letters were used to determine OA. First, all the participants were requested complete general questionnaires to report the incidence of OA and other relevant diseases (see “General characteristics, covariates, and comorbidity” section). Questionnaires were checked by research assistants in close cooperation with the participants. Subjects who listed or reported diseases after inquiry were further interviewed with respect to the corresponding disease. Initially, 246 participants suffered from OA. However, after detailed inquiry, only those subjects who said they had OA based on the diagnosis of their physician were requested to complete a questionnaire that asked for incidence, severity, and localization of OA (n=241). The research assistants then interviewed those participants to verify the data. In cases of doubt, written OA indications attested by the responsible physician were requested. OA indication of nine participants was vague and not confirmed by their physician; thus, in total, 232 subjects were included in the OA group.
General characteristics, covariates, and comorbidity
Beside general characteristics (eg, family and educational status, occupational career, and menopausal age), questionnaires and short interviews were conducted with all participants (n=1,343) to ascertain diseases, medication, and lifestyle with special emphasis on physical activity and fitness using a dedicated questionnaire.Citation17 Participants were asked to list their medication and diseases at home, and the research assistants then checked the questionnaire for completeness and accuracy together with the participant. Specific interviews and questionnaires aimed at confirming and operationalizing specific diseases (eg, osteoporosis, coronary heart diseases, diabetes mellitus, OA) listed by the participants were finally conducted in close cooperation with the participants. In cases of doubt, written indications attested by the responsible doctor were requested.
Statistical analysis
Descriptive statistics (ie, mean values with SD (MV ± SD), and proportions) were used to describe characteristics and key parameters of the study cohort. Additionally, the range and 95% confidence interval have been given in to characterize the young study cohort that represents the basis of our T-Score-derived relative ASMM calculationCitation12 more clearly.
Differences between the groups categorized for either age ( and ) or OA () were consistently calculated using Welch t-test for continuous variable and chi-square test or, when appropriate, Fisher’s exact test for categorical variables. In detail, the corresponding statistical tests for each group comparison can be found in the legends of , , and . Although at least our secondary hypothesis would allow a one-tailed test procedure, for consistency and conservativeness, all the tests were analyzed with a more discrete two-sided testing procedure with a P-value of less than 0.05 considered as statistically significant. SPSS 21.0 (SPSS Inc, Chicago, IL, USA) was used for all statistical procedures.
Table 3 Sarcopenia parameters in 1,325 community-dwelling females 70 years and older living in northern Bavaria, Germany
Table 4 Characteristics of study participants with and without osteoarthritis of the hip and lower limbs
Results
General characteristic of the study participants were given in . With respect to anthropometric data, lifestyle, number and distribution of diseases, and medication, the results for our cohort coincide with Bavarian and German data.Citation15,Citation18 The same is true for family, education, and social status (not given in ). Further, the age distribution among our cohort was comparable with Bavarian or German data for CD females 70 years and older.Citation15
Prevalence of sarcopenia in German (Northern Bavaria) women 70 years and older
shows the parameters that constituted “sarcopenia” according to the EWGSOP proposalCitation8 for all (n=1,325), women <80 years (n=1,022) and women 80 years and older (n=303). Significant differences between the groups (<80 vs ≥80 years) were observed for all sarcopenia criteria.
Applying the algorithm of the EWGSOP proposal (), the prevalence of sarcopenia in our cohort was 4.5% (70–79 years: 2.8% vs ≥80 years: 9.9% P<0.001) (). In detail (), only 55 women failed to reach the cutoff value of ≤0.8 m/s for gait speed and were thus immediately assessed for muscle mass. For the remaining 1,268 females faster than 0.8 m/s, a grip strength lower than 20 kg (n=237) led to a subsequent muscle mass assessment, while subjects with normal grip strength (and normal gait speed) were defined as nonsarcopenic. Thus, finally muscle mass was determined in the 291 remaining women. Following the EWGSOP criteria for low muscle mass (ie, ≤5.66 kg/m2 for our cohort), altogether 59 subjects were categorized as “sarcopenic” while 232 were nonsarcopenic according to the EWGSOP algorithm.Citation8
Thus, hypothesis 1 confirmed that the prevalence of sarcopenia in CD females 70 years and older was low (<5%).
Effect of OA on sarcopenia prevalence
shows the characteristics of participants with and without OA at the hip and lower limbs. As expected, age varies significantly between the groups; however, total difference only averaged ≈1.3 years. More importantly, the groups differ significantly (P<0.001) for parameters that may relevantly affect muscle mass and functional capacity (ie, body fat, number of diseases, long-term glucocorticoid use, physical fitness, and participation in sports and exercise).
Differences of sarcopenia parameters given in were not consistently aligned. While functional sarcopenia parameters were significantly lower in women suffering from OA at hip and lower limbs compared with women without OA (−10% to 12%; P<0.001), a slightly higher relative ASMM (0.6%, P=0.480) was determined for the arthritic participants.
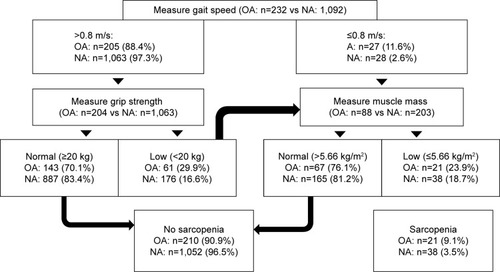
In parallel to and the EWGSOP algorithm described earlier, shows the procedure to determine sarcopenia prevalence in participants with OA and without OA (no arthritis [NA]) at the hip, knee, or ankle joint. In accordance with the descriptive sarcopenia parameters given in , the proportion of women meeting the sarcopenia criteria for gait speed (≤0.8 m/s: OA: 11.6% vs NA: 2.6) and grip strength (<20 kg: OA: 29.9% vs NA: 16.6%) differs significantly (P=0.001) between the groups. Also, the difference between OA and NA participants with low muscle mass (≤5.66 kg/m2) remained nonsignificant (OA: 23.9 vs NA: 18.7; P=0.327) during the final step (measure muscle mass) of the EWGSOP assessment. However, the low(er) sample size of remaining participants during this final step may contribute to the lack of significant results.
Figure 2 Flowchart when applying the EWGSOP algorithm in community-dwelling females 70 years and older with respect to their osteoarthritis status (OA vs NA).
In summary, the prevalence of sarcopenia in women with OA compared with NA peers was significantly higher than in women without corresponding limitation.
Thus, hypothesis 2 confirmed is that the prevalence of sarcopenia was significantly higher in participants with OA compared with nonarthritic peers.
Discussion
To our knowledge, this is the first study to address the prevalence of sarcopenia in CD older females in Germany. In summary, the overall prevalence rate was relatively low (4.5%) in this cohort of Bavarian (German) females 70 years and older. This can also be applied for our subgroup of females 80 years or older (9.9%). Reviewing the literature, Cruz-JentoftCitation5 reported a prevalence rate of 1%–30% in women 50 years and older. Although only studies that applied the EWGSOP definition (ie, muscle mass, muscle strength, or functional performance) were included, the methods to determine these parameters vary widely. As an example, the study that reported the highest sarcopenia rate (30.1%) determined midarm circumferenceCitation19 in Italian females 80–85 years old. Additionally, the inconsistency of the diagnostic muscle mass criteria (eg, LBM, SMM, and ASMM), the corresponding calculation (ie, muscle mass adjusted for height,Citation12 weight,Citation20 or/and fat massCitation21,Citation22), and the cutoff definition (T-Score vs Z-Score based) complicate a meaningful comparison of the present studies.
Limiting the data to CD European females 70 years and older applying the EWGSOP algorithm and using dual-energy X-ray absorptiometry (DXA) or segmental multifrequency BIA devices to determine ASMM (kg/m2), sarcopenia prevalence ranges from 0.9% in 70- to 80-year-old Finnish womenCitation6 to 20.2% for a female Belgian cohort 65 years and older.Citation23 Our result basically confirmed the lower rates of Patil et al,Citation6 especially when taking into account that the authors used the lower ASMM cutoff value of Baumgartner et alCitation12 (≤5.45 kg/m2). Application of this lower cutoff point resulted in a sarcopenia prevalence of 3.1% in our cohort (70–79: 1.8% vs ≥80 years: 7.6%). Revisiting the study of Beaudart et alCitation23 in one of their eight approaches, the authors applied sarcopenia cutoff points (ASMM: ≤5.67 kg/m2,Citation21 gait speed <0.8 m/s, grip strength <20 kg) nearly identical to the present study. However, although the Belgian cohort (n=243) was slightly younger (73.8±6.2 vs 76.4±4.9 years), its sarcopenia prevalence was more than three times as high (16%) compared with the present study. It is implausible that difference with respect to body-composition assessment (ie, DXA vs BIA) contributes to this result since both Patil et alCitation6 and Beaudart et alCitation23 used DXA devices. Additionally, it is rather unlikely that slight variations with respect to functional testing (eg, 4 vs 10 m walking trial, stopwatch vs automatic timers) could lead to such differences. Although Pasma et alCitation24 reported a significantly higher gait speed for 10 m compared with the 4 m walking trial in a cohort of elderly outpatients, this result was not confirmed for healthy, CD elderly people 65 years and older.Citation25 However, it is noticeable that gait speed among the present study (1.29±0.23 m/s) was considerably higher than described for a comparable cohort.Citation26 In contrast, per the EWGSOP algorithm, participants with gait speed above 0.8 m/s were not excluded but assessed additionally for handgrip strength, which proved to be in the range of normative data for this cohort,Citation27 however.
Thus, in summary, the finding that sarcopenia prevalence may considerably vary between neighboring countries despite highly comparable or even identical sarcopenia definition, criteria, method, cutoff, sex, age, social system, and origin was unexpected and should be addressed by dedicated studies.
Addressing our second and subordinated research topic, we demonstrated that sarcopenia prevalence in CD women 70+ years was significantly higher in women with OA at the hip and lower limbs.
Indeed, clinical evidence suggests that both conditions may be linked via functional and cellular pathways.Citation28 With respect to the functional pathway, lower limb muscle weakness favors OA progression and vice versa.Citation29,Citation30 Indeed, habitual walking speed was significantly lower in the OA group compared with the NA group, a result confirmed by Waters et alCitation31,Citation32 Additionally, a higher proportion among our OA group (OA: 19% vs NA: 13%) showed OA of the hand and finger joints, which may explainCitation33 the lower handgrip strength of this group. However, we are unable to determine a lower ASMM (or lower limb muscle mass) in the OA subgroup compared with the NA group (). This finding was not expected. In addition to the functional interaction of muscle and cartilage, chondrocytes and skeletal muscle cells share common pathological pathways;Citation28 thus, muscle mass in participants with OA should be reduced. However, a recent review the literature on OA and sarcopenia (ie, low muscle mass)Citation34 stated that neither a direct effect of sarcopenia on OA development nor the opposite relation can be supported on the basis of the present literature. In summary, although more dedicated studies should address this issue, the study provided some evidence that OA contributed to the development of sarcopenia in elderly females. As a clinical implication, physicians should be aware of an increased risk of sarcopenia in their patients with OA. Consequently, these patients should be encouraged to start dedicated exercise programs and protein/vitamin D supplementation to maintain or increase their muscle mass.
However, some features or limitations may reduce the evidence of the present studies, especially with respect to our secondary hypothesis: 1) It can be argued that the spatial restriction on a single German region and/or incomplete compliance of the participants contacted (16.8%) generated a sampling bias that prevents generalization of our results. We are unable to completely negate this argument, although the most important anthropometric (eg, body mass index and age distribution), demographic (eg, education and family status), and health (eg, diseases and medication) and lifestyle parameters (eg, smoking, and habitual physical activity) of our cohort corresponded with Bavarian or German data for CD women ≥70 years.Citation15,Citation18,Citation35 However, participation in sports and exercise by our cohort (59.5%) was considerably higher than reported for the basic population of German females ≥65 years (50.8%). Since the study participants undertaking exercise demonstrated a significantly higher gait speed compared with their sedentary peers (1.32 vs 1.18 m/s), this may contribute to the exceptionally high gait speed in our cohort. Due to varying exercise participation in the OA vs NA group (), this factor may also affect the OA/sarcopenia issue, although the corresponding cause–effect association (ie, chicken–egg problem) remains unclear.Citation28 2) A limitation with respect to our second research aim was the cross-sectional nature of the study with the corresponding restricted ability to determine causal effects. 3) Also our procedure for recording OA incidence via questionnaires and interviews alone was suboptimum. Retrospectively, a specific evaluation of OA using more sophisticated assessments and diagnostic tools may have allowed a more comprehensive analysis including the application of logistic regression models to determine the independent effect of OA on sarcopenia prevalence. 4) With respect to body composition assessment, we decided to use segmental multifrequency BIA for two main reasons. First, BIA is considered as a time- and cost-effective technique with portable devices and thus optimal for screening of large cohorts.Citation36 Further, due to the lack of radiation, this technique is highly accepted and can be applied without any ethical or administrative restrictions. With respect to the accuracy of this technique, Beaudart et alCitation37 reported a systematic overestimation of muscle mass when compared with DXA that is still the “golden standard”. However, other researchers and we do not share this opinion.Citation38–Citation40 Particularly, Ling et alCitation38 reported an “excellent agreement” of BIA (InBody 720, Biospace Ltd, Seoul, Korea) and DXA (QDR 4500a; Hologic, Bedford, MA, USA). In any case, since our cutoff for “low muscle mass” is based on either a young reference cohort (<−2 SD T-Score) or the distribution (lowest quintile) within the own cohort as assessed with the same BIA device, prevalence rates should not be affected.
Author contributions
All of the authors 1) made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; 2) drafted the article or revised it critically for important intellectual content; 3) finally approved the version to be published; and 4) agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Acknowledgments
This work was supported by the “Bayerische Forschungsstiftung” (Munich, Germany) (grant number AZ 1044-12) and the “Universitätsbund Erlangen-Nürnberg” (grant number 21/2015).
Disclosure
The authors report no conflicts of interest in this work.
References
- MilteRCrottyMMusculoskeletal health, frailty and functional declineBest Pract Res Clin Rheumatol201428339541025481423
- FriedLPGuralnikJMDisability in older adults: evidence regarding significance, etiology, and riskJ Am Geriatr Soc1997451921008994496
- Cruz-JentoftAJLandiFTopinkovaEMichelJPUnderstanding sarcopenia as a geriatric syndromeCurr Opin Clin Nutr Metab Care20101311719915458
- JanssenIShepardDSKatzmarzykPTRoubenoffRThe healthcare costs of sarcopenia in the United StatesJ Am Geriatr Soc2004521808514687319
- Cruz-JentoftAJLandiFSchneiderSMPrevalence of and interventions for sarcopenia in ageing adults: a systematic review. Report of the International Sarcopenia Initiative (EWGSOP and IWGS)Age Ageing201443674875925241753
- PatilRUusi-RasiKPasanenMKannusPKarinkantaSSievanenHSarcopenia and osteopenia among 70-80-year-old home-dwelling Finnish women: prevalence and association with functional performanceOsteoporos Int201324378779622688541
- ZoicoEDi FrancescoVGuralnikJMPhysical disability and muscular strength in relation to obesity and different body composition indexes in a sample of healthy elderly womenInt J Obes Relat Metab Disord200428223424114708033
- Cruz-JentoftAJBaeyensJPBauerJMSarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older PeopleAge Ageing201039441242320392703
- FieldingRAVellasBEvansWJSarcopenia: an undiagnosed condition in older adults. Current consensus definition: prevalence, etiology, and consequences. International working group on sarcopeniaJ Am Med Dir Assoc201112424925621527165
- Lloyd-SherlockPEpidemiological change and health policy for older people in developing countries: some preliminary thoughtsAgeing Horizons200522124
- LauretaniFRussoCRBandinelliSAge-associated changes in skeletal muscles and their effect on mobility: an operational diagnosis of sarcopeniaJ Appl Physiol20039551851186014555665
- BaumgartnerRNKoehlerKMGallagherDEpidemiology of sarcopenia among the elderly in New MexicoAm J Epidemiol199814787557639554417
- KemmlerWvon StengelSTeschlerMPrävalenz von Sarkopenie und Sarcopenic Obesity bei selbstständig lebender Frauen über dem 70. Lebensjahr [Prevalence of sarcopenia and sarcopenic obesity in community dwelling females 70 years and older]Osteologie201524120
- BayLfStaDStatistisches Jahrbuch für Bayern 2014 [Statistical annual for Bavaria 2014]MünchenBayerisches Landesamt für Statistik2014
- DESTATISStatistisches Jahrbuch 2014 [Statistical annual 2014]Wiesbaden, GermanyStatistisches Bundesamt2014
- FritzSLusardiMWhite paper: “walking speed: the sixth vital sign”J Geriatr Phys Ther2009322464920039582
- KemmlerWWeineckJKalenderWAEngelkeKThe effect of habitual physical activity, non-athletic exercise, muscle strength, and VO2max on bone mineral density is rather low in early postmenopausal osteopenic womenJ Musculoskelet Neuronal Interact20044332533415615501
- Verteilung der Bevölkerung auf Body-Mass-Index-Gruppen in ProzentStatistisches Bundesamt2012 Available from: https://www.gbe-bund.de/stichworte/BMI.htmlAccessed March 30, 2015
- LandiFLiperotiRRussoAAssociation of anorexia with sarcopenia in a community-dwelling elderly population: results from the ilSIRENTE studyEur J Nutr20135231261126822923016
- JanssenIHeymsfieldSBRossRLow relative skeletal muscle mass (sarcopenia) in older persons is associated with functional impairment and physical disabilityJ Am Geriatr Soc200250588989612028177
- DelmonicoMJHarrisTBLeeJSAlternative definitions of sarcopenia, lower extremity performance, and functional impairment with aging in older men and womenJ Am Geriatr Soc200755576977417493199
- NewmanABKupelianVVisserMSarcopenia: alternative definitions and associations with lower extremity functionJ Am Geriatr Soc200351111602160914687390
- BeaudartCReginsterJYSlomianJBuckinxFLocquetMBruyereOPrevalence of sarcopenia: the impact of different diagnostic cut-off limitsJ Musculoskelet Neuronal Interact201414442543125524968
- PasmaJHStijntjesMOuSSBlauwGJMeskersCGMaierABWalking speed in elderly outpatients depends on the assessment methodAge (Dordr)2014366973625479936
- PetersDMFritzSLKrotishDEAssessing the reliability and validity of a shorter walk test compared with the 10-Meter Walk Test for measurements of gait speed in healthy, older adultsJ Geriatr Phys Ther2013361243022415358
- BohannonRWWilliams AndrewsANormal walking speed: a descriptive meta-analysisPhysiotherapy201197318218921820535
- DesrosiersJBravoGRejeanHDutilENormative Data for grip strength of elderly men and womenAm J Occup Ther19944976376447573334
- De CeuninckFFradinAPastoureauPBearing arms against osteoarthritis and sarcopenia: when cartilage and skeletal muscle find common interest in talking togetherDrug discovery today201419330531123973339
- ConroyMBKwohCKKrishnanEMuscle strength, mass, and quality in older men and women with knee osteoarthritisArthritis Care Res20126411521
- ScottDBlizzardLFellJJonesGProspective study of self-reported pain, radiographic osteoarthritis, sarcopenia progression, and falls risk in community-dwelling older adultsArthritis Care Res20126413037
- WatersRLPerryJConatyPLunsfordBO’MearaPThe energy cost of walking with arthritis of the hip and kneeClin Orthop Relat Res19872142782843791753
- ZeniJAHigginsonJSKnee osteoarthritis affects the distribution of joint moments during gaitThe Knee201118315615920510618
- DingMOdgaardAHvidIAccuracy of cancellous bone volume fraction measured by micro-CT scanningJ Biomech199932332332610093033
- PapaliaRZampognaBTorreGSarcopenia and its relationship with osteoarthritis: risk factor or direct consequence?Musculoskeletal surgery201498191424482109
- Robert-Koch-InstitutDaten und Fakten: Ergebnisse der Studie »Gesundheit in Deutschland aktuell 2012« [Data and facts: results of the “health in germany study 2012”]BerlinRobert-Koch-Institut2014
- RubbieriGMosselloEDi BariMTechniques for the diagnosis of sarcopeniaClinical Cases in Mineral and Bone Metabolism: the Official Journal of the Italian Society of Osteoporosis, Mineral Metabolism, and Skeletal Diseases2014113181184
- BeaudartCReginsterJYSlomianJEstimation of sarcopenia prevalence using various assessment toolsExp Gerontol201561313725449859
- LingCHde CraenAJSlagboomPEAccuracy of direct segmental multi-frequency bioimpedance analysis in the assessment of total body and segmental body composition in middle-aged adult populationClinical Nutrition201130561061521555168
- ShaferKJSidersWAJohnsonLKLukaskiHCValidity of segmental multiple-frequency bioelectrical impedance analysis to estimate body composition of adults across a range of body mass indexesNutrition2009251253218723322
- von StengelSKemmlerWEngelkeKValidität von BIA im Vergleich zur DXA bei der Erfassung der Körperzusammensetzung [Validity of BIA to determine body composition. A comparison with DXA]Dtsch Z Sportmed2013627/8200
- SchaferIvon LeitnerECSchonGMultimorbidity patterns in the elderly: a new approach of disease clustering identifies complex interrelations between chronic conditionsPLoS One2010512e1594121209965