
Abstract
Aim of the database
The aim of the Danish Adult Diabetes Registry (DADR) is to provide data from both the primary health care sector (general practice [GP]) and the secondary sector (specialized outpatient clinics) to assess the quality of treatment given to patients with diabetes. The indicators represent process and outcome indicators selected from the literature.
Study population
The total diabetes population in Denmark is estimated to be ~300,000 adult diabetes patients. Approximately 10% have type 1 diabetes, which is managed mainly in the secondary sector, and 90% have type 2 diabetes with the majority (80%) being treated in primary health care. In 2014, DADR included data from a total of 70,826 patients.
Main variables
The following variables are assessed: date of analysis as well as the outcome for hemoglobin A1c, blood pressure, lipids, urinary albumin–creatinine ratio, smoking status, glucose-, blood pressure-, and lipid-lowering treatment (yes/no), insulin pump treatment (yes/no), and date of last eye and foot examination.
Descriptive data
In 2014, the annual report included data regarding over 38,000 patients from outpatient clinics, which is assumed to have included almost all patients in this setting, and >32,000 from GPs, reflecting improved but still limited coverage from this setting. The annual results are published in a compiled report of Danish Diabetes Care, which included DADR, data from the pediatric diabetes database, and the national ophthalmological diabetes database. The annual report is published, which included data on national, regional, and local level (individual outpatient clinics and corresponding GPs). This allows a comprehensive overview of diabetes care in Denmark.
Conclusion
The database covers an increasing fraction of patients with diabetes in Denmark, and the structure for full coverage is in place. Annual reporting has helped to ensure focus on the quality of diabetes treatment in the primary and secondary health care. Furthermore, it is an important resource for Danish register-based diabetes research.
Background
Diabetes is a widespread chronic disease with >300,000 patients in Denmark. Approximately 10% have type 1 diabetes, which is managed primarily in outpatient clinics, and 90% have type 2 diabetes, among whom the majority (80%) are treated in primary health care.
The treatment has evolved in recent decades, with better options for education, self-care, and individualized insulin treatment with pens and pumps, focus on multifactorial intervention including lifestyle modification, and control of glucose, blood pressure, and lipids. As a result, the prognosis for patients has improved considerably regarding the development of micro- and macrovascular complications and survival.Citation1–Citation5 Structured care with regular screening for complications and targeted intervention has been important for this development.
Aim
Quality monitoring is necessary to ensure that patients with type 1 and type 2 diabetes in Denmark benefit from current improvements in care, and are treated according to nationally agreed treatment guidelines. The aim of the Danish Adult Diabetes Registry (DADR) (initially The National Indicator Project for Diabetes) is to provide data from both the primary health care sector (general practice [GP]) and the secondary sector (specialized outpatient clinics) to assess the quality of treatment given to patients with diabetes, with respect to selected well-documented and treatment-relevant process and result indicators. The registry has published an annual report since 2005.
Study population
All diabetes outpatient clinics have had an obligation to report to the database since 2004, data from the GPs were included from 2006, and inclusion became mandatory from 2014. The reporting is done through various information technology systems ranging from manual data entry from paper records to automated data capture from electronic patient records.
As >80% of patients with type 2 diabetes are taken care of by GPs, the reporting from primary care to the DADR has been a very important and unique feature, compared to most other registries relying on secondary health care data.
Main variables and quality indicators
National evidence-based guidelines for treatment and control have been developed to guide clinicians toward optimal treatment for all patients.Citation6,Citation7 Furthermore, disease management programs, defined as the total cross-disciplinary, multisectoral, and coordinated health care services for a given chronic condition, have been evolved to create a framework that ensures the application of evidence-based recommendations for health care intervention, including a precise description of tasks and coordination between all parties involved.
To ensure the indicators are perceived as relevant and meaningful for reporting GPs and hospital units, indicators have been selected for quality assessment, covering aspects of cardiometabolic control and complication-screening activity. To reduce burden of reporting results, the number of variables initially had to be limited. Selection of indicators has been based on the following criteria: 1) a strong association with disease progression and prognosis, 2) standardized measurability, and 3) comparability across reporting units. Consequently, indicators of, for example, lifestyle, such as diet and physical activity, have so far been opted out, due to lack of a standardized tool for monitoring in clinical practice. Besides basic information on age, sex, and year of diabetes diagnosis, the following variables are reported annually to the DADR: glycated hemoglobin A1c (HbA1c), blood pressure, lipids, urinary albumin–creatinine ratio, estimated glomerular filtration rate, body mass index, smoking status, glucose-, blood pressure-, and lipid-lowering treatment (yes/no), insulin pump treatment (yes/no), date of last eye examination result known by the treating physician, and date of last foot examination. For each indicator, the steering committee for the database has agreed on a standard that the program should aim to reach. and present the development in completeness over time for selected variables.
Figure 1 Change in completeness for reporting of HbA1c values over time.
Abbreviations: HbA1c, hemoglobin A1c; GP, general practice.
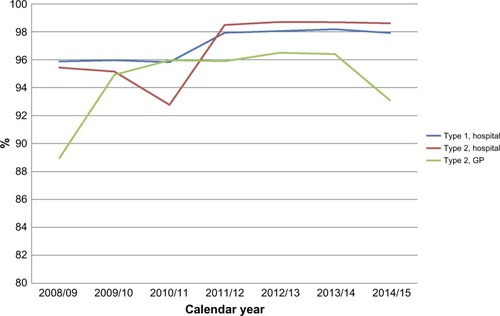
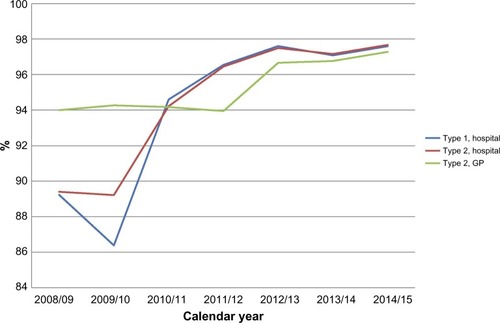
Figure 2 Change in completeness for reporting of smoking habits over time.
Abbreviation: GP, general practice.
Derived process indicators and standards include:
Annual measurement of HbA1c with a standardized method in 95% of patients
Annual measurement of blood pressure in 95% of patients
Measurement of lipids every second year in 90% of patients
Foot examination in 95% of patients within 2 years
Examination of urinary albumin–creatinine ratio in 95% of patients within 2 years
Eye examination within a 2-year period in 90% of patients and within a 4-year period in 95% of patients
Prescribed antidiabetic treatment among patients with HbA1c ≥53 mmol/mol (no standard decided upon yet)
Prescribed antihyptertensive treatment among patients with blood pressure ≥140/90 mmHg (standard 80%)
Prescribed lipid-lowering medication among patients with low-density lipoprotein cholesterol >2.5 mmol/L (no standard decided upon yet)
Prescribed renin–angiotensin system blockade among patients with micro- or macroalbuminuria (no standard decided upon yet)
In the annual report, the indicators are presented separately for primary and secondary health care on a national, regional, and local level (with primary care data shown for clusters referring to the same outpatient clinic). In addition, each outpatient clinic or GP has access to their own quality data. This allows a comprehensive overview of diabetes care in Denmark. presents an example of the data.
Table 1 Foot examination within a 2-year period
Follow-up
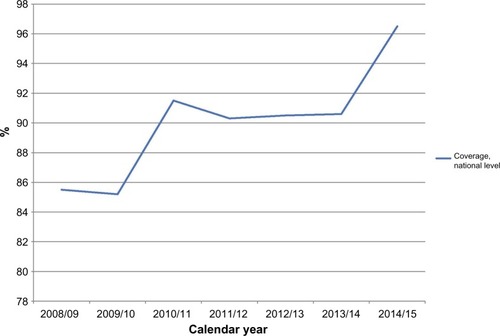
It is an ongoing focus to ensure valid data. Validity is evaluated and discussed on regional and national audits, and when compared to other registries of patients in outpatient clinics in Denmark, it is estimated that the data coverage is 97% in 2014. , , and presents the development over time. Particularly in the beginning of the project, it has been a challenge. Currently, it is estimated that data completeness from the outpatient clinics, matching data to the administrative data in the Danish National Patient Register on all hospital contacts, is up to 95%. Furthermore, the setup has proved to be able to capture data from all outpatient clinics, and all GPs. Approximately 10% of the data are entered manually into a data system, whereas the remaining 90% are captured directly from the electronic medical record systems, which minimize risk of data entry errors.
Figure 3 Coverage of the diabetes register over time for patients in outpatient clinics in secondary care.
Unfortunately, uncertainty regarding data security and database approvals has stopped delivery of data from the GPs since September 2014, affecting primarily completeness of data regarding type 2 diabetes.
The annual 2014 report included data regarding over 38,000 patients from outpatient clinics, which is assumed to have included almost all patients in this setting, and >32,000 from GPs (collected before September 2014). The annual results are published in a compiled report of Danish Diabetes Care, which included DADR, data from the pediatric diabetes database, and the national ophthalmological diabetes database.Citation1
The reported results are discussed at annual meetings. At the national audit, the indicators and standards for good clinical practice and care for patients with diabetes are discussed, and recommendations are agreed upon. In case of outlier results, local audit is recommended. The final report, including recommendations for improvement, is published online at https://www.sundhed.dk.Citation8
Use of the database for research
The nationwide reporting of unbiased, valid, and standardized information to the registry makes it attractive for research purposes. The unique Danish personal identification number allows linkage at the individual level of the database with other Danish registers, for example, the National Patient Register and the cause of death register, offering opportunities to study differences in treatment and control across geographical and other specified subpopulations. For example, the DADR has been used for follow-up of the Danish Centre for Strategic Research in Type 2 Diabetes (DD2) cohort for information about prescription of antidiabetic therapies in newly diagnosed diabetes.Citation9 Another epidemiological study has linked information from the DADR with information from the Danish Civil Registration System on country of origin. In a research field where longitudinal data were lacking, this study demonstrated a higher incidence of most micro- and macrovascular complications among migrants with diabetes from Sub-Saharan Africa, Middle East, and Asia compared to Danish born. These ethnic differences persisted after adjustment for a wide range of confounders, including HbA1c, blood pressure, lipids, body mass index, smoking, diabetes duration, age, and sex.Citation10
The number of published studies based on the registry is still limited, probably reflecting initial concerns about data validity and coverage. As these concerns have been resolved, there has been a steady increase in applications for data, and as the coverage of the patient population and duration of follow-up increases, the database will provide a valuable data source for Danish register-based diabetes research.
Administrative issues and funding
During the past decade, reporting has been increasingly automated and valid. However as mentioned, a recent discussion on data protection agreements has stopped data delivery from GPs. As the majority of patients are seen by GPs, an overview of diabetes care in Denmark will be far from complete without these data, so it is crucial that data will soon again be reported.
The registry is funded by the Danish Regions and administered by the Danish Clinical Registries (Regionernes Kliniske Kvalitetsudviklings Program) that constitute the infrastructure of the national clinical quality databases in Denmark.
The registry is run by a steering committee with representatives both from the secondary and the primary sector from the five regions, and from the Danish Diabetes Association.
Conclusion
The database has helped significantly to ensure the quality of diabetes treatment in the primary and secondary health care sector in Denmark and can continue to do so if data from the GPs are included again. Furthermore, it is an important resource for Danish register-based diabetes research.
Acknowledgments
This paper was funded by the Program for Clinical Research Infrastructure established by the Lundbeck Foundation and the Novo Nordisk Foundation and administered by the Danish Regions.
Disclosure
The authors report no conflicts of interest in this work.
References
- GaedePLund-AndersenHParvingHHPedersenOEffect of a multifactorial intervention on mortality in type 2 diabetesN Engl J Med2008358658059118256393
- AndresdottirGJensenMLCarstensenBImproved survival and renal prognosis of patients with type 2 diabetes and nephropathy with improved control of risk factorsDiabetes Care20143761660166724623028
- FaerchKCarstensenBAlmdalTPJorgensenMEImproved survival among patients with complicated type 2 diabetes in Denmark: a prospective study (2002–2010)J Clin Endocrinol Metab2014994E642E64624483155
- JorgensenMEAlmdalTPCarstensenBTime trends in mortality rates in type 1 diabetes from 2002 to 2011Diabetologia201356112401240423949580
- JorgensenMEAlmdalTPFaerchKReduced incidence of lower-extremity amputations in a Danish diabetes population from 2000 to 2011Diabet Med201431444344724111834
- Dansk Selskab for Almen Medicin: Type 2 diabetes - et metabolisk syndromDenmark2012 Available from: http://vejledninger.dsam.dk/type2/Accessed March 7, 2016 Danish
- Dansk Endokrinologisk Selskab: Type 1 diabetes mellitusCopenhagen2014 Available from: http://endocrinology.dk/index.php/nbvhovedmenu/1-diabetes-mellitus/3-type-1-diabetes-mellitusAccessed March 7, 2016 Danish
- Danish Diabetes Database, national annual report 2014–15 Available from: https://www.sundhed.dk/content/cms/87/4687_kom_%C3%A5rsrapport_diabetes_2014_15_27082015_endelig.pdfAccessed March 7, 2016
- AndersenGSJørgensenMESøbergSEthnicity, migration and T2DM [Internet]Diapedia2015 Available from: http://dx.doi.org/10.14496/dia.3104465162.16Accessed March 7, 2016
- MorABerencsiKSvenssonEPrescribing practices and clinical predictors of glucose-lowering therapy within the first year in people with newly diagnosed Type 2 diabetesDiabet Med201532121546155426032247