Abstract
Background
The purpose of this study was to determine the prevalence of atrial fibrillation (AF) in the general population and to validate an administrative diagnosis register, ie, the National Patient Register (NPR), and an electrocardiography (ECG) database in estimating disease prevalence.
Methods
The study was conducted in a well defined region in northern Sweden (population n=75,945) which consists of one hospital and eleven primary health care centers. Subjects with AF were identified by searching the combined inpatient and outpatient International Classification of Diseases (ICD)-based NPR (ICD-10 code I48) and an ECG database with computer-interpreted AF from January 1, 2004 to December 31, 2010. All identified cases with AF were validated.
Results
AF was confirmed in 2,274 patients. The overall prevalence was 3.0% (3.4% in men and 2.6% in women). AF prevalence rose steadily with age, and was 16.8% in patients aged 75 years and older and 21.9% in patients 85 years and older. Of all patients with validated AF, the NPR identified 93.2%. The ECG database identified an additional 6.8%, of which 81% were over 70 years of age. According to the NPR, the proportion of false positives and false negatives was 3.5% and 6.8%, respectively. The corresponding figure for the ECG database was 11.3% and 9.2%, respectively.
Conclusion
Our study shows a high prevalence of AF, especially among the elderly. Searching the ECG database enhanced the detection of AF. The reliability of the NPR was high, with a relatively low proportion of false positives and negatives.
Introduction
Studies investigating the prevalence of atrial fibrillation (AF) have been conducted in several settings with differing results.Citation1–Citation8 Many studies are based on review of inpatient records or by screening populations and diagnosing AF with a single electrocardiogram (ECG). Reported prevalence rates range widely. The variation in prevalence may depend, among other things, on the selection of the population and methods used for identification and validation of AF. A recent systematic review of methods for identifying AF with administrative data showed that using an International Classification of Diseases (ICD) diagnosis code performed relatively well, but most studies have focused on inpatient data.Citation9 The authors suggested that additional research combining representative populations (both inpatient and outpatient) with electronic ECG data would be optimal.
Contemporary ECG systems allow for computerized interpretation, electronic storage and transmission, and a searchable database categorized by diagnosis. This gives an opportunity to identify subjects with AF who would not have been previously diagnosed and registered within the health care system.
The primary objective of this study was to determine the prevalence of AF in the general population within a defined geographical area using both the administrative diagnosis register and the ECG database. A secondary objective was to validate the administrative diagnosis register and the ECG database in estimating disease prevalence.
Materials and methods
Skellefteå County Hospital is situated in northern Sweden and is the only hospital in the catchment area. The number of inhabitants living in the area as of December 31, 2010 was 75,945 according to the Swedish National Registry.Citation10 All patients in the area requiring specialized care are primarily treated at Skellefteå County Hospital, while patients with complicated cardiac conditions are referred to the University Hospital in Umeå, returning to Skellefteå Hospital for post-procedural care and follow-up. Compared with the rest of Sweden, the population of the Skellefteå region is slightly older (mean age 43.0 years versus 42.1 years) and characterized by a low level of migration in and out of the county (3.0% versus 5.6% of the population annually).Citation10
Swedish health care registers rely on a 12-digit personal identity number (PIN) as a unique identifier. All individuals who live in Sweden on a permanent basis are assigned a PIN. It can be used to trace and identify subjects in health care records and databases and to eliminate the risk of duplication when studying the prevalence of a specific diagnosis. All individuals with a PIN are registered in the Total Population Register (TPR) which includes information on current residence. The PIN therefore gives an opportunity to identify individuals with a specific ICD-code in a defined area.Citation11
The administrative diagnosis register, ie, the National Patient Register (NPR) in Sweden, codes all diagnoses of inpatients and outpatients according to the World Health Organization ICD classification system. We searched the NPR for the Skellefteå Hospital and the eleven primary health care centers in order to identify patients with AF in the area. Patients who had received a diagnosis of AF or atrial flutter (ICD-10 code I48) from January 1, 2004 to December 31, 2010 were included for further review.
All primary health care centers, hospitals, and ambulances in the area use a resting 5-second 12-lead ECG tracings recorder, primarily a MAC 5000 (General Electric, Fairfield, CT, USA) with the Marquette system for computerized interpretation. The ECGs are transmitted electronically and stored in a central ECG database. The Marquette system has been shown to have a sensitivity of 90.8% for AF and 61.0% for atrial flutter; the specificity is 98.9% and 99.9%, respectively, in non-paced ECGs.Citation12 We searched the ECG database in the Skellefteå region for any ECG collected with the computerized interpretation of AF during the designated time period. The database contained 144,000 ECGs representing 36,000 unique individuals. Diagnosed cases of AF were also requested from the seven private general practitioners in the region who are not connected to the central database.
By relying on the TPR we could exclude deceased, migrated from the area, and non-residents as of December 31, 2010. The remaining cases with a diagnosis of AF and an available 12-lead ECG in the database were manually validated by two physicians through interpretation of the ECG tracings. One verified episode of AF was determined sufficient for study inclusion. If there were any uncertainties, a consultant cardiologist was asked for a final interpretation. If AF could not be confirmed or any uncertainty persisted, the diagnosis was discarded.
In addition, for cases with a diagnosis of AF according to the NPR, but without an ECG available in the ECG database, we included and interpreted the 12-lead ECGs retrieved from other sources (eg, outside facilities or printouts from the medical records archive). The AF diagnosis was also considered confirmed when based upon documentation of AF in patient records by physicians at the Department Of Medicine by 12-lead ECG, rhythm strip, pacemaker/implantable cardioverter-defibrillator electrogram, or Holter ECG. Finally, the diagnosis of AF was considered confirmed when supporting documentation of the AF diagnosis was found to be convincing in the patient records, eg, referrals from other hospitals or a known history of cardioverted AF.
Statistical analysis
Data from the Swedish National Registry regarding the number of inhabitants defined by age and sex currently residing in the Skellefteå region on December 31, 2010 was obtained for estimation of prevalence. Estimations of false positive and false negative rates were calculated. All manually confirmed AF cases were used as a gold standard against which the two examined methods were compared. The study was approved by the research ethics committee at Umeå University.
Results
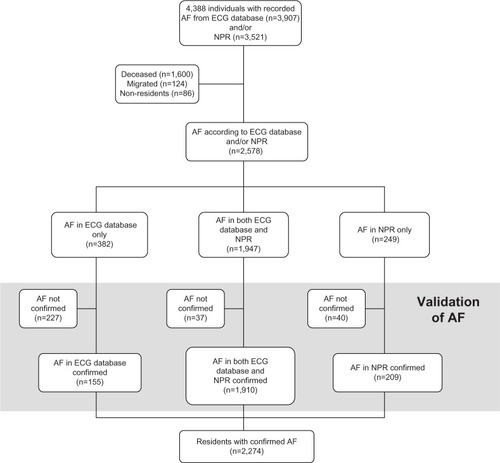
Using both ICD-codes and the ECG database, a total of 4,388 unique cases with AF were identified between 2004 and 2010. Of these 1,810 were registered as deceased, migrated from the area, or as non-residents, leaving 2,578 cases for further examination. After validation, the diagnosis of AF was confirmed in 2,274 cases out of 75,945 residents living in the area as of December 31, 2010. For a detailed description see .
Figure 1 Schematic figure showing the method for finding and validating cases with AF from the ECG database and/or the NPR.
In the population as a whole, AF prevalence was 3.0% (3.4% in men and 2.6% in women). The median age of the patients was 77 years and 43% were women. The prevalence was 0.2% in the age stratum of 30–39 years and rose with increasing age, reaching a peak prevalence of 25.4% in the stratum of 90–94 years (). The prevalence of AF in the different age groups was 7.9% in patients aged 55 years and older, 11.4% in patients aged 65 years and older, 16.8% in patients aged 75 years and older, and 21.9% in patients over 85 years of age.
Table 1 Prevalence of AF for men and women in the Skellefteå region in 2010 according to age
The age stratum with the largest number of patients with AF was 80–84 years. The proportion of women increased over the age groups from 12% in those 50 years and younger to more than 50% among those 80 years and older.
We identified 2,196 patients with a diagnosis of AF according to the NPR, and in 2,119 (96.5%) patients the AF diagnosis was confirmed (). Thus, the proportion of false positives was 3.5% in this group. From the ECG database we identified 2,329 patients with an ECG diagnosis of AF, and in 2,065 (88.7%) patients the diagnosis was confirmed. The proportion of false positives was 11.3%. Patients with confirmed AF from the ECG database alone totaled 155, equal to 6.8% of all 2,274 confirmed with AF. Of these, 126 (81%) were over 70 years of age. Patients identified with AF in both the NPR and the ECG database totaled 1,947, and in 1,910 (98.1%) the diagnosis was confirmed, yielding 1.9% false positives. Of the 2,274 patients with confirmed AF, the NPR identified 93.2%, the ECG database 90.8%, and 84.0% were identified with AF in both the NPR and the ECG database.
Table 2 Numbers and proportions of false negative and false positive subjects classified as having AF for the different electronic health data sources
Discussion
We found a relatively high prevalence of AF especially in the elderly in the Skellefteå region compared with previous studies. The reliability of the NPR was high, with a low proportion of both false positives and negatives. AF cases identified by the ECG database but not found in the NPR moderately increased the prevalence. Despite this, we believe that there are additional cases that remain undiscovered. Considering that AF is often asymptomatic and no routine screening efforts are typically made, our study likely captures a minimum prevalence that includes only patients already known to the health care system.
We compared the prevalence in our study with four European studies in relation to various age strata.Citation4,Citation5,Citation7,Citation8 The prevalence found by Murphy et alCitation5 is considerably lower than in our study. They used cross-sectional data from primary care practices where the diagnosis of AF was captured and recorded during the course of 1 year. One explanation for this lower rate may be that only patients consulting their general practitioner during the short study period were included. The observational period in our study was 7 years, giving a better opportunity to identify patients with AF who seek care intermittently. When we searched the NPR for a single year (2010), only about half of the AF patients were identified as compared with the search made between 2004 and 2010 (data not shown).
In the Rotterdam study, Heeringa et alCitation4 used a population-based cohort design. All inhabitants in the area were invited and ECGs were collected in 70%.Citation4 In addition, they used general practitioners’ records and hospital discharge diagnoses to document AF. Overall, the prevalence rates reported were high in all age groups, with the highest prevalence among those over 85 years of age. The observed increase with advancing age corresponds to the findings in our study, especially among those over 75 years. The Rotterdam study, as in our study, used a combination of ECG tracings as well as hospital and general practitioners’ patient records to identify patients with AF, which may capture a larger proportion of elderly patients. It has been reported that AF incidence is rising in the general population over time.Citation13 The Rotterdam study was performed between 1990 and 1993 and the present study was performed from 2004 to 2010. The higher prevalence we found may reflect an actual increase of AF during this period.
In another study by Andersson et al,Citation7 also performed in northern Sweden between 2008 and 2010, patients with AF were recruited from a local oral anticoagulation treatment and AF quality registry (AURICULA) and from the NPR.Citation7 The prevalence in those 75 years and younger was similar to our findings, yet lower in the oldest age groups when compared with our results. The authors suggest that AF might have been missed in elderly people living in assisted care homes. In our study we found that a majority of the AF patients solely identified from the ECG database were over 70 years. This partially explains the higher prevalence found among elderly people in the present study. The longer recruitment period in our study may have contributed to a higher prevalence rate.
Wilke et alCitation8 used data on documented AF diagnoses from two large health insurance funds.Citation8 The overall prevalence in this population was 2.1% and increased with age. They suggest that the inclusion criteria for their study were conservative because two AF diagnoses in two different quarters were required for outpatients and this may explain the lower overall prevalence compared with the present study. We found a higher prevalence in the oldest age group compared with the studies by both Andersson et al and Wilke et al,Citation7,Citation8 indicating that our search methodology managed to identify more AF among the elderly.
In a systematic review, Jensen et al reported 16 unique studies that identified patients with AF and utilized electronic health data to provide validation information.Citation9 AF was verified by medical records review in 14 studies, while three studies used electronic ECG data for case identification or validation. They found that the overall positive predictive value ranged from 70% to 96% and sensitivity from 57% to 95%.
In the study by Brophy et al, an ECG database was used to identify cases with ECG-documented AF and the national Veterans Affairs clinical database was used to verify a diagnosis code for AF.Citation14 They verified 74.5% of the ECG-identified cases. However, no manual validation was performed. In our study, a similar method would verify 75.5% of AF cases identified in the ECG database. Manual validation discarded only 1.9%. On the other hand, the method used by Brophy et al would lead to a considerable number of unidentified AF cases, which according to our study was 16%.
Finding individuals with AF by utilizing the NPR will miss 6.8% of cases and include 3.5% without a confirmed diagnosis. The prevalence of AF in our population according to the NPR was 2.9%, compared with 3.0% for all AF with a confirmed diagnosis. Using only the ECG database will miss even more (9.2%) and include a substantial number (11.3%) where the diagnosis is not confirmed. Similarly, the prevalence according to the ECG database was 3.1%. In this instance, those with a missed diagnosis are counterbalanced by a higher number with false positives. Thus, using the NPR to identify AF cases is superior to using the ECG database and would be preferable for studies on determinants and prognosis of AF. Estimating the prevalence by accepting the diagnosis only if cases are found in both databases would lower the prevalence rate to 2.6%, but the proportion with a false positive diagnosis decreases to 1.9%. This search strategy may be optimal when it is crucial that the diagnosis is correct, for example when estimating complications during anticoagulant treatment.
Strengths and limitations
We have chosen to include cases with a single episode of AF, such as perioperative AF and AF following coronary surgery, where AF occurs in as many as one in three patients. Although common, perioperative AF is associated with lower long-term survival, increased risk of recurring AF, and a higher risk of dying from thromboembolic events. Thus, this subgroup is clinically important.
Since we have studied the total population that attended the health care system in the catchment area over several years, many elderly patients and even those individuals living in nursing homes have been included. These patient categories usually exhibit low participation rates in screening programs. It is reasonable to assume that the majority of people with symptomatic AF seek medical care and are identified through our methods. On the other hand, persons with asymptomatic permanent AF are likely to be missed with our strategy, but would be identified in screening programs with ECG recordings. Asymptomatic paroxysmal AF is unlikely to be identified with any of these methods, but may be diagnosed with repeated ECG screening, using tools such as the thumb-ECG.
It is known that hypertension and cardiovascular disease is associated with increased risk for AF. Are these risk factors more common in northern Sweden than elsewhere? The incidence of myocardial infarction in northern Sweden is around the national average.Citation15 By international comparison, the population in northern Sweden have intermediate blood pressure levels. Furthermore, the MONICA (Multinational MONItoring of trends and determinants in CArdiovascular disease) study from 1986 to 2009 demonstrated substantial improvements in hypertension, smoking, and hypercholesterolemia in northern Sweden.Citation16 Thus, in our population, the risk factors associated with AF are probably comparable with those in other European populations, making the high prevalence of AF representative for western populations.
In conclusion, our study demonstrates a higher prevalence of AF, especially among the elderly, than previously published studies. Searching the ECG database contributed to the high prevalence among those over 70 years of age. For most observational studies, searching the NPR during an observational period over several years is a sufficient and time-saving method for identification of AF, with a low proportion of false positive as well as false negative diagnoses.
Disclosure
The authors report no conflicts of interest in this work.
References
- WolfPAAbbottRDKannelWBAtrial fibrillation as an independent risk factor for stroke: the Framingham StudyStroke19912289839881866765
- FurbergCDPsatyBMManolioTAGardinJMSmithVERautaharjuPMPrevalence of atrial fibrillation in elderly subjects (the Cardiovascular Health Study)Am J Cardiol19947432362418037127
- GoASHylekEMPhillipsKAPrevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) StudyJAMA2001285182370237511343485
- HeeringaJvan der KuipDAHofmanAPrevalence, incidence and lifetime risk of atrial fibrillation: the Rotterdam studyEur Heart J200627894995316527828
- MurphyNFSimpsonCRJhundPSA national survey of the prevalence, incidence, primary care burden and treatment of atrial fibrillation in ScotlandHeart200793560661217277353
- SchmutzMBeer-BorstSMeiltzALow prevalence of atrial fibrillation in asymptomatic adults in Geneva, SwitzerlandEuropace201012447548120007160
- AnderssonPLondahlMAbdonNJTerentAThe prevalence of atrial fibrillation in a geographically well-defined population in northern Sweden: implications for anticoagulation prophylaxisJ Intern Med2012272217017622250988
- WilkeTGrothAMuellerSIncidence and prevalence of atrial fibrillation: an analysis based on 8.3 million patientsEuropace201315448649323220354
- JensenPNJohnsonKFloydJHeckbertSRCarnahanRDublinSA systematic review of validated methods for identifying atrial fibrillation using administrative dataPharmacoepidemiol Drug Saf201221Suppl 114114722262600
- Population statistics 2011Statistics Sweden2011 Available from: http://www.scb.se/Pages/SSD/SSD_TreeView.aspx?id=340478Accessed October 25, 2013
- LudvigssonJFOtterblad-OlaussonPPetterssonBUEkbomAThe Swedish personal identity number: possibilities and pitfalls in health care and medical researchEur J Epidemiol2009241165966719504049
- PoonKOkinPMKligfieldPDiagnostic performance of a computer-based ECG rhythm algorithmJ Electrocardiol200538323523816003708
- MiyasakaYBarnesMEGershBJSecular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalenceCirculation2006114211912516818816
- BrophyMTSnyderKEGaehdeSIvesCGagnonDFioreLDAnticoagulant use for atrial fibrillation in the elderlyJ Am Geriatr Soc20045271151115615209654
- The National Board of Health and WelfareMyocardial Infarctions in Sweden 1987–2002Stockholm, SwedenThe National Board of Health and Welfare2005
- ErikssonMHolmgrenLJanlertULarge improvements in major cardiovascular risk factors in the population of northern Sweden: the MONICA study 1986–2009J Intern Med2011269221923121158982