
Abstract
Aims
Carefully designed and established biobanks are considered one of the most essential resources to foster biomedical research as they provide cost-effective and rapid access to a vast variety of biological materials and related anthropometrics allowing for testing of various biomarkers as well as numerous original and pertinent bioclinical hypotheses related to human disease etiology and prognosis. The objective of the present study was to present the baseline data, design, and methods used for the establishment of the Vejle Diabetes Biobank. Further aims included assessment of the prevalence of diabetes and quality of diabetes treatment in a specified Danish region.
Methods
The Vejle Diabetes Biobank was established from 2007 to 2010 as a regional Biobank containing blood, DNA, and urine samples from patients with diabetes and a gender- and age-matched control population aged 25–75 years. Anthropometrics were obtained by physical examination, questionnaires, and interviews at the time of inclusion into the Biobank. The cohort was linked to the Danish Civil Registration System, the Danish National Patient Registry, and the Danish National Prescription Registry.
Results
In total, 4,255 nondiabetic individuals and 3,320 patients with diabetes were included. Type 2 diabetes (T2D) patients had a higher body mass index (30 kg/m2) than type 1 diabetes (T1D) patients (25 and 26 kg/m2 in women and men, respectively) and control subjects (25 and 27 kg/m2 in women and men, respectively). Fasting levels of plasma triglycerides and blood pressure were higher in T2D patients (1.5 mmol/L and 148/85 mmHg, respectively) compared with T1D patients (0.9 mmol/L and 139/81 mmHg, respectively), whereas glycated hemoglobin (HbA1c), plasma high density lipoprotein, low density lipoprotein, and total cholesterol were lower in T2D patients (51 mmol/mol, 1.2 mmol/L, 2.2 mmol/L, and 4.2 mmol/L, respectively) compared with findings in T1D patients (61 mmol/mol, 1.6 mmol/L, 2.3 mmol/L, and 4.4 mmol/L, respectively). At the time of inclusion into the Biobank, 56% of the T2D patients and 25% of T1D patients had an HbA1c <7% (53 mmol/mol). Only 28% and 34% of the T2D patients, respectively, reached treatment target for blood pressure and lipids.
Conclusion
The Vejle Diabetes Biobank represents one of the largest open diabetes case-control cohorts in Denmark. The Biobank invites collaborative investigations of diabetes and diabetes complication etiologies as well as studies of prognostic or predictive biomarkers.
Background
Biobanks have become one of the most valuable resources in biomedical researchCitation1 as they provide cost-effective and rapid access to a vast spectrum of biological materials and related anthropometric data allowing for comprehensive studies, often to be shared by multiple research environments. Recently, a Canadian studyCitation2 suggested that biorepositories coordinating the activity of biobanking “rank among the most important of established health research infrastructures as contributors to research publications.” Biobanking of human biological materials together with relevant coupling to national disease and mortality registries enable longitudinal follow-up, improved opportunity of understanding disease mechanism, and contribute to documentation of quality and lifelong patient outcomes.
The primary objective for establishing the Vejle Diabetes Biobank was to enable the investigation of prognostic and predictive values of a variety of possible etiological components. Further, to investigate the prognostic and predictive value of biomarkers for development of diabetes, its associated complications, and outcomes. Repeated data analyses were performed during follow-up on patients with time.
The objective of the present study is to present the baseline data, design, and methods used for the establishment of the Vejle Diabetes Biobank and provide information about the quality of diabetes patient treatment at the time of the establishment of the Biobank with the ultimate goal of providing information about the resource for national and international investigators in this research field.
Materials and methods
Recruitment of study participants
The Vejle Diabetes Biobank was established as a regional Biobank containing blood and urine samples from individuals with diabetes and a gender- and age-matched control population aged between 25 and 75 years (both ages included) as of the inclusion date per December 31, 2006.
Subjects eligible for the cohort were identified using information from the Civil Registration System.Citation3,Citation4 The identified diabetes and control populations were limited to individuals who were alive and residing in the former County of Vejle area on December 31, 2006. These eligible individuals received an information letter asking them to participate in the Biobank as diabetes or control subjects, respectively. In case of not responding, an information letter was sent as a reminder. The subjects participating were not given any compensation for their donation of blood and urine.
Individuals who responded positively subsequently received a questionnaire (Supplementary material) to fill in at home and were given an appointment at one out of four hospitals in the predefined region of Denmark (Vejle, Kolding, Fredericia, and Horsens) for anthropometric examinations and biological sampling. The participants were asked to fast overnight from 10 p.m. and to abstain from physical activity 72 hours before their appointment for entering the Biobank. They were examined by laboratory technicians or healthcare assistants at the respective hospital and the completed questionnaire was reviewed together with the participant. The patients’ verification of the diabetes diagnosis was considered the gold standard;Citation5 thus, only subjects acknowledging having diabetes were included in the diabetes cohort. The participants requested as control individuals were likewise asked if they acknowledged not having diabetes. Only subjects acknowledging no diabetes were included in the control cohort.
The inclusion and exclusion criteria for the diabetic cohort
The patients with diabetes were identified by the following inclusion criteria of which at least one criteria had to be met: A) At least one glycated hemoglobin (HbA1c) value ≥6.6% (≥48.6 mmol/mol) registered in the Clinical Laboratory Information System (LABKA),Citation6 in the period from January 1996 to December 2006. B) At least three HbA1c values <6.6% (48.6 mmol/mol) registered in LABKA in the period from January 2002 to December 2006. C) Patients registered in the Danish National Prescription RegistryCitation7 with at least one prescription handled in the former County of Vejle in the period from January 1, 2006 to December 31, 2006 for oral antidiabetic agents or insulin with the Anatomical Therapeutic Chemical (ATC) Classification SystemCitation8 code A10A (insulin) and/or A10B (oral antidiabetic agents). D) All patients registered in the Danish National Patient RegistryCitation9 with a contact (inpatient- or outpatient-based) in the period from 1977 to December 2006Citation10 at hospitals in the former County of Vejle with a diabetes diagnosis (both primary and secondary diagnoses) (International Classification of Diseases [ICD] code 250 [Eighth Revision] and/or codes DE10 and/or DE11 [Tenth Revision] [ICD10], which is in use since 1994 in Denmark).Citation11
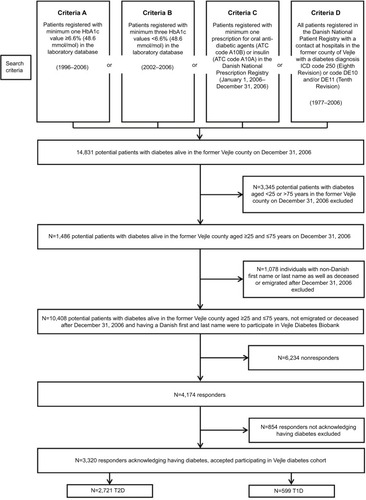
Based on the above-mentioned four criteria, the eligible study participants for the diabetes sample comprised of 14,831 patients who potentially might suffer from diabetes, of whom 3,345 were excluded due to age under 25 or age above 75 years.
In order to minimize the enrolment of individuals with a different genetic background than Danish, individuals with a non-Danish first name and/or last name were not asked to participate in the Biobank (n=647 corresponding to 6% of the diabetic population selected). Detailed information on the inclusion of diabetes patients is given in flow diagram (). In total, 10,408 potential diabetic individuals were asked to participate in the Vejle Diabetes Biobank, whereof 4,174 responded positively (response rate of 40%). In total, 3,320 individuals consented to join the Vejle Diabetes Biobank as patients with diabetes. The patients were classified according to their own statement as either type 1 diabetes (T1D) or type 2 diabetes (T2D) patients as previously validated by Kristensen et al.Citation5 Patients who did not have knowledge of their own classification (~2%) were stratified based on the following criteria for T2D and T1D, respectively; T2D: diabetes debut after the age of 30 years and treatment with oral antidiabetic agents (ATC Classification System code A10B) for at least 1 year following time of diagnosis and/or dietary treatment after diagnosis, and T1D: treatment with insulin or insulin analogues from time of diagnosis (ATC Classification System code A10A) without any oral antidiabetic agents (ATC Classification System code A10B). According to the above stated criteria, 599 patients were classified as T1D patients and 2,721 patients were classified as T2D patients ().
Figure 1 Selection of patients with diabetes for the Vejle Diabetes Biobank.
Inclusion and exclusion criteria for individuals in the control cohort
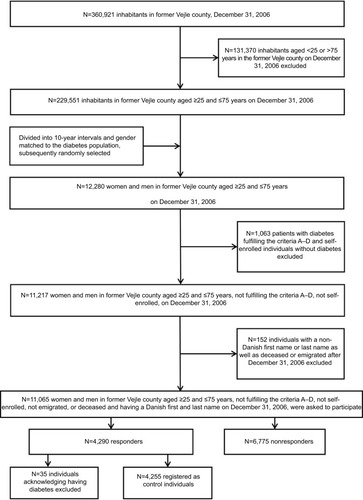
The individuals for the control cohort were selected by the Danish Civil Registration System from the background population of the former County of Vejle, Denmark (n=360,921). Planned sampling was 1:1.
All citizens of the County of Vejle aged ≥25 and ≤75 years (n=229,551) and alive at the inclusion date December 31, 2006 were divided into 10-year age intervals in order to obtain a random control from the background population, and gender-matched to the diabetes population, subsequently randomly selected. Of the 11,065 control subjects who received a request to participate in the Biobank, 4,290 chose to participate (response rate of 39%). Thirty-five subjects who did not fulfill any of the four diabetes criteria A–D but acknowledged having diabetes were excluded from the control population. In total, the control population constituted of 4,255 individuals without diabetes. Detailed information on the inclusion of the control persons is given in flow diagram ().
Figure 2 Selection of participants without diabetes for the Vejle Diabetes Biobank.
Anthropometrics
The following anthropometrics were examined during the visit at the enrolment in the Vejle Diabetes Biobank: height (ultrasound height rod, Soehnle Industrial Solutions GmbH, Backnang, Germany), weight with indoor clothes but without shoes, body mass index (BMI) calculated by dividing weight in kilograms by the squared height in meters,Citation12 body fat percentage (Tanita Body Composition Analyzer 418, IL, USA), waist and hip circumference was measured according to World Health Organization standard,Citation13 and systolic and diastolic blood pressures were measured after 5 minutes rest in sitting position (Omron M5 Professional, Osaka, Japan).
The following information was obtained through the questionnaire: smoking status (daily, occasionally, former-smoker, ever-smoker), alcohol consumption (none, occasionally, 1–7 units per week, 7–14 units per week, 14–21 units per week, more than 21 units per week), exercise habit (no, yes; if yes: number of times per week, number of minutes per time; low intensity, moderate intensity, high intensity), gestational diabetes (yes, no), age at onset of diabetes, heart diseases (eg, acute myocardial infarction, angina pectoris, congestive heart failure), cerebral diseases (eg, stroke), late diabetic complications: eyes, kidneys, nerves, foot ulcers (yes, no, not known), diabetes in parents/siblings and/or children (yes, no), diabetes medication (insulin, glucagon-like peptide 1 analogues/dipeptidyl peptidase IV inhibitors, biguanides [metformin] alone or in drug combinations, β-cell stimulating drugs [ie, sulfonylurea and meglitinides], alpha-glucosidase inhibitors, glitazones), and other medication (cholesterol-lowering agents, anticoagulants, antihypertensive drugs (angiotensin converting enzyme [ACE]-inhibitors, angiotensin 2 receptor [AT2]-antagonists, β-blockers, calcium antagonists, renin-inhibitors, diuretics, other).Citation14
Advocating and advertising for participating in the biobank were repeatedly done in the local media and information flyers were distributed at the general practitioners in the local area and the outpatient clinics at the four hospitals participating in the recruitment as an attempt to improve the response rate.
Biological sample collection and storage conditions
In the period from March 1, 2007 to May 1, 2010, blood (125 mL) and urine (10 mL, first-morning urine sample brought by the participant) samples were collected from each participant at attendance and plasma, serum, and buffy coat were separated, aliquoted, and stored at ‒80°C until analysis.Citation14 In total, for every subject, 56 tubes of serum, ethylenediaminetetraacetic acid (EDTA)- and Li-heparin plasma, EDTA whole blood, and buffy coat were stored centrally at Vejle Hospital.
Blood samples were analyzed for HbA1c, fasting plasma glucose (FPG), C-peptide, triglycerides, total cholesterol, high and low density lipoproteins (HDL, LDL), middle sensitive CRP (measurable down to 0.3 mg/L), p-albumin, calcium, alanine aminotransferase (ALAT), and p-creatinine. Due to financial restrictions, ALAT and p-creatinine in the control population were analyzed in February 2016 on Cobas 8000 (Hoffmann-La Roche Ltd., Basel, Switzerland), whereas in the diabetes population it was analyzed in 2009–2010 on a Modular P system (Hoffmann-La Roche Ltd.). Urine samples in the diabetes cohort were analyzed for U-albumin, U-creatinine, U-protein, and U-albumin/creatinine ratio. GFR was estimated by the use of the CKD-EPI equation.Citation15
Venous blood for FPG measurements was drawn from an antecubital vein in tubes containing Li-heparin (Venosafe®, Terumo Europe NV, Leuven, Belgium). The samples were immediately cooled in ice water, centrifuged at 5°C at 3,000× g for 10 minutes, and plasma separated within 30 minutes.Citation16 Aliquots of plasma were stored at −80°C until analysis. Glucose measurements as well as triglycerides, total cholesterol, HDL, LDL, CRP, p-albumin, calcium, ALAT, p-creatinine, U-albumin, U-creatinine, U-protein, and U-albumin/creatinine ratio were performed on a Modular P system (Hoffmann-La Roche Ltd.). Total imprecision and analytical bias were controlled by external HK1 control material purchased from the Danish Institute for External Quality Assurance for Laboratories in Health Care, Glostrup, Denmark.Citation17 The analyses performed in the laboratory fulfilled the generally accepted criteria for bias and coefficient of variation.Citation18,Citation19
All samples were thawed in an incubator until reaching a temperature of 37°C, then mixed by vortexing and centrifuged at 2,000× g for 10 minutes before analyzing. Whole blood samples for HbA1c measurements were drawn from the same puncture as for FPG analysis. Samples were collected in tubes containing EDTA (K3E, Venosafe) and stored at −80°C until analysis.Citation14 HbA1c analysis was carried out on a fully automated glycohemoglobin analyzer (Tosoh HLC-723 G7, Tosoh, Tessenderlo, Belgium) with total analytical imprecision <1.8% Diabetes Control and Complication Trial (DCCT) in the range 5.0–9.0 HbA1c%, corresponding to <2.7% International Federation of Clinical Chemistry (IFCC) in the range 31–75 mmol/mol.Citation16 Analytical bias was assessed by external control materials (no. 3044 F1) from LabqualityCitation20 and in the analyzing period positive bias was measured below 3.5% in the range 5.0%–9.0% in DCCT units (below 5.2% IFCC in the range 31–75 mmol/mol), which was acceptable according to the DCCT/National Glycohemoglobin Standardization Program criteria.Citation21 C-peptide was analyzed on an Advia Centaur System (Siemens Healthineers, Erlangen, Germany).
Sample size and selection considerations
The goal of the establishment of the Vejle Diabetes Biobank was to include all patients with T2D aged between 25 and 75 years in the former Vejle County. All patients with possible diabetes were thus primarily elected. For case-control genotyping studies, statistical power calculation demonstrated a power allowing for the detection of common genetic risk variants with an allele frequency of >10% with a relative risk (RR) of 1.3 based on the inclusion of 1,000 patients with T2D (cases) and 1,000 control persons. At allele frequency of >35% in the same setup, the calculation demonstrated a statistical power of 80% for the identification of genetic risk variants with an RR of 1.2. In this study having more than 2,000 cases and over 4,000 controls, a statistical power of 80% will allow for identification of genetic risk variants with an allele frequency of >8% with an RR of 1.3.
Follow-up
The prospect of the Biobank was estimated to 10–15 years with consecutive follow-up data analysis on the existing data without repeated sampling.
Data sources
The cohort was linked to the Danish Civil Registration SystemCitation3,Citation4 and the Danish National Patient RegistryCitation9 in 2011 and again in August 2015. Since the establishment in 1968, the Civil Registration System identifies all living and deceased persons in Denmark by using the Danish Personal Identification Number. This is a 10-digit number unique for every citizenCitation4 and used for all purposes involving health care, social, and administrative transactions. The Danish Civil Registration System provides information about vital status, emigration, or in case of deceased subjects the date of death, whereas the Danish National Patient Registry contains records of all hospital contacts (in- and outpatient) and ICD8 and ICD10 diagnostic codes.Citation10,Citation22 The Danish National Prescription RegistryCitation7 was accessed in the initial phase in order to find patients registered with at least one prescription in the period from January 1, 2006 to December 31, 2006 for oral antidiabetic agents or insulin. LABKA was accessed in order to obtain the laboratory data produced.
Validation of the anthropometrics
Data were visualized by graphic presentation and checked for reliability and consistency. Flawed data were corrected according to primary data source.
Treatment goals
The latest recommended target for glycemic regulation in nonpregnant adults with diabetes is HbA1c <7.0% (53 mmol/mol), although it is recognized that some diabetes patients may benefit from less strict control (HbA1c <7.5%–8.0%, 58–64 mmol/mol) and others from a more rigorous control (HbA1c <6.0%–6.5%, 42–48 mmol/mol).Citation23–Citation27 For these reasons, the analyses of the diabetes cohort at several HbA1c limits were done. For comparison over time, the authors also did the analysis with a target limit for normalization of HbA1c of 6.6% (48.6 mmol/mol) corresponding to the 99.9 percentile limit in a nondiabetic population in the former Vejle County as previously documented.Citation28 This limit was also used in the inclusion criteria A and B for the diabetes population.
Regarding hypertension, it is recommended to maintain the systolic blood pressure below 140 mmHg and the diastolic blood pressure below 90 mmHg.Citation29 The guidelines on antihypertensive treatment in diabetes patients recommend either an ACE-inhibitor or AT2 antagonist as first choice.
In managing the dyslipidemia closely related to T2D, it is recommended to treat patients aged ≥40 years with statins, dosage dependent on the presence of cardiovascular disease risk factors.Citation29 The targets are triglycerides <1.7 mmol/L (150 mg/dL), LDL <2.6 mmol/L (100 mg/dL), HDL ≥1.0 mmol/L (40 mg/dL) for men and ≥1.3 mmol/L (50 mg/dL) for women, and total cholesterol <4.5 mmol/L.
Statistical methods
Normally distributed data are presented as mean ± standard deviation; nonparametric data are presented as median and 25–75 percentiles. For the statistical analyses, SPSS version 23 (IBM Corporation, Armonk, NY, USA) and the R project for statistical programming (R version 3.2.3) were used.
Ethics
The study was approved by the Danish Data Protection Agency (j. no. 2006-53-1385 and j. no. 2008-58-0035) and by The Regional Scientific Ethical Committees for Southern Denmark (j. no. S-20080097).
Results
In total, 4,255 control persons with no diabetes and 3,320 patients with diabetes, hereof 2,721 T2D patients and 599 T1D patients, were included from March 1, 2007 to May 1, 2010.
Anthropometrics and biochemistry
The baseline characteristics of the study participants in the Vejle Diabetes Biobank are described in . It is evident that T2D patients were heavier and had a higher median BMI (30 and 30 kg/m2 in women and men, respectively) than T1D patients (25 and 26 kg/m2 in women and men, respectively) and control subjects (25 and 27 kg/m2 in women and men, respectively). Plasma triglycerides and blood pressure were higher in T2D patients (1.5 mmol/L and 148/85 mmHg, respectively) compared with T1D patients (0.9 mmol/L and 139/81 mmHg, respectively), whereas plasma HDL was lower in T2D patients (1.2 mmol/L) than in T1D patients (1.6 mmol/L). HbA1c was lower in T2D patients (51 mmol/mol) compared to T1D patients (61 mmol/mol); moreover, plasma LDL and total cholesterol levels were lower in T2D patients (2.2 and 4.2 mmol/L, respectively) compared to T1D patients (2.3 and 4.4 mmol/L). Plasma levels of CRP and ALAT in women were, despite being in normal range, elevated in T2D patients compared with both controls and T1D patients. The plasma concentration of ALAT in men was higher in T2D patients compared to T1D patients.
Table 1 Baseline characteristics of the study population in the Vejle Diabetes Biobank
Quality of diabetes care
The distribution of patients fulfilling key quality criteria for diabetes treatment is demonstrated in and , . As shown in , 56% and 32% of patients with T2D, respectively, had HbA1c <7.0% and <6.5%, at time of inclusion into the cohort (2007–2010). Correspondingly for patients with T1D, 25% and 11% presented with HbA1c <7.0% and <6.5%, respectively. In this period, 37% (42% of T2D and 16% of T1D) were below the 99.9 percentile limit of 6.6% (). The percentage of patients reaching the recommended treatment targets for blood pressure and circulating levels of triglycerides, LDL, and HDL is visualized in , . HbA1c <7%, systolic blood pressure, triglycerides, and LDL cholesterol are depicted in and .
Figure 3 HbA1c: Cumulative percentage of individuals and HbA1c (%), females and males, respectively, in T2D patients (solid curve), T1D patients (dotted curve), and control individuals (dot-dash curve). Vertical solid line: HbA1c =7%.
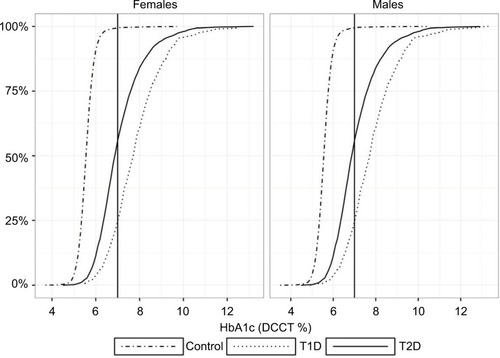
Figure 4 (A) Cumulative percentage of individuals and systolic blood pressure (mmHg), females and males, respectively, in T2D patients (solid curve), T1D patients (dotted curve) and control individuals (dot-dash curve). Vertical solid line: systolic blood pressure =140 mmHg. (B) Cumulative percentage of individuals and triglycerides (mmol/L), females and males, respectively, in T2D patients (solid curve), T1D patients (dotted curve), and control individuals (dot-dash curve). Vertical solid line: triglycerides =1.7 mmol/L. (C) Cumulative percentage of individuals and LDL (mmol/L), females and males, respectively, in T2D patients (solid curve), T1D patients (dotted curve), and control individuals (dot-dash curve). Vertical solid line: LDL =2.6 mmol/L.
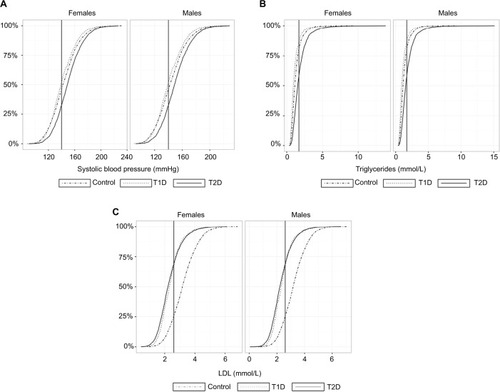
Table 2 Number and percentage of subjects in each group reaching stated criteria for HbA1c
Table 3A Percentage and number of females fulfilling the stated key criteria
Table 3B Percentage and number of males fulfilling the stated key criteria
In this Vejle cohort, 28% of the T2D patients achieved the treatment target for blood pressure (140/90 mmHg) compared with 48% in T1D patients (); 81% and 89% of T2D and T1D patients, respectively, were treated with at least an ACE-inhibitor or AT2 antagonist, whereas only 50% of the control population treated with antihypertensive agents received an ACE-inhibitor or AT2 antagonist.
Table 4 Percentage and number of subjects fulfilling the stated criteria
Of the 2,721 patients with T2D, 74% were treated with cholesterol-lowering agents, and among the T2D patients aged ≥40 years, 74% received statins. However, the percentage of T2D patients aged ≥40 years having a serum total cholesterol >4.5 mmol/L and not being treated with statins was 44% (). Thirty-four percent of the T2D and 55% of the T1D patients met treatment targets for serum lipids ().
Table 5 Highlights of findings for T2D and T1D patients
Discussion
Behind the idea of establishing the Vejle Diabetes Biobank was an intention to increase the etiological knowledge about T2D and its comorbidities and to enhance the quality of diabetes care on the population level as well as for the individual patient. Along with the expanding genetic knowledge and the economic restriction in most healthcare systems, there has been a growing demand for individually precision tailored and targeted intervention. Biorepositories are in this regard most valuable resources as they allow for investigation of etiologies and intermediate, predictive, and prognostic biomarkers of disease of interest as well as of comorbidities; hence, new analytical tests with potential predictive value for diabetes or its related complications can be tested before being used prospectively.Citation30
The strength of the Vejle Diabetes Biobank is its well-characterized individuals, completeness, and extent of laboratory, genetic, and anthropometric variables. This provides valuable data on modifiable lifestyle cardiovascular risk factors as body weight, BMI, blood pressure, smoking status, and physical activity. The possibility of linkage between the cohort and various Danish national population registries (eg, the Danish National Patient Registry, the Danish Civil Registration System and the Danish National Prescription Registry) gives access to consecutive information on the diabetes prognosis. The Vejle Diabetes Biobank represents one of the largest diabetes case-control cohorts in Denmark sampled from the same geographic area. Another biobank, the nationwide Danish Diabetes DD2 cohort, has since spring 2011 systematically collected and stored blood, urine, and obtained questionnaires from newly diagnosed T2D patients.Citation31–Citation33 This gives unique follow-up possibilities from time of diagnosis, but only ~5% of incident T2D patients per year are enrolled in the DD2 cohortCitation30 making the risk of selection bias substantially high. Further, the DD2 has no control cohort. In the Vejle Diabetes Biobank, both the diabetes and the control population show a response rate of 39%–40%. This is a level corresponding to similar investigations based on voluntary participation.Citation34
The limitation of the Vejle Diabetes Biobank is the lack of repeated sampling and repeated questionnaires over time, thus limiting the laboratory data and anthropometrics to the time of entry into the cohort. This can however partly be compensated by the ability to search clinical and laboratory data covering all patients in the region, and stored in national accessible registries. Further, the study is limited by the fact that the study participants have not been followed from their birth or the time of diagnosis and delayed entry will bias all attempts on absolute mortality estimation.Citation35
As previously demonstrated,Citation36 only 8% in 1993 and 22% in 2001 of patients with diabetes in the Vejle County had HbA1c below the 99.9 percentile limit of 6.6% (48.6 mmol/mol). In 2007–2010, 37% (42% of patients with T2D and 16% patients with T1D) were below the 6.6% limit, which is a significant increase in percentage of diabetes patients achieving glycemic regulation (HbA1c) below 6.6% of 29 and 15 percentage points, respectively. The former statistics was performed on the basis of all HbA1c measures available in the laboratory database in the Vejle County from both hospitals and primary care centers, counting both T2D and T1D patients. In the present study, the statistics analyses were done only among the Vejle Diabetes Biobank participants (40% responders). This fact might contribute to a better result due to the selection bias as it is well known that participants often are of better health and belong to a higher socioeconomic group than the nonparticipants.Citation22 Consistent with this, the authors previously showed that participants in the Vejle Diabetes Biobank, both diabetic and control individuals, had a significantly lower number of registered diagnoses, ie, lower Charlson Comorbidity Index Score,Citation37 than their nonparticipant counterparts and demonstrated all over healthier biomarkers.Citation38
Having improved diabetes care over the years by better glycemic regulation and increased focus on the importance of controlling the patient’s cardiovascular risk factorsCitation39,Citation40 and modifying the lifestyle, there still seems to be room for improvement as only less than six out of ten T2D patients (56%) and only one out of four T1D patients (25%) in this cohort (2007–2010) fulfilled the international consensus treatment goals of HbA1c <7%. Nationally, 70% of T2D and 44% of T1D patients achieved a glycemic level at or under 7.5% in 2014–2015;Citation41 in this cohort, the corresponding numbers were 75% and 46%, respectively (), thus slightly better than the reported present national average.Citation41
In Germany, a significant improvement of 33 percentage points in glycemic regulation over a 10-year time period was observed among a cohort of T2D patients, as 32% of the patients in 1997–1999 (n=333) versus 65% in 2008–2011 (n=526) had an HbA1c <7%,Citation42 thus a superior result compared to what the authors found.
Only 28% of the T2D patients achieved treatment target for blood pressure (140/90 mmHg) compared with 48% in T1D patients. In this cohort, 81% and 89% of T2D and T1D patients, respectively, were treated with ACE-inhibitors or AT2 antagonists, thus fulfilling the guidelines on anti-hypertensive treatment in which the first choice is either an ACE-inhibitor or AT2 antagonist. Of the T2D patients aged 40 years or more, 74% were treated with lipid-lowering agents; still, 44% of diabetes patients having total cholesterol values >4.5 mmol/L were not treated with statins and only 34% of the T2D patients met the treatment target for lipids. Today, increased awareness of the importance of controlling the patients’ cardiovascular risk factors may lead to more extended use of lipid-lowering agents and more intensive use of antihypertensive treatment, thereby reducing diabetes related cardiovascular morbidity and mortality.Citation43,Citation44 Even so, the Guidance studyCitation45 found scope for further improvement in diabetes care (HbA1c, blood pressure, and LDL) in eight European countries.
At present, the Vejle Diabetes Biobank has led to various publications in the field of diabetes, metabolism, and geneticsCitation16,Citation38,Citation46–Citation57 and is continuously an open resource for international and national researchers. Thus, all research groups are invited to contact the authors and present their scientific hypotheses on a collaborative basis to have access to biological materials and available clinical data.
Data access
Data on biomarkers in anonymized form can be accessed at http://dda.dk/catalogue/19269?lang=en
Declaration of consent
For the study:
“Biobank for diabetes”
The aim of the study is to establish a biobank with samples of blood and urine, stored frozen for subsequent research. Do you permit that your blood and urine samples are collected in the biobank and subsequently used for identifying biochemical and heritable markers? (Please mark with a cross)
In this study we might find out that certain persons have specific changes in the biochemical markers increasing the risk for complications to diabetes (e.g. thrombus in the heart, diabetic eye disorder, or calcification).
If assuming that we can improve the treatment of your diabetes, do you want to get information about the findings in your particular blood samples? (Please mark with a cross)
You can change your decision about this information anytime by contacting:
Laboratory, Department of Clinical Biochemistry
Vejle Hospital
Kabbeltoft 25
7100 Vejle
Tel: 7 940 6506
If you have questions to the above, please contact:
Attachment 3: Questionnaire for patients
Acknowledgments
The project was funded by the Danish Council for Independent Research/Medical Sciences, the Research Council of Vejle Hospital, the Department of Internal Medicine, Vejle Hospital, Vejle County, the Danish Research Fund, the Lions Club International Denmark, and anonymous donations.
The authors would like to thank the laboratory technologists Britta Kristensen, Lene Juul Hansen, Annette Kaaris, Jan Johannsen, Merete Willumsen, Birgitte Henriksen, Camilla Davidsen, and Sara Egsgaard for their continued engagement and dedicated work.
Supplementary material
Information for patients
We kindly ask you to participate in the study: “Biobank for diabetes”.
“Biobank for diabetes”
The prevalence of diabetes has increased during the last years, particularly the type 2 diabetes. Genetic inheritance and environmental factors play a role for the development of type 2 diabetes. The aim of this study is:
To establish a biobank with blood samples and urine samples from 6,000 patients with diabetes and 6,000 persons without diabetes (control persons). The collection of data will last for 2–3 years.
To identify biochemical and molecular markers in blood and urine samples.
To compare the results of diabetes patients and control persons.
Hopefully to find the differences in lifestyle, environmental and inheritable factors, which causes diabetes and reduces lifetime due to diabetes-related complications.
To apply the knowledge in prevention and treatment of current and future patients.
What are the procedures on the day of examination, when you choose to register in the Biobank?
You only have to meet up once. You can choose Vejle, Kolding, Fredericia, or Horsens Hospital.
The examination will take place between 7.15 and 09.30 a.m. It will take about half an hour. Height, weight, waist and hip measurement, body fat percentage, blood pressure and blood glucose will be recorded, and you will get a copy of the data.
A number of samples will be taken for storage in the Biobank (all together about 125 mL blood).
Before the day of examination you will receive a container for the urine sample, please bring the urine sample on the day of examination.
Before the examination you will also receive a questionnaire about tobacco, alcohol, exercise etc. Please bring this as well on the day of examination.
After the examination you are offered some breakfast and coffee or tea. (If you need to take any medication, it will be possible at this time).
What to remember on the day of examination when registering in the Biobank
Please fast overnight, i.e. no eating, drinking (coffee, tea, milk, alcohol, juice etc.) or smoking from 10 p.m. the day before the examination. You are allowed 1–2 glasses of water from 10.00 p.m. until the examination takes place.
Please do not take medication for blood glucose regulation (insulin or tablets). This morning please try to avoid taking medication unless absolutely necessary until the examination has finished.
Please do not run or ride a bike on the day of examination.
Please remember to bring the urine sample mentioned above.
Please remember to bring the questionnaire mentioned above.
Moreover, you should live and eat as usually the last 3 days before examination.
What are the disadvantages/risks from participating in the study?
There is no physical risk or side effects from participating. The blood sampling might cause some temporary pain and bruise at the puncture site.
What are the advantages from participation in the study?
The study is expected to generate important information about the heritable differences in the Danish population causing diabetes and reducing the life span because of insufficient effect of the medical treatment and diabetes-related complications. Therefore, the study is useful in preventing new cases of diabetes and improving treatment for future diabetes patients.
The study might be able show if you belong to a group with higher risk of diabetes-related complications and therefore might have an extended need for treatment to avoid complications and premature death.
Can you be excluded from the study?
No, only if you choose to.
The study can be stopped if the funding discontinues. In that case all biological samples and data will be destructed.
Economy
The study was funded by the Danish Council for Independent Research/Medical Sciences, the Research Council of Vejle Hospital, the Department of Internal Medicine, Vejle Hospital, Vejle County, and the Danish Research Fund. The budget is 12 million DDK.
Your participation in the study is completely voluntary. You can withdraw your consent at any time. The paper: “The rights of a trial subject in a biomedical research project” is attached. It is elaborated by the National Committee for Health Research Ethics.
If you have any questions, you are welcome to contact the doctors.
Disclosure
The authors report no conflicts of interest in this work.
References
- RicchiutiVGunterEWVaughtJBiorepositories: Worth Their Weight in Gold American Association for Clinical ChemistryWashington DC2011 [CD-ROM] Product ID: 6634
- Castillo-PelayoTBabinszkySLeBlancJWatsonPHThe importance of biobanking in cancer researchBiopreserv Biobank201513317217726035006
- PedersenCBThe Danish Civil Registration SystemScand J Public Health2011397 Suppl222521775345
- PedersenCBGotzscheHMollerJOMortensenPBThe Danish Civil Registration System. A cohort of eight million personsDan Med Bull200653444144917150149
- KristensenJKSandbaekALassenJFBroFLauritzenTUse and validation of public data files for identification of the diabetic population in a Danish countyDan Med Bull2001481333711258150
- ChristiansenJUMaruardCDNielsenHCLABKA. A real-time computer system for the clinical laboratoryScand J Clin Lab Invest Suppl198919457612772556
- KildemoesHWSorensenHTHallasJThe Danish National Prescription RegistryScand J Public Health2011397 Suppl384121775349
- WHO Collaborating Centre for Drug Statistics MethodologyNorwegian Institute of Public Health Available from: http://www.whocc.no/atc_ddd_index/Accessed August 7, 2016
- SchmidtMSchmidtSASandegaardJLEhrensteinVPedersenLSorensenHTThe Danish National Patient Registry: a review of content, data quality, and research potentialClin Epidemiol2015744949026604824
- LyngeESandegaardJLReboljMThe Danish National Patient RegisterScand J Public Health2011397 Suppl303321775347
- World Health OrganizationInternational Statistical Classification of Diseases and Related Health ProblemsGenevaWorld Health Organization 10th Revision, ICD-10: Version2016
- KeysAFidanzaFKarvonenMJKimuraNTaylorHLIndices of relative weight and obesityJ Chronic Dis19722563293434650929
- World Health OrganizationWaist Circumference and Waist–Hip Ratio: Report of a WHO Expert ConsultationGenevaWHO Library Cataloguing-in-Publication Data. 8–112008
- NielsenAAOptimization of a regional algorithm for the identification of patients with diabetes for establishing a “Biobank of patients with diabetes” and comparison with the Danish national algorithm. Estimating the number of undiagnosed patients with diabetes after introduction of HbA1c for diagnosis – translation from DanishPhD Thesis at the Faculty of Health Sciences at the University of Southern Denmark120141206
- LeveyASStevensLASchmidCHA new equation to estimate glomerular filtration rateAnn Intern Med2009150960461219414839
- NielsenAAPetersenPHGreenAChristensenCChristensenHBrandslundIChanging from glucose to HbA1c for diabetes diagnosis: predictive values of one test and importance of analytical bias and imprecisionClin Chem Lab Med20145271069107724659606
- Danish Institute for External Quality Assurance for Laboratories in Health Care, DEKS. Danish.
- FraserCGBiological Variation: From Principles to PracticeWashington, DCAACC Press2001
- WestgardJOCareyRNWoldSCriteria for judging precision and accuracy in method development and evaluationClin Chem19742078258334835236
- International EQAS – Ensuring excellent results – Labquality Available from: http://www.labquality.fi/eqa-eqas/Accessed December 23, 2015
- Quality Assurance of laboratory activities in general practices (Kvalitetssikring af laboratoriemedicinske aktiviteter i almen praksis – translated from Danish)2010 Available from: http://www.laeger.dk/nyhed/download/docs/F26051/kvalitetssikring%20og%20kvalitetsk-rav%20hovedrapport.pdfAccessed December 23, 2015
- TjonnelandAOlsenABollKStrippCChristensenJEngholmGOvervadKStudy design, exposure variables, and socioeconomic determinants of participation in Diet, Cancer and Health: a population-based prospective cohort study of 57,053 men and women in DenmarkScand J Public Health200735443244117786808
- American Diabetes AssociationGlycemic targetsDiabetes Care201538Suppl 1S33S4025537705
- InzucchiSEBergenstalRMBuseJBManagement of hyperglycaemia in type 2 diabetes: a patient-centered approach. Position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD)Diabetologia20125561577159622526604
- InzucchiSEBergenstalRMBuseJBManagement of hyperglycemia in type 2 diabetes: a patient-centered approach: position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD)Diabetes Care20123561364137922517736
- InzucchiSEBergenstalRMBuseJBManagement of hyperglycemia in type 2 diabetes, 2015: a patient-centered approach: update to a position statement of the American Diabetes Association and the European Association for the Study of DiabetesDiabetes Care201538114014925538310
- InzucchiSEBergenstalRMBuseJBManagement of hyperglycaemia in type 2 diabetes, 2015: a patient-centred approach. Update to a position statement of the American Diabetes Association and the European Association for the Study of DiabetesDiabetologia201558342944225583541
- JorgensenLGBrandslundIStahlMHyltoft PetersenPIversenSKlitgaardNde Fine OlivariusNUpper reference limit, analytical quality specifications and clinical use of haemoglobin A1CScand J Clin Lab Invest200262860962212564619
- American Diabetes AssociationCardiovascular disease and risk managementDiabetes Care201538Suppl 1S49S5725537708
- ChristensenHNielsenJSSorensenKMMelbyeMBrandslundINew national Biobank of The Danish Center for Strategic Research on Type 2 Diabetes (DD2)Clinical Epidemiol201243742
- NielsenJSThomsenRWSteffensenCChristiansenJSThe Danish Centre for Strategic Research in Type 2 Diabetes (DD2) study: implementation of a nationwide patient enrollment systemClinical Epidemiol20124Suppl 12736
- ThomsenRWFriborgSNielsenJSSchrollHJohnsenSPThe Danish Centre for Strategic Research in Type 2 Diabetes (DD2): organization of diabetes care in Denmark and supplementary data sources for data collection among DD2 study participantsClin Epidemiol20124Suppl 1151923071407
- ThomsenRWNielsenJSUlrichsenSPPedersenLHansenAMNilssonTThe Danish Centre for Strategic Research in Type 2 Diabetes (DD2) study: collection of baseline data from the first 580 patientsClin Epidemiol20124434823071401
- TolonenHKoponenPAromaaAReview of Health Examination Surveys in EuropeHelsinki, FinlandNational Public Health Institute2008
- KeidingNIndependent Delayed EntryColumbus, Ohio, USAKluwer Academic Publisher1992
- JorgensenLGPetersenPHChristensenCEriksenEWBrandslundIImprovement in glycemic control over 11 years in patients monitored for diabetes in one countyClin Chem Lab Med2006441929816375593
- CharlsonMEPompeiPAlesKLMacKenzieCRA new method of classifying prognostic comorbidity in longitudinal studies: development and validationJ Chronic Dis19874053733833558716
- NielsenAAChristensenHLundEDChristensenCBrandslundIGreenADiabetes mortality differs between registers due to various disease definitionsDan Med J2014615A484024814742
- AliMKBullardKMSaaddineJBCowieCCImperatoreGGreggEWAchievement of goals in U.S. diabetes care, 1999–2010N Engl J Med2013368171613162423614587
- SaaddineJBCadwellBGreggEWEngelgauMMVinicorFImperatoreGNarayanKMImprovements in diabetes processes of care and intermediate outcomes: United States, 1988–2002Ann Intern Med2006144746547416585660
- Danish Diabetes Database – Annual report 2014/2015 Available from: https://www.sundhed.dk/content/cms/87/4687_kom_%C3%A5rsrapport_diabetes_2014_15_27082015_endelig.pdfAccessed March 21, 2016
- DuYHeidemannCSchaffrath RosarioAChanges in diabetes care indicators: findings from German National Health Interview and Examination Surveys 1997–1999 and 2008–2011BMJ Open Diabetes Res Care201531e000135
- GaedePLund-AndersenHParvingHHPedersenOEffect of a multifactorial intervention on mortality in type 2 diabetesN Engl J Med2008358658059118256393
- GaedePVedelPLarsenNJensenGVParvingHHPedersenOMultifactorial intervention and cardiovascular disease in patients with type 2 diabetesN Engl J Med2003348538339312556541
- StoneMACharpentierGDoggenKQuality of care of people with type 2 diabetes in eight European countries: findings from the Guideline Adherence to Enhance Care (GUIDANCE) studyDiabetes Care20133692628263823628621
- AhluwaliaTSAllinKHSandholtCHDiscovery of coding genetic variants influencing diabetes-related serum biomarkers and their impact on risk of type 2 diabetesJ Clin Endocrinol Metab20151004E664E67125599387
- FumagalliMMoltkeIGrarupNGreenlandic Inuit show genetic signatures of diet and climate adaptationScience201534962541343134726383953
- HansenTHVestergaardHJorgensenTImpact of PTBP1 rs11085226 on glucose-stimulated insulin release in adult DanesBMC Med Genet2015161725927630
- HarderMNAppelEVGrarupNThe type 2 diabetes risk allele of TMEM154-rs6813195 associates with decreased beta cell function in a study of 6,486 DanesPloS one2015103e012089025799151
- ImamuraMTakahashiAYamauchiTGenome-wide association studies in the Japanese population identify seven novel loci for type 2 diabetesNat Commun201671053126818947
- MahajanASimXNgHJIdentification and functional characterization of G6PC2 coding variants influencing glycemic traits define an effector transcript at the G6PC2-ABCB11 locusPLoS Genet2015111e100487625625282
- StoyJKampmannUMengelAReduced CD300LG mRNA tissue expression, increased intramyocellular lipid content and impaired glucose metabolism in healthy male carriers of Arg82Cys in CD300LG: a novel genometabolic cross-link between CD300LG and common metabolic phenotypesBMJ Open Diabetes Res Care201531e000095
- AlbrechtsenAGrarupNLiYExome sequencing-driven discovery of coding polymorphisms associated with common metabolic phenotypesDiabetologia201356229831023160641
- FlannickJThorleifssonGBeerNLLoss-of-function mutations in SLC30A8 protect against type 2 diabetesNat Genet201446435736324584071
- Le ChatelierENielsenTQinJRichness of human gut microbiome correlates with metabolic markersNature2013500746454154623985870
- SnogdalLSGrarupNBanasikKStudies of association of AGPAT6 variants with type 2 diabetes and related metabolic phenotypes in 12,068 DanesBMC Med Genet20131411324156295
- SteinthorsdottirVThorleifssonGSulemPIdentification of low-frequency and rare sequence variants associated with elevated or reduced risk of type 2 diabetesNature Genet201446329429824464100