
Abstract
Background
Statins have been linked to new-onset osteoporotic fractures (NOFs), and different statins may alter the risk for the development of NOFs.
Aim
In this study, we investigated the association between different statins and the development of NOFs.
Patients and methods
This was a longitudinal cohort study performed using data from claim forms submitted to the Taiwan Bureau of National Health Insurance, including case patients with NOFs from January 2004 to December 2013 and non-NOF subjects. We estimated the hazard ratios (HRs) of NOFs associated with statin use. Nonuser subjects served as the reference group.
Results
A total of 44,405 patients with NOFs were identified from among 170,533 patients with hyperlipidemia during the study period. The risk of developing NOFs after adjusting for age, sex, comorbidities, and concurrent medication use was lower among users of atorvastatin (HR, 0.77; 95% CI, 0.71–0.84) and rosuvastatin (HR, 0.72; 95% CI, 0.64–0.81) than among simvastatin users. Lovastatin, pravastatin, fluvastatin, and pitavastatin were not associated with the risk of developing NOFs compared with simvastatin users.
Conclusion
This study supports previous reports regarding a beneficial effect of statin use and NOF risk, but not all statins. Patients taking atorvastatin or rosuvastatin were at lower risk of developing NOFs compared with simvastatin users during the 10-year follow-up. Other statins such as pravastatin, fluvastatin, lovastatin, and pitavastatin were not associated with NOFs. This study also highlighted that high-potency statin has a dose–response effect on lower NOF risk.
Background
The incidence of osteoporotic fractures is increasing worldwide, especially in developed and developing countries.Citation1,Citation2 An estimated 9 million osteoporotic fractures were reported worldwide in 2000, and fractures of the hip and spine were found to be associated with an increased mortality rate of 10%–20%.Citation3 Furthermore, recent reports estimate that the expected burden of osteoporotic fractures will increase by 20% by 2020 only in postmenopausal women.Citation4,Citation5 Concerns regarding the health care of osteoporotic fractures, particularly in terms of new-onset osteoporotic fractures (NOFs), have gradually increased worldwide.Citation6,Citation7 Moreover, osteoporotic fractures may result in significant health care costsCitation8 because they have been shown to adversely affect the health-related quality of life, including limitation of ambulation, depression, loss of independence, and chronic pain and have become a major public health burden.Citation9
Statins are effective agents to control hyperlipidemia and are widely used in the prevention of cardiovascular diseases.Citation10,Citation11 In particular, statins may influence bone metabolism by increasing bone formation.Citation12 Recently, several randomized trials have led to a debate on whether the use of statins is associated with a lower risk of developing NOFs in hyperlipidemic patients undergoing treatment.Citation13–Citation18 However, the results of these studies are inconsistent, partly because of the inability to completely adjust for risk factors in baseline characteristics between statin users and nonusers or the short follow-up periods.Citation19,Citation20 It is also unclear whether different statins are associated with a lower risk of developing NOFs when compared with other statins in patients with hyperlipidemia during long-term follow-up. Therefore, the objective of this retrospective cohort study was to investigate the effect of different statins (simvastatin, pravastatin, lovastatin, fluvastatin, atorvastatin, rosuvastatin, and pitavastatin) on the risk of developing NOFs among hyperlipidemic patients in Taiwan.
Patients and methods
Study population
Data were collected from claim forms of the Taiwan National Health Insurance (NHI) that had been submitted to the Taiwan Bureau of National Health Insurance from 2002 to 2013. The Taiwan NHI program has been operating since 1995 and represents ~99% of Taiwan’s population. The claim forms contain inpatient and outpatient records. The information from the claim forms is stored in two tables, a visit table and a prescription table. Visit tables contain patient identification numbers, sex, age, three diagnostic codes, medical expenditures, and hospital and physician information. Prescription tables contain the quantity and expenditure of all drugs, surgeries, and treatments. Patients were included in the study if they had been diagnosed with hyperlipidemia and were statin users without osteoporotic fractures at baseline (January 1, 2004). Statin users were those patients who received at least a 180-day statin prescription during the period between January 1, 2004, and December 31, 2004. Nonusers were those patients who did not receive a statin prescription throughout the whole study period. We summarized the claim records of each patient into one record.
Study design
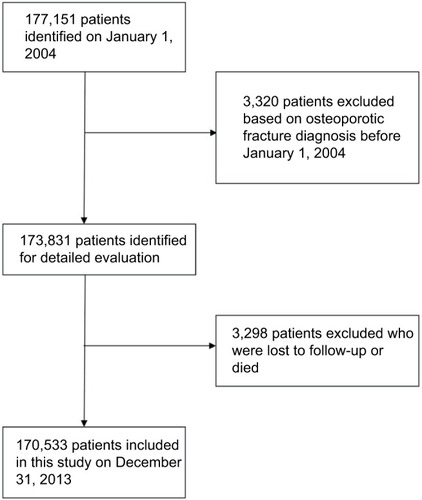
Participants were included in the study if they had been diagnosed with hyperlipidemia (International Classification of Diseases, Ninth Revision, Clinical Modification [ICD-9-CM] code 272) between January 1, 2004, and June 30, 2004. At least one of the following enrollment criteria had to be met for inclusion in the study: 1) two or more outpatient visits within a 6-month period, 2) all prescriptions of statins continuously administered to the patients for >6 months within a 10-year follow-up period, or 3) one or more inpatient admissions with a diagnosis of hyperlipidemia. The primary endpoint was the development of NOFs, which was defined by the time an osteoporotic fracture (ICD-9-CM codes 733.11 and 805–829) or a fracture-related surgery (ICD-9-CM codes 78.1, 78.4, 78.5, 78.9, 79, and 81) first appeared in the inpatient or outpatient claim records. Comorbidities related to osteoporotic fractures were defined according to the ICD-9-CM code and included coronary artery disease (ICD-9-CM code 410–415), hypertension (ICD-9-CM code 401–405), diabetes mellitus (ICD-9-CM code 250), alcohol-related disorders (ICD-9-CM codes 291, 303, 305, 571.0, 571.1, 571.2, 571.3, 790.3, and V11.3), chronic obstructive pulmonary disease (COPD) (ICD-9-CM codes 490–492 and 496), hyperthyroidism (ICD-9-CM code 242), liver cirrhosis (ICD-9-CM codes 571.5 and 571.6), stroke (ICD-9-CM code 430–438), and chronic kidney disease (ICD-9-CM code 585). Statins are available only by prescription in Taiwan. Patients using only one type of statins before the development of NOFs were categorized as single users based on the type of statin prescribed, including simvastatin, pravastatin, lovastatin, fluvastatin, atorvastatin, rosuvastatin, and pitavastatin. Patients who fulfilled any of the following criteria were excluded from the study: 1) had a prior history of an osteoporotic fracture or a fracture-related surgery before January 1, 2004, 2) patients taking calcium supplements, biphosphates, selective serotonin-specific reuptake inhibitors, serotonin–norepinephrine reuptake inhibitors, tricyclic antidepressants, estrogen, or calcitonin, and 3) patients suffering from other major medical problems, leaving those with a life expectancy of <6 months. Individuals in our nonuser statin group did not receive statin during the entire study period but were administered diet control, niacin, or fibrates for the treatment of hyperlipidemia. Initially, 177,151 outpatients fulfilled the inclusion criteria; however, 3,320 patients were excluded based on the diagnosis of an osteoporotic fracture before January 1, 2004. Therefore, a total of 173,831 patients were enrolled in the study at baseline (). Furthermore, 2,045 patients who were lost to follow-up and 1,253 patients who died without the diagnosis of NOFs or NOF-related deaths were excluded. Finally, a total of 170,533 outpatients were included in this study. This study was approved by the ethics committee of Chung Shan Medical University Hospital (CS2-16086). Due to all patients’ records/information being de-identified, a patient consent to review their medical claim records was not required by the ethics committee of Chung Shan Medical University Hospital (CS2-15104).
Figure 1 Flowchart of selection of patients for the inclusion in this study.
Statins are used to reduce the risk of cardiovascular events and are classified as high, moderate, or low intensity depending on the potency with which they reduce low-density lipoprotein cholesterol (LDL-cholesterol).Citation21 High potency statin treatment was defined as at least 10 mg rosuvastatin and at least 20 mg atorvastatin; all other statin treatments were defined as having low to moderate potency. The toxic doses of statins were defined as >40 mg rosuvastatin, >80 mg atorvastatin, >80mg lovastatin, >80 mg fluvastatin, >80 mg pravastatin, >4 mg pitavastatin, and >40 mg simvastatin. Currently, in Taiwan, seven kinds of statins (high-potency atorvastatin and rosuvastatin and low- to moderate-potency fluvastatin, pravastatin, pitavastatin, and simvastatin) are used; however, the standard statin dose in Taiwan is lower than that in the American College of Cardiology/American Heart Association guidelines.Citation21
Statistical analysis
The basic information of the study cohort includes mean and standard deviation (SD) for age and duration of statin prescription, presented as number and percentage for sex, along with baseline comorbidity and medication. Student’s t-test and chi-square tests were used to evaluate whether there was a significant difference between statin-treated and statin nonusers. The NOF-free survival rates of the two groups were estimated by the Kaplan–Meier method using the log-rank test. This study aimed to examine the association between the use of certain types of statins and the risk of developing NOFs. The Cox proportional hazard regression model was used to compare the risk of NOF development between statin users and nonusers. The Cox proportional hazard regression model was also used to compare the risk of NOF development between different statins using simvastatin as reference group. Adjusted hazard ratios (HRs) and 95% confidence intervals (CIs) were calculated, adjusting for important risk factors for the development of osteoporotic fractures, including age, sex, comorbidities, and concurrent medication use. P-values <0.05 were considered to be statistically significant. All statistical calculations were performed using statistical analysis software, version 9.3 (SAS Institute Inc., Cary, NC, USA).
Results
Baseline characteristics of all patients
Baseline characteristics, comorbidities, and concurrent medication use among the overall study population are presented in . Among 170,533 eligible patients with defined hyperlipidemia, 44,405 (26.0%) developed NOFs from January 2004 to December 2013. There were more men than women in this study population. The mean age of patients with statin user group was 67.0 years and that of nonuser group was 66.4 years, which was statistically significantly different (p<0.0001).
Table 1 Baseline characteristics of all patients between statin users and nonusers
Patients in the statin user group had more comorbidities, including alcohol-related disorders, COPD, chronic kidney disease, diabetes mellitus, hypertension, hyperthyroidism, liver cirrhosis, coronary artery disease, and stroke. There was a higher percentage of hormone replacement therapy, fibrates, and niacin users in the nonuser group than that in the statin user group. Regarding the duration of use of the statin subtype in this study, lovastatin was used for the longest duration and pitavastatin was used for the shortest duration.
Relative risk of NOF
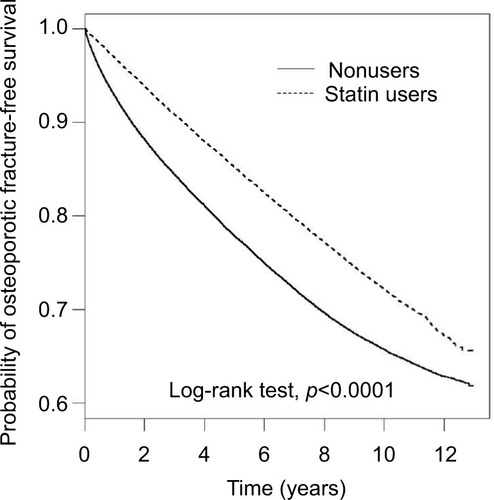
Results of the Kaplan–Meier survival analysis are shown in , which indicate that the risk of developing NOFs was significantly lower among statin users than that among the nonuser cohort (log-rank test; p<0.001).
Figure 2 Kaplan–Meier analysis comparing probabilities of osteoporotic fracture between statin users and nonusers.
The analyses by defined daily doses (DDDs) indicated a tendency of decreasing risk for NOFs with increasing DDDs. The high DDDs (91–365 and ≥366) of statins showed a significantly lower risk for NOF development (crude HR, 0.37; 95% CI, 0.36–0.39; adjusted HR, 0.32; 95% CI, 0.31–0.34). Conversely, the low DDDs (<28) of statins revealed a significant association with the risk for NOF development (crude HR, 1.24; 95% CI, 1.18–1.30; adjusted HR, 1.07; 95% CI, 1.02–1.13).
The crude HR of developing NOFs was lower among nonusers (HR, 0.85; 95% CI, 0.80–0.91, ) compared with simvastatin users. However, after adjusting for age, sex, comorbidities, and concurrent medication use, the risk for NOF development was not associated with the nonusers (HR, 0.99; 95% CI, 0.93–1.06, ). Patients who took atorvastatin (crude HR, 0.76; 95% CI, 0.70–0.83; adjusted HR, 0.77; 95% CI, 0.71–0.84) and rosuvastatin (crude HR, 0.70; 95% CI, 0.62–0.79; adjusted HR, 0.72; 95% CI, 0.64–0.81) were at lower risk of developing NOFs compared to that of simvastatin users. Lovastatin, pravastatin, fluvastatin, and pitavastatin were not associated with the risk of developing NOFs compared with simvastatin users (p>0.05, ). Finally, lipophilic and hydrophilic statins showed similar effects in patients with hyperlipidemia in terms of the risk of developing NOFs.
Table 2 Crude and adjusted HRs of statins for new-onset osteoporotic fracture
Discussion
This study indicated that the risk of developing NOFs was significantly lower among statin users than among nonusers, suggesting that using a statin continuously may have a potential impact of preventing the development of NOFs. This study also demonstrated that the use of atorvastatin and rosuvastatin was independently associated with a decreased risk of NOF development compared with simvastatin users in hyperlipidemic patients. Lovastatin, pravastatin, fluvastatin, and pitavastatin were not associated with the risk of NOF development compared to that of simvastatin users in patients with hyperlipidemia. Finally, the study also showed that statin has a dose–response effect on lower NOF risk.
In the current study, patients using high DDDs (91–365 or ≥366) of statin use were found to have a significantly protective effect against NOFs, whereas low DDDs of statin use were significantly associated with a higher risk of developing NOFs. It demonstrated that statin has a dose–response effect on lower NOF risk. To our knowledge, this is the first study to directly compare the incidence of osteoporotic fractures in patients treated with different statins. All the previous NOF studies were placebo-controlled or head-to-head comparison trials and had a short duration (2–5 years).Citation13–Citation18 These observational studies did not use a DDD for continuous prescription of statins. However, we are not certain whether our finding is consistent with those of observational studies. Additional studies using a DDD for continuous prescription of statins are required in the future.
In this study, pravastatin was not significantly associated with a decrease in the risk of NOF development compared with simvastatin users. This result is consistent with the results reported by Reid et al, who showed that the relative risk for NOF development in individuals taking pravastatin compared with those not taking statin was 0.94 (95% CI, 0.77–1.16).Citation22 Similarly, Hippisley-Cox and Coupland also reported that pravastatin was not associated with a decreased risk of developing NOF (adjusted HR, 0.91; 95% CI, 0.75–1.11 in men; adjusted HR, 1.00; 95% CI, 0.73–1.36 in women) in hyperlipidemic patients.Citation23 A potential explanation exists for ours and these two studies that the use of pravastatin may have little effect on bone in vivo.Citation4
Lovastatin has been shown to accelerate ossification-related gene expressions in fracture healing in osteoporotic rats that were continuously administered lovastatin for >4 weeks.Citation24 Our results contradicted this study, which may be because of not using a combination of tocotrienol or the use of lovastatin may have little effect on bone in vivo.Citation25,Citation26
The use of statins has been demonstrated to have a significant positive effect on osteoporotic fractures as reported by several observational studies.Citation13–Citation17 However, in our study comprising a 10-year follow-up period, no relationship was observed between the risk of developing NOF and the use of lovastatin, pravastatin, fluvastatin, and pitavastatin compared with that among simvastatin users. A similar finding has also been reported by several observational studies.Citation4,Citation19,Citation27,Citation28 For instance, Ward et al analyzed 46,249 patients in a Military Healthcare System and reported that there was no significant association between the risk of developing NOF and statin use.Citation4
In vitro data show that statins have a catabolic effect on bones.Citation12,Citation24,Citation29–Citation31 Therefore, atorvastatin is generally considered to decrease the risk of developing NOFs.Citation4,Citation32 However, one study has indicated that atorvastatin is not associated with a decreased risk of developing NOFs compared with simvastatin.Citation23 Our results showed a beneficial effect on the risk of developing NOFs, and this study is the first long-term longitudinal epidemiological investigation of the association between the use of atorvastatin and the risk of developing osteoporotic fractures with a follow-up period of 10 years.
In this study, rosuvastatin was associated with a decrease in the risk of NOF development compared with simvastatin users. This result is in contrast with the results reported by Hippisley-Cox and Coupland, who showed a nonstatistically significant decrease in the risk of developing NOFs (adjusted HR, 0.89; 95% CI, 0.65–1.21 in men; adjusted HR, 0.61; 95% CI, 0.36–1.03 in women).Citation22 Our present study is also the first long-term longitudinal epidemiological investigation of the association between the use of rosuvastatin and the risk of developing osteoporotic fractures with a follow-up period of 10 years.
Some observational studies have recommended that lipophilic statins (lovastatin, simvastatin, and atorvastatin) were independently associated with a decreased risk of NOF development in patients with hyperlipidemia, whereas hydrophilic statins (pravastatin, fluvastatin, and rosuvastatin) were not.Citation16,Citation27,Citation33 However, in our study that included a 10-year follow-up period, the association with NOF risk reduction was similar between lipophilic and hydrophilic statins. Similarly, our result is consistent with that reported by Ward et al, who enrolled 6,967 pairs of statin users and nonusers with hyperlipidemia and did show a reduction in the risk of developing femoral neck fractures in statin users compared to that in statin nonusers.Citation4 In particular, a risk reduction among the users of high-potency statins (atorvastatin and rosuvastatin) and dose–response effect on NOF risk were observed in our study. The reason for these findings in our study is unclear, but it may be attributable to the statin dose (high vs low) and duration (10 vs 2–5 years).Citation13,Citation15,Citation16,Citation27 These findings emphasize the need for further investigation of the mechanistic links between these high-potency statins and the risk of developing NOFs.
Some limitations of this study need to be emphasized. First, this was a descriptive retrospective study conducted in Taiwan over a period of 10 years. Moreover, we excluded irregularly treated hyperlipidemic patients from the analyses. Therefore, caution must be exercised in interpreting our data. Second, all cases in this study were collected from claimed data sets of the Taiwan NHI that the diagnoses were based on physician reports only; therefore, it is unclear how our findings can be generalized to patients in different areas of the world. Third, the process of osteoporosis in patients who developed NOF in this study would have started many years before the diagnoses, and NOF may have coexisted with the process of hyperlipidemia for which statins were used. Thus, the cause-and-effect relationships between NOF and statins cannot be determined in this study.
Conclusion
In conclusion, our results show that hyperlipidemic patients who use atovastatins and rosuvastatins were independently associated with a decreased risk of NOF compared with simvastatin users. Other statins such as lovastatin, pravastatin, fluvastatin, and pitavastatin were not associated with NOFs. Our findings may provide some support for the hypothesis that there are differences in the risk of developing NOF with the use of different types of statins in hyperlipidemic patients. It also highlighted the lower risk of NOF associated with more commonly prescribed high-potency statins. These findings emphasize the need for further investigation of the mechanistic links between these high potency statins and NOFs.
Disclosure
The authors report no conflicts of interest in this work.
References
- CenterJRNguyenTVSchneiderDSambrookPNEismanJAMortality after all major types of osteoporotic fracture in men and women: an observational studyLancet1999353915687888210093980
- HolroydCCooperCDennisonEEpidemiology of osteoporosisBest Pract Res Clin Endocrinol Metab200822667168519028351
- IoannidisGPapaioannouAHopmanWMRelation between fractures and mortality: results from the Canadian Multicentre Osteoporosis StudyCMAJ2009181526527119654194
- WardIMMortensenEMBattafaranoDFFreiCRMansiIAssociation of statins and risk of fractures in a military health system: a propensity score-matched analysisAnn Pharmacother201448111406141425070396
- CawstonHMaravicMFardellonePEpidemiological burden of postmenopausal osteoporosis in France from 2010 to 2020: estimations from a disease modelArch Osteoporos201271–223724623060309
- JohnellOKanisJAAn estimate of the worldwide prevalence and disability associated with osteoporotic fracturesOsteoporos Int200617121726173316983459
- HsiaoPCChenTJLiCYRisk factors and incidence of repeat osteoporotic fractures among the elderly in Taiwan: a population-based cohort studyMedicine201594e53225700317
- GauthierAKanisJAJiangYEpidemiological burden of postmenopausal osteoporosis in the UK from 2010 to 2021: estimations from a disease modelArch Osteoporos201161–217918822886104
- AdachiJDAdamiSGehlbachSGLOW InvestigatorsImpact of prevalent fractures on quality of life: baseline results from the global longitudinal study of osteoporosis in womenMayo Clin Proc201085980681320634496
- NaciHBrugtsJAdesTComparative tolerability and harms of individual statins: a study-level network meta-analysis of 246 955 participants from 135 randomized, controlled trialsCirc Cardiovasc Qual Outcomes20136439039923838105
- TaylorFHuffmanMDMacedoAFStatins for the primary prevention of cardiovascular diseaseCochrane Database Syst Rev20131CD004816
- MundyGGarrettRHarrisSStimulation of bone formation in vitro and in rodents by statinsScience199928654461946194910583956
- ChanKAAndradeSEBolesMInhibitors of hydroxymethylglutaryl-coenzyme A reductase and risk of fracture among older womenLancet200035592222185218810881890
- RayWADaughertyJRGriffinMRLipid-lowering agents and the risk of hip fracture in a Medicaid populationInj Prev20028427627912460961
- ScrantonREYoungMLawlerESolomonDGagnonDGazianoJMStatin use and fracture risk: study of a US veterans populationArch Intern Med2005165172007201216186471
- RejnmarkLVestergaardPMosekildeLStatin but not nonstatin lipid-lowering drugs decrease fracture risk: a nationwide case-control studyCalcif Tissue Int2006791273616868664
- Helin-SalmivaaraAKorhonenMJLehenkariPStatins and hip fracture prevention: a population based cohort study in womenPLoS One2012710e4809523144731
- McCandlessLawrenceCStatin use and fracture risk: can we quantify the healthy-user effect?Epidemiology201324574375223883870
- van StaaTPWegmanSde VriesFLeufkensBCooperCUse of statins and risk of fracturesJAMA2001285141850185511308398
- LaCroixAZCauleyJAPettingerMStatin use, clinical fracture, and bone density in postmenopausal women: results from the Women’s Health Initiative Observational StudyAnn Intern Med200313929710412859159
- StoneNJRobinsonJGLichtensteinAH2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice GuidelinesJ Am Coll Cardiol201463252889293424239923
- ReidIRHagueWEmbersonJEffect of pravastatin on frequency of fracture in the LIPID study: secondary analysis of a randomised controlled trial. Long-term Intervention with Pravastatin in Ischaemic DiseaseLancet2001357925550951211229669
- Hippisley-CoxJCouplandCUnintended effects of statins in men and women in England and Wales: population based cohort study using the QResearch databaseBMJ2010340c219720488911
- N’IbrahimMohamedNSoelaimanINShuidANThe effects of targeted deliveries of lovastatin and tocotrienol on ossification-related gene expressions in fracture healing in an osteoporosis rat modelInt J Environ Res Public Health20151210129581297626501302
- N’IbrahimKhamisMFMod YunohMFAbdullahSMohamedNShuidANTargeted delivery of lovastatin and tocotrienol to fracture site promotes fracture healing in osteoporosis model: micro-computed tomography and biomechanical evaluationPLoS One2014912e11559525526611
- KlontzasMEKenanidisEIMacFarlaneRJInvestigational drugs for fracture healing: preclinical & clinical dataExpert Opin Investig Drugs2016255585596
- RejnmarkLOlsenMLJohnsenSPVestergaardPSorensenHTMosekildeLHip fracture risk in statin users: a population-based Danish case-control studyOsteoporos Int200415645245815205716
- Heart Protection Study Collaborative GroupMRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: a randomised placebo-controlled trialLancet2002360932672212114036
- TanJFuXSunCGA single CT-guided percutaneous intraosseous injection of thermosensitive simvastatin/poloxamer 407 hydrogel enhances vertebral bone formation in ovariectomized minipigsOsteoporos Int201627275776726223190
- KajiHKanataniMSugimotoTChiharaKStatins modulate the levels of osteoprotegerin/receptor activator of NFkappaB ligand mRNA in mouse bone-cell culturesHorm Metab Res2005371058959216278780
- IssaJPIngraci de LuciaCDos Santos KotakeBGThe effect of simvastatin treatment on bone repair of femoral fracture in animal modelGrowth Factors201533213914825798995
- BauerDCMundyGRJamalSAUse of statins and fracture: results of 4 prospective studies and cumulative meta-analysis of observational studies and controlled trialsArch Intern Med2004164214615214744837
- LuisettoGCamozziVStatins, fracture risk, and bone remodelingJ Endocrinol Invest2009324 Suppl323719724164