
Abstract
Background
Normal gastrointestinal (GI) mucosa on endoscopy has been linked to a lower risk of colorectal cancer (CRC) but its association to overall death is unknown.
Methods
We identified 466,987 individuals with a first GI biopsy 1965–2016 with normal mucosa (60.6% upper GI and 39.4% lower GI) through all Swedish pathology departments (n = 28). They were individually matched to 2,321,217 reference individuals without a GI biopsy and also compared to 505,076 full siblings. Flexible parametric models were applied to estimate hazard ratio (HRs) and 95% confidence interval (95% CI) for death.
Results
During a median follow-up of ~11 years, 85,859 (18.39%) of individuals with normal mucosa and 377,653 (16.27%) of reference individuals died. This corresponded to incidence rates of 147.56/10,000 vs 127.90/10,000 person-years respectively (rate difference: 19.66/10,000 person-years), with the multivariable-adjusted HR of 1.21 (95% CI: 1.20–1.22). Excess mortality was seen for both upper and lower biopsy with normal mucosa. Particularly higher HRs for death were seen in males, individuals biopsied when aged <40 years, those without a prior record of GI disease, and those with high education. Mortality risk was most increased in the first five years after biopsy (HR = 1.34; 95% CI: 1.32–1.36) but decreased thereafter. Having a GI biopsy with normal mucosa was associated with excess mortality from cardiovascular (CVD)disease (HR = 1.02; 95% CI: 1.01–1.03), cancer (HR = 1.58; 95% CI: 1.56–1.61), GI disease (HR = 1.65; 95% CI: 1.58–1.71), and other causes (HR = 1.10; 95% CI: 1.08–1.11). Sibling comparisons yielded similar results.
Conclusion
Compared with individuals without a GI biopsy, those with a normal GI biopsy due to clinical symptoms had a higher mortality particularly in the first five years after biopsy, and especially from GI disease and cancer.
Keywords:
Introduction
In 2018, about 0.6% of the Swedish population underwent an upper gastrointestinal (GI) endoscopy as outpatients,Citation1 while 0.7% had a lower endoscopy (colonoscopy).Citation1 In Sweden, >1% of the population have an endoscopy every year, with a larger percentage in ages where colorectal cancer (CRC) is common, for example, 2–3% of those aged 60–70 years.Citation1 The most common finding on endoscopy is normal mucosa (i.e., normal histological feature),Citation2 but data on the long-term prognosis of these individuals are largely missing.
With the introduction of more active screening guidelines around the world (already today, American guidelines stipulates CRC screening for average-risk adults aged 45–75 yearsCitation3), more and more people will be informed that their endoscopy was normal. For almost all GI diseases, there are guidelinesCitation4–9 for follow-up and an extensive knowledge of their prognosis, but apart from recommendations on follow-up with regards to CRC riskCitation10 (and appending data on CRC risk in patients with normal mucosa),Citation11 we are not aware of any guidelines for the follow-up of individuals with a GI biopsy showing normal mucosa, or any study exploring the risk of overall death in these individuals.
In this study, we followed up 466,987 individuals with a GI biopsy showing normal mucosa from 1965 to 2016, and calculated their absolute and relative risks of deaths, compared with matched reference individuals selected from the general population and their siblings.
Methods
Study Design and Participants
Between 2015 and 2017 we extracted histopathologic data from the ESPRESSO study (Epidemiology Strengthened by histoPathology Reports in Sweden).Citation12 That study is a compilation of GI biopsy reports from all 28 pathology departments in Sweden from 1965 to 2016.Citation12 Retrieved data included morphology codes (a Swedish version of the Systematized Nomenclature of Medicine (SNOMED) coding) and topography (where T60-T65 represented the upper GI tract and T66-T69 or T6X the lower part). We defined the exposed group as having a normal mucosa (SnoMed codes: M00100 and M00110). An earlier validation of 320 individuals (upper GI (T62-T65): n = 160; colorectal (T67-T68): n = 160) found a positive predictive value of >98% for normal mucosal histology.Citation13
For each individual with a first GI biopsy of normal mucosa, the government agency Statistics Sweden identified up to five reference individuals from the general populationCitation14 that matched on age, sex, county of residence, and calendar period. Reference individuals had not undergone any GI biopsy and were alive in Sweden at time of matching. The biopsy/selection date served as date of cohort entry for the exposed and the unexposed (reference individuals), respectively.
Follow-Up and Ascertainment of Death
Through the unique personal identity numberCitation15 assigned to all residents in Sweden, study participants were linked to the Swedish national health registers as well as the Total Population RegisterCitation14 allowing for a virtually complete follow-up from date of cohort entry to emigration, death, or December 31 2017, whichever occurred first.
Date of death was retrieved from the Swedish Total Population Register,Citation14 while cause of death was ascertained through the Swedish Cause of Death register.Citation16 Secondary outcomes consisted of cause-specific death: cardiovascular (CVD), cancer, GI disease, and other cause of mortality (ICD codes in Supplementary Table 1).
Covariates
The following five covariates were considered in our models: (I). country of birth (Nordic vs other country); (II). educational attainment (four categories: 0–9 years, 10–12 years, ≥13 years, and “missing”), retrieved from the Swedish LISA database;Citation17 (III). number of health care visits between 2 years and 6 months prior to biopsy/selection date (four categories: 0, 1, 2–3, and ≥4), as a proxy for general health status, and health care visits between 6 months and until the biopsy/selection date was not considered to avoid over-adjustment; (IV). the Charlson comorbidity index up until the biopsy/selection date (three categories: 0, 1, and ≥2; without considering peptic ulcer disease), as a proxy for general health status.Citation18 Finally, we included history of GI disease prior to biopsy/selection date (yes vs no), as such disease may lead to endoscopy and in many diseases endoscopic remission is an important aim of GI disease managementCitation5 (ICD codes in Supplementary Table 1).
Statistical Analysis
We used flexible parametric model with 5 degrees of freedom for baseline effects and 4 degrees of freedom for the time-dependent effect to estimate the average hazard ratio ([HR] together with 95% confidence interval [CI]) and the temporal pattern of HR of mortality since biopsy.Citation19 This approach is similar to the Cox proportional hazards model but allows the effect of a covariate vary over time rather than just assuming a constant hazard.
We firstly adjusted for the matching variables (birth year, sex, county of residence, and calendar period) in model 1, then additionally adjusted for country of birth, educational attainment, number of health care visits, Charlson comorbidity index, and history of GI disease in model 2. We carried out a number of subgroup analyses, stratified for sex, age at cohort entry (<18 y, 18-<40 y, 40-<60 y, and ≥60 y), biopsy location (upper vs lower GI tract), start year of follow-up (1965–1989, 1990–1999, 2000–2009, and 2010–2016), educational attainment, and history of GI disease. As very few children (<18 years) died from CVD or GI disease, we combined <18 y and 18–40 y into one group when investigating those two outcomes.
Sensitivity Analyses
Since comorbidity and health care utilization have a substantial effect on both endoscopy use and mortality rates, we carried out several sensitivity analyses restricted to: (I). individuals with a Charlson comorbidity index of zero; (II). individuals with a number of prior health care visit of zero; (III). individuals without a record of endoscopy before cohort entry (for relevant codes, see Supplementary Table 2); (IV). individuals free of colectomy or proctocolectomy before cohort entry (for relevant codes, see Supplementary Table 2); (V) individuals free of GI diseases or cancers before six months after biopsy (for relevant ICD-codes, see Supplementary Table 1); (VI) excluding deaths in the first week after biopsy to minimize the influence of post-endoscopy complications on our risk estimates.Citation20 Furthermore, as one individual might have undergone multiple GI biopsies with different results during follow-up, we additionally considered GI biopsy result as a time-varying exposure in the model.
Finally, although we considered a range of possible confounders in model 2, all observational studies may suffer from residual confounding. To further reduce this, we compared individuals with normal mucosa with their siblings, which can adjust for shared genetic and early environmental factors as well as health care seeking behavior (leading up to a GI biopsy). Siblings were identified through the multi-generation part of the Total Population Register.Citation14 We requested that siblings were alive and free of an earlier GI biopsy on the biopsy date of the index siblings.
Data analyses were performed using SAS version 9.4 (SAS Institute Inc, Cary, NC), Stata (version 15.0; StataCorp LP, College Station, TX), and R version 3.6.0.Citation21 A two-sided P ≤ 0.05 was considered statistically significant.
Patient Involvement
There was no patient involvement in the planning or writing up of this study, but a representative of the Swedish patient society for GI disease served as a contact person for the overall ESPRESSO study.
Ethics and Data Availability
This study was approved by the Ethical Review Board in Stockholm (DNR: 2014/1287-31/4). Given its register-based nature, the need of individual informed consent was waived.Citation22 Due to legal and ethical reasons, the data cannot be shared. The data accessed complied with relevant data protection and privacy regulations.
Results
We identified 466,987 individuals with a GI biopsy with normal mucosa (: 60.62% upper GI and 39.38% lower GI on first biopsy).
Table 1 Characteristics of Individuals with a GI Biopsy Result of Normal Mucosa and Their Matched References, a Nationwide Matched Cohort Study in Sweden, 1965–2016
Individuals with normal mucosa were matched to 2,321,217 reference individuals. Median age at biopsy was 43.9 years with 8.68% undergoing biopsy in childhood (n = 40,551). Around 62% were female and 90% born in the Nordic countries. Around 38% of biopsied individuals and 26% of reference individuals had at least one health care visit between 2 years and 6 months prior to the date of cohort entry. Individuals undergoing a biopsy with normal mucosa had a higher frequency of Charlson comorbidity index ≥1 (24%, vs 15%) and GI disease (47% vs 15%), but very few individuals in either group had a record of earlier GI cancer (0.58% vs 0.13%). Educational attainment was similar in the exposed and unexposed ().
Overall Death
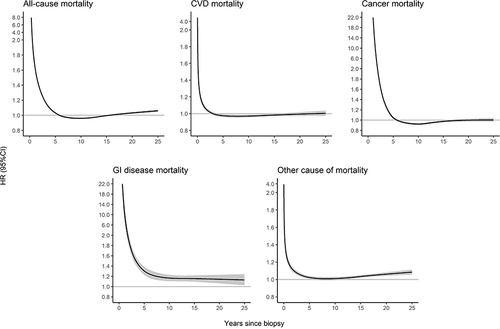
During a median follow-up of ~11 years, 85,859 (18.39%) of individuals with normal mucosa and 377,653 (16.27%) of reference individuals died (). This corresponded to incidence rates of 147.56 vs 127.90 per 10,000 person-years, respectively (rate difference 19.66/10,000 per person-years) and an HR of 1.38 (95% CI = 1.37–1.39) (, model 1). After additionally adjusting for potential confounders, the overall HR decreased to 1.21 (95% CI: 1.20–1.22) (, model 2). Mortality risk was most increased in the first five years after biopsy (HR=1.34; 95% CI: 1.32–1.36) and decreased thereafter (HR = 1.03; 95% CI: 1.02–1.05) (, Supplementary Table 3, Supplementary Table 4). In the temporal pattern of HR and 95% CI, the risk of overall death rapidly decreased to just below one around 10 years, but then increased and exceeded one at around 18 years after biopsy ().
Table 2 Mortality in Individuals with a GI Biopsy Result of Normal Mucosa and Their Matched References
Figure 1 The HR and 95% CI of all-cause and cause-specific mortality as a function of time since biopsy, comparing individuals with a GI biopsy result of normal mucosa with their matched references. Estimated by the flexible parametric model that conditioned on matching set (birth year, gender, county of residence, and calendar period) and further adjusted for country of birth, educational attainment, number of health care visits, Charlson comorbidity index, and history of GI diseases.
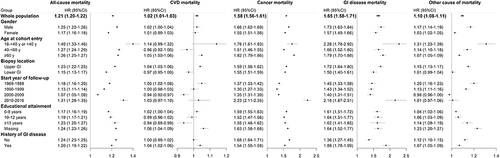
Stratified analyses showed a stronger association in males (HR = 1.25; 95% CI: 1.23–1.26) than females (HR = 1.17; 95% CI: 1.16–1.18), and for upper GI biopsy (HR = 1.23; 95% CI: 1.22–1.25) than lower GI biopsy (HR = 1.15; 95% CI: 1.13–1.17) (). The association was also stronger for biopsy in childhood (HR = 2.38; 95% CI: 2.11–2.69) and 18-<40 years (HR = 1.40; 95% CI: 1.33–1.46), compared with thereafter, and among individuals without a prior record of GI disease (HR = 1.24; 95% CI: 1.23–1.25), and individuals with an education ≥13 years (HR = 1.24; 95% CI: 1.23–1.26), compared with others. Finally, the association was strongest in the latest calendar period 2010–2016 (HR = 1.31; 95% CI: 1.28–1.35), compared with earlier calendar periods (). We observed similar temporal pattern of HR in stratified analyses (Supplementary Figure 1) and similar result of normal mucosa with risk of all-cause mortality among those underwent upper or lower GI biopsy (Supplementary Figure 2).
Figure 2 Subgroup analyses of the associations between normal mucosa and risk of mortality. Individuals biopsied in childhood (age at cohort entry<18 y) demonstrated a much higher risk for all-cause mortality (HR = 2.38; 95% CI: 2.11–2.69), cancer mortality (HR = 2.92; 95% CI: 2.11–4.05) and other cause of mortality (HR = 2.23; 95% CI: 1.95–2.56). Estimated by the flexible parametric model that conditioned on matching set (birth year, gender, county of residence, and calendar period) and further adjusted for country of birth, educational attainment, number of health care visits, Charlson comorbidity index, and history of GI diseases.
Cause-Specific Death
Having a GI biopsy with normal mucosa was associated with excess mortality for all secondary outcomes: CVD (HR = 1.02; 95% CI: 1.01–1.03), cancer (HR = 1.58; 95% CI: 1.56–1.61), GI disease (HR = 1.65; 95% CI: 1.58–1.71), and other cause of mortality (HR = 1.10; 95% CI: 1.08–1.11) ( and ). Individuals with normal GI mucosa were at increased risk of GI disease mortality and other cause of mortality until 25 years since biopsy, but not at increased risk of CVD or cancer mortality after around 5 years since biopsy (, Supplementary Table 3, and Supplementary Table 4).
Sibling Analyses and Sensitivity Analyses
We identified 273,681 individuals with a GI biopsy with normal mucosa and ≥1 sibling alive at time of biopsy (n = 505,076). Supplementary Table 5 outlined the characteristics of siblings.
Sibling analyses were adjusted for the same covariates as the main analyses, and showed similar results for overall mortality (model 2: HR = 1.34; 95% CI: 1.31–1.37) and for cause-specific death: CVD (HR = 1.07; 95% CI: 1.02–1.11), cancer (HR = 1.58; 95% CI: 1.53–1.63), GI disease (HR = 1.75; 95% CI: 1.59–1.92), and other cause of mortality (HR = 1.23; 95% CI: 1.19–1.27) ().
Table 3 Mortality in Individuals with a GI Biopsy Result of Normal Mucosa and Their Siblings
In a series of sensitivity analyses, similar patterns for overall and cause-specific mortality were also observed (Supplementary Figure 3).
Discussion
The present study found a 21% increased risk of death in individuals with a GI biopsy of normal mucosa. This translates into one extra death per 10 years in 50 individuals with a normal mucosa at GI biopsy, with a much higher excess mortality in the first five years, which was mainly driven by GI disease and cancer. The increased risk persisted across the sensitivity analyses and also when we used siblings as comparators to decrease residual confounding. While the excess mortality decreased when we excluded individuals diagnosed with GI disease or cancer in the first 6 months after biopsy, individuals with normal mucosa remained at an increased risk of death.
A number of studies have explored the value of normal biopsy/endoscopy for the CRC risk and mortality.Citation11,Citation23–25 These studies show a protective effect of having a normal mucosa on CRC, and current screening recommendations suggest that individuals with a normal endoscopy can abstain from another colonoscopy for ten years.Citation26 The lower CRC mortality suggests that the increased cancer mortality seen among our study participants might have been due to other cancers. In other studies, we have shown that in individuals with celiac disease serology,Citation27 normal duodenal/jejunal mucosa is linked to future autism,Citation28 epilepsy,Citation29 and Chronic obstructive pulmonary disease (COPD).Citation30 Recently we also reported that a normal GI mucosa is associated with consequent amyotrophic lateral sclerosis.Citation13 For almost all GI diseases, there are guidelines for follow-up and an extensive knowledge of their prognosis (Supplementary Table 6), but until now, data on individuals with normal mucosa have been sparse.
The 21% increased mortality in in our study was almost identical to that seen in our earlier studies on microscopic colitis (HR = 1.17),Citation31 and celiac diseaseCitation32 (HR = 1.21; the HR decreased to 1.14 after adjustment for more confounders).Citation32 But mortality following a biopsy with normal mucosa seems to be lower than that in ulcerative colitis or Crohn’s disease (HRs of 1.66 and 1.74 respectively in two recent Nordic studiesCitation33,Citation34).
However, the increased mortality risk within the first five years after biopsy may have several implications. First, an active clinical approach may be motivated in this group of individuals, albeit with a normal GI histological feature. The high relative risks 0–5 years do stress the importance of informing individuals with normal mucosa that while certain diseases have been ruled out, this does not mean that they are healthy, and that they should seek health care again in case alarming symptoms appear even after a normal endoscopy. Second, it suggests that upper and lower endoscopy with a normal mucosa have little predictive value for future survival.
The temporal pattern with especially high HRs for GI disease death and cancer death in the 1–2 years after biopsy suggests that some of these individuals might have undergone endoscopy due to symptoms from other disorders. When Elfström et al examined the risk of incident GI cancer after biopsy, the risk was substantially increased in the first year after biopsy, in both patients with celiac disease (HR = 5.95) and those with normal mucosa but positive celiac serology (HR = 8.10); the risk was then normalized during 1-<5 years after biopsy (HR = 1.21 and 0.63 respectively).Citation35 Unfortunately, we did not have data on the indications for the GI biopsy, but of note the excess mortality risk in the first years after biopsy also persisted when we took pre-existing GI disease into consideration. Neither was the high initial mortality likely due to complications from the index endoscopy, since as suggested in a 2016 meta-analysis, mortality rates after colonoscopy are low (2.9 deaths per 100,000 colonoscopies).Citation20 The excess mortality risk vanished 5 years after biopsy, which might be a consequence of the depletion of susceptible individuals due to the premature finding for high-risk individuals in the first 5 years after biopsy.
The higher HR of death in children in relation to normal mucosa is consistent with several prognostic studies of childhood-onset GI diseases.Citation32–34 Excess risks in this age group are probably due to the fact that children without a GI biopsy very rarely die or suffer from any comorbidity. The same reasoning may explain the slightly higher HRs for death in those with education ≥13 years and in those without a prior record of GI disease, where the reference groups may be healthier than the reference groups of those only completing elementary school (≤9 years) and those with a prior record of GI disease. It is more difficult to explain the higher overall mortality risk in males. This contrasts with the slightly lower HRs for CRC death in males in our recent paper (HR = 0.59 in males, and 0.64 in females).Citation11
Strengths and Limitations
Our study had a number of strengths. Following up 466,987 individuals and >2.3 million general population controls yielded an unprecedented statistical power, which allowed us to explore informative subgroups. For instance we had access to mortality data in >40,000 unique individuals undergoing biopsy with normal mucosa in childhood, and were also able to demonstrate potential sex differences. The nationwide approach safeguards against selection bias and inflated data that are regularly seen in studies restricted to tertiary centers. Moreover, our data on normal mucosa have a satisfactory positive predictive value (>98%).Citation13
The long follow-up with 54% individuals followed-up for >10 years allowed us to explore temporal patterns of mortality risk. This demonstrated strikingly high HRs in the first few years, followed by null results from 5 years after biopsy, and potentially a slightly increased risk again 18 years after biopsy. This has implications for the follow-up of individuals with normal mucosa in the clinics. While our earlier research suggests a protective effect against death from CRC,Citation11 physicians should be aware of the slightly higher risk of other causes of death in individuals undergoing endoscopy even in the absence of mucosal abnormalities on GI biopsy.
Even more importantly, we were able to confirm our results from the general population analysis in a large-scale sibling comparison. This and the consistent results in a range of sensitivity analyses argues against that our findings would be random.
Lack of data on indications for biopsy is a major limitation. While the Stockholm region started organized CRC screening in 2008 for asymptomatic average-risk individuals aged 60–69 years (through fecal occult blood test or fecal immunochemical test), even in 2013 only 63% of Swedes in the recommended age groups underwent CRC screening.Citation36 However, few of the individuals with a GI biopsy in our study were likely to have been asymptomatic, the normal mucosa findings in the present study, therefore, do not likely represent screening-detected normal mucosa. But where screening constituted a reason for endoscopy, this will have taken place in the colorectum, and it is possible that a larger proportion of true screening contributed to the lower HRs in lower as opposed to upper GI normal mucosa (1.15 vs 1.23).
While we adjusted for GI disease, and adjusted for Charlson comorbidity index and number of health care visits before biopsy, we cannot rule out that residual disease has contributed to the excess mortality. This said, HRs were similarly increased also in the sibling comparison where eg health-seeking pattern and genetic factors should have been better adjusted for. Still we acknowledge the risk of residual confounding. Should smoking, obesity, and degree of physical exercise be associated with chance of undergoing endoscopy and having a normal mucosa, that might have influenced our findings. We also had no information on endoscopic quality.
In conclusion, we found an increased risk of death in individuals with a GI biopsy with normal mucosa, especially from GI disease and cancer. The risk estimates were on par with that of, e.g., microscopic colitis and celiac disease, but had a very specific temporal pattern, with a higher mortality risk in the first five years after biopsy.
Abbreviations
CI, confidence interval; CRC, colorectal cancer; ESPRESSO, Epidemiology Strengthened by histoPathology Reports in Sweden; GI, gastrointestinal; HR, hazard ratio; IBD, inflammatory bowel disease; ICD, International Classification of Diseases; SD, standard deviation; SNOMED, Systematized Nomenclature of Medicine.
Ethical Approval
This study was approved by the Stockholm Ethics Review Board (2014/1287-31/4).
Role of the Sponsor
The funders had no role in design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review, or approval of the manuscript; and the decision to submit the manuscript for publication.
Disclosure
All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare:
JFL coordinates a study on behalf of the Swedish IBD quality register (SWIBREG) and that study has received funding from Janssen corporation.
OO has been a PI on projects at Karolinska Institutet, partly financed by investigator-initiated grants from Janssen and Ferring, and Karolinska Institutet; he has received fees for lectures and participation on advisory boards from Janssen, Ferring, Takeda, and Pfizer. OO also reports a grant from Pfizer in the context of a national safety monitoring program.
JH served as speaker and/or advisory board member for AbbVie, Celgene, Celltrion, Dr Falk Pharma and the Falk Foundation, Ferring, Galapagos, Gilead, Hospira, Index Pharma, Janssen, MEDA, Medivir, MSD, Novartis, Pfizer, Prometheus Laboratories Inc., Sandoz, Shire, Takeda, Thermo Fisher Scientific, Tillotts Pharma, Vifor Pharma, UCB and received grant support from Janssen, MSD and Takeda.
HK is supported by the American College of Gastroenterology Senior Research Award and the Beker Foundation; HK has received consulting fees from Abbvie and Takeda; HK has also received grant funding from Pfizer and Takeda.
The other authors report no conflict of interest.
Additional information
Funding
References
- Socialstyrelsen. Statistikdatabas för operationer i specialiserad öppen vård (dagkirurgi) (by the Swedish National Board of Health and Welfare) 2020. Available from: https://sdb.socialstyrelsen.se/if_dagk/resultat.aspx. Accessed July 11, 2022.
- Bowles CJ, Leicester R, Romaya C, et al. A prospective study of colonoscopy practice in the UK today: are we adequately prepared for national colorectal cancer screening tomorrow? Gut. 2004;53(2):277–283. doi:10.1136/gut.2003.016436
- Force USPST, Davidson KW, Barry MJ, et al. Screening for Colorectal Cancer: US Preventive Services Task Force Recommendation Statement. JAMA. 2021;325(19):1965–1977. doi:10.1001/jama.2021.6238
- Banks M, Graham D, Jansen M, et al. British Society of Gastroenterology guidelines on the diagnosis and management of patients at risk of gastric adenocarcinoma. Gut. 2019;68(9):1545–1575. doi:10.1136/gutjnl-2018-318126
- Ludvigsson JF, Bai JC, Biagi F, et al. Diagnosis and management of adult coeliac disease: guidelines from the British Society of Gastroenterology. Gut. 2014;63(8):1210–1228. doi:10.1136/gutjnl-2013-306578
- Tursi A, Brandimarte G, Di Mario F, et al. International Consensus on Diverticulosis and Diverticular Disease. Statements from the 3rd International Symposium on Diverticular Disease. J Gastrointestin Liver Dis. 2020;28:57–66. doi:10.15403/jgld-562
- Lieberman DA, Rex DK, Winawer SJ, et al. Guidelines for colonoscopy surveillance after screening and polypectomy: a consensus update by the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2012;143(3):844–857. doi:10.1053/j.gastro.2012.06.001
- Hassan C, Wysocki PT, Fuccio L, et al. Endoscopic surveillance after surgical or endoscopic resection for colorectal cancer: European Society of Gastrointestinal Endoscopy (ESGE) and European Society of Digestive Oncology (ESDO) Guideline. Endoscopy. 2019;51(3):266–277. doi:10.1055/a-0831-2522
- Pardi DS, Tremaine WJ, Carrasco-Labra A. American Gastroenterological Association Institute Technical Review on the Medical Management of Microscopic Colitis. Gastroenterology. 2016;150(1):247–74 e11. doi:10.1053/j.gastro.2015.11.006
- Rex DK, Boland CR, Dominitz JA, et al. Colorectal Cancer Screening: recommendations for Physicians and Patients From the U.S. Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2017;153(1):307–323. doi:10.1053/j.gastro.2017.05.013
- Song M, Emilsson L, Hultcrantz R, et al. Long-Term Incidence and Mortality of Colorectal Cancer After Endoscopic Biopsy With Normal Mucosa: a Swedish-Matched Cohort Study. Am J Gastroenterol. 2020. doi:10.14309/ajg.0000000000001018
- Ludvigsson JF, Lashkariani M. Cohort profile: ESPRESSO (Epidemiology Strengthened by histoPathology Reports in Sweden). Clin Epidemiol. 2019;11:101–114. doi:10.2147/CLEP.S191914
- Sun J, Ludvigsson JF, Roelstraete B, et al. Gastrointestinal biopsies and amyotrophic lateral sclerosis - results from a cohort study of 1.1 million individuals. Amyotroph Lateral Scler Frontotemporal Degener. 2021;22(5–6):410–418. doi:10.1080/21678421.2021.1883666
- Ludvigsson JF, Almqvist C, Bonamy AE, et al. Registers of the Swedish total population and their use in medical research. Eur J Epidemiol. 2016;31(2):125–136. doi:10.1007/s10654-016-0117-y
- Ludvigsson JF, Otterblad-Olausson P, Pettersson BU, et al. The Swedish personal identity number: possibilities and pitfalls in healthcare and medical research. Eur J Epidemiol. 2009;24(11):659–667. doi:10.1007/s10654-009-9350-y
- Brooke HL, Talback M, Hornblad J, et al. The Swedish cause of death register. Eur J Epidemiol. 2017;32(9):765–773. doi:10.1007/s10654-017-0316-1
- Ludvigsson JF, Svedberg P, Olen O, et al. The longitudinal integrated database for health insurance and labour market studies (LISA) and its use in medical research. Eur J Epidemiol. 2019;34(4):423–437. doi:10.1007/s10654-019-00511-8
- Ludvigsson JF, Appelros P, Askling J, et al. Adaptation of the Charlson Comorbidity Index for Register-Based Research in Sweden. Clin Epidemiol. 2021;13:21–41. doi:10.2147/CLEP.S282475
- Lambert PC, Royston P. Further development of flexible parametric models for survival analysis. Stata J. 2009;9(2):265–290. doi:10.1177/1536867x0900900206
- Reumkens A, Rondagh EJ, Bakker CM, et al. Post-Colonoscopy Complications: a Systematic Review, Time Trends, and Meta-Analysis of Population-Based Studies. Am J Gastroenterol. 2016;111(8):1092–1101. doi:10.1038/ajg.2016.234
- R Core Team. R: a language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria; 2020. Available from: https://www.R-project.org/. Accessed July 11, 2022.
- Ludvigsson JF, Haberg SE, Knudsen GP, et al. Ethical aspects of registry-based research in the Nordic countries. Clin Epidemiol. 2015;7:491–508. doi:10.2147/CLEP.S90589
- Lee JK, Jensen CD, Levin TR, et al. Long-term Risk of Colorectal Cancer and Related Deaths After a Colonoscopy With Normal Findings. JAMA Intern Med. 2019;179(2):153–160. doi:10.1001/jamainternmed.2018.5565
- Pilonis ND, Bugajski M, Wieszczy P, et al. Long-Term Colorectal Cancer Incidence and Mortality After a Single Negative Screening Colonoscopy. Ann Intern Med. 2020;173(2):81–91. doi:10.7326/M19-2477
- Thiis-Evensen E, Kalager M, Bretthauer M, et al. Long-term effectiveness of endoscopic screening on incidence and mortality of colorectal cancer: a randomized trial. United European Gastroenterol J. 2013;1(3):162–168. doi:10.1177/2050640613483290
- Gupta S, Lieberman D, Anderson JC, et al. Recommendations for Follow-Up After Colonoscopy and Polypectomy: a Consensus Update by the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2020;158(4):1131–53 e5. doi:10.1053/j.gastro.2019.10.026
- Ludvigsson JF, Brandt L, Montgomery SM. Symptoms and signs in individuals with serology positive for celiac disease but normal mucosa. BMC Gastroenterol. 2009;9:57.
- Ludvigsson JF, Reichenberg A, Hultman CM, et al. A nationwide study of the association between celiac disease and the risk of autistic spectrum disorders. JAMA Psychiatry. 2013;70(11):1224–1230. doi:10.1001/jamapsychiatry.2013.2048
- Ludvigsson JF, Zingone F, Tomson T, et al. Increased risk of epilepsy in biopsy-verified celiac disease: a population-based cohort study. Neurology. 2012;78(18):1401–1407. doi:10.1212/WNL.0b013e3182544728
- Ludvigsson JF, Inghammar M, Ekberg M, et al. A nationwide cohort study of the risk of chronic obstructive pulmonary disease in coeliac disease. J Intern Med. 2012;271(5):481–489. doi:10.1111/j.1365-2796.2011.02448.x
- Khalili H, Bergman D, Roelstraete B, et al. Mortality of Patients with Microscopic Colitis in Sweden. Clin Gastroenterol Hepatol. 2019. doi:10.1016/j.cgh.2019.12.012
- Lebwohl B, Green PHR, Soderling J, et al. Association Between Celiac Disease and Mortality Risk in a Swedish Population. JAMA. 2020;323(13):1277–1285. doi:10.1001/jama.2020.1943
- Olen O, Erichsen R, Sachs MC, et al. Colorectal cancer in ulcerative colitis: a Scandinavian population-based cohort study. Lancet. 2020;395(10218):123–131. doi:10.1016/S0140-6736(19)
- Olen O, Erichsen R, Sachs MC, et al. Colorectal cancer in Crohn’s disease: a Scandinavian population-based cohort study. Lancet Gastroenterol Hepatol. 2020. doi:10.1016/S2468-1253(20
- Elfstrom P, Granath F, Ye W, et al. Low risk of gastrointestinal cancer among patients with celiac disease, inflammation, or latent celiac disease. Clin Gastroenterol Hepatol. 2012;10(1):30–36. doi:10.1016/j.cgh.2011.06.029
- Senore C, Basu P, Anttila A, et al. Performance of colorectal cancer screening in the European Union Member States: data from the second European screening report. Gut. 2019;68(7):1232–1244. doi:10.1136/gutjnl-2018-317293