
Abstract
Background
Long-term mortality and causes of death in patients with pulmonary tuberculosis (PTB) and extrapulmonary tuberculosis (EPTB) are poorly documented. In this study, long-term mortality and causes of death in PTB and EPTB patients were compared with the background population and it was investigated whether mortality was associated with family-related risk factors.
Methods
A nationwide cohort study was conducted including: all adult Danes notified with PTB or EPTB from 1977 to 2008 and alive 1 year after diagnosis; a randomly selected comparison cohort matched on birth date and sex; adult siblings of PTB patients; and population controls. Data were extracted from national registries. All-cause and cause-specific mortality rate ratios were calculated for patients and siblings and compared with their respective control cohorts. A total of 8,291 patients (6,402 PTB and 1,889 EPTB), 24,873 population controls, 1,990 siblings of PTB patients and 11,679 siblings of PTB population controls were included.
Results
Overall, the mortality rate ratio was 1.86 (95% confidence interval [CI] 1.77–1.96) for PTB patients and 1.24 (95% CI 1.12–1.37) for EPTB patients. Both patient cohorts had significantly increased risk of death due to infectious diseases and diabetes. Further, the PTB patients had increased mortality due to cancers (mainly respiratory and gastrointestinal tract), liver and respiratory system diseases, and alcohol and drug abuse. The PTB patients had increased mortality compared with their siblings (mortality rate ratio 3.55; 95% CI 2.57–4.91) as did the siblings of the PTB patients compared with the siblings of population controls (mortality rate ratio 2.16; 95% CI 1.62–2.87).
Conclusion
We conclude that adult PTB patients have an almost two-fold increased long-term mortality whereas EPTB patients have a slightly increased long-term mortality compared with the background population. The increased long-term mortality in PTB patients stems from diseases associated with alcohol, tobacco, and drug abuse as well as immune suppression, and family-related factors.
Introduction
Tuberculosis (TB) causes more than 1.4 million deaths annually and is the second leading cause of death due to an infectious disease after human immunodeficiency virus (HIV).Citation1 The morbidity and mortality associated with TB is especially pronounced in low-income developing countries where malnutrition, crowded living conditions, and lack of TB control measures makes the disease a serious public health burden.Citation1–Citation3 In high-income industrialized nations, the epidemiology of TB has changed, with immigrants from endemic countries now constituting a major proportion of new TB cases.Citation4,Citation5 Several studies have established specific risk factors and predictors of short-term case fatality rates, but the long-term prognosis of patients with TB is still poorly described.Citation6–Citation8
In order to assess whether long-term mortality is affected in patients who have survived a TB episode compared with the background population, we conducted a nationwide population-based cohort study to determine long-term mortality and causes of death in patients diagnosed with pulmonary (PTB) or extrapulmonary tuberculosis (EPTB). To investigate potential family-related risk factors, we also estimated mortality in siblings of the patients with TB.
Materials and methods
Ethics statement
This study is a registry-based cohort study involving data from various Danish national registries. All data were anonymized before any statistical analysis was performed and the study was approved by the Danish Data Protection Agency.
Study design
This study was conducted as a population-based nationwide cohort study. The study populations were all PTB and EPTB patients registered in Denmark in the period 1977–2008 and a cohort from the background population individually matched on age and sex. Outcomes were time to death and to cause-specific death. The risk of these outcomes was further estimated in the siblings of the patients with TB and compared with that of the siblings of the comparison cohort.
Setting
The population of Denmark was 5.08 million on January 1, 1977 and 5.48 million on January 1, 2008.Citation9 The incidence of TB decreased in the study period from 12/100.000 in 1977 to 6/100.000 in 2008.Citation10,Citation11 Denmark has an estimated HIV prevalence of 0.07%.Citation12 Throughout the study period, Danish citizens had access to free health care and antituberculosis medication. The Bacille Calmette Guerin vaccine was phased out of the Danish national childhood vaccination program in the period 1976–1980. All culture-based TB diagnostics are centralized at the International Reference Laboratory of Mycobacteriology at Statens Serum Institut, Copenhagen, Denmark.
Data sources
The unique 10-digit personal identification number assigned to all Danish citizens at birth or immigration was used to avoid multiple registrations and to track individuals in the following registries.
Danish Tuberculosis Registry
All TB patients diagnosed in Denmark are notified to the Danish Tuberculosis Registry by the treating physician and by the International Reference Laboratory of Mycobacteriology. This notification is mandatory for all patients initiating anti-TB treatment. The Danish Tuberculosis Registry contains data on anatomical localization of TB, ethnic origin, date of diagnosis, residence, and microbiologic data.
Danish National Patient Registry
The Danish National Patient Registry (DNPR) contains information on all patients discharged from Danish somatic hospitals since 1977.Citation13 Data includes dates of admission and discharge diagnosis coded by the International Classification of Diseases, Eighth Revision (ICD-8), until the end of 1993 and the Tenth Revision (ICD-10) thereafter. From this registry, date of first admission with PTB or EPTB was extracted.
Danish Civil Registration System
The Danish National Patient Registry (DCRS) was established in 1968 and contains information on date and place of birth and death, sex, immigration and/or emigration for all Danish residents.Citation14
Danish Registry of Causes of Death
The Danish Registry of Causes of Death contains data from all Danish death certificates since 1943 and is updated to December 31, 2009.Citation15 Causes of death are coded according to ICD-8 until the end of 1993 and according to ICD-10 thereafter. The physician can code one immediate cause of death followed by secondary and/or tertiary causes of death and finally one underlying (main) cause of death.
Study population
PTB and EPTB patients
We included all individuals who fulfilled the following five criteria: notified to the Danish Tuberculosis Registry from January 1, 1977 until December 31, 2008; registered in the DNPR with a diagnosis of PTB (ICD-8 codes 011.00–013.00 and ICD-10 codes A15.0–17.0) or EPTB (ICD-8 codes 014.00–019.00 and ICD-10 codes A 18.0–20.0); notified to the Danish Tuberculosis Registry within 1 year of DNPR date of discharge; ≥16 years of age at time of diagnosis; and registered in the DCRS. EPTB was defined as TB of all anatomical localizations other than lungs and pleura, with the exception of tuberculous meningitis and intracerebral tuberculoma (a detailed study of this patient category has recently been published by Christensen et al)Citation16 and patients diagnosed with miliary TB (to ensure uniform patient populations with sole organ involvement). Diagnosis was either microbiologically verified by positive culture, nucleic acid amplification, or direct microscopy, or based on clinical symptoms and/or radiology. The date of TB diagnosis was defined as the date of first admission for TB according to DNPR, and the index date as 1 year after TB diagnosis. Patients were excluded from the study population if they died, emigrated, or were lost to follow-up within the first year of TB diagnosis.
Population comparison cohorts
For each TB patient, we identified all Danish citizens in the DCRS who were born in Denmark with the same birth date and sex as the patient and were alive and not diagnosed with TB on the index date of the respective patient. From this population, we randomly identified three individuals per TB patient who constituted the comparison cohort. The index date for the population controls was therefore the same as for the TB patient to whom they were matched.
Siblings
From the DCRS, all siblings of the PTB patients and PTB population controls were identified who fulfilled the following criteria: full siblings; born after January 1, 1952, and alive and not younger than 16 years of age at the time of the patient’s or control’s index date. Less than 10% of siblings of individuals born before 1952 could be identified in DCRS, rising to 43% in the 1952 birth cohort and 96% for individuals born after 1958.Citation17 EPTB siblings were not included due to inadequate study population size which did not allow for sibling mortality studies.
Comorbidity
A modified Charlson Comorbidity Index (CCI) score was used as a measurement of comorbidity and calculated from DNPR diagnoses prior to the first TB diagnosis.Citation18 Three levels of comorbidity were defined: none (CCI score 0), low (CCI score 1–2), and high (CCI score >3). As an alternative measure of comorbidity, data on in-hospital patient admissions in the 5 years prior to the date of TB diagnosis was extracted from the DNPR for all patients, population controls, and siblings. These data were subcategorized according to diagnostic categories based on discharge diagnosis.
Statistical analysis
Time was calculated from index date to the date of death, emigration, loss to follow-up or December 31, 2009, whichever came first. Kaplan–Meier analyses were used to construct survival curves. All-cause mortality rate ratios (MRR), representing relative risk of death, and 95% confidence intervals (CIs) were calculated and stratified according to sex, age at time of diagnosis, ethnicity, and level of CCI score of the TB patient. Cause-specific MRRs were based on the underlying cause of death and categorized as listed in the Supplementary materials.
For siblings we computed time from January 1, 1977, or the index date of the respective patient or population control, whichever came last, until date of death, emigration, loss to follow-up, or December 31, 2009, whichever came first. Poisson regression analyses were used to calculate all-cause and cause-specific MRRs (adjusted for age and sex) for siblings of PTB patients compared with siblings of the PTB population controls and for PTB patients born after 1 January, 1952 compared with their respective siblings. Statistical Package for the Social Sciences version 15.0 for Windows (SPSS Inc., Chicago, IL, USA), R version 2.13.0 (R Foundation for Statistical Computing, Vienna, Austria), and Stata version 11 (StataCorp, College Station, TX, USA) were used for data analysis.
Results
Characteristics of TB patient cohorts
We identified 11,258 TB patients of whom 6,402 PTB patients and 1,889 EPTB patients fulfilled the inclusion criteria (). A total of 5,290 (82.6%) PTB patients and 1,713 (90.7%) EPTB patients were microbiologically verified. For both cohorts, the proportion of immigrants increased with calendar time (). Due to the study design, the control cohorts were well matched with respect to age and sex, but PTB and EPTB patients had more comorbidity and had been hospitalized more frequently than their respective population control cohorts ().
Figure 1 Summary of study design.
Abbreviations: EPTB, extrapulmonary tuberculosis; LFU, lost to follow-up; PTB, pulmonary tuberculosis; TB, tuberculosis; yrs, years.
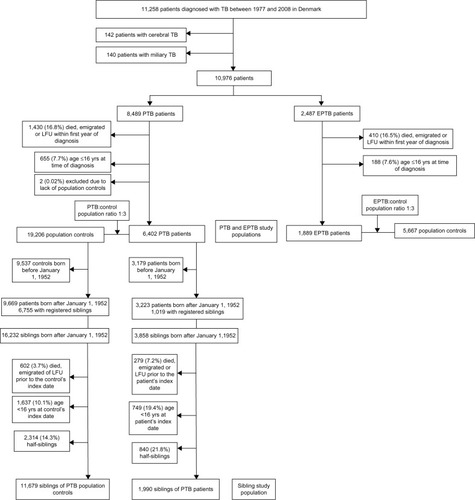
Table 1 Characteristics of PTB and EPTB patient cohorts, population comparison cohorts, and sibling cohorts
Characteristics of sibling cohorts
A total of 1,990 siblings of PTB patients and 11,679 siblings of the PTB control cohort were identified. The PTB patients’ siblings had slightly increased comorbidity, including TB, and more were HIV-positive compared with the siblings of the population control cohort ().
Mortality in PTB patient population versus matched population controls
A total of 2,388 (37.3%) PTB patients and 4,683 (24.4%) PTB population controls died during the study period. A Kaplan–Meier survival curve for the PTB cohort and their population control cohort is shown in . An overall MRR of 1.86 (95% CI 1.77–1.96) was found for the PTB cohort ().
Figure 2 Kaplan–Meier survival curves.
Abbreviations: EPTB, extrapulmonary tuberculosis; PTB, pulmonary tuberculosis.
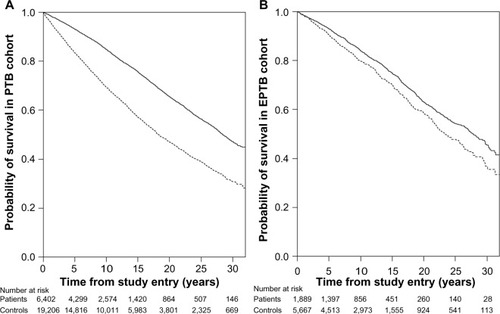
Table 2 All-cause mortality rate ratios in PTB and EPTB patients, population controls, and siblings, Denmark, 1977–2008
When stratified by individual risk factors, a higher mortality was found in the PTB cohort for males (MRR 2.04; 95% CI 1.92–2.17) compared with females (MRR 1.61; 95% CI 1.48–1.75). The MRR decreased with increasing age at time of TB diagnosis and the relative risk of death increased with increased comorbidity (). Danish-born PTB patients had a slightly higher risk of death (MRR 1.94; 95% CI 1.84–2.04) than immigrants (MRR 1.71; 95% CI 1.48–1.98).
The PTB patients had an increased risk of death from natural causes (infectious, malignant, respiratory, rheumatic, liver/pancreatic diseases, and diabetes) and also from unnatural causes of death (alcohol and drug abuse, injury, and poisoning; and ). The increased risk of malignant diseases in PTB patients was mainly driven by cancers of the respiratory tract, esophagus, breast, and hematologic system.
Table 3 Cause-specific mortality rate ratios in PTB and EPTB patients, population controls, and siblings, Denmark, 1977–2008
Mortality in EPTB patient population versus matched population controls
A total of 515 (27.3%) EPTB patients and 1,379 (24.3%) EPTB population controls died during the study period. A Kaplan–Meier survival curve for the EPTB cohort and their respective population control cohort is shown in . An overall MRR of 1.24 (95% CI 1.12–1.37) was found for the EPTB cohort (). When stratified by individual risk factors, the MRR was found to decrease with increasing age at time of TB diagnosis. Also, the MRR increased with higher levels of comorbidity. The relative risk of death was not found to differ significantly when data were stratified by sex and ethnicity. The EPTB patients had an increased risk of death due to infectious, gastrointestinal, and genitourinary diseases, diabetes, and gastrointestinal and hematologic neoplasms ( and ).
Mortality in PTB patient population versus their siblings
Compared with their respective siblings, the PTB patients had a significantly increased relative risk of death (MRR 3.55; 95% CI 2.57–4.91). In the stratified analyses we observed an increased risk of death in all subgroups (). As all siblings were born after January 1, 1952, for comparison we calculated MRR for PTB patients born in the same period compared with their respective control cohort (MRR 4.62; 95% CI 3.85–5.57). Compared with their siblings, the PTB patients were at increased risk of death from infectious diseases (MRR 10.56; 95% CI 2.33–47.83), malignant neoplasms (MRR 2.71; 95% CI 1.15–6.37), and cardiovascular, respiratory, and gastrointestinal diseases ().
Mortality in siblings of PTB patient population versus siblings of PTB control population
The siblings of the PTB patients had a more than twofold excess mortality compared with siblings of the PTB control cohort (), and this was not substantially reduced after exclusion of siblings with a history of TB (MRR 1.99; 95% CI 1.48–2.69), data not shown in tables. In the stratified analyses, an increased relative risk of death (MRR 2.45; 95% CI 1.76–3.40) was found for male siblings of PTB patients compared with male siblings of PTB controls.
Compared with siblings of the population controls, the siblings of the PTB patients had a significantly increased risk of death from infectious diseases (MRR 10.53; 95% CI 1.76–63.00), mental disorders, including alcohol and/or drug abuse (MRR 4.66; 95% CI 2.90–10.37), and gastrointestinal diseases (MRR 4.17; 95% CI 1.82–9.53, ).
Discussion
In this nationwide, population-based cohort study, we observed an almost two-fold increased long-term mortality in PTB patients compared with an age-matched and sex-matched population comparison cohort. Increased relative risk of death was mainly predicted by male sex, younger age, native citizenship, comorbidity, and HIV coinfection. Further, an increased mortality was observed in the siblings of PTB patients. An increased risk of death was also identified in EPTB patients, although smaller than for the PTB patients.
To our knowledge, this is the first study to investigate long-term mortality in TB patients in a nationwide, population-based, cohort study design including estimates of mortality in siblings of TB patients. Our study has several strengths. First, the centralized registration of TB patients in Denmark enabled us to identify a large cohort of TB patients over a more than 30-year period. Second, having a purely native Danish population control cohort excludes the possible confounding related to a mixed ethnic control cohort. Third, the high proportion of microbiologically verified TB cases minimized risk of misclassification. Fourth, the extracted data originated from Danish national registries with high coverage and long-term and complete follow-up, thus providing high validity. Finally, access to the Danish registries allowed us to generate well matched, population-based comparison cohorts and identify siblings of the patients and population comparison cohorts. We were not able to adjust for potential confounding from smoking, alcohol abuse, and socioeconomic factors which may partly explain the observed excess mortality. We did not have access to patient files and were therefore not able to account for clinical parameters and treatment regimes. Also, our results are derived from a high-income setting with a low incidence of TB and HIV, and may not be comparable with settings of developing nations with a high incidence of HIV and drug-resistant TB.
Several studies have identified age, male sex, comorbidity, diabetes, HIV, and native citizenship as risk factors for active TB and short-term mortality in TB patients.Citation19,Citation20 We identified the same factors, except age, to be risk factors for increased long-term relative risk of death. The relative risk of death was highest in the younger age categories which may seem counterintuitive, but reflects the fact that the absolute risk of death is highest in the older background population, and increased mortality in the older TB patients thereby leads to a minor impact on relative risk of death.
Both PTB and EPTB patients were at increased risk of death due to TB, which is in accordance with a study from the UK which found TB to be responsible for 21% of all deaths during a 14-year follow-up.Citation20 Both our cohorts were also at increased risk of death due to diabetes, a disease associated with not only an increased risk of TB but also increased mortality in TB patients; two retrospective US cohort studies both reported more than a six-fold increased mortality in diabetic TB patients compared with nondiabetic controls.Citation21,Citation22 With increasing use of biologic disease-modifying antirheumatic drugs, patients with rheumatic diseases are at increased risk of TB infection;Citation23 this is reflected in our results, with PTB patients exhibiting more than a two-fold increased risk of death due to underlying rheumatic disease.
The epidemiologic evidence that alcohol abuse and exposure to cigarette smoke increase the risk of active TB is strong.Citation24,Citation25 The prevalence of alcohol abuse disorders among TB patients in developed countries ranges from 10% to 50%,Citation26–Citation30 and it has been estimated that almost one third of Danish PTB patients suffer from alcohol abuse and one in ten from drug abuse.Citation31,Citation32 This is supported in our data on in-hospital admissions in the 5 years prior to TB diagnosis, where admissions linked to alcohol abuse were significantly more frequent among the PTB patients compared with population controls. Further, lower socioeconomic status is associated with active transmission of TB among native Danes.Citation33 We observed an increased risk of long-term mortality in PTB patients from chronic lung diseases and lung cancer, alcohol and drug abuse, and gastrointestinal diseases, particularly liver-related. Also, the risk of death was increased in the siblings of these patients. Our data thereby underlines the fact that conditions related to tobacco, alcohol and drug abuse, immune suppression, and socioeconomic factors are not only risk factors for contracting TB and short-term mortality, but also are main determinants of long-term mortality.
Compared with PTB patients, we observed only minor increased risk of death in the EPTB patients, which supports previous results of lower case fatality rates among patients with EPTB.Citation19 Also, the findings point toward less impact from tobacco, alcohol, and drug abuse.
We found a significantly increased risk of death due to malignant neoplasms in the PTB patient group compared with population controls. This excess mortality was primarily driven by an increased prevalence of deaths due to cancers of the airways, esophagus, breast and hematopoietic system. The majority of these subcategories have been strongly associated with smoking, alcohol abuse, and immunodeficiency.Citation34–Citation39 A recent population-based cohort study from Taiwan that included 5,657 TB patients and 23,984 controls found a statistically significant increased incidence of lung cancer in the years after TB infection (269 per 100,000 person-years) compared with population controls (153 per 100,000 person-years).Citation40
The siblings of the PTB patients were at markedly increased risk of death compared with the siblings of the population controls and appeared to be at increased risk of death due to infectious and gastrointestinal diseases and alcohol and drug abuse. This high excess mortality among the siblings of PTB patients indicates that the excess long-term mortality among PTB patients cannot solely be attributed to an effect of TB infection, but must also be influenced by other family-associated, behavioral, and/or socioeconomic-related factors. We presume that these associations are explained by the fact that alcohol and drug abuse clusters in families and also leads to increased risk of TB as well as death due to infectious and gastrointestinal diseases. However, the MRR of PTB patients born after January 1, 1952 was almost twice that of their siblings, indicating that specific risk factors are also present in the PTB patient cohort and increase their mortality, although part of this excess mortality can be reflected in the younger age of the siblings. Studies have shown that growing up in an environment of low socioeconomic status increases the risk of death later in life;Citation41,Citation42 hence, one explanation might be that the patients and siblings share the same low socioeconomic status during childhood and are thus at increased risk of death in adulthood. Genetic predisposition to death from infectious diseasesCitation43 has been proposed along with evidence of increased genetic host susceptibility to acquiring infectious diseases such as TB.Citation44–Citation47
Our study has several clinical implications. It emphasizes that, in high-income settings, PTB patients suffer from substantially increased long-term mortality compared with EPTB patients and compared with the background population. Furthermore, it establishes that classical risk factors for active TB and short-term mortality are also the main risk factors for long-term mortality, and that PTB patients are at a significantly increased risk of dying from conditions related to tobacco, alcohol, and drug abuse and immune suppression. The study underlines the importance of addressing lifestyle and socioeconomic risk factors to substantially reduce long-term mortality in PTB patients.
Supplementary materials
Detailed subcategorization of causes of death according to ICD-8 and ICD-10 diagnosis codes
The 18 categories of specific underlying causes of death were specified by the International Classification of Diseases, Eighth Revision (ICD-8), codes for the years 1977–1993 and the International Classification of Diseases, Tenth Revision (ICD-10), codes for 1994–2006. For infectious diseases, the codes were 000–134.99/A00–B99; cancer 140–209/C00–C96; blood/immune diseases 280–289.99/D50–D89; endocrine diseases 240–279.09/E00–E90; mental and behavioral disorders, including those due to psychoactive substance use and inebriation 290–315/F00–F99; nervous system diseases 320–358.09/G00–G99; diseases of the sensory organs 360–389.99/H00–H59; cardiovascular diseases 390–458.99/I00–I99; respiratory diseases 460–519.99/J00–J99; digestive system diseases 520–577.99/K00–K93; skin diseases 680–709.99/L00–L99; rheumatic diseases 710–738.09/M00–M99; genitourinary diseases 580–629.99/N00–N99; neonatal/congenital disorders 740–779.99/P00–Q99; pregnancy-related diseases 630–678.09/O00–O99; injury/poisoning 800–999/S00–T98, V, W, X, Y; ill-defined causes 780–796.99/R00–R99; and no cause of death reported.
Table S1 Detailed cause-specific mortality rate ratios in PTB and EPTB patients compared with population controls, Denmark, 1977–2008
Disclosure
The authors report no conflicts of interest in this work.
References
- World Health OrganizationGlobal Tuberculosis Control: WHO Report 2011 Available from: http://www.who.int/tb/publications/global_report/2011/gtbr11_full.pdfAccessed May 7, 2013
- LonnrothKJaramilloEWilliamsBGDyeCRaviglioneMDrivers of tuberculosis epidemics: the role of risk factors and social determinantsSoc Sci Med200968122240224619394122
- LienhardtCFieldingKSillahJSInvestigation of the risk factors for tuberculosis: a case-control study in three countries in West AfricaInt J Epidemiol200534491492315914505
- European Centre for Disease Prevention and Control Migrant HealthBackground note to the ECDC report on migration and infectious diseases in the EU72009 Available from: http://www.ecdc.europa.eu/en/publications/publications/0907_ter_migrant_health_background_note.pdfAccessed August 15, 2013
- Statens Serum Institut, Department of Infectious Disease EpidemiologyEpi-News No 49, 2011. Tuberculosis 2010 Part 1 Available from: http://www.ssi.dk/English/News/EPI-NEWS/2011/No%2049%20-%202011.aspxAccessed November 27, 2012
- Pablos-MendezASterlingTRFriedenTRThe relationship between delayed or incomplete treatment and all-cause mortality in patients with tuberculosisJAMA199627615122312288849749
- LefebvreNFalzonDRisk factors for death among tuberculosis cases: analysis of European surveillance dataEur Respir J20083161256126018515556
- StraetemansMGlaziouPBierrenbachALSismanidisCvan der WerfMJAssessing tuberculosis case fatality ratio: a meta-analysisPLoS One201166e2075521738585
- Denmark’s StatisticsPopulations and elections: population in Denmark Available from: http://www.statistikbanken.dk/statbank5a/default.asp?w=1600Accessed November 27, 2012
- Statens Serum Institut, Department of Infectious Disease EpidemiologyEpi-News No 50, 2009. Tuberculosis 2008 Part 1 Available from: http://www.ssi.dk/English/News/EPI-NEWS/~/media/Indhold/EN%20-%20engelsk/EPI-NEWS/2009/pdf/EPI-NEWS%20-%202009%20-%20No%2050.ashxAccessed November 27, 2012
- AndersenPHKamper-JorgensenZStenzFSoborgBVarious strategies for elimination of tuberculosisUgeskr Laeger201117312872875 Danish21419054
- LohseNHansenABJensen-FangelSDemographics of HIV-1 infection in Denmark: results from the Danish HIV Cohort StudyScand J Infect Dis200537533834316051569
- AndersenTFMadsenMJorgensenJMellemkjoerLOlsenJHThe Danish National Hospital Register. A valuable source of data for modern health sciencesDan Med Bull199946326326810421985
- FrankLEpidemiology. When an entire country is a cohortScience200028754622398239910766613
- JuelKHelweg-LarsenKThe Danish registers of causes of deathDan Med Bull199946435435710514943
- ChristensenASRoedCOmlandLHAndersenPHObelNAndersenABLong-term mortality in patients with tuberculous meningitis: a Danish nationwide cohort studyPLoS One2011611e2790022132165
- ChristensenKSchmidtMMVaethMOlsenJAbsence of an environmental effect on the recurrence of facial-cleft defectsN Engl J Med199533331611647791818
- CharlsonMEPompeiPAlesKLMacKenzieCRA new method of classifying prognostic comorbidity in longitudinal studies: development and validationJ Chronic Dis19874053733833558716
- AnyamaNBracebridgeSBlackCNiggebruggeAGriffinSJWhat happens to people diagnosed with tuberculosis? A population-based cohortEpidemiol Infect200713571069107617288641
- HorneDJHubbardRNaritaMFactors associated with mortality in patients with tuberculosisBMC Infect Dis20101025820799975
- DooleyKETangTGolubJEDormanSECroninWImpact of diabetes mellitus on treatment outcomes of patients with active tuberculosisAm J Trop Med Hyg200980463463919346391
- OurslerKKMooreRDBishaiWRSurvival of patients with pulmonary tuberculosis: clinical and molecular epidemiologic factorsClin Infect Dis200234675275911850859
- BrassardPKezouhASuissaSAntirheumatic drugs and the risk of tuberculosisClin Infect Dis200643671772216912945
- LonnrothKWilliamsBGStadlinSJaramilloEDyeCAlcohol use as a risk factor for tuberculosis – a systematic reviewBMC Public Health2008828918702821
- ShangSOrdwayDHenao-TamayoMCigarette smoke increases susceptibility to tuberculosis – evidence from in vivo and in vitro modelsJ Infect Dis201120391240124821357942
- BrudneyKDobkinJResurgent tuberculosis in New York City. Human immunodeficiency virus, homelessness, and the decline of tuberculosis control programsAm Rev Respir Dis199114447457491928942
- EnarsonDAWangJSDirksJMThe incidence of active tuberculosis in a large urban areaAm J Epidemiol19891296126812762786330
- LaiferGWidmerAFSimcockMTB in a low-incidence country: differences between new immigrants, foreign-born residents and native residentsAm J Med2007120435035617398230
- MilneRCAlcoholism and tuberculosis in VictoriaMed J Aust19702219559605493339
- PincockTAAlcoholism in tuberculosis patientsCan Med Assoc J19649185185414217248
- LillebaekTPoulsenSKok-JensenATuberculosis treatment in Denmark: treatment outcome for all Danish patients in 1992Int J Tuberc Lung Dis19993760361210423223
- AndersenRMBjorn-PraestSOGradelKONielsenCNielsenHIEpidemiology, diagnostic delay and outcome of tuberculosis in North Jutland, DenmarkDan Med Bull2011583A425621371406
- Kamper-JorgensenZAndersenABKok-JensenAClustered tuberculosis in a low-burden country: nationwide genotyping through 15 yearsJ Clin Microbiol20125082660266722675129
- RodriguezTAltieriAChatenoudLRisk factors for oral and pharyngeal cancer in young adultsOral Oncol200440220721314693246
- KreuzerMKreienbrockLGerkenMRisk factors for lung cancer in young adultsAm J Epidemiol199814711102810379620046
- XueFWillettWCRosnerBAHankinsonSEMichelsKBCigarette smoking and the incidence of breast cancerArch Intern Med2011171212513321263102
- SandlerDPShoreDLAndersonJRCigarette smoking and risk of acute leukemia: associations with morphology and cytogenetic abnormalities in bone marrowJ Natl Cancer Inst199385241994038246285
- ThomasXChelghoumYCigarette smoking and acute leukemiaLeuk Lymphoma20044561103110915359988
- FranceschiSTalaminiRBarraSSmoking and drinking in relation to cancers of the oral cavity, pharynx, larynx, and esophagus in northern ItalyCancer Res19905020650265072208109
- WuCYHuHYPuCYPulmonary tuberculosis increases the risk of lung cancer: a population-based cohort studyCancer2011117361862420886634
- GalloVMackenbachJPEzzatiMSocial inequalities and mortality in Europe – results from a large multi-national cohortPLoS One201277e3901322848347
- StrandBHGroholtEKSteingrimsdottirOAEducational inequalities in mortality over four decades in Norway: prospective study of middle aged men and women followed for cause specific mortality, 1960–2000BMJ2010340c65420179132
- ObelNChristensenKPetersenISorensenTISkyttheAGenetic and environmental influences on risk of death due to infections assessed in Danish twins, 1943–2001Am J Epidemiol201017191007101320375195
- StorgaardMVarmingKHerlinTObelNNovel mutation in the interferon-gamma-receptor gene and susceptibility to mycobacterial infectionsScand J Immunol200664213713916867158
- BaghdadiJEOrlovaMAlterAAn autosomal dominant major gene confers predisposition to pulmonary tuberculosis in adultsJ Exp Med200620371679168416801399
- Motsinger-ReifAAAntasPROkiNOPolymorphisms in IL1-beta, vitamin D receptor Fok1, and Toll-like receptor 2 are associated with extrapulmonary tuberculosisBMC Med Genet2010113720196868
- GaoLTaoYZhangLJinQVitamin D receptor genetic polymorphisms and tuberculosis: updated systematic review and meta-analysisInt J Tuberc Lung Dis2010141152320003690