
Abstract
Objective
The aim was to investigate whether coffee or caffeine consumption is associated with reproductive endpoints among women with natural fertility (ie, time to pregnancy [TTP] and spontaneous abortion [SAB]) and among women in fertility treatment (ie, clinical pregnancy rate or live birth rate).
Design
This study was a systematic review and dose–response meta-analysis including data from case–control and cohort studies.
Methods
An extensive literature search was conducted in MEDLINE and Embase, with no time and language restrictions. Also, reference lists were searched manually. Two independent reviewers assessed the manuscript quality using the Newcastle–Ottawa Scale (NOS). A two-stage dose–response meta-analysis was applied to assess a potential association between coffee/caffeine consumption and the outcomes: TTP, SAB, clinical pregnancy, and live birth. Heterogeneity between studies was assessed using Cochrane Q-test and I2 statistics. Publication bias was assessed using Egger’s regression test.
Results
The pooled results showed that coffee/caffeine consumption is associated with a significantly increased risk of SAB for 300 mg caffeine/day (relative risk [RR]: 1.37, 95% confidence interval [95% CI]: 1.19; 1.57) and for 600 mg caffeine/day (RR: 2.32, 95% CI: 1.62; 3.31). No association was found between coffee/caffeine consumption and outcomes of fertility treatment (based on two studies). No clear association was found between exposure to coffee/caffeine and natural fertility as measured by fecundability odds ratio (based on three studies) or waiting TTP (based on two studies).
Conclusion
Results from this meta-analysis support the growing evidence of an association between coffee/caffeine intake and the risk of SAB. However, viewing the reproductive capacity in a broader perspective, there seems to be little, if any, association between coffee/caffeine consumption and fecundity. In general, results from this study are supportive of a precautionary principle advised by health organizations such as European Food Safety Authority (EFSA) and World Health Organization (WHO), although the advised limit of a maximum of two to three cups of coffee/200–300 mg caffeine per day may be too high.
Plain language summary
Coffee and other caffeinated beverages are widely consumed by women desiring to conceive as well as pregnant women. Whether such consumption reduces the chance of achieving a pregnancy or may have harmful effects on the developing fetus is widely debated. As a contribution to this debate and given the growing concern of subfecundity and infertility in public health, we investigated the risk of coffee or caffeine consumption on the ability to conceive a pregnancy and to carry the pregnancy to term. Results from this study showed an increased risk of experiencing a spontaneous abortion with increasing consumption of coffee/caffeine during early pregnancy. No clear association was found between coffee/caffeine consumption and the chance of achieving a pregnancy among women/couples trying to conceive naturally or by women/couples receiving fertility treatment. Results from this study support the precautionary principle advised by health organizations such as European Food Safety Authority (EFSA) and World Health Organization (WHO), although the advised limit of a maximum of two to three cups of coffee/200–300 mg caffeine per day may be too high.
Introduction
Subfecundity and infertility are multifactorial conditions of growing concern in public health. Worldwide, one in six couples experience fecundity problems during their reproductive lifetime.Citation1–Citation3 While the cause often may be explained by failure of ovulation, damages on the fallopian tubes, or low sperm count, the reduced fecundity is still unexplained in many cases. Thus, investigations of a potential effect of modifiable exposures on longer waiting time to pregnancy (TTP), increased rate of spontaneous abortion (SAB), or reduced live birth rate are important.
Coffee consumption is common among people throughout the world. Worldwide, Finland has the highest consumption (12.0 kg coffee/person/year), with Denmark being the fourth most coffee-consuming country (8.7 kg coffee/person/year). Also, coffee and other caffeine-containing drinks and foods are widely consumed by women desiring to conceive and by pregnant women. On average, a cup of coffee contains ~100 mg of caffeine.Citation4
Even small effects of coffee or caffeine intake on fecundity could have considerable public health consequences, considering the large consumption of these substances.
The European Food Safety Authority (EFSA) recommends women desiring to conceive and pregnant women to keep their daily caffeine consumption below 200 mg,Citation5 while WHO recommends a daily caffeine intake below 300 mg.Citation6 Caffeine is a central ingredient in coffee, while other sources of caffeine include tea, soft drinks, chocolate, and some medications.
The association between caffeine intake and female fecundity has been studied with inconsistent findings, in studies with both retrospectivelyCitation7–Citation13 and prospectively collected exposure data.Citation14–Citation19 A high level of coffee consumption during pregnancy has been associated with an increased risk of fetal death after 20 weeks of gestationCitation20,Citation21 and stillbirth.Citation22 In meta-analyses, an increased risk of low birth weight and small for gestational age was found,Citation23 but no association was found between caffeine intake during pregnancy and the risk of preterm birth.Citation23,Citation24
Recently, a meta-analysis reported that an increment in intake of 100 mg caffeine per day was associated with a 14% increased risk of SAB.Citation23 However, the authors did not account for the varying quality of the included studies, including varying (or none) adjustment for potential confounders. Studies that fail to adjust for important risk factors associated with SAB may over- or underestimate the risk associated with caffeine consumption. Hence, taking adjustment status into account would considerably improve the quality of a meta-analysis. Moreover, other substances in coffee besides caffeine might play an important role. Finally, applying a broader view on fecundity through inclusion of different reproductive endpoints among both women conceiving naturally and following fertility treatment could extend the use of the results and help general practitioners and fertility clinics provide balanced information to women and couples seeking advice or even fertility treatment. No meta-analysis has previously reported on a possible association between coffee/caffeine intake and TTP or endpoints among couples in fertility treatment.
The aim of this systematic review and dose-response meta-analysis was to investigate whether consumption of coffee or caffeine is associated with reproductive endpoints among women with natural fertility (ie TTP and SAB) and among women in fertility treatment (ie clinical pregnancy rate and live birth rate).
Methods
A review protocol is available from the PROSPERO database.Citation25 The protocol was registered on June 9, 2015 (registration number: CRD42015020333).
Search strategy and selection
We conducted a comprehensive literature search in MED-LINE and Embase databases with the help of a medical librarian on May 26, 2015. The following keywords and medical subject headings were used to identify relevant articles in the databases: ([“Fertility” or “Infertility, Female” or “Reproduction” or “Preconception Care”) or [“Reproductive Techniques, Assisted” or “Reproductive Techniques” or “fertility treatment”]) AND (“Caffeine/adverse effects” or “Coffee”) AND (“Case-Control Studies” or “Cohort Studies”). To include non-indexed new literature, an additional search was performed using free text terms. No restrictions were made regarding study language or year of publication. Further, the reference lists of retrieved articles and reviews were searched manually for additionally relevant studies. The first author reviewed all retrieved articles for eligibility by title and abstract by consulting with at least one co-author in cases of any doubt about the inclusion of a given study or not. Potentially eligible articles were thoroughly read in full text to check whether they fulfilled the following inclusion criteria:
Participants had to be either women/couples trying to conceive naturally or women/couples trying to conceive by medically assisted reproduction (MAR) treatment
Studies that reported a numerical exposure range of either coffee or caffeine consumption
Studies that investigated at least one of the outcomes of interest: TTP, SAB, clinical pregnancy, and live birth
Articles that reported data from original studies (ie, no review articles)
Studies of which the design was a case-control study or a cohort study (ie, no RCT)
Data extraction
All included full text articles were read independently by at least two authors. A data extraction form was developed a priori, ensuring a standardized procedure. The following data were extracted: lead author surname, study title, country of origin, year of publication and journal, study design, study population (size and selection), exposure and outcome assessment, covariates adjusted for, main results, study limitations, and assessment of quality scoring.
We assessed the quality of all included studies using the Newcastle–Ottawa Scale (NOS).Citation26 Thus, the selection process and comparability of the study groups as well as the ascertainment of exposure or outcome of interest of the included studies were evaluated for either cohort or case–control studies (please see scoring details in the Supplementary material). In addition to the NOS scheme, we constructed an explanatory form ensuring a standardized scoring among the authors with regard to the specific scope of this review (Supplementary material). When using NOS to evaluate study comparability, one has to choose the two most important covariates. Hence, based on the current knowledge, maternal age was chosen as the most important factor to adjust for. As additionally important adjustment factors, smoking was chosen for studies evaluating TTP and MAR treatment, while maternal alcohol consumption was chosen for those investigating SAB. All studies were allocated a total score between 0 and 9 independently by a minimum of two authors. Any inconsistency was resolved by discussion, leading to a uniform decision. Studies with a total score of ≥7 were considered as “ high-quality studies”, and in a sub-analysis, studies were stratified according to this selected cut-off value. Regardless of total NOS score, all studies were included in the review.
This review is reported in accordance with the PRISMA statementCitation27 for reporting of systematic review and meta-analysis. Supplementary material regarding the full search strategy for MEDLINE, elaborated reasons for exclusion, and NOS explanatory form are all available online.
Outcomes
The ability to naturally conceive was investigated by two broad fecundability measures including TTP (ie, the number of months or cycles taken by a couple to conceive, when being sexually active and not using birth control) and fecund-ability odds ratio (FOR) (ie, the ratio of couple’s probability of conceiving in one menstrual cycle).Citation28 The capability of maintaining a pregnancy after conception was evaluated by the risk of experiencing an SAB (yes/no). Among couples receiving MAR treatment, a possible association was investigated using different endpoints to evaluate a successful fertility treatment (ie, achieving a pregnancy or live birth after fertility treatment; yes/no).
Statistical analysis
Although still included in the review, studies were excluded from the meta-analyses if they did not provide information on the number of cases and total number of subjects within each exposure category and whose corresponding author did not respond to emails asking for additional data to calculate these numbers.Citation7,Citation9,Citation10,Citation14,Citation15,Citation17,Citation29–Citation33 Also, we excluded studies that did not report on three or more quantitative categories of coffee/caffeine consumption,Citation34–Citation37 as these cannot contribute sufficient data when performing a dose–response meta-analysis.Citation38
We applied a two-stage dose–response meta-analysis to assess a potential association between coffee/caffeine consumption and our outcomes.Citation39 For fecundability and MAR treatment, we included only fixed effects in the meta-analysis due to the low number of included studies,Citation40 while for SAB, we conducted a random-effects meta-analysis after considering heterogeneity between studies. As coffee/caffeine consumption was reported on various scales, we converted exposure data into a uniform measurement (mg/day). Studies reporting consumption in cups of coffee were recalculated into an approximate caffeine content, assuming that one cup of coffee in general contains 100 mg caffeine.Citation4,Citation41 As the approximation of caffeine content per cup of coffee might be imprecise, a sensitivity analysis was performed, assuming that one cup of coffee contained 150 mg caffeine. Coffee/caffeine consumption was modeled using restricted cubic splines with three knots at the 10th, 50th, and 90th percentiles of the distribution of doses.Citation38,Citation42,Citation43 For each model, we present an overall p-value testing that the two regression coefficients describing the nonlinear relationship were simultaneously equal to zero. Also, upon finding a statistical significant association, we present a p-value testing the linear versus nonlinear relationship.Citation44 When analyzing risk of SAB, we performed stratified analyses by type of consumption (caffeine vs coffee), adjustment status (crude vs any adjustment), study quality (NOS>7 vs NOS<7), and study design (cohort vs case–control). Similar analyses were not possible for other outcomes due to the low number of studies. Heterogeneity between studies was assessed using the Cochrane Q-test and the I2 statistic. Low heterogeneity was defined by I2 values <25%, while a I2 value >75% was considered an indicator of substantial heterogeneity.Citation45 Publication bias was assessed for SAB studies, using Egger’s regression test.Citation46 As meta-analysis for fecundity and MAR endpoints only included a maximum of three studies, tests of heterogeneity and publication bias were irrelevant for these outcomes.Citation47 All statistical analyses were performed using the “dosresmeta” and “metafor” packages in R version 3.3.1.Citation48,Citation49 p-values <0.05 were considered statistically significant.
Results
Characteristics of the included studies
A total number of 379 articles were identified through the systematic literature search, and an additional 68 articles were identified through a manual search of their references (). Of the total 447 articles, 136 were duplicates and thus excluded. The remaining 311 unique articles were screened by title and, if necessary, by abstract, and 195 did not meet the eligibility criteria. Full-texts were assessed for the remaining 116 articles. Of these, 68 articles were excluded due to not meeting the eligibility criteria, and one article was excluded due to insufficient data reporting.
Figure 1 Flow diagram.
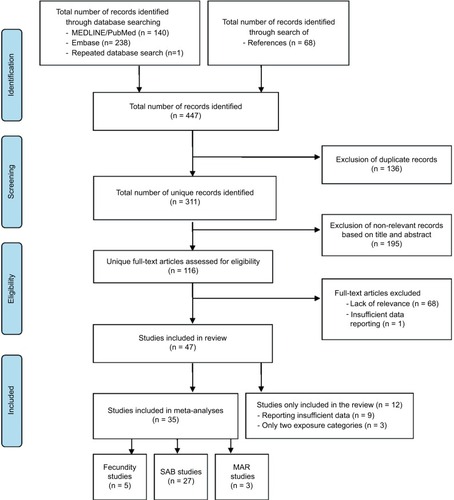
Thus, a total of 47 studies were included in the systematic review. Of these, 35 studies had dose–response information (ie, reporting at least three or more quantitative exposure categories) and were included in our meta-analyses. Of these 35 studies, 5 studies reported about the endpoints of fecundityCitation9,Citation10,Citation16,Citation19,Citation50, 27 studies reported about SAB,Citation21,Citation32,Citation34,Citation51–Citation73 and 3 studies reported on the outcomes of MAR.Citation74–Citation76 Results from the remaining 12 studies that did not provide sufficient data to be included in the meta-analysis are included as a narrative description.
All included studies were published between 1988 and 2015. Thirty-one were cohort studies, while 16 were case–control studies. Study characteristics, results, and the assigned total NOS scores are presented in – (for NOS elaborations, please see the Table S1). The presented results cover a variety of countries with large differences in exposure levels ranging from non-consumers to those who consume over 1,200 mg/day (corresponding to 12 cups of coffee/day). Also, adjustment for potential confounders varied considerably between studies (–).
Table 1 Characteristics and results of publications on coffee/caffeine and fecundity endpoints
Table 3 Characteristics and results of publications on coffee/caffeine and MAR treatment
FOR
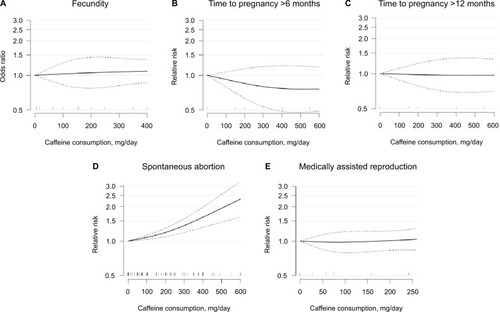
In the three cohort studies providing sufficient data to be included in the meta-analysis, we found no indication of an association between caffeine intake up to 400 mg/day and altered FOR (overall p=0.76; ). Compared with no caffeine intake, the pooled odds ratios for altered fecundability were 1.03 (95% confidence interval [CI]: 0.83; 1.28) for 100 mg caffeine/day and 1.09 (95% CI: 0.86; 1.37) for 400 mg caffeine/day.
Figure 2 Dose–response association between caffeine consumption and odds ratio of fecundability (A), relative risk of time to pregnancy >6 months (B) and >12 months (C), spontaneous abortion (D), and live birth rate among couples receiving MAR treatment (E) compared to 0 mg consumption as reference. Odds ratios/relative risks are plotted on the log scale with 95% confidence intervals for the spline model. Tick marks on the x-axis represent category medians of exposure from the included studies.
Studies not eligible for meta-analysis
Five other studies have addressed a possible association between coffee/caffeine consumption and fecundability with contradicting findings. Two studies from the USCitation13,Citation15 including a total of 104 and 6,303 women, respectively reported reduced fecundability with higher caffeine consumption in the late 1980s. However, results by three later studies (two European studies and one US study)Citation14,Citation17,Citation30 including 259 and 423, and 470 women, respectively, support the findings of no association between caffeine consumption on fecundability.
TTP
Only two cohort studies provided sufficient data on TTP, to be included in the dose–response meta-analysis. The results did not indicate an association (p=0.43 for TTP >6 months and p=0.98 for TTP >12 months) ( and ).
Compared with no caffeine intake, the pooled relative risks for TTP >6 months were 0.92 (95% CI: 0.79; 1.07) for 100 mg caffeine/day and 0.76 (95% CI: 0.49; 1.18) for 600 mg caffeine/day. For TTP >12 months, the pooled relative risks were 0.99 (95% CI: 0.88; 1.11) for 100 mg caffeine/day and 0.97 (95% CI: 0.71; 1.33) for 600 mg caffeine/day, compared with no caffeine intake.
Studies not eligible for meta-analysis
Two studies that were not included in the meta-analysis have investigated a possible association between caffeine consumption and TTP. Bolúmar et alCitation7 reported on 3,146 European women and found an increased risk of TTP >9.5 months with a caffeine intake of >500 mg/day when reporting retrospectively on their first pregnancy. However, no association was found when reporting on the most recent waiting time. Another study including 66 American womenCitation29 did not find an association between caffeine consumption and TTP.
SAB
We found that higher intake of caffeine was associated with higher risk of spontaneous abortion (overall association p<0.0001; p for non-linearity <0.01), based on 27 studies providing sufficient data to be included in the meta-analysis (). Compared with no caffeine intake, the pooled relative risks for SAB were 1.08 (95% CI: 1.03; 1.13) for 100 mg caffeine/day, 1.37 (95% CI: 1.19; 1.57) for 300 mg caffeine/day, and 2.32 (95% CI: 1.62; 3.31) for 600 mg caffeine/day. There was evidence of significant between-study heterogeneity (I2=73,7%; p<0.0001), and Egger’s regression test provided evidence of substantial publication bias (p<0.0001; ).
Table 2 Characteristics and results of publications on coffee/caffeine and spontaneous abortion (SAB)
We stratified the SAB analyses on type of consumption, adjustment status, study quality, and study design. The analyses revealed that the associations were similar between studies reporting caffeine and coffee consumption (p for heterogeneity=0.87). Also, the associations were similar across strata according to adjustment status (ie, studies with adjusted results compared to unadjusted results) (p for heterogeneity=0.44) and according to study quality (ie, comparing studies with NOS ≥7 with those of NOS <7) (p for heterogeneity=0.22). We found weak evidence of a difference by study design with the associations being more pronounced in cohort studies than in case–control studies (p for heterogeneity=0.04). In a sensitivity analysis, changing the conversion factor of caffeine contained in one cup of coffee from 100 mg to 150 mg did not substantially change the results.
Studies not eligible for meta-analysis
Five other studies, not included in the meta-analysis, have investigated a possible association between coffee/caffeine consumption and SAB with consistent findings in line with our results. A Swedish cohort study including 654 womenCitation31 reported an increased risk of SAB with a daily coffee consumption greater than three cups, while a case–control study among 452 Saudi-Arabian womenCitation37 showed an association at caffeine consumption levels >150 mg/day. Also, the association of an increased risk of SAB with caffeine consumption was found among a selected group of 191 American women with type-1 diabetes.Citation35 In an Italian case–control study including 312 women,Citation33 a dose–response association was reported between caffeine intake and risk of recurrent SAB. Also, Parazzini et alCitation36 found an association with any coffee consumption among women with recurrent pregnancy loss in a case–control study including 260 women; however, results were not statistically significant.
MAR treatment
Only two cohort studies provided sufficient data on live birth rate among couples undergoing in vitro fertilization (IVF) treatmentCitation74,Citation76 to be included in the dose–response meta-analysis. The results did not indicate an association between caffeine intake and the live birth rate among women in fertility treatment (p= 0.94; ). The pooled relative risks for achieving a live birth were 0.99 (95% CI: 0.89; 1.10) for 100 mg caffeine/day and 1.00 (95% CI: 0.80; 1.24) for 300 mg caffeine/day, compared with no caffeine intake.
Study not eligible for meta-analysis
Only one study by Al-Saleh et alCitation75 reported on the pregnancy rate among couples undergoing fertility treatment. The study showed no association between coffee/tea consumption or serum caffeine concentration and the success rate of pregnancy among 619 Saudi-Arabian women undergoing their first IVF-treatment cycle. However, the number of eggs was lower at higher levels of serum caffeine.
Discussion
This systematic review and meta-analysis showed no clear association between exposure to coffee/caffeine and natural fertility as measured by FOR or waiting TTP. However, due to the limited number of studies included, no firm conclusions can be drawn for these endpoints. Our pooled results indicate that coffee/caffeine consumption is associated with a significantly increased risk of SAB, as expected from previous reviews and meta-analyses.Citation23,Citation78,Citation79 Further, in addition to previous studies, we intended to capture nonlinear associations using novel statistical methods but found no evidence of a “threshold effect”. With regard to the potential effect of coffee or caffeine consumption on the outcomes of fertility treatment, our sparse results on MAR treatment as measured by the pregnancy and live birth rate in connection with IVF treatment did not show an association. Yet, the data available enable us to conclude little about the potential dose–response relationship.
Various hypotheses exist concerning the possible mechanisms of the potential effect of caffeine on different fecundity and pregnancy outcomes, but the eventual mechanisms are still unclear. Within the human body, caffeine acts as a non-selective adenosine antagonist;Citation80 it increases the intracellular concentration of cyclic AMPCitation81 and alters the blood levels of catecholamines.Citation82 Coffee and caffeine consumption may affect the reproductive health by affecting endogenous hormone levels through changes in ovarian function or alterations in hormone metabolism: numerous studies have reported an inverse association between coffee/caffeine intake and levels of free estradiolCitation83–Citation86 in line with the increased levels of sex hormone–binding globulin reported by others.Citation87–Citation89 However, contradicting results of increased levelsCitation76,Citation90 or no effects on estradiol levels are also reported.Citation87,Citation88,Citation91,Citation92 Caffeine and estradiol are both metabolized by the hepatic enzyme CYP1A2Citation93,Citation94, so a possible pathway for caffeine to interfere with estradiol levels is through a common metabolism. Also, besides caffeine, coffee contains numerous other bioactive substances including lignans and isoflavonoids, both belonging to the phytoestrogen family with great affinity for the estrogen receptor.Citation4 As a consequence, changes in hormonal levels might impact on the menstrual cycle, and a daily caffeine consumption >300 mg has been associated with shorter but not with longer menstrual cycle length.Citation95 Moreover, caffeine intake was not associated with the number of oocytes retrieved, the fertilization rate, or implantation rate among women receiving fertility treatment.Citation76 The conflicting results on coffee’s potential effect on the hormonal pathways are in line with our results suggesting no clear association with fecundity endpoints. In pregnant women, caffeine readily crosses the placental barrier and as a result is distributed to all fetal tissue, making the fetus exposed to the same caffeine levels as the mother.Citation96 Also, coffee intake has been associated with decreased levels of both estrogen and hCG,Citation97 and caffeine consumption during pregnancy is shown to increase levels of catecholamines and cyclic adenosine monophosphate that might impact on placental blood flow.Citation98–Citation100 Indeed, these pathways could have an influence on the increased risk of SAB as observed in this meta-analysis.
This review and meta-analysis has several strengths, including the broader investigation of possible routes of interfering with the ability to conceive and carry a pregnancy to term. Another strength is the dose–response analysis, allowing us to include all information on exposure outcome by including information on intermediate categories, thus making the analysis more effective than the traditional highest versus lowest approach. Using this method, we were able to provide a detailed and more flexible description of the risk of outcome throughout the observed range of exposure. For the SAB analysis, we were able to include a relatively large number of studies providing higher statistical power and allowing us to perform stratified analyses. Hence, we were able to consider potential sources of heterogeneity, including taking into account the varying quality of the included studies.
However, this systematic review and dose–response meta-analysis also has several potential limitations. Though a majority of the included studies adjusted for potential confounders, the presence of residual or unmeasured confounding cannot be excluded due to the observational nature of the included studies. We observed marked between-study heterogeneity, which can be caused by methodological or actual differences between the included studies. Consequently, data on SAB were analyzed using a random-effects model. In addition, possible sources of heterogeneity in SAB studies were addressed in stratified analysis, and only study design was found of significance.
Based on the current knowledge, we chose alcohol instead of smoking to be the second most important factor to adjust for in studies reporting on SAB. However, had smoking been selected instead, the NOS would have differed only by one point in three of the 33 evaluated studies as 18 adjusted for both alcohol consumption and smoking, while 12 did not adjust for either of the two. A priori, we determined the threshold for depicting a high-quality study as an NOS ≥7. However, changing the threshold in a sensitivity analysis to NOS ≥8 did not noticeably alter the association in the two strata (p for heterogeneity=0.28).
We found evidence of publication bias for studies reporting on SAB, indicating that small studies not reporting any association are less likely to be published. Thus, results from SAB analysis should be interpreted bearing this in mind. Due to the limited number of studies reporting sufficient data on fecundity or MAR endpoints, assessment of publication bias for these could not be done.
As data on caffeine were self-reported and obtained by various questionnaires or interview, exposure misclassification of coffee/caffeine intake is unavoidable. Especially studies with retrospectively collected exposure data are prone to recall bias. Further, due to the numerous types of questionnaires used to assess exposure, the accuracy and data quality are expected to differ accordingly.
Yet, validation studies support that coffee consumption can be assessed with fairly high validity.Citation101 Due to the various sources of exposure, it is difficult to estimate the total caffeine consumption accurately. Further, coffee contains a series of different chemical substances, making it difficult to segregate potential biological effects from caffeine from those of other bioactive compounds. Also, content of the different substances in coffee varies by type of bean, brewing method, and cup size.Citation102 Thus, a possible association might be caused by other compounds or by a cocktail effect due to simultaneous exposure to multiple bioactive substances. However, most studies have focused on exposure to caffeine and thus only to some extent on exposure to coffee. In general, exposure assessment was reported as the average daily intake, and consequently we were not able to take the consumption patterns of coffee/caffeine into account. Also, different conversion factors were used in studies when translating coffee consumption into caffeine. In the meta-analysis, we tried to quantify the amount of caffeine intake when exposure was only reported as cups of coffee, but by doing so, we were unable to integrate the pronounced variation in caffeine content by different types of coffee consumed. However, changing the conversion factor up to 150 mg caffeine per cup of coffee in a sensitivity analyses did not change the risk of SAB markedly.
The actual level of caffeine exposure might vary greatly due to individual differences in the CYP1A2 gene activity.Citation70,Citation103 Hence, polymorphism of CYP1A2 has been linked to both variability in the clearance rate of caffeineCitation104 and variability in serum estradiol concentrations.Citation105 As a consequence, the half-life of caffeine varies between 1.5 hours for fast metabolizers and up to 10 hours for slow metabolizers,Citation4 making it difficult to settle on a relevant window of exposure.
In the context of SAB, reverse causation has to be considered; a viable pregnancy might produce more pronounced pregnancy symptoms, resulting in greater aversion to coffee and thus a decreased caffeine intake. However, a clinically verified SAB may be diagnosed weeks after the actual fetal demise and thus the yet unrecognized pregnancy loss might be the cause of an increased caffeine consumption rather than the opposite – an increased consumption causing adverse reproductive outcomes. In contrast to previous meta-analysesCitation78,Citation79 that presented pooled endpoints of SAB with still birth/fetal death, we only included SAB, as the underlying etiology indeed are different.
Six cohort studies out of the included 32 studies on SAB verified the presence of a pregnancy at the time of reporting exposure, thereby reducing the risk of reversed causation. Among these studies, an association between caffeine intake and SAB was indicated, albeit only statistically significant in three studies.
Due to the great differences in caffeine metabolism, future studies may benefit from actually evaluating circulating caffeine levels or its metabolites (eg, serum paraxanthine, the main metabolite) in linkage with genotyping to heighten the information of the actual exposure level. Thus, future studies could consider Mendelian randomization. Also, to possibly segregate effects of caffeine from those of other bioactive substances in coffee, future studies could consider evaluating the consumption of decaffeinated coffee.
Conclusion
In conclusion, results from this dose–response meta-analysis support the evidence of an association between coffee/caffeine intake and the risk of SAB. However, results from the SAB analyses have to be interpreted with caution due to the significant heterogeneity and risk of bias detected, not least the considerable risk of publication bias. As coffee is the main source of caffeine consumption, it is still unclear whether the association between coffee/caffeine consumption and SAB is related to the potential harmful effects of caffeine or to some of the other bioactive components of coffee. Viewing the reproductive capacity in a broader perspective, there seems to be little, if any, association between coffee/caffeine consumption and fecundity. Even so, there is still a need for further studies to investigate the fecundity and MAR endpoints on a larger scale than previously done, using better study designs and including improved reporting combined with relevant adjustment strategies.
Author contributions
All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Acknowledgments
JL is supported by a fully financed PhD-scholarship from Aarhus University. AH is supported by the Danish Diabetes Academy. The Danish Diabetes Academy is funded by the Novo Nordisk Foundation. The funding sources had no involvement in the conduct of this article.
Disclosure
The authors report no conflicts of interest in this work.
References
- JuulSKarmausWOlsenJRegional differences in waiting time to pregnancy: pregnancy-based surveys from Denmark, France, Germany, Italy and Sweden. The European Infertility and Subfecundity Study GroupHum Reprod19991451250125410325272
- SchmidtLInfertility and assisted reproduction in Denmark. Epidemiology and psychosocial consequencesDan Med Bull20065339041717150146
- JacobMCMcQuillanJGreilALPsychological distress by type of fertility barrierHum Reprod200722388589417178745
- HermansenKBechBHDragstedLO“Kaffe, sundhed og sygdom”, Vidensråd for Forebyggelse. [Coffee, health and disease]2015 Available from: http://www.vidensraad.dk/sites/default/files/vidensrad_for_forebyggelse_kaffe_sundhed_og_sygdom_2015.pdfAccessed November 13, 2017 Danish
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA)Scientific Opinion on the safety of caffeineEFSA J20151354102
- WHORecommendations on Antenatal Care for a Positive Pregnancy ExperienceGenevaWHO2016152
- BolumarFOlsenJRebagliatoMBisantiLCaffeine intake and delayed conception: a European multicenter study on infertility and subfecundity. European Study Group on Infertility SubfecundityAm J Epidemiol199714543243349054236
- HatchEEBrackenMBAssociation of delayed conception with caffeine consumptionAm J Epidemiol199313812108210928266910
- OlsenJCigarette smoking, tea and coffee drinking, and subfecundityAm J Epidemiol199113377347392018028
- AldereteEEskenaziBSholtzREffect of cigarette smoking and coffee drinking on time to conceptionEpidemiology1995644034087548349
- JoesoefMRBeralVRolfsRTAralSOCramerDWAre caffeinated beverages risk factors for delayed conception?Lancet199033586821361371967434
- CurtisKMSavitzDAArbuckleTEEffects of cigarette smoking, caffeine consumption, and alcohol intake on fecundability19971463241
- ChristiansonREOechsliFWBergBJCaffeinated beverages and decreased fertilityLancet198918634378
- JensenTKHenriksenTBHjollundNHCaffeine intake and fecundability: a follow-up study among 430 Danish couples planning their first pregnancyReprod Toxicol19981232892959628552
- WilcoxAWeinbergCBairdDCaffeinated beverages and decreased fertilityLancet198828626–8627145314562904572
- CaanBQuesenberryCPJrCoatesAODifferences in fertility associated with caffeinated beverage consumptionAm J Public Health19988822702749491020
- FlorackEIZielhuisGARollandRCigarette smoking, alcohol consumption, and caffeine intake and fecundabilityPrev Med19942321751808047523
- SpinelliAFiga-TalamancaIOsbornJTime to pregnancy and occupation in a group of Italian womenInt J Epidemiol19972636016099222786
- HakimRBGrayRHZacurHAlcohol and caffeine consumption and decreased fertilityFertil Steril1998706326379797089
- MatijasevichABarrosFCSantosISYeminiAMaternal caffeine consumption and fetal death: a case-control study in UruguayPaediatr Perinat Epidemiol200620210010916466428
- BechBHNohrEAVaethMHenriksenTBOlsenJCoffee and fetal death: a cohort study with prospective dataAm J Epidemiol20051621098399016207803
- WisborgKKesmodelUBechBHHedegaardMHenriksenTBMaternal consumption of coffee during pregnancy and stillbirth and infant death in first year of life: prospective studyBMJ2003326738642012595379
- GreenwoodDCThatcherNJYeJCaffeine intake during pregnancy and adverse birth outcomes: a systematic review and dose-response meta-analysisEur J Epidemiol2014291072573425179792
- MaslovaEBhattacharyaSLinSWMichelsKBCaffeine consumption during pregnancy and risk of preterm birth: a meta-analysisAm J Clin Nutr20109251120113220844077
- PROSPEROInternational prospective register of systematic reviews2017 Available from: https://www.crd.york.ac.uk/PROSPERO/Accessed November 13, 2017
- WellsGASheaBO’ConnellDNewcastle-Ottawa Scale (NOS)2017 Available from: http://www.ohri.ca/programs/clinical_epidemiology/oxford.aspAccessed May 8, 2017
- LiberatiAAltmanDGTetzlaffJThe PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaborationAnn Intern Med20091514W65W9419622512
- WilcoxAFertility and PregnancyNew York, NYOxford University Press2010
- PollackAZBuck LouisGMSundaramRLumKJCaffeine consumption and miscarriage: a prospective cohort studyFertil Steril201093130430619732873
- TaylorKCSmallCMDominguezCEAlcohol, smoking, and caffeine in relation to fecundability, with effect modification by NAT2Ann Epidemiol2011211186487221684175
- AxelssonGRylanderROutcome of pregnancy in women engaged in laboratory work at a petrochemical plantAm J Ind Med19891655395452589330
- CnattingiusSSignorelloLBAnnerenGCaffeine intake and the risk of first-trimester spontaneous abortionN Engl J Med2000343251839184511117975
- StefanidouEMCaramellinoLPatriarcaAMenatoGMaternal caffeine consumption and sine causa recurrent miscarriageEur J Obstet Gynecol Reprod Biol2011158222022421636205
- SrisuphanWFBrackenMBCaffeine consumption during pregnancy and association with late spontaneous abortion198615411420
- KhouryJCMiodovnikMBuncherCRConsequences of smoking and caffeine consumption during pregnancy in women with type 1 diabetesJ Matern Fetal Neonatal Med2004151445015101611
- ParazziniFBoccioloneLFedeleLNegriELa VecchiaCAcaiaBRisk factors for spontaneous abortionInt J Epidemiol19912011571612066215
- LubnaAAl-AnsaryZABRisk factors for spontaneous abortion: a preliminary study on Saudi womenJ Roy Soc Health19941141881937932496
- OrsiniNLiRWolkAKhudyakovPSpiegelmanDMeta-analysis for linear and nonlinear dose-response relations: examples, an evaluation of approximations, and softwareAm J Epidemiol20121751667322135359
- CrippaAONDose-response meta-analysis of differences in meansBMC Med Res Methodol2016169127485429
- ChenDGFangDWilsonJRMeta-analysis of two studies with random effects?J Minim Invasive Gynecol201724568969028552623
- McCuskerRRGoldbergerBAConeEJCaffeine content of specialty coffeesJ Anal Toxicol200327752052214607010
- GreenlandSDose-response and trend analysis in epidemiology: alternatives to categorical analysisEpidemiology1995643563657548341
- DurrlemanSSimonRFlexible regression models with cubic splinesStat Med1989855515612657958
- DesquilbetLMariottiFDose-response analyses using restricted cubic spline functions in public health researchStat Med20102991037105720087875
- HigginsJPThompsonSGDeeksJJAltmanDGMeasuring inconsistency in meta-analysesBMJ2003327741455756012958120
- EggerMDavey SmithGSchneiderMMinderCBias in meta-analysis detected by a simple, graphical testBMJ199731571096296349310563
- Green JPHaSCochrane Handbook for Systematic Reviews of Interventions2017 Available from: http://handbook.cochrane.org/chapter_10/10_4_3_1_recommendations_on_testing_for_funnel_plot_asymmetry.htmAccessed June 2, 2017
- R Core TeamR: A language and environment for statistical computing2009 Available from: https://www.r-project.orgAccessed November 13, 2017
- ViechtbauerWConducting meta-analyses in R with metafor packageJ Stat Softw201036348
- HatchEEWiseLAMikkelsenEMCaffeinated beverage and soda consumption and time to pregnancyEpidemiology201223339340122407137
- FensterLEskenaziBWindhamGCSwanSHCaffeine consumption during pregnancy and spontaneous abortionEpidemiology1991231681742054397
- FensterLHubbardAESwanSHCaffeinated beverages, decaffeinated coffee, and spontaneous abortionEpidemiology1997855155239270953
- ArmstrongBGMcDonaldADSloanMCigarette, alcohol, and coffee consumption and spontaneous abortionAm J Public Health199282185871536340
- Dominguez-RojasVde Juanes-PardoRAstasio-ArbizaPOrtega-MolinaPGordillo-FlorencioESpontaneous abortion in a hospital population: are tobacco and coffee intake risk factors?Eur J Epidemiol19941066656687672044
- DlugoszLBelangerKHellenbrandKHolfordTRLeadererBBrackenMBMaternal caffeine consumption and spontaneous abortion: a prospective cohort studyEpidemiology1996732502558728437
- AgnesiRValentiniFFedeliUMaternal exposures and risk of spontaneous abortion before and after a community oriented health education campaignEur J Public Health201021328228520534692
- AgnesiRValentiniFMastrangeloGRisk of spontaneous abortion and maternal exposure to organic solvents in the shoe industryInt Arch Occup Environ Health19976953113169192214
- GiannelliMDoylePRomanEPelerinMHermonCThe effect of caffeine consumption and nausea on the risk of miscarriagePaediatr Perinat Epidemiol200317431632314629312
- GeorgeLGranathFJohanssonALOlanderBCnattingiusSRisks of repeated miscarriagePaediatr Perinat Epidemiol200620211912616466430
- KlineJLevinBSilvermanJCaffeine and spontaneous abortion of known karyotypeEpidemiology1991264094171790192
- Infante-RivardCFernandezAGauthierRDavidMRivardGEFetal loss associated with caffeine intake before and during pregnancyJAMA199327024294029438254854
- MillsJLHolmesLBAaronsJHModerate caffeine use and the risk of spontaneous-abortion and intrauterine growth-retardationJAMA199326955935978421363
- ParazziniFChatenoudLDi CintioECoffee consumption and risk of hospitalized miscarriage before 12 weeks of gestationHum Reprod1998138228622919756312
- MaconochieNDoylePPriorSSimmonsRRisk factors for first trimester miscarriage – results from a UK-population-based case-control studyBJOG2007114217018617305901
- GreenwoodDCAlwanNBoylanSCaffeine intake during pregnancy, late miscarriage and stillbirthEur J Epidemiol201025427528020306287
- WilcoxAJWeinbergCRBairdDDRisk factors for early pregnancy lossEpidemiology1990153823852078614
- ZhangHBrackenMBTree-based, two-stage risk factor analysis for spontaneous abortionAm J Epidemiol1996144109899968916510
- WenWShuXOJacobsDRJrBrownJEThe associations of maternal caffeine consumption and nausea with spontaneous abortionEpidemiology2001121384211138817
- TolstrupJSMunkCMadsenLBOttesenBBergholtTGronbaekMDoes caffeine and alcohol intake before pregnancy predict the occurrence of spontaneous abortion?Hum Reprod200318122704271014645195
- SataFYamadaHSuzukiKCaffeine intake, CYP1A2 polymorphism and the risk of recurrent pregnancy lossMol Hum Reprod200511535736015849225
- SavitzDAChanRLHerringAHHowardsPPHartmannKECaffeine and miscarriage riskEpidemiology2008191556218091004
- WengXOdouliRLiDKMaternal caffeine consumption during pregnancy and the risk of miscarriage: a prospective cohort studyAm J Obstet Gynecol20081983279.e1818221932
- HahnKAWiseLARothmanKJCaffeine and caffeinated beverage consumption and risk of spontaneous abortionHum Reprod20153051246125525788567
- Klonoff-CohenHBlehaJLam-KruglickPA prospective study of the effects of female and male caffeine consumption on the reproductive endpoints of IVF and gamete intra-Fallopian transferHum Reprod20021771746175412093834
- Al-SalehIEl-DoushIGrisellhiBCoskunSThe effect of caffeine consumption on the success rate of pregnancy as well various performance parameters of in-vitro fertilization treatmentMed Sci Monit20101612CR598CR60521119578
- ChoiJHRyanLMCramerDWHornsteinMDMissmerSAEffects of caffeine consumption by women and men on the outcome of in vitro fertilizationJ Caffeine Res201111293424761261
- RaschVCigarette, alcohol, and caffeine consumption: risk factors for spontaneous abortionActa Obstet Gynecol Scand200382218218812648183
- LiJZhaoHSongJMZhangJTangYLXinCMA meta-analysis of risk of pregnancy loss and caffeine and coffee consumption during pregnancyInt J Gynaecol Obstet2015130211612226026343
- ChenLWWuYNeelakantanNChongMFPanAvan DamRMMaternal caffeine intake during pregnancy and risk of pregnancy loss: a categorical and dose-response meta-analysis of prospective studiesPublic Health Nutr20161971233124426329421
- FredholmBBOn the mechanism of action of theophylline and caffeineActa Med Scand198521721491532986418
- SoykaLFEffects of methylxanthines on the fetusClin Perinatol1979613751225087
- BelletSRomanLDeCastroOKimKEKershbaumAEffect of coffee ingestion on catecholamine releaseMetabolism19691842882915777013
- LondonSWillettWLongcopeCMcKinlaySAlcohol and other dietary factors in relation to serum hormone concentrations in women at climactericAm J Clin Nutr19915311661711845789
- PetridouEKatsouyanniKSpanosESkalkidisYPanagiotopoulouKTrichopoulosDPregnancy estrogens in relation to coffee and alcohol intakeAnn Epidemiol1992232412471342274
- KotsopoulosJEliassenAHMissmerSAHankinsonSETworogerSSRelationship between caffeine intake and plasma sex hormone concentrations in premenopausal and postmenopausal womenCancer2009115122765277419384973
- SchliepKCSchistermanEFMumfordSLCaffeinated beverage intake and reproductive hormones among premenopausal women in the BioCycle StudyAm J Clin Nutr201295248849722237060
- GotoASongYChenBHMansonJEBuringJELiuSCoffee and caffeine consumption in relation to sex hormone-binding globulin and risk of type 2 diabetes in postmenopausal womenDiabetes201160126927521030499
- NagataCKabutoMShimizuHAssociation of coffee, green tea, and caffeine intakes with serum concentrations of estradiol and sex hormone-binding globulin in premenopausal Japanese womenNutr Cancer199830121249507508
- FerriniRLBarrett-ConnorECaffeine intake and endogenous sex steroid levels in postmenopausal women. The Rancho Bernardo StudyAm J Epidemiol199614476426448823059
- LuceroJHarlowBLBarbieriRLSlussPCramerDWEarly follicular phase hormone levels in relation to patterns of alcohol, tobacco, and coffee useFertil Steril200176472372911591405
- KinneyAKlineJKellyAReussMLLevinBSmoking, alcohol and caffeine in relation to ovarian age during the reproductive yearsHum Reprod20072241175118517261576
- CooperCAtkinsonEJWahnerHWIs caffeine consumption a risk factor for osteoporosis?J Bone Miner Res1992744654711609631
- ButlerMAIwasakiMGuengerichFPKadlubarFFHuman cytochrome P-450PA (P-450IA2), the phenacetin O-deethylase, is primarily responsible for the hepatic 3-demethylation of caffeine and N-oxidation of carcinogenic arylaminesProc Natl Acad Sci U S A19898620769677002813353
- YamazakiHShawPMGuengerichFPShimadaTRoles of cytochromes P450 1A2 and 3A4 in the oxidation of estradiol and estrone in human liver microsomesChem Res Toxicol19981166596659625734
- FensterLQualeCWallerKCaffeine consumption and menstrual functionAm J Epidemiol1999149655055710084244
- AldridgeABaileyJNeimsAHThe disposition of caffeine during and after pregnancySemin Perinatol1981543103147302604
- LawsonCCLeMastersGKLevinLSLiuJHPregnancy hormone metabolite patterns, pregnancy symptoms, and coffee consumptionAm J Epidemiol2002156542843712196312
- KirkinenPJouppilaPKoivulaAVuoriJPuukkaMThe effect of caffeine on placental and fetal blood flow in human pregnancyAm J Obstet Gynecol198314789399426650631
- WeathersbeePSLodgeJRCaffeine: its direct and indirect influence on reproductionJ Reprod Med19771925563197235
- MorrisMBWeinsteinLCaffeine and the fetus: is trouble brewing?Am J Obstet Gynecol198114066076107258232
- FerraroniMTavaniADecarliAReproducibility and validity of coffee and tea consumption in ItalyEur J Clin Nutr200458467468015042137
- BrackenMBTricheEGrossoLHellenbrandKBelangerKLeadererBPHeterogeneity in assessing self-reports of caffeine exposure: implications for studies of health effectsEpidemiology200213216517111880757
- GrossoLMBrackenMBCaffeine metabolism, genetics, and perinatal outcomes: a review of exposure assessment considerations during pregnancyAnn Epidemiol200515646046615967394
- SachseCBrockmollerJBauerSRootsIFunctional significance of a C-->A polymorphism in intron 1 of the cytochrome P450 CYP1A2 gene tested with caffeineBr J Clin Pharmacol199947444544910233211
- LurieGMaskarinecGKaaksRStanczykFZLe MarchandLAssociation of genetic polymorphisms with serum estrogens measured multiple times during a 2-year period in premenopausal womenCancer Epidemiol Biomarkers Prev20051461521152715941966