
Abstract
Background
Excess body weight in adulthood is associated with risk for asthma admission (AA). Our aim was to investigate if this association also applies to the relation between body mass index (BMI) in childhood and AAs in early adulthood (age 20–45 years).
Methods
This was a prospective study of 310,211 schoolchildren (born 1930–1989) from the Copenhagen School Health Records Register. Height and weight were measured annually, and generated BMI z-scores were categorized as low (lower quartile), normal (interquartile) and high (upper quartile). Associations between BMI at ages 7–13 and AA were estimated by Cox regressions, and presented as hazard ratios (HRs) and 95% confidence intervals (CI). Main outcome was incident hospital AAs (extracted from the Danish National Patient Register) in early adulthood.
Results
During 4,708,607 person-years of follow-up, 1,813 incident AAs were observed. Nonlinear associations were detected between childhood BMI and AAs. The risk of AA increased for females in the highest BMI category in childhood, with the highest HR of 1.3 (95% CI 1.16–1.55) at the age of 13 years. By contrast, males in the low BMI category had a higher risk of AA in early adulthood, with the highest HR of 1.24 (95% CI 1.03–1.51) at the age of 12 years. Females with an increase in BMI between ages 7 and 13 years had an increased risk of AA compared with females with stable BMI (HR 1.28, 95% CI 1.10–1.50).
Conclusion
The association between childhood BMI and AA in early adulthood is non-linear. High BMI increases the risk of AA in females, whereas low BMI increases the risk in males.
Introduction
The association between obesity and incident asthma in adults was first described by Camargo et al in 1999,Citation1 and has more recently been reported in children.Citation2 However, the mechanisms underlying the association are still incompletely understood.Citation3 Furthermore, studies have also shown that obesity in both children and adults is associated with increased asthma incidence and severity,Citation3,Citation4 together with a less favorable response to both reliever and controller medication for asthma.Citation5–Citation7
Based on 18 years of follow-up of the Isle of Wight birth cohort (n=1,456), Ziyab et alCitation8 reported that early persistent obesity is associated with a 2.2-fold increased risk of having asthma. In line with this, Egan et alCitation9 reported from an 11-year follow-up of adolescents in the Norwegian HUNT study that individuals with general overweight and abdominal obesity had an increased risk of asthma. However, large-scale studies with longer follow-up time are likely to add important knowledge regarding the association between body mass index (BMI) in childhood and hospital admissions for asthma later in life.
Previous studies of sex differences in the impact of adiposity on the risk of asthma have yielded conflicting results.Citation9,Citation10 In keeping with this, Benedetti et alCitation11 reported from a cross-sectional study of adolescents that both general overweight and abdominal adiposity in girls were associated with a high prevalence of asthma, whereas in boys it was primarily excess abdominal adiposity that was associated with a higher risk of asthma. Furthermore, based on a cross-sectional study of 4,828 adolescents, Lu et alCitation12 reported that overweight/obesity was associated with an increased prevalence of asthma in girls but not in boys. However, by contrast, Chen et alCitation13 reported from a cross-sectional study of approximately 7,192 boys and girls from Taiwan that the effect of asthma and high BMI on forced expiratory volume in 1 second/forced vital capacity ratio was more pronounced in boys than in girls. Our current knowledge, therefore, points to potentially important differences in the impact of childhood BMI on long-term asthma risk in males and females.
Schatz et alCitation14 showed in a cohort of children (n=10,700) and adults (n=17,316) that a higher BMI was associated with an increased risk of asthma exacerbations and, in a further analysis of data from the same cohort, that obesity at baseline was associated with subsequent poor asthma control, including exacerbations.Citation15 The latter observation is in accordance with a recently published study of 90 patients evaluated at a clinic specialized in severe asthma by Tay et al.Citation16
Asthma is a heterogeneous disease. Compared with asthma with onset in childhood, adult-onset asthma is not only more often non-allergic, but also generally more difficult to controlCitation17 and has a less favorable prognosis with regard to morbidity and long-term outcomes.Citation18–Citation21 Furthermore, in middle-aged and older adults it can be problematic to distinguish asthma from COPD as these patients frequently have a non-reversible airflow limitation at the time of diagnosis.Citation18 Based on these observations, we therefore decided to focus the present analysis on asthma admissions (AAs) in individuals in the age group of 20–45-years.
As far too many children are overweight or obese worldwide,Citation22 it is of utmost importance to understand the consequences of excess body weight on the risk for asthma exacerbations of such severity that they lead to hospital admissions. In the present study of a very large cohort of schoolchildren, we therefore investigated the association between BMI in childhood and incident hospital admissions for asthma in early adulthood, focusing on potential differences between females and males.
Methods
Study population
We studied 310,211 children born from 1930 through 1989 who were included in the Copenhagen School Health Records Register (CSHRR). All schoolchildren underwent mandatory annual health examinations at public or private schools in Copenhagen from 1st to 7th grade through 1983 and thereafter only at school entrance and exit, unless the child had specific health requirements. As part of the examinations, performed by school doctors or nurses, height and weight were measured (with the child either naked or wearing light clothes). All children were assigned a health card on which the child’s name, date of birth, birth weight as reported by the parents, and yearly height and weight were recorded. As described previously, the register can be considered virtually complete with regard to inclusion of Copenhagen’s school children.Citation23
BMI was calculated as weight in kilograms divided by the square of height in meters for each child at each age. Internal age- and sex-specific BMI references were calculated using data from health examinations performed for children born from 1955 to 1960, when the prevalence of obesity was low and stable. Afterwards, BMI z-scores were calculated using the Lambda Mu Sigma method.Citation24 Positive values indicate a BMI value higher than the average and negative values indicate a BMI value lower than the average in our reference population. BMI data and corresponding z-scores (and percentiles) were available from ages 7 through 13 years.
From 1968 onwards, all Danish citizens were assigned a unique identification number.Citation25 These numbers were recorded on the health cards for children attending school at this time or thereafter, and they were retrieved for children who left school prior to this time.Citation23 Using the identification numbers, linkages were made to the Danish National Patient Register (DNPR), which contains information on discharge diagnoses from all somatic hospitals in Denmark since 1977 and from emergency and outpatient departments since 1995.Citation26
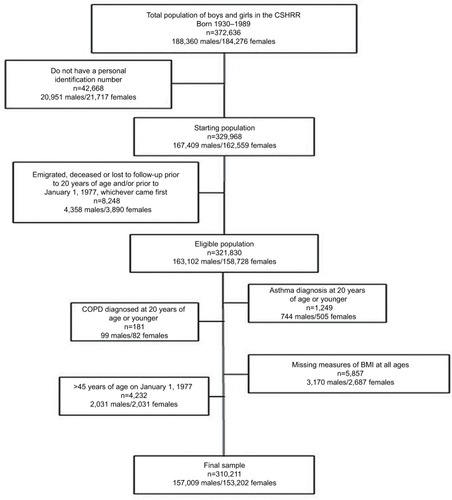
Information about hospital admissions for asthma and chronic obstructive lung disease up to age 45 years for children (n=321,830) included in the CSHRR was obtained by linking to the DNPR. All diagnoses in DNPR are classified according to the International Classification of Diseases (ICD); ICD-8 until 1994 and ICD-10 thereafter as ICD-9 codes were never implemented in Denmark. Data were extracted for first-ever diagnoses of asthma (ICD-8: 493 and ICD-10: J45-46) and COPD (ICD-8: 490-92, 494-96 and ICD-10: J40-44) as primary diagnoses. As the focus of the present analysis was incidence of first-ever AA, individuals with asthma or COPD admission before the age of 20 years (n=1,249 and n=181, respectively) were excluded; further details are given in .
Figure 1 Flowchart of individuals from the CSHRR included in the present analysis.
The primary outcome of interest was first-ever hospital admission for asthma until age 45 years. The age limit of 45 years was chosen, as distinguishing asthma from COPD can be problematic in older adultsCitation21 together with previous reports showing that late-onset asthma differs from early-onset asthma with regard to morbidity and outcomes.Citation20
Follow-up of individuals began at 20 years of age or on 1st January 1977 (when the DNPR was established), whichever came later. We chose 20 years as the earliest entry age to restrict our analyses to new-onset asthma in adulthood. Individuals were followed up until date of asthma hospital admission, the date of death, emigration or December 31, 2013, whichever came last.
Statistical analysis and ethics
Descriptive statistics (mean and standard deviation [SD]) were computed for BMI from age 7 through 13 years. Furthermore, the incidence rate per 10,000 person-years of follow-up by age group, sex and AA was computed as the incidence divided by the person-years at risk.
Cox proportional hazards regressions were used to examine association between childhood BMI z-scores at each age from 7 to 13 years and the risk of hospital admission for asthma between 20 and 45 years of age with age as the underlying time scale. Linearity was assessed by testing against a restricted cubic spline with four knots. Analyses were performed with individuals stratified according to birth cohort and separately for females and males. The results of the analyses are presented as the estimated hazard ratio (HR) and the corresponding 95% confidence intervals (95% CI); furthermore, the fitted association and corresponding confidence bands were plotted. The proportional hazard assumptions were assessed by a test based on Schoenfeld residuals, and no significant deviations were detected.
Further analyses of the risk for AA were carried out by categorizing the childhood BMI z-scores into three groups by age and sex: lower quartile, interquartile range and upper quartile. The estimation of risk was analyzed in a Cox proportional hazards regression model with categorized BMI z-score as a factor and with individuals stratified according to birth cohort; the underlying time scale was age and the analyses were performed separately for males and females.
This study was approved by the Danish Data Protection Agency. According to Danish law, ethical approval is not required for secondary analyses of data derived from registers. The data used in the present study are based on a combination of data with personal identification numbers from third parties, the CSHRR and data from national health registers. Furthermore, also according to Danish law, this information cannot be publicly available, but access to the subset of data included in the present study may be obtained by submitting a project application to the senior author Jenifer L Baker and pending approval by the data steering committee.
Results
Cohort characteristics
Height and weight measurements, and therefore BMI data, were available for 310,211 individuals. As expected for children, the mean BMI values and SDs increased with age from 15.5 kg/m2 (SD 1.3) at age 7 years to 18.4 kg/m2 (SD 2.4) at age 13 years. During the 36-year study period, 1,148 females and 665 males had at least one hospital admission for asthma between age 20 and 45 years. There were 4,708,607 person-years of follow-up.
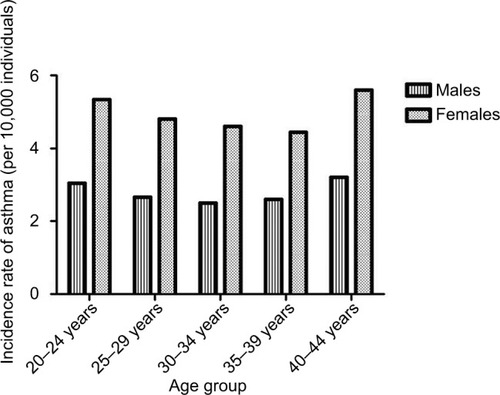
The incidence rate for first AA in adulthood was 3.85 per 10,000 person-years of follow-up and was very similar across age groups. As expected, a higher incidence rate was observed for females than for males in all age groups ().
Figure 2 Incidence rate of asthma admissions between age 20 and 45 years in individuals from the Copenhagen School Health Records Register (n=310,211) by age group and sex.
Investigating linearity of the association between childhood BMI and AA
The fitted functional form and corresponding confidence intervals for associations between childhood BMI z-score for females and males at ages 7 and 13 years, respectively, and risk of AA in early adulthood (age 20–45 years) are given in . Significant deviations from linearity were observed at all ages for females and males (all p-values ≤0.009).
Figure 3 Association between childhood BMI z-scores at ages 7 and 13 years for females and males, respectively, and first-ever hospital admissions for asthma in early adulthood (between age 20 and 45 years) among individuals in the Copenhagen School Health Records Register (n=310,211).
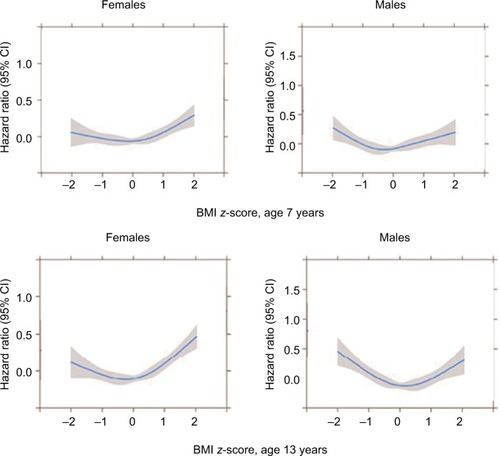
In females, higher BMI z-scores at age 7 years increased the risk of hospital admission for asthma in early adulthood (). The risks started to significantly increase around values of 0.5 z-scores, which is equivalent to the 70th percentile of the BMI distribution. BMI z-scores below 0.5 were not significantly associated with AAs as the confidence intervals included 1. At age 13 years, the pattern was similar except that BMI z-scores just smaller and greater than average (z-score=0) were significantly associated with a reduced risk of AAs. In contrast with the females, among males low BMI z-scores at age 7 years increased the risk of AAs (). At age 13 years, the estimates were stronger, and the risks began to increase for boys with a BMI z-score of approximately −1, which is equivalent to the 16th percentile of the BMI distribution. Similar to the females, boys with z-scores just around the average (z-score=0) had significantly reduced risks for AAs.
Childhood BMI and risk for AA in early adulthood
The risk of AA was significantly higher for females with a BMI in the highest quartile in childhood than in females with a normal BMI (value within the interquartile range), with the highest HR of 1.34 (95% CI 1.16–1.55) at the age of 13 years (). The risk of AA for females who had a BMI in the lowest quartile in childhood was not significantly different from the risk in females with a normal BMI (HR 1.05, 95% CI 0.90–1.23, at age 13 years). By contrast, among males, and similar to what is illustrated in , there was a consistent pattern that males with a childhood BMI in the lowest quartile in childhood had a higher risk of AA in early adulthood than males with normal BMI, although these differences did not always reach statistical significance. The highest HR was observed at the age of 12 years, with a value of 1.24 (95% CI 1.03–1.51) (). The risk of incident AAs for males with high BMI values in childhood was not significantly higher than for males with normal BMI at ages from 7 to 13 years.
Table 1 Associations (HR and 95% CI) between childhood BMI z-score and incident hospital admissions for asthma (n=1,813) in early adulthood (between age 20 and 45 years) among individuals in the Copenhagen School Health Records Register (n=310,211)
Change in BMI during school age and risk for AA in early adulthood
The risk of incident AA was higher for girls who gained weight from 7 to 13 years of age, i.e., those with an increase in their BMI z-score from interquartile range to the upper quartile (HR 1.28, 95% CI 1.10–1.50), than for girls with a stable weight (HR 1.06, 95% CI 0.90–1.24). The risk of AA until age 45 years was similar in boys whose body weight increased during these years (HR 1.09, 95% CI 0.90–1.34) and those who had a stable weight (HR 1.10, 95% CI 0.90–1.34).
Discussion
In this very large, population-based cohort study of 310,211 children, we found non-linear associations between childhood BMI and AA in early adulthood. Higher childhood BMI increases the risk for hospital admission for asthma in early adulthood for females, whereas for males low BMI values in childhood were associated with a higher risk of AA in early adulthood. Our study has therefore revealed important differences between males and females with regard to the association between childhood BMI and risk for more severe asthma in adulthood.
The very large cohort studied provided us with the statistical power to investigate the effects of childhood BMI separately by sex. We observed an association between high BMI in childhood and subsequent risk of more severe asthma in females, which is in line with previous, albeit much smaller cohorts with shorter observation periods, studies of children and adolescents.Citation11,Citation12,Citation27–Citation29 Furthermore, Ho et alCitation30 reported from a cross-sectional study of approximately 4,000 individuals aged 13–15 years that overweight girls had higher odds ratio for physician-diagnosed asthma compared with normal weight participants. Among males we observed that low BMI increased the risk of hospital admissions for asthma. This contrasts with the findings of Ho et al in which they did not find any significant associations between BMI and asthma in boys at ages 13–15 years. These results are consistent with those from a Norwegian study of 2,300 adolescents that also did not detect associations.Citation29 Therefore, in contrast with previously published studies, our study revealed a novel finding of an association between having a low BMI in childhood and risk for AA in early adulthood among males. Furthermore, Chen et alCitation31 published a systematic review and meta-analysis addressing sex differences in childhood overweight/obesity in predicting the risk of incident asthma. They reported from their review of six studies fulfilling the inclusion criteria that obese boys had a higher risk of asthma compared with obese girls; however, they included only pediatric studies of individuals from 5 to 18 years of age that examined incident asthma in childhood. After puberty, incident asthma is more common in females than in males,Citation32 which is in line with our findings (), whereas in childhood the incidence of allergic asthma is much higher in boys than in girls.Citation32
Additionally, we investigated how change in body size from the ages of 7 to 13 years is associated with AAs. For females, we found that girls with a normal BMI at the age of 7 years that increased to a high one at the age of 13 years had a significantly increased risk of AAs. We defined “high” as the 75th percentile or more as we chose to focus on the effects at the upper end of the distribution rather than on extremely heavy girls. In boys, we did not detect significant effects of increasing BMI from ages 7 to 13 years. Our findings are consistent with those from the Tucson Children’s Respiratory Study in which Castro-Rodríquez et alCitation28 reported that girls who became overweight or obese between 6 and 11 years of age were more likely to develop asthma symptoms than those with stable BMI, but this relationship was not seen in boys.
It is well known that late-onset asthma is generally more severe and difficult to control than early-onset asthma, especially compared to allergic asthma.Citation33 The low BMI-AA association observed in males, in contrast with our observations in females, in the present study might be due to differences in adipokine levels between males and females, including serum leptin, as an adipokine imbalance is associated with both pro-inflammatory status and asthma.Citation34 Differences in leptin levels are possibly triggered by different performances of the leptin gene caused by differences in diet and exercise habits between males and females.Citation3,Citation35,Citation36 On the other hand, apart from differences in levels of obesity-related inflammatory markers between males and females, the observed association between high childhood BMI and AA in adulthood observed in girls might be explained by higher estrogen levels in obese compared with normal weight females.Citation3,Citation37,Citation38 However, there might also be a more simple explanation for the observed differences between males and females caused by differences in smoking rates, as the smoking rate is higher for females than for males in Denmark, especially in the younger age groups. It is well known that adiposity tracks from childhood into adulthood, so young adult females may take up or continue smoking because they believe in a weight reduction effect, and by that increase their risk of episodes of uncontrolled asthma leading to hospital admission, as tobacco exposure has substantial negative impact on asthma control.Citation39 On the contrary, the risk of poor asthma control in thin young males may also be related to smoking as it may be seen as having positive impact on self-confidence.
Strengths and limitations
Our study takes advantage of being based on a very large cohort. The CSHR register includes virtually all schoolchildren in Copenhagen from 1930 to 1989, where mandatory health examinations were performed at all public and private schools, and thus selection bias due to socioeconomic status is eliminated from the present study. Furthermore, due to the unique identification number for each individual and the effectiveness of the DNPR, complete follow-up was available for eligible individuals. In the present study, we have only analyzed hospital admissions for asthma, and by that more severe asthma. It may, therefore, be argued that our findings do not necessarily apply to the asthmatic population in general. However, it has previously been shown in a Danish study that episodes of poor asthma control, including hospital admissions, are seen in as many as 25% of patients classified as having mild to moderate asthma, defined according to level of treatment;Citation40 furthermore, in a country with free access to healthcare, many admissions for asthma are caused by low adherence with controller therapy,Citation41 primarily inhaled corticosteroids, and lack of recognition of need for controller therapy by both patients and doctors. Furthermore, the remission rate of asthma is very low in individuals aged 20 years and older, in contrast to asthma earlier in life; so by using this cutoff point in the present study, we have most likely primarily identified individuals with life-long asthma.Citation42,Citation43
Perspectives
As the prevalence and severity of asthma in young adults are increasing, the associations that we identified with childhood body size are of great importance. Our findings are based upon children born during different phases of the obesity epidemic. In all years, the prevalence of childhood overweight and obesity is much lower than what is observed in contemporary populations where approximately 30% of children in economically developed countries are classified as overweight or obese. Noteworthy is our finding among females that the risk of AAs begins to increase at BMI levels that are far lower than international definitions of childhood overweight and obesity. Our results suggest that the current obesity epidemic will make a significant contribution to AAs in young females. By contrast, we found that low BMI values increased the risk of admissions in males. We speculate that low BMI may be a marker of illness or other disease processes, and it highlights the importance of screening for underweight individuals in this era where there is large focus on excess weight.
Conclusion
The present long-term study of 310,211 schoolchildren showed that the association between childhood BMI and incident AA in early adulthood is non-linear for both males and females; importantly, our study also revealed that having a high BMI in childhood is associated with a higher risk of incident hospital admission for asthma in early adulthood in females, whereas having a low BMI in childhood increases this risk in males. Our findings may, therefore, offer guidance for measures aiming at reducing the future burden of severe asthma.
Acknowledgments
The abstract of this paper was presented at the annual meeting of the European Respiratory Society as a conference talk with interim findings. The abstract was published in the European Respiratory Journal; 2016;(suppl 60):OA 3315.
Disclosure
The authors report no conflicts of interest in this work.
References
- CamargoCAJrWeissSTZhangSWillettWCSpeizerFEProspective study of body mass index, weight change, and risk of adult-onset asthma in womenArch Intern Med1999159212582258810573048
- BybergKKEideGEFormanMRJúlíussonPBØymarKBody mass index and physical activity in early childhood are associated with atopic sensitization, atopic dermatitis and asthma in later childhoodClin Transl Allergy2016613327559467
- AliZUlrikCSObesity and asthma: a coincidence or a causal relationship? A systematic reviewRespir Med201310791287130023642708
- SilveiraDHZhangLPrietschSOVecchiAASusinLRNutritional status, adiposity and asthma severity and control in childrenJ Paediatr Child Health201551101001100625872953
- JuelCTUlrikCSObesity and asthma: impact on severity, asthma control, and response to therapyRespir Care201358586787323258582
- DixonAEHolguinFSoodAAmerican Thoracic Society Ad Hoc Subcommittee on Obesity and Lung DiseaseAn official American Thoracic Society Workshop report: obesity and asthmaProc Am Thorac Soc20107532533520844291
- CamargoCAJrBouletLPSutherlandERBody mass index and response to asthma therapy: fluticasone propionate/salmeterol versus montelukastJ Asthma2010471768220100025
- ZiyabAHKarmausWKurukulaaratchyRJZhangHArshadSHDevelopmental trajectories of Body Mass Index from infancy to 18 years of age: prenatal determinants and health consequencesJ Epidemiol Community Health2014681093494124895184
- EganKBEttingerASDeWanATHolfordTRHolmenTLBrackenMBLongitudinal associations between asthma and general and abdominal weight status among Norwegian adolescents and young adults: the HUNT studyPediatr Obes201510534535225405952
- MaltzLMatzELGordish-DressmanHSex differences in the association between neck circumference and asthmaPediatr Pulmonol201651989390026774073
- BenedettiFJBosaVLGiestaJMFischerGBAnthropometric indicators of general and central obesity in the prediction of asthma in adolescents; central obesity in asthmaNutr Hosp20153262540254826667701
- LuKDBillimekJBar-YosephRRadom-AizikSCooperDMAnton-CulverHSex differences in the relationship between fitness and obesity on risk for asthma in adolescentsJ Pediatr2016176364227318375
- ChenYCHuangYLHoWCWangYCYuYHGender differences in effects of obesity and asthma on adolescent lung function: results from a population-based studyJ Asthma201754327928527435689
- SchatzMZeigerRSZhangFChenWYangSJCamargoCAJrOverweight/obesity and risk of seasonal asthma exacerbationsJ Allergy Clin Immunol Pract20131661862224565709
- SchatzMZeigerRSYangSJProspective study on the relationship of obesity to asthma impairment and riskJ Allergy Clin Immunol Pract201534560565.e125975622
- TayTRRadhakrishnaNHore-LacyFComorbidities in difficult asthma are independent risk factors for frequent exacerbations, poor control and diminished quality of lifeRespirology20162181384139027363539
- GibsonPGMcDonaldVMMarksGBAsthma in older adultsLancet2010376974380381320816547
- PorsbjergCLangePUlrikCSLung function impairment increases with age of diagnosis in adult onset asthmaRespir Med2015109782182725962648
- UlrikCSOutcome of asthma: longitudinal changes in lung functionEur Respir J199913490491810362061
- HaldarPPavordIDShawDECluster analysis and clinical asthma phenotypesAm J Respir Crit Care Med2008178321822418480428
- (GINA) GIfAAsthma, COPD and the asthma-COPD overlap syndrome (ACOS)2014Accessed April 22, 2018
- HeymsfieldSBWaddenTAMechanisms, pathophysiology, and management of obesityN Engl J Med2017376325426628099824
- BakerJLOlsenLWAndersenIPearsonSHansenBSørensenTCohort profile: the Copenhagen School Health Records RegisterInt J Epidemiol200938365666218719090
- ColeTJGreenPJSmoothing reference centile curves: the LMS method and penalized likelihoodStat Med19921110130513191518992
- PedersenCBThe Danish Civil Registration SystemScand J Public Health201139Suppl 7222521775345
- LyngeESandegaardJLReboljMThe Danish National Patient RegisterScand J Public Health201139Suppl 7303321775347
- GoldDRDamokoshAIDockeryDWBerkeyCSBody-mass index as a predictor of incident asthma in a prospective cohort of childrenPediatr Pulmonol200336651452114618644
- Castro-RodríguezJAHolbergCJMorganWJWrightALMartinezFDIncreased incidence of asthmalike symptoms in girls who become overweight or obese during the school yearsAm J Respir Crit Care Med200116361344134911371399
- TollefsenELanghammerARomundstadPBjermerLJohnsenRHolmenTLFemale gender is associated with higher incidence and more stable respiratory symptoms during adolescenceRespir Med2007101589690217084607
- HoWCLinYSCaffreyJLHigher body mass index may induce asthma among adolescents with pre-asthmatic symptoms: a prospective cohort studyBMC Public Health20111154221740558
- ChenYCDongGHLinKCLeeYLGender difference of childhood overweight and obesity in predicting the risk of incident asthma: a systematic review and meta-analysisObes Rev201314322223123145849
- LeynaertBSunyerJGarcia-EstebanRGender differences in prevalence, diagnosis and incidence of allergic and non-allergic asthma: a population-based cohortThorax201267762563122334535
- Prevention GSfAMaGlobal Initiative for Asthma (GINA) Available from: www.ginasthma.org2015Accessed April 22, 2018
- MucMMota-PintoAPadezCAssociation between obesity and asthma – epidemiology, pathophysiology and clinical profileNutr Res Rev201629219420127514726
- GulerNKirerleriEOnesUTamayZSalmayenliNDarendelilerFLeptin: does it have any role in childhood asthma?J Allergy Clin Immunol2004114225425915316499
- ThomsenSFExploring the origins of asthma: lessons from twin studiesEur Clin Respir J20141Suppl 1142
- CareyMACardJWVoltzJWIt’s all about sex: gender, lung development and lung diseaseTrends Endocrinol Metab200718830831317764971
- CareyMACardJWVoltzJWGermolecDRKorachKSZeldinDCThe impact of sex and sex hormones on lung physiology and disease: lessons from animal studiesAm J Physiol Lung Cell Mol Physiol20072932L272L27817575008
- GrarupPAJannerJHUlrikCSPassive smoking is associated with poor asthma control during pregnancy: a prospective study of 500 pregnanciesPLoS One2014911e11243525409513
- von BülowAKriegbaumMBackerVPorsbjergCThe prevalence of severe asthma and low asthma control among Danish adultsJ Allergy Clin Immunol Pract20142675976725439368
- UlrikCSBackerVSøes-PetersenULangePHarvingHPlaschkePPThe patient’s perspective: adherence or non-adherence to asthma controller therapy?J Asthma200643970170417092852
- De MarcoRLocatelliFCerveriIBugianiMMarinoniAGiammancoGItalian Study on Asthma in Young Adults study groupIncidence and remission of asthma: a retrospective study on the natural history of asthma in ItalyJ Allergy Clin Immunol2002110222823512170262
- PesceGLocatelliFCerveriISeventy years of asthma in Italy: age, period and cohort effects on incidence and remission of self-reported asthma from 1940 to 2010PLoS One20151010e013857026439263