
Abstract
Introduction
Type 2 diabetes mellitus (T2DM) is a leading cause of chronic kidney disease (CKD) globally. Both conditions substantially worsen patients’ prognosis. Current data on German in-hospital CKD cohorts are scarce. The multinational CaReMe study was initiated to evaluate the current epidemiology and healthcare burden of cardiovascular, renal and metabolic diseases. In this substudy, we share real-world data on CKD inpatients stratified for coexisting T2DM derived from a large German hospital network.
Methods
This study used administrative data of inpatient cases from 89 Helios hospitals from 01/01/2016 to 28/02/2022. Data were extracted from ICD-10-encoded discharge diagnoses and OPS-encoded procedures. The first case meeting a previously developed CKD definition (defined by ICD-10- and OPS-codes) was considered the index case for a particular patient. Subsequent hospitalizations were analysed for readmission statistics. Patient characteristics and pre-defined endpoints were stratified for T2DM at index case.
Results
In total, 48,011 patients with CKD were included in the present analysis (mean age ± standard deviation, 73.8 ± 13.1 years; female, 44%) of whom 47.9% had co-existing T2DM. Patients with T2DM were older (75 ± 10.6 vs 72.7 ± 14.9 years, p < 0.001), but gender distribution was similar to patients without T2DM. The burden of cardiovascular disease was increased in patients with T2DM, and index and follow-up in-hospital mortality rates were higher. Non-T2DM patients were characterised by more advanced CKD at baseline. Patients with T2DM had consistently higher readmission numbers for all events of interest, except for readmissions due to kidney failure/dialysis, which were more common in non-T2DM patients.
Conclusion
In this study, we present recent data on hospitalized patients with CKD in Germany. In this CKD cohort, nearly half had T2DM, which substantially affected cardiovascular disease burden, rehospitalization frequency and mortality. Interestingly, non-diabetic patients had more advanced underlying renal disease, which affected renal outcomes.
Graphical Abstract
Introduction
Chronic kidney disease (CKD) is a significant global health issue, with a prevalence of 9%–13%.Citation1–3 Associated mortality in patients with CKD is predominantly due to the increased cardiovascular risk.Citation1,Citation3,Citation4 Type 2 diabetes mellitus (T2DM) is a common cause of CKD. Through microvascular alterations, it leads to a specific form of glomerulopathy, known as diabetic kidney disease (DKD).Citation5 CKD prevalence in patients with T2DM varies across European countries,Citation6,Citation7 ranging from 15.4% to 41.5%.Citation8 DKD often progresses to kidney failure and is considered the leading cause of kidney failure worldwide.Citation9,Citation10 Co-existence of both T2DM and CKD significantly increases cardiovascular mortality.Citation5,Citation11 However, the true origin of CKD can only be reliably identified through kidney biopsy.Citation5,Citation12 Hence, for some patients with T2DM, a non-diabetic cause of the underlying CKD cannot be ruled out.Citation5 Non-diabetic kidney disease (NDKD) is a common cause of CKD, with hypertension being the most common non-diabetic cause.Citation1,Citation13,Citation14 Population-based studies have demonstrated NDKD patients to be at increased risk for long-term adverse cardiovascular and renal outcomes.Citation13,Citation15 However, when compared to CKD patients with coexisting diabetes, patients with NDKD tend to have lower event rates and more favourable outcomes.Citation16,Citation17 This is consistent with the DAPA-CKD trial, where patients with both CKD and T2DM consistently had higher event ratesCitation18,Citation19 for the primary outcome measure.
Few recent European population-based studies have yet examined the epidemiology, characteristics, and respective in-hospital outcomes of hospitalised CKD patients with and without coexisting T2DM.Citation20–23 The multinational CaReMe study was initiated to report on the current epidemiology and healthcare burden of cardiovascular, renal and metabolic diseases using healthcare data from 12 countries. In a recent CaReMe-CKD analysis, the prevalence of diabetes (including type 1 diabetes mellitus) was 38–39% among 2.4 million included patients.Citation2 Aim of the present study was an analysis and comparative characterisation of a German in-hospital cohort of the CaReMe-CKD study, stratified for coexisting T2DM, over a 5-year observational period. Patient characteristics, comorbidity burden and in-hospital outcomes were evaluated, highlighting differences between patients with and without T2DM.
Methods
Data Source
In this retrospective observational cohort study, we analysed administrative (claims) data from 89 hospitals in Germany’s Helios network – primary, secondary, tertiary care centres and specialty care centres – that included inpatient cases between 01/01/2016 and 02/28/2022. The study used the International Statistical Classification of Diseases and Related Health Problems (ICD-10-GM [German Modification]) codes to identify patients with CKD and relevant comorbidities at hospital discharge, and Operations and Procedures codes (OPS [German adaptation of the International Classification of the Procedures in Medicine of the World Health Organization, version 2017]) to identify in-hospital medical procedures from administrative data. In-hospital death was defined by the type of hospital discharge. Hospital categories were extracted from administrative data. Supplemental Table 1 provides detailed information on the ICD-10-GM and OPS codes used. Patients ≥18 years of age with complete inpatient treatment, meeting one of the following CKD definition criteria, were included:
Main discharge diagnosis of CKD
Main diagnosis of acute kidney injury with a secondary diagnosis of CKD
Any CKD-associated procedure indicating dialysis (according to OPS codes, Supplemental Table 1) with CKD as the main or secondary diagnosis at hospital discharge.
The index case was defined as the first case of each patient meeting the inclusion criteria. Patients with type 1 diabetes mellitus were excluded. The study did not differentiate between incident and prevalent CKD.
Study Variables
Baseline characteristics, including demographic and comorbidity information, were stratified for T2DM at the index case. In case of multiple codes for CKD stage, the most severe stage was considered. Kidney failure was defined as either CKD stage 5 or by ICD-10-GM/OPS codes indicating dialysis (Supplemental Table 1). Additionally, we calculated a modified Elixhauser comorbidity weighted score excluding the components “diabetes mellitus, complicated” and “diabetes mellitus, uncomplicated” to reduce confounding.Citation24,Citation25 Supplemental Table 2 describes ICD−10-GM codes used to calculate the Elixhauser comorbidity weighted score.
For longitudinal analysis of readmission events during the observational period, only the first readmission per endpoint for one particular patient was included. Patients with incident T2DM during follow-up (FU) were counted as non-diabetic and patients with incident type 1 diabetes mellitus were excluded for this analysis. Pre-defined readmission event rates (for definitions, see Supplemental Table 3) were compared between stratification groups.
Statistical Analysis
Administrative data were extracted from QlikView (QlikTech, Radnor, Pennsylvania, USA); all statistical analyses were performed within the R environment. No statistical comparison of baseline characteristics was performed as per STROBE guidelines for observational analyses.Citation26 Readmission events were analysed as follows:
As a time-to-first-event analysis (duration between the index case and the first occurrence of a given event). Median readmission time in days [25–75% quantiles] and P-values from negative-binomial regression adjusted for age are reported.
As a cumulative event rate (percentage of index patients readmitted with a given endpoint during the FU period). N (%), odds ratios (OR) [95% confidence interval, CI] and P-values from Fisher’s exact test are reported. ORs [95% CI] are displayed in a Forest plot.
As a cumulative event rate per 100 patient-years.
As a Cox regression analysis for selected endpoints (any readmission, readmission for kidney failure/dialysis, in-hospital mortality during FU, readmission for heart failure, readmission for kidney disease) adjusted for age, gender, T2DM status, Elixhauser comorbidity weighted score at baseline, hospital category (primary/secondary care centre, tertiary care centre, specialty care centre). FU was right censored at the date of in-hospital death if occurred during FU, except for the endpoint “in-hospital mortality”.
Ethical Considerations
Patient data were stored in a double-pseudonymised form. Data use was approved by the local ethics committee of the University of Leipzig (AZ 010/21-ek) and the Helios Kliniken GmbH data protection authority. Considering the retrospective analysis of double-pseudonymised administrative clinical routine data, individual informed consent was not obtained. The study followed the STROBE guidelines for observational analyses.
Results
In total, 89 hospitals contributed inpatient cases to the database (33.4% primary care/secondary care centres; 34.3% tertiary care centres; 32.3% specialty care centres). A total of 48,011 patients (female, 44%; mean age ± standard deviation, 73.8 ± 13.1 years) fulfilled the pre-defined CKD definition. Of these, 22,994 (47.9%) had co-existing T2DM at the time of index hospitalization. Patients with T2DM were older (72.7 ± 14.9 vs 75 ± 10.6 years) and had a higher burden of comorbidities, especially cardiovascular diseases (CVD). Hypertension (71.8%) and heart failure (46%) were the most common comorbidities in the overall cohort and within stratification groups (). In patients with CKD and T2DM, baseline prevalences of complications associated with T2DM were 16.4% for diabetic neuropathy, 3.6% for diabetic retinopathy and 1.5% for diabetic foot complications. The underlying CKD was more advanced in the non-T2DM group as indicated by the prevalence of CKD stage 5 (42.1% vs 32.8%) and kidney failure (52.7% vs 47.5%) as defined above. Prevalence of acute kidney injury (AKI) was higher in the T2DM group at index case (54% vs 59.1%). Total index case in-hospital mortality was 11.2%, with a higher proportion of renal deaths compared to cardiovascular deaths (7.1% vs 2.2%, for definition, see Supplemental Table 3) and a significant difference in all-cause in-hospital mortality between T2DM and non-T2DM patients (10.8% vs 11.7%). This was mainly caused by a between-group discrepancy in cardiovascular death rates (1.5% vs 2.2%; ).
Table 1 Baseline Characteristics of CKD Patients Stratified for Prevalent T2DM
Circa fifty percent of the total cohort (n = 24,046) was rehospitalized at least once during FU (). Median (25%–75%) time from discharge of the index case until the last observed readmission event was 331 (92–776) while the mean number (±standard deviation) of readmissions per patient was 3.08 ± 3.08. Time-to-event analyses revealed a median (25%–75%) time to first readmission (any readmission) of 76 (24–239) days with no significant difference within stratification for T2DM (non-T2DM vs T2DM: 76 [24–244] vs 76 [24–235] days; p = 0.175; ). shows plots of time-to-event analyses. There were no other significant differences in time-to-event analyses for individual readmission events except for the pre-defined endpoints “kidney disease” (non-T2DM vs T2DM: 111 [37–362] vs 136 [41–393.5]; p = 0.048; ) and “peripheral artery disease” (non-T2DM vs T2DM: 269 [84.5–644.2] vs 239 [86–573]; p = 0.038; ). The most common reason for hospital readmission was kidney failure/dialysis (18.8% in the overall cohort). This endpoint occurred more frequently in the non-T2DM group (20.0% vs 17.5%; OR [95% CI] 1.179 [1.125, 1.234]; p < 0.001). Patients with T2DM showed higher rehospitalization rates due to cardiovascular comorbidities (, ) as well as higher all-cause (non-T2DM vs T2DM: 9.7% vs 12.0%; OR [95% CI] 0.782 [0.738, 0.829]; p < 0.001), cardiovascular (2.4% vs 3.4%; OR [95% CI] 0.691 [0.619, 0.771]; p < 0.001) and renal (1.0% vs 1.5%, OR [95% CI] 0.671 [0.567, 0.793]; p < 0.001) in-hospital mortality during FU. Hyperkalaemia was more common in patients with T2DM during the FU period (12.2% vs 14.1%; OR [95% CI] 0.851 [0.806, 0.897]; p < 0.001). Most rehospitalization events were emergency readmissions.
Table 2 Time-to-First-Readmission Analysis Stratified for T2DM
Table 3 Cumulated Readmission Events of the CKD Cohort Stratified by T2DM
Figure 1 Time-to-first-readmission analyses stratified for prevalent T2DM at index case. Shown is the median duration between index case discharge and the first admission for a given event (days, median [25–75%]). For detailed numbers see .
![Figure 1 Time-to-first-readmission analyses stratified for prevalent T2DM at index case. Shown is the median duration between index case discharge and the first admission for a given event (days, median [25–75%]). For detailed numbers see Table 2.](/cms/asset/e3386cef-5093-4298-a934-fe1e547022a7/dcle_a_12304530_f0001_c.jpg)
Figure 2 Readmission events stratified for prevalent T2DM at index case. Odds ratios with 95% CI are displayed (non-T2DM vs T2DM). For detailed numbers see .
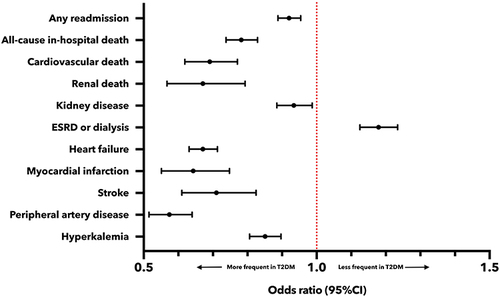
In Cox regression analysis, presence of T2DM was associated with a higher risk for all combined readmission events during FU, readmission for heart failure, readmission for “kidney disease” (according to Supplemental Table 3) and in-hospital mortality during FU (Supplemental Table 4). However, presence of T2DM was not associated with an increased risk for the endpoint kidney failure/dialysis (hazard ratio [95% CI] 0.996 [0.955, 1.039]; p = 0.868). Treatment in tertiary care centres and specialty care centres as well as male sex were associated with increased risk for this endpoint. Increased age was not associated with a higher risk for readmission for kidney failure/dialysis or the endpoint “kidney disease”.
displays the corresponding OR, and provides detailed numbers for all cumulated readmission events. Supplemental Table 4 shows results from Cox regression analyses. Supplemental Table 5 shows event rates per 100 patient-years.
Discussion
The present sub-analysis of the CaReMe-CKD study provides real-world in-hospital data up to 2022 of patients in Germany with and without T2DM. We highlight the following main findings: hospitalised patients with CKD represent a high-risk population, characterized by a high burden of comorbidities, particularly related to cardiovascular issues. These patients often experience adverse events such as rehospitalizations and in-hospital death. Prevalence of T2DM leads to a significant increase in the burden of CVD, which consequently has a substantial effect on mortality. However, deaths attributed to the underlying renal disease were the primary factor contributing to in-hospital mortality among index cases. In our cohort, hospitalised CKD patients without T2DM were younger but presented with more advanced kidney disease, as indicated by the proportion of patients with CKD stage 5/kidney failure at baseline and the higher number of rehospitalizations due to kidney failure/dialysis during FU. With this analysis, we emphasize the need to focus on patients with DKD as well as NDKD in everyday clinical practice to continuously optimise therapy and halt the progression of the underlying renal disease and prevent adverse outcomes. To the best of our knowledge, this is currently the largest analysis of real-world data analysing characteristics and outcomes of hospitalized CKD patients in Germany.
Our study once more highlights the interplay between diabetes mellitus, CKD and CVD and its consequences for patients’ prognosis among a large cohort of inpatients. Taken together, these conditions pose a serious challenge for healthcare systems worldwide.Citation1,Citation27 Various pathophysiological mechanisms such as liberation of mediators of inflammation and fibrosis in patients with diabetic metabolic disorders promoting both CKD and CVD have been described.Citation27–30 However, promising therapeutic targets also emerge from the shared pathophysiology within the triad of cardiovascular, renal and metabolic disease opening up novel treatment options that have been shown to significantly improve outcomes, leading to a paradigm shift in medical therapy for these patient cohorts.Citation27,Citation31,Citation32 Intensified risk factor control with respect to hypertension, dyslipidaemia and hyperglycaemia has also been shown to reduce the risk for major adverse cardiovascular events in patients with DKD,Citation33 which once more emphasizes the importance of an adequate patient management within the triad of CKD, diabetes mellitus and CVD.
For our analysis, we aimed to establish a homogenous cohort of patients with CKD and evaluate the influence of T2DM on patient outcomes. Therefore, we excluded patients with type 1 diabetes mellitus as they generally have younger age and a diverse risk profile.Citation34 T2DM prevalence was 47.9%, which is slightly higher than the overall diabetes prevalence reported in the CaReMe-CKD global study.Citation2 In the 2021 US renal data system report, diabetes (including type 1 diabetes mellitus) was present in ~50% of insured individuals with CKD.Citation35 In the German cohort of the multinational Chronic Kidney Disease Outcomes and Practice Patterns Study (CKDopps),Citation36 a prospective cohort including ~1800 patients with stage 3 and 4 CKD and a comparable demographic profile (median age, 75 years; female, 42%), 42% of patients had diabetes, which is comparable with our reported prevalence.Citation37 The German Chronic Kidney Disease (GCKD) prospective study established one of the largest European CKD cohorts with over 5000 patients.Citation38,Citation39 The lower mean age in this cohort of 60 years might explain the reported lower diabetes prevalence of 35%. Nevertheless, CVD burden was pronounced in both GCKD and CKDopps study populations, with significant differences between patients with and without diabetes.Citation37,Citation39 The prevalence of heart failure in our cohort was 46%, which is considerably higher than the 13% reported for CKDopps.Citation37 This difference could be attributed to the fact that our analysis included only inpatients and the majority had terminal kidney failure, and the risk of heart failure increases with CKD severity.Citation40 We also observed high prevalence of coronary heart disease and atrial fibrillation, which are common causes of heart failure.Citation41 Notably, CKDopps and GCKD trials excluded patients with kidney failure and recruitment occurred in the outpatient setting; hence, cohorts must be cautiously compared.
Patients with T2DM showed very low rates of diabetic eye complications (diabetic retinopathy) in comparison to previous published data.Citation42 Within the disease management program for T2DM in Germany, a structured screening program for diabetic retinopathy is recommended every 1–2 years,Citation43 however, a lack of screening for this complication was previously reported.Citation44,Citation45 Hence, diabetic retinopathy is likely to be significantly underdiagnosed in our cohort, especially considering that patients were hospitalised with CKD during the index cases, where screening for diabetic retinopathy is unlikely to be part of routine patient assessment.
Most patients presented with CKD stage 5 (37.6%) with a significant difference between T2DM (32.8%) and non-T2DM (42.1%) patients. To accurately identify the patient cohort with kidney failure, we used an augmented definition that included dialysis-specific OPS codes (Supplemental Table 1). Per this definition, kidney failure was present in 50% of the total cohort. In-hospital mortality during index case was 11.2% and 10.8% during FU for the total cohort. In the German CKDopps trial, which excluded patients with CKD stage 5, the underlying CKD progressed to kidney failure in 24.9% of patients at a median FU 29 months and 24.4% died.Citation37 Among other variables, diabetes was identified as a predictor of kidney failure and death. In the significantly younger GCKD patient cohort, all-cause mortality was 7.2%Citation46 and 11.8% in 4 years and 6.5 years of FU,Citation47 respectively. CVDs were major drivers of mortality in both CKDopps and GCKD.Citation37,Citation46,Citation47 In accordance with the high baseline prevalence of advanced CKD in our claims data-based cohort, deaths attributed to renal causes, according to the pre-defined endpoints, were the major driver of index in-hospital mortality albeit cardiovascular death was more frequently observed during FU. To the best of our knowledge, large representative studies with specific focus on German in-hospital populations with CKD are lacking. Therefore, when comparing outcomes of our study to the available data, it is important to consider the composition of cohorts. Patients in our study were predominantly hospitalised because of the underlying renal pathology (see CKD definition in section “Methods”) suggesting a severe disease state. Our study included inpatient data only, so it was not possible in a meaningful way to differentiate between incident and prevalent CKD. A high proportion of patients with prevalent CKD is, however, likely as most patients presented with CKD stage 5 or kidney failure (per the above mentioned definition) at index hospitalization.
One of the key findings of this study is that despite a lower mean age, non-T2DM patients had more advanced underlying CKD. This was indicated by the prevalence of CKD stage 5/kidney failure at baseline and differences in the cumulative number of readmission events for kidney failure/dialysis during FU. In adjusted Cox regression analysis, T2DM was not associated with an increased risk for rehospitalizations for kidney failure/dialysis. Previous investigations have consistently identified diabetes as a major risk factor for severe CKD and progression to kidney failure.Citation16,Citation17,Citation37,Citation39 However, NDKD patients also represent a high-risk population, as reported in a retrospective study by Menon et al, where 56% of the NDKD cohort patients advanced to kidney failure (median FU, 88 months) and 22% died (median FU, 123 months).Citation15 A recent claims data-based analysis from the United States reported an event rate of 10.3/100 patient-years for the composite kidney outcome (end-stage renal disease/kidney failure/dialysis) and 4.0/100 for heart failure hospitalizations, which compares well with our data.Citation13 In 2004, Germany introduced a structured disease management program for patients with diabetes, which includes regular (quarterly or half-yearly) check-ups at the treating general practitioner.Citation48,Citation49 Less advanced CKD and better renal outcomes in T2DM patients could be due to better FU in the outpatient setting compared to non-T2DM patients. We recommend evaluating the possibilities of establishing disease management programs for patients with CKD as presently, no such care program exists in Germany. Importantly, data on the true cause of the underlying renal disease were not available in our administrative database due to the unavailability of kidney biopsy results. The cause of CKD in patients with T2DM might also be non-diabetic;Citation5 however, this influence could not be investigated in our study. Due to the higher burden of especially cardiovascular comorbidities in the CKD-T2DM cohort, more frequent hospitalizations also prior to the index hospitalization can be expected. Therefore, a closer monitoring of renal function and initiation of therapeutic interventions during those hospitalizations is likely in this cohort, which may be a possible influencing factor explaining our observation of less advanced renal disease in the CKD-T2DM cohort.
In line with the increased CVD burden at the index case, we also observed more and earlier rehospitalizations due to CVD in patients with T2DM during FU. The prevalence of AKI in the overall cohort at index case was high with a significant difference between T2DM and non-T2DM patients. AKI is associated with increased long-term mortality risk.Citation50,Citation51 A large meta-analysis by Odutayo et al provided additional evidence of an increased risk for cardiovascular adverse events in patients with AKI.Citation51 In addition to a higher baseline CVD burden, the observed difference in AKI prevalence at index hospitalization may have negatively influenced cardiovascular outcomes in the CKD-T2DM cohort during FU. Additionally, readmission numbers for hyperkalaemia were significantly higher in the T2DM cohort. The increased risk for hyperkalaemia in patients with CKD is evidentCitation52 and exacerbated in the presence of DKD.Citation53,Citation54 From a pathophysiological perspective, diabetes leads to hyporeninemic hypoaldosteronism resulting in lower aldosterone levels, reduced potassium excretion and type IV renal tubular acidosis.Citation53–57 Patients presenting with the triad of diabetes, CKD and CVD, especially those with heart failure, must be considered a high-risk population for the development of hyperkalaemia as guideline-recommended medical therapy in these cohorts, such as inhibitors of the renin-angiotensin-aldosterone system or potassium-sparing diuretics, may cause additional increases in serum potassium levels.Citation53 Potassium-lowering agents might present an option for these patients in order to continue guideline-directed medical therapy up to the maximum tolerated dose.Citation52,Citation53 The influence of hyperkalaemia in our CKD-T2DM cohort on the increased risk of cardiovascular events and mortality during FU should be noted, as previous studies have already provided evidence in this regard.Citation58–60
Limitations
We acknowledge several limitations in connection with this study. First, this study was an observational cohort study using retrospective data only. Retrospective data are generally considered to be of inferior quality compared to prospective data.Citation61 However, a major advantage of retrospective data analysis is the ability to examine large nationwide datasets and provide a population-based overview on characteristics of specific patient cohorts, as our study has shown. Observational studies, however, only allow to describe associations and no cause-and-effect relationship. Hence, no hypothesis testing was performed.
Administrative data in general come with limitations as the data quality depends on correct coding and the data are stored not for research but remuneration reasons.Citation62 For CKD, this is especially important as the CaReMe global trial highlighted a discrepancy between eGFR-measured and diagnosed CKD.Citation2 A recent study by Bothe et al reported an acceptable sensitivity of ICD-10-GM codes to identify CKD, however, with limited discrimination between CKD stages.Citation63 Due to the unavailability of laboratory values, only patients with an ICD-10-GM-encoded CKD diagnosis (according to the definition described above) were analysed. Therefore, the number of CKD cases (including “measured” CKD) during the observation period is likely to be higher and it can be expected that a significant number of patients with CKD could not be identified in our data set.
In our study, there was a marked discrepancy between encoded CKD stage 5 diagnoses (ICD-10-GM code N18.5) and kidney failure (as defined by N18.5 or ICD-10-GM/OPS codes indicating dialysis), suggesting a significant proportion of patients requiring dialysis but without a code for CKD stage 5 (see “Results” section). It is possible that some patients in the kidney failure cohort required only time-limited dialysis in an acute setting. However, OPS codes describing continuous methods for haemodialysis or haemofiltration, which are predominantly used to treat acute renal failure, were not included in our definitions (Supplemental Table 1). Nonetheless, incorrect coding cannot be ruled out in this context.
Furthermore, CKD definitions vary between studies. Most investigators use eGFR-based definitions,Citation13,Citation37,Citation39 which could not be applied in our claims data-based cohort as laboratory values were unavailable. This may hinder comparability between studies. However, we believe that our multimodal definition using ICD-10-GM and OPS codes helped establish a well-selected cohort of hospitalised patients with CKD.
Due to data structure and data protection regulations, linking patient data between hospitals was not possible, potentially leading to double counting of patients treated in different hospitals (fulfilling the above mentioned CKD definition), therefore affecting the cohort composition. Additionally, an underestimation of readmission numbers is likely, which is especially important in the light of Cox regression analyses. Lastly, we acknowledge that patient tracking during FU was only possible using in-hospital data from the Helios hospital network (no outpatient data or hospital data outside of Helios), potentially underestimating FU mortality and rehospitalization prevalence.
Conclusion
In this cohort of inpatients with CKD from a large-scale German hospital network, T2DM was present in nearly half of the patients. Hospitalised CKD patients are at a high risk for adverse outcomes. Patients with both CKD and T2DM have an increased prevalence of CVD and are prone to higher in-hospital mortality and rehospitalization rates. However, hospitalized CKD patients without T2DM had more advanced underlying renal disease. Future prospective studies including also outpatient data are required to understand the characteristics and outcomes of CKD patients with and without T2DM in Germany. The data derived from the CaReMe trial add to the body of evidence focusing on these specific patient cohorts in the hospital setting and highlight the need for close monitoring of patients with CKD to prevent adverse outcomes in the inpatient and outpatient sectors in Germany.
Abbreviations
AKI, acute kidney injury; CI, confidence interval; CKDopps, Chronic Kidney Disease Outcomes and Practice Patterns Study; CVD, cardiovascular diseases; DKD, diabetic kidney disease; GCKD, German Chronic Kidney Disease study; eGFR, estimated glomerular filtration rate; FU, follow-up; ICD-10-GM, International Statistical Classification of Diseases and Related Health Problems Version 10, German Modification; NDKD, non-diabetic kidney disease; OPS, Operation and Procedure classification system; OR, odds ratio; T2DM, Type 2 diabetes mellitus.
Statement of Ethics
The analysis was conducted according to the principles outlined in the Declaration of Helsinki. Patient-related data were stored in an anonymised form. The local ethics committee (vote: AZ 010/21-ek) and the Helios Kliniken GmbH data protection authority approved data use for this study.
Author Contributions
All named authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The Helios Health Institute has a research cooperation with AstraZeneca Germany. AstraZeneca financially supported the analyses underlying this publication. No authors received any personal payment nor is any employee of the Helios Health Institute (financially) related to AstraZeneca. The authors report no other conflicts of interest in this work.
Acknowledgments
The authors thank PD Dr Max Lennart Eckstein, Dr Jakob Birnbaum, Dr Marlena Müller for their help with content support while conducting this study. We also thank Dr Celina M. Gollop, Pia Schmitz and Konstantinos Mouratis for their help concerning project management.
Data Sharing Statement
Helios Health and Helios Hospitals have strict rules regarding data sharing because health claims data are a sensible data source and have ethical restrictions imposed due to privacy concerns. Access to anonymised data supporting the findings of this study is available on request from the Helios Health Institute (www.helios-health-institute.com). Please direct queries to the data protection officer (Email: [email protected]) and refer to the study “CaReMe CKD”.
Additional information
Funding
References
- Bikbov B, Purcell CA, Levey AS, et al. Global, regional, and national burden of chronic kidney disease, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2020;395(10225):709–733. doi:10.1016/s0140-6736(20)30045-3
- Sundström J, Bodegard J, Bollmann A, et al. Prevalence, outcomes, and cost of chronic kidney disease in a contemporary population of 2·4 million patients from 11 countries: the CaReMe CKD study. Lancet Region Health. 2022;20:100438. doi:10.1016/j.lanepe.2022.100438
- Hill NR, Fatoba ST, Oke JL, et al. Global prevalence of chronic kidney disease – A systematic review and meta-analysis. PLoS One. 2016;11(7):e0158765. doi:10.1371/journal.pone.0158765
- Matsushita K, Kaptoge S, Hageman SH, et al. Including measures of chronic kidney disease to improve cardiovascular risk prediction by SCORE2 and SCORE2-OP. Euro J Prevent Cardiol. 2022. doi:10.1093/eurjpc/zwac176
- Anders H-J, Huber TB, Isermann B, Schiffer M. CKD in diabetes: diabetic kidney disease versus nondiabetic kidney disease. Nat Rev Nephrol. 2018;14(6):361–377. doi:10.1038/s41581-018-0001-y
- Koye DN, Magliano DJ, Nelson RG, Pavkov ME. The global epidemiology of diabetes and kidney disease. Adv Chronic Kidney Dis. 2018;25(2):121–132. doi:10.1053/j.ackd.2017.10.011
- Wu B, Bell K, Stanford A, et al. Understanding CKD among patients with T2DM: prevalence, temporal trends, and treatment patterns—NHANES 2007–2012. BMJ Open Diabetes Res Care. 2016;4(1):e000154. doi:10.1136/bmjdrc-2015-000154
- Brück K, Stel VS, Gambaro G, et al. CKD prevalence varies across the European general population. J Am Soc Nephrol. 2016;27(7):2135–2147. doi:10.1681/asn.2015050542
- Tuttle KR, Bakris GL, Bilous RW, et al. Diabetic kidney disease: a report from an ADA consensus conference. Diabetes Care. 2014;37(10):2864–2883. doi:10.2337/dc14-1296
- Thomas MC, Cooper ME, Zimmet P. Changing epidemiology of type 2 diabetes mellitus and associated chronic kidney disease. Nat Rev Nephrol. 2016;12(2):73–81. doi:10.1038/nrneph.2015.173
- Navaneethan SD, Schold JD, Jolly SE, Arrigain S, Winkelmayer WC, Nally JV. Diabetes control and the risks of ESRD and Mortality in Patients With CKD. Am J Kidney Dis. 2017;70(2):191–198. doi:10.1053/j.ajkd.2016.11.018
- Fiorentino M, Bolignano D, Tesar V, et al. Renal biopsy in patients with diabetes: a pooled meta-analysis of 48 studies. Nephrol Dial Transplant. 2017;32(1):97–110. doi:10.1093/ndt/gfw070
- Wanner C, Schuchhardt J, Bauer C, et al. Clinical characteristics and disease outcomes in non-diabetic chronic kidney disease: retrospective analysis of a US healthcare claims database. J Nephrol. 2022;36(1):45–54. doi:10.1007/s40620-022-01340-x
- Webster AC, Nagler EV, Morton RL, Masson P. Chronic kidney disease. Lancet. 2017;389(10075):1238–1252. doi:10.1016/S0140-6736(16)32064-5
- Menon V, Wang X, Sarnak MJ, et al. Long-term outcomes in nondiabetic chronic kidney disease. Kidney Int. 2008;73(11):1310–1315. doi:10.1038/ki.2008.67
- Zhang X, Fang Y, Zou Z, et al. Risk Factors for Progression of CKD with and without Diabetes. J Diabetes Res. 2022;2022:1–12. doi:10.1155/2022/9613062
- Go AS, Yang J, Tan TC, et al. Contemporary rates and predictors of fast progression of chronic kidney disease in adults with and without diabetes mellitus. BMC Nephrol. 2018;19:1. doi:10.1186/s12882-018-0942-1
- Heerspink HJL, Stefánsson BV, Correa-Rotter R, et al. Dapagliflozin in patients with chronic kidney disease. N Engl J Med. 2020;383(15):1436–1446. doi:10.1056/nejmoa2024816
- Wheeler DC, Stefánsson BV, Jongs N, et al. Effects of dapagliflozin on major adverse kidney and cardiovascular events in patients with diabetic and non-diabetic chronic kidney disease: a prespecified analysis from the DAPA-CKD trial. Lancet Diabetes Endocrinol. 2021;9(1):22–31. doi:10.1016/s2213-8587(20)30369-7
- Darbà J, Marsà A. Chronic kidney disease in Spain: analysis of patient characteristics, incidence and direct medical costs (2011–2017). J Med Econo. 2020;23(12):1623–1629. doi:10.1080/13696998.2020.1830782
- Escobar C, Aranda U, Palacios B, et al. Epidemiology, clinical profile, management, and two-year risk complications among patients with chronic kidney disease in Spain. Nefrologia. 2021;41(6):670–688. doi:10.1016/j.nefroe.2022.01.008
- Hobson P, Kumwenda M, Shrikanth S, Nair H, Wong S. Risk and incidence of cognitive impairment in patients with chronic kidney disease and diabetes: the results from a longitudinal study in a community cohort of patients and an age and gender-matched control cohort in North Wales, UK. BMJ Open. 2022;12(3):e053008. doi:10.1136/bmjopen-2021-053008
- Palanca A, Castelblanco E, Perpiñán H, et al. Prevalence and progression of subclinical atherosclerosis in patients with chronic kidney disease and diabetes. Atherosclerosis. 2018;276:50–57. doi:10.1016/j.atherosclerosis.2018.07.018
- Moore BJ, White S, Washington R, Coenen N, Elixhauser A. Identifying Increased Risk of Readmission and In-hospital Mortality Using Hospital Administrative Data: the AHRQ Elixhauser Comorbidity Index. Med Care. 2017;55(7):698–705. doi:10.1097/MLR.0000000000000735
- Gasparini A. comorbidity: an R package for computing comorbidity scores. J Open Source Software. 2018;3(23):648. doi:10.21105/joss.00648
- Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. 2007;370(9596):1453–1457. doi:10.1016/s0140-6736(07)61602-x
- Morales J, Handelsman Y. Cardiovascular outcomes in patients with diabetes and kidney disease. J Am College Cardiol. 2023;82(2):161–170. doi:10.1016/j.jacc.2023.04.052
- Ronco C, Bellasi A, Di Lullo L. Cardiorenal Syndrome: an Overview. Adv Chronic Kidney Dis. 2018;25(5):382–390. doi:10.1053/j.ackd.2018.08.004
- Barrera-Chimal J, Jaisser F. Pathophysiologic mechanisms in diabetic kidney disease: a focus on current and future therapeutic targets. Diabetes Obesity Metab. 2020;22(S1):16–31. doi:10.1111/dom.13969
- Ormazabal V, Nair S, Elfeky O, Aguayo C, Salomon C, Zuñiga FA. Association between insulin resistance and the development of cardiovascular disease. Cardiovasc Diabetol. 2018;17(1). doi:10.1186/s12933-018-0762-4
- Swamy S, Noor SM, Mathew RO. Cardiovascular disease in diabetes and chronic kidney disease. J Clin Med. 2023;12(22):6984. doi:10.3390/jcm12226984
- Handelsman Y, Anderson JE, Bakris GL, et al. DCRM Multispecialty Practice Recommendations for the management of diabetes, cardiorenal, and metabolic diseases. J diabet complicat. 2022;36(2):108101. doi:10.1016/j.jdiacomp.2021.108101
- Sasso FC, Pafundi PC, Simeon V, et al. Efficacy and durability of multifactorial intervention on mortality and MACEs: a randomized clinical trial in type-2 diabetic kidney disease. Cardiovasc Diabetol. 2021;20:1. doi:10.1186/s12933-021-01343-1
- Piscitelli P, Viazzi F, Fioretto P, et al. Predictors of chronic kidney disease in type 1 diabetes: a longitudinal study from the AMD Annals initiative. Sci Rep. 2017;7(1). doi:10.1038/s41598-017-03551-w
- Johansen KL, Chertow GM, Gilbertson DT, et al. US Renal Data system 2021 annual data report: epidemiology of kidney disease in the United States. Am J Kidney Dis. 2022;79(4):A8–A12. doi:10.1053/j.ajkd.2022.02.001
- Mariani L, Stengel B, Combe C, et al. The CKD Outcomes and Practice Patterns Study (CKDopps): rationale and Methods. Am J Kidney Dis. 2016;68(3):402–413. doi:10.1053/j.ajkd.2016.03.414
- Reichel H, Zee J, Tu C, et al. Chronic kidney disease progression and mortality risk profiles in Germany: results from the chronic kidney disease outcomes and practice patterns study. Nephrol Dial Transplant. 2020;35(5):803–810. doi:10.1093/ndt/gfz260
- Eckardt KU, Bärthlein B, Baid-Agrawal S, et al. The German Chronic Kidney Disease (GCKD) study: design and methods. Nephrol Dial Transplant. 2012;27(4):1454–1460. doi:10.1093/ndt/gfr456
- Titze S, Schmid M, Köttgen A, et al. Disease burden and risk profile in referred patients with moderate chronic kidney disease: composition of the German Chronic Kidney Disease (GCKD) cohort. Nephrol Dial Transplant. 2015;30(3):441–451. doi:10.1093/ndt/gfu294
- Tuegel C, Bansal N. Heart failure in patients with kidney disease. Heart. 2017;103(23):1848. doi:10.1136/heartjnl-2016-310794
- McDonagh TA, Metra M, Adamo M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021. doi:10.1093/eurheartj/ehab368
- Teo ZL, Tham YC, Yu M, et al. Global prevalence of diabetic retinopathy and projection of burden through 2045: systematic review and meta-analysis. Ophthalmology. 2021;128(11):1580–1591. doi:10.1016/j.ophtha.2021.04.027
- Nationale Versorgungsleitlinie (NVL) Type 2-Diabetes (National guideline for type 2 diabetes mellitus). Available from: https://www.leitlinien.de/themen/diabetes/version-3. Accessed June 7, 2024.
- Federal Robert Koch Institute (RKI): diabetes surveillance in Germany. Available from: https://diabsurv.rki.de/Webs/Diabsurv/EN/diabetes-in-germany/adults/quality_type-2-diabetes_care/2-158_ophthalmological_examination.html. Accessed June 7, 2024.
- Kreft D, McGuinness MB, Doblhammer G, Finger RP. Diabetic retinopathy screening in incident diabetes mellitus type 2 in Germany between 2004 and 2013 - A prospective cohort study based on health claims data. PLoS One. 2018;13(4):e0195426. doi:10.1371/journal.pone.0195426
- Fazzini F, Lamina C, Raschenberger J, et al. Results from the German Chronic Kidney Disease (GCKD) study support association of relative telomere length with mortality in a large cohort of patients with moderate chronic kidney disease. Kidney Int. 2020;98(2):488–497. doi:10.1016/j.kint.2020.02.034
- Pammer LM, Lamina C, Schultheiss UT, et al. Association of the metabolic syndrome with mortality and major adverse cardiac events: a large chronic kidney disease cohort. J Internal Med. 2021;290(6):1219–1232. doi:10.1111/joim.13355
- Mehring M, Donnachie E, Bonke FC, Werner C, Schneider A. Disease management programs for patients with type 2 diabetes mellitus in Germany: a longitudinal population-based descriptive study. Diabetol Metab Syndr. 2017;9(1). doi:10.1186/s13098-017-0236-y
- Stock S, Drabik A, Büscher G, et al. German diabetes management programs improve quality of care and curb costs. Health Affairs. 2010;29(12):2197–2205. doi:10.1377/hlthaff.2009.0799
- Coca SG, Yusuf B, Shlipak MG, Garg AX, Parikh CR. Long-term risk of mortality and other adverse outcomes after acute kidney injury: a systematic review and meta-analysis. Am J Kidney Dis. 2009;53(6):961–973. doi:10.1053/j.ajkd.2008.11.034
- Odutayo A, Wong CX, Farkouh M, et al. AKI and Long-term risk for cardiovascular events and mortality. J Am Soc Nephrol. 2017;28(1):1.
- Costa D, Patella G, Provenzano M, et al. Hyperkalemia in CKD: an overview of available therapeutic strategies. Front Med. 2023:10. doi:10.3389/fmed.2023.1178140
- Albakr RB, Sridhar VS, Cherney DZI. Novel therapies in diabetic kidney disease and risk of hyperkalemia: a review of the evidence from clinical trials. Am J Kidney Dis. 2023;82(6):737–742. doi:10.1053/j.ajkd.2023.04.015
- Goia-Nishide K, Coregliano-Ring L, Rangel ÉB. Hyperkalemia in diabetes mellitus setting. Diseases. 2022;10(2):20. doi:10.3390/diseases10020020
- Sousa AG, Cabral JV, El-Feghaly WB, de Sousa LS, Nunes AB. Hyporeninemic hypoaldosteronism and diabetes mellitus: pathophysiology assumptions, clinical aspects and implications for management. World J Diabetes. 2016;7(5):101–111. doi:10.4239/wjd.v7.i5.101
- Batlle D, Arruda J. Hyperkalemic forms of renal tubular acidosis: clinical and pathophysiological aspects. Adv Chronic Kidney Dis. 2018;25(4):321–333. doi:10.1053/j.ackd.2018.05.004
- Palmer BF, Kelepouris E, Clegg DJ. Renal tubular acidosis and management strategies: a narrative review. Adv Ther. 2021;38(2):949–968. doi:10.1007/s12325-020-01587-5
- Collins AJ, Pitt B, Reaven N, et al. Association of serum potassium with all-cause mortality in patients with and without heart failure, chronic kidney disease, and/or diabetes. Am J Nephrol. 2017;46(3):213–221. doi:10.1159/000479802
- Kohsaka S, Okami S, Kanda E, Kashihara N, Yajima T. Cardiovascular and renal outcomes associated with hyperkalemia in chronic kidney disease: a hospital-based cohort study. Mayo Clin Proc. 2021;5(2):274–285. doi:10.1016/j.mayocpiqo.2020.10.001
- Hoppe LK, Muhlack DC, Koenig W, Carr PR, Brenner H, Schöttker B. Association of abnormal serum potassium levels with arrhythmias and cardiovascular mortality: a systematic review and meta-analysis of observational studies. Cardiovasc Drugs Ther. 2018;32(2):197–212. doi:10.1007/s10557-018-6783-0
- Wang X, Kattan MW. Cohort studies. Chest. 2020;158(1):S72–S78. doi:10.1016/j.chest.2020.03.014
- Quan H, Sundararajan V, Halfon P, et al. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med Care. 2005;43(11):1130–1139. doi:10.1097/01.mlr.0000182534.19832.83
- Bothe T, Fietz A-K, Schaeffner E, et al. Diagnostic validity of chronic kidney disease in health claims data over time: results from a cohort of community-dwelling older adults in Germany. Clin Epidemiol. 2024;16:143–154. doi:10.2147/clep.s438096