
Abstract
Follicular lymphoma (FL) is the second most common type of non-Hodgkin’s lymphoma. FL is an incurable disease with treatment options ranging from a “watch-and-wait” approach to localized therapy with radiation or systemic therapy with rituximab in combination with chemotherapy regimens. This review summarizes the role of rituximab across the spectrum of FL treatment and the evolving therapeutic landscape with the emergence of novel agents currently in clinical development. Despite the prospect of new agents on the horizon, it is widely accepted that rituximab will remain as the cornerstone of therapy because of its established long-term efficacy. Many biologics, including rituximab, have lost exclusivity of composition-of-matter patent or will do so in the next few years, which is a concern for patients and physicians alike. Moreover, access to rituximab is challenging, particularly in countries with restricted resources. Together, these concerns have fueled the development of safe and effective biosimilars. The term “biosimilar” refers to a biologic product that is highly similar to an approved reference (or originator) product, notwithstanding minor differences in clinically inactive components, and for which there are no clinically meaningful differences in purity, potency, or safety. Biosimilars are developed to treat the same condition(s) using the same treatment regimens as an approved reference biologic, and have the potential to increase access to more affordable treatment of FL. Herein, we also discuss the potential benefits of eagerly awaited rituximab biosimilars, which may mitigate the impact of the lack of access to rituximab.
Introduction
Non-Hodgkin’s lymphoma (NHL) accounts for approximately 3%–4% of all cancers worldwide.Citation1 NHL is a growing problem, with the global prevalence projected to rise to more than 0.4 million in 2016, and estimates suggest that approximately half of new NHL cases will result in death.Citation2
Follicular lymphoma (FL) is the second most common type of NHL and accounts for 10%–20% of all lymphomas.Citation3 The most ubiquitous indolent lymphoma, FL is typically diagnosed in individuals 55–60 years of age and is slightly more prevalent in females.Citation3 FL is characterized by painless swelling in several lymph node sites, with bone marrow involvement in approximately 70% of cases.Citation4 Approximately 19% of patients present with “B symptoms”, such as fever, weight loss, or night sweats, at the time of diagnosis.Citation3,Citation4 FL predominantly originates from B lymphocytes. CD20 is a B-cell-specific antigen expressed on both malignant B cells, including FL and healthy cells, and is involved in the proliferation and differentiation of normal B cells.Citation5 As such, targeting CD20 is an optimal therapeutic strategy and plays a central role in the treatment of FL.
Rituximab (Rituxan®; Genentech, South San Francisco, CA, USA/MabThera®; Roche, Basel, Switzerland) is a chimeric anti-CD20 monoclonal antibody that binds specifically to CD20.Citation6,Citation7 In addition to its role in the treatment of diffuse large B-cell lymphoma (DLBCL) in the first-line or relapsed/refractory settings, rituximab is also approved for use in FL as a single agent or in combination with first-line chemotherapy.Citation6,Citation7 Given the importance of rituximab across the spectrum of FL treatment and the evolving therapeutic landscape with the emergence of novel agents, the role of rituximab in the future management of FL is described. The role of rituximab biosimilars in the future of FL treatment and how the introduction of biosimilars can help to relieve this lack of access are also discussed.
FL: the role of rituximab in the current standard of care
The National Comprehensive Cancer Network (NCCN)Citation8 () and the European Society for Medical Oncology (ESMO) guidelinesCitation9 () outline the recommended treatment regimens for patients with FL in the US and Europe, respectively. Owing to its established long-term efficacy, rituximab is an important component of FL treatment.Citation10
Table 1 Current standard of care in Grade 1–2 follicular lymphoma: NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) 2017Citation8
Figure 1 Current standard of care in follicular lymphoma: ESMO guidelines 2014.
Abbreviations: ESMO, European Society for Medical Oncology; RB, rituximab plus bendamustine; R-CHOP, rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone; R-CVP, rituximab plus cyclophosphamide, vincristine, and prednisone.
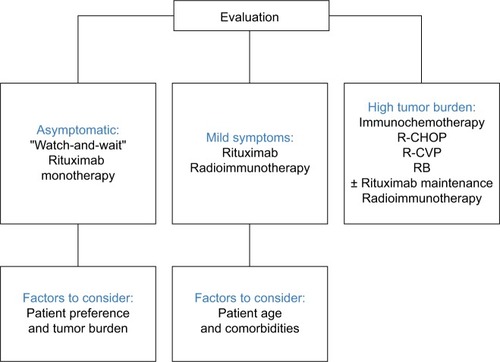
Treatment options for patients with limited-stage disease (stage I/II) include radiation,Citation11–Citation13 “watch-and-wait” approach,Citation14 or rituximab alone or in combination with chemotherapy (eg, bendamustine plus rituximab [BR]; rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone [R-CHOP]; or rituximab plus cyclophosphamide, vincristine, and prednisone [R-CVP]).Citation15 Despite the paucity of randomized clinical trials, radiation therapy is the preferred treatment for patients with non-bulky stage I FL. Patients with Grade 3b FL or those undergoing histologic transformation are best treated with chemoimmunotherapy regimens, such as R-CHOP. Patients with stage II FL are appropriate candidates for treatment with either rituximab alone or in combination with chemotherapy, depending on their clinical presentation. In general, the treatment approach for patients with stage II FL includes “watch-and-wait”, single-agent rituximab vs rituximab plus chemotherapy, or radiation for those with contiguous nodal involvement. Patients with bulky disease or those with an adverse prognosis presenting with B symptoms and/or clinically significant tumor load are candidates for treatment with rituximab plus chemotherapy.Citation8,Citation9
Treatment options for patients with advanced-stage (stage III/IV) FL are similar to those for stage II FL. For asymptomatic patients with non-bulky disease, the watch- and-wait approach with treatment upon disease progression may be appropriate.Citation16 Results from a study by Ardeshna et al conducted in asymptomatic patients with advanced-stage low-tumor-burden FL showed that 88% of patients on maintenance treatment with rituximab did not require treatment at 3 years compared with 46% in the watch-and-wait group (P<0.0001).Citation15 The rituximab induction arm was affected by early closure because of poor accrual. Moreover, there were 18 serious adverse events, possibly as a consequence of treatment with rituximab. However, this study highlights that rituximab monotherapy is a possible option for patients with asymptomatic, low-tumor-burden FL, particularly for those who may not tolerate chemotherapy or for those with slowly progressive disease.Citation8
Patients with advanced-stage FL that is progressive, symptomatic, and/or has associated cytopenias are candidates for chemoimmunotherapy. The choice of chemotherapy agents depends on the drug availability and physician choice. Common treatment regimens include BR, R-CHOP, and R-CVP. Recent evidence suggests that BR is effective as a first-line regimen in patients with advanced disease. In a randomized Phase III study, treatment with BR resulted in non-inferior clinical response compared with standard rituximab chemotherapy (R-CHOP or R-CVP), with an acceptable toxicity profile.Citation17 In a prospective, randomized, open-label study in patients with previously untreated indolent lymphoma, first-line therapy with BR resulted in greater progression-free survival and fewer toxic effects compared with R-CHOP.Citation18
Patients who respond to induction treatment with R-CVP or R-CHOP are potential candidates for maintenance therapy with rituximab. Primary RItuximab and MAintenance (PRIMA) was a randomized open-label study to investigate the effect of 2 years of rituximab maintenance therapy (375 mg/m2 every 8 weeks) after first-line treatment with rituximab plus chemotherapy.Citation19 At a median follow-up of 3 years, progression-free survival was significantly improved in the rituximab maintenance group (75%) compared with the observation group (58%) (P<0.0001). Furthermore, a significantly greater proportion of patients achieved a complete response with rituximab maintenance therapy than those in the observation group (72% vs 52%, respectively; P=0.0001). However, there was no difference in the overall survival between the 2 groups in this study.Citation19 Further investigation is needed to understand the long-term toxicities of rituximab maintenance therapy and to identify the patients most likely to benefit from this treatment regimen.
A recent study by Kahl et alCitation20 failed to demonstrate a significant clinical benefit from continuing rituximab maintenance treatment in patients with advanced-stage, low-tumor-burden FL after induction with the single-agent rituximab. Although rituximab maintenance therapy should be considered after rituximab plus chemotherapy, it is not recommended after rituximab monotherapy (; ). Furthermore, rituximab maintenance therapy after induction with rituximab monotherapy is of less clinical benefit in patients with low-tumor-burden FL, compared with rituximab re-treatment.Citation20
Rituximab is also effective in the re-treatment setting and is used in combination with chemotherapy regimens for the treatment of relapsed/refractory FL. Common chemotherapy regimens include first-line (BR, R-CHOP, and R-CVP) and second-line (fludarabine, cyclophosphamide plus mitoxantrone or fludarabine monotherapy) regimens (). In patients with early relapse (1–2 years), a non-cross-resistant regimen is preferable (eg, bendamustine before or after CHOP). If patients subsequently experience remission for 6 months, the addition of rituximab should be considered ().Citation8
Novel agents on the horizon: the evolving treatment landscape of FL
Following the clinical success of rituximab in the treatment of FL, novel agents are emerging and currently under development. Ibrutinib, an oral, selective, and covalent Bruton’s tyrosine kinase inhibitor, has been approved by the US Food and Drug Administration (FDA) for the treatment of patients with mantle cell lymphoma who have received at least 1 prior therapy,Citation21 chronic lymphocytic leukemia (CLL)/small lymphocytic lymphoma, and Waldenström’s macroglobulinemia.Citation22 Ibrutinib has also been approved by the European Medicines Agency (EMA) for the treatment of patients with relapsed/refractory mantle cell lymphoma, in the first-line, refractory, and relapsed/refractory settings of CLL, for those with Waldenström’s macroglobulinemia who have received at least 1 prior therapy, and in the first-line setting for patients unsuitable for chemoimmunotherapy. Citation23 Ibrutinib has shown promising results in the treatment of FL. Ibrutinib is currently under investigation for use in combination with rituximab (ClinicalTrials.gov, NCT01980654) and as monotherapy for relapsed/refractory FL (ClinicalTrials.gov, NCT01849263).
Idelalisib, an oral phosphoinositide 3-kinase-delta inhibitor, has been approved by the FDA for the treatment of patients with relapsed/refractory CLL and relapsed/refractory FL.Citation24 A Phase I/II study to evaluate the efficacy and safety of idelalisib in patients with previously treated low-grade FL is ongoing (ClinicalTrials.gov, NCT01306643). A Phase II study is planned to explore the efficacy and safety of idelalisib in combination with rituximab in patients with previously untreated FL and small lymphocytic lymphoma (ClinicalTrials.gov, NCT02258529).
Obinutuzumab is a humanized immunoglobulin G1 monoclonal antibody, with a novel glycoengineered Fc region. In combination with chemotherapy, obinutuzumab has been approved by the FDA for the treatment of CLL. Obinutuzumab is approved for use in combination with bendamustine followed by obinutuzumab monotherapy for the treatment of patients with FL who relapsed after, or are refractory to, a rituximab-containing regimen.Citation25 Approval was based on an open-label, randomized, Phase III trial in patients with indolent NHL refractory to rituximab.Citation26 In another study, obinutuzumab demonstrated clinical efficacy and an acceptable safety profile in the relapsed/refractory FL setting.Citation27 In a Phase III study, obinutuzumab-based induction and maintenance therapy resulted in small improvements in progressionfree survival in treatment-naïve patients with FL; however, a higher incidence of Grades 3–5 adverse events was observed compared with rituximab.Citation28 A Phase I study in patients with NHL or CLL showed that induction and maintenance therapy with obinutuzumab offered clinical benefits, with a favorable safety profile.Citation29 Similarly, obinutuzumab showed encouraging results in patients with relapsed/refractory NHL.Citation30
Lenalidomide, an immunomodulatory agent, has been approved by the FDA for the treatment of patients with multiple myeloma, myelodysplastic syndromes, and relapsed/refractory mantle cell lymphoma.Citation31 In a Phase II trial, lenalidomide in combination with rituximab was effective and well tolerated as initial treatment for patients with advanced indolent NHL.Citation32 In light of these promising results, a Phase III study to evaluate the efficacy and safety of rituximab in combination with lenalidomide compared with R-CHOP, R-CVP, or BR in patients with previously untreated FL is ongoing (ClinicalTrials.gov, NCT01476787).
Rituximab: challenges for the future
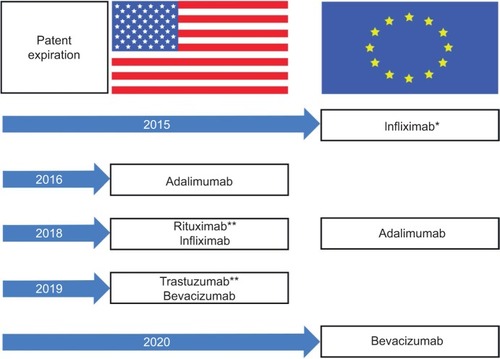
Despite an array of novel agents emerging and in clinical development, it is likely that rituximab will remain at the forefront of FL treatment.Citation33 However, patents for many biologics have expired or will lose exclusivity over the coming years (). Importantly, the composition-of-matter patent covering rituximab in Europe (MabThera®) expired in 2013, and its counterpart in the US (Rituxan®) will expire in 2018. Moreover, rituximab is not widely available to physicians and patients in several countries, including the US, Mexico, Turkey, Russia, and Brazil. In a recent survey of 450 oncologists and hematologists, 31% considered rituximab an easily accessible option in Brazil. Similarly, 25% and 19% reported challenges in getting access to rituximab in Mexico and Russia, respectively. Issues related to insurance coverage, treatment guidelines, and patient comorbidities were the most common barriers to access or use of rituximab. Indeed, these barriers have the potential to compromise clinical outcomes and patient care across the spectrum of FL treatment, potentially resulting in a change or delay in treatment with rituximab, largely the result of payment issues or patient response. However, Baer et al found physicians who participated in the survey would increase use of rituximab if a more affordable version were available, without compromising efficacy, safety, or patient care.Citation34
Figure 2 Patent expiration of biologics in the US and Europe.
Another concern in the biologics arena is that these agents are likely to be susceptible to drug shortages as a consequence of sparse active ingredients, coupled with obstacles in manufacture and supply. In addition, suboptimal compliance with current good manufacturing practice, changes in clinical standards, a greater demand for rituximab, and manufacturing delays are the most common factors that contribute to drug shortages.Citation35 The supply of chemotherapeutics, such as 5-fluorouracil, liposomal doxorubicin, and fludarabine, as well as rituximab, may be adversely affected by looming drug shortages, with potentially pernicious outcomes for patients.Citation36 Drug shortages can lead to delays in treatment, use of alternative, potentially less effective treatment, increased case management for health care professionals, and poor availability of more effective, well-tolerated combination therapies.Citation35
What’s next? The rationale for developing biosimilars
The loss of exclusivity and limited access to rituximab has led to the development of well-characterized, safe, and effective biosimilars to rituximab. Biosimilars are defined as biologic products that are highly similar to the reference biologic product, notwithstanding minor differences in clinically inactive components.Citation37 The availability of biosimilars may mitigate the impact of the limited access to rituximab. Biosimilars provide a greater spectrum of treatment choices and may offer efficiencies to the health care system. In addition, biosimilars increase access to biologics and foster greater use of biologic therapies, which may facilitate improved overall health outcomes at a time when a shortage of biologics may become a barrier to the treatment of patients with FL. Biosimilars have the potential to increase access to therapies by offering more affordable treatment options. Savings with biosimilars could facilitate the reallocation of expenditure to optimize treatment of patients with FL, resulting in patients receiving treatment earlier in therapy, with more patients able to access medicines such as rituximab.Citation37
Understanding biosimilars: an overview of development and pathways to approval
Biosimilars are large, structurally complex molecules developed to be similar to and treat the same condition(s), using the same treatment regimens as an existing licensed or approved (originator or reference) biologic. Development of biosimilars involves a stepwise approach of physicochemical and biological evaluation, along with a series of comparative nonclinical and clinical studies. Several factors influence the extent of clinical data required for the approval of biosimilars, including the similarity to the originator biologic and strength of preclinical data as well as the molecular complexity. The ultimate aim of biosimilar development is to demonstrate that there are no clinically meaningful differences based on the “totality of evidence” encompassing all available analytical, nonclinical, and clinical data. The totality of evidence approach is specifically tailored for biosimilars and applies a different paradigm than the regulation of originator biologics, for which the aim is to establish de novo efficacy and safety. Furthermore, the biosimilar developer is not required to demonstrate efficacy to the reference biologic in each indication, as the extrapolation of clinical data across indications is permitted, and any differences may be considered in the totality of evidence, given appropriate scientific justification.Citation38
The approval of biosimilars is a highly regulated and comprehensive process (). The EMA and the US FDA have published extensive guidance documents with their respective definitions of biosimilars, and the requirement of a series of detailed analytical and similarity assessments, nonclinical in vivo evaluation, and safety and efficacy studies, all in comparison with the reference biologic.Citation38,Citation39
Table 2 Regulatory definitions of biosimilars
The biosimilars approval pathway was established in the European Union (EU), with 8 biosimilars (under 20 different trade names) authorized by the EMA over the past decade.Citation40 The first biosimilar in the US (filgrastim-sndz [Zarxio®]), a biosimilar version of Neupogen®, was granted approval in 2015 under the US Biologics Price Competition and Innovation Act of 2009.Citation41,Citation42 Although complex, the regulatory approval process for biosimilars in Europe,Citation39 the US,Citation38 and elsewhereCitation43 has been tailored and is often shorter than that required for originator biologics.
The advent of rituximab biosimilars: where are we now?
A biosimilar version of rituximab (Truxima™) has recently been granted approval for the treatment of NHL, CLL, and rheumatoid arthritis (RA) in South Korea.Citation44 Several potential rituximab biosimilars are currently in development, each in comparison with the originator (reference) rituximab (). A study in patients with newly diagnosed advanced FL showed pharmacokinetic similarity between a potential biosimilar to rituximab, CT-P10, and rituximab (each administered with CVP), with similar B-cell kinetics and immunogenicity.Citation45 In another study, CT-P10 and rituximab showed equivalent pharmacokinetics, and comparable efficacy, pharmacodynamics, immunogenicity, and safety in patients with RA.Citation46 A clinical study in patients with previously untreated FL showed therapeutic equivalence in overall response rate between another proposed biosimilar to rituximab, GP-2013, and rituximab sourced from the EU. In this trial, similarity was demonstrated for efficacy, pharmacokinetic, and pharmacodynamic parameters, with similar safety findings.Citation47 In addition, the efficacy and safety of another potential biosimilar, BI-695500, in patients with low-tumor-burden lymphoma is under clinical investigation (ClinicalTrials.gov, NCT01950273). ABP 798, a potential biosimilar to rituximab, is in clinical development in patients with CD20-positive B-cell NHL (ClinicalTrials.gov, NCT02747043). Another potential biosimilar to rituximab, MabionCD20, is in development in patients with CD20-positive DLBCL (ClinicalTrials.gov, NCT02617485).
Table 3 Rituximab biosimilars in clinical development for NHL
In nonclinical studies, PF-05280586, a proposed bio-similar to rituximab, showed the same primary amino acid sequence and similar physicochemical and in vitro functional properties as the licensed originator biologic.Citation48 A study in patients with active RA demonstrated pharmacokinetic similarity of PF-05280586 to rituximab sourced from the EU (rituximab-EU) and the US (rituximab-US) and that of rituximab-EU to rituximab-US.Citation49 In this trial, all 3 treatments were generally well tolerated, and the incidence of treatment-related adverse events was low. These encouraging findings support the ongoing development of PF-05280586 as a potential biosimilar to rituximab. A trial is ongoing to compare the efficacy, safety, pharmacokinetics, and immunogenicity of PF-05280586 to rituximab in patients with low-tumor-burden FL (ClinicalTrials.gov, NCT02213263).
Conclusion
FL accounts for up to 20% of all lymphomas. Debate continues over the optimal treatment strategy for untreated FL: the watch- and-wait approach vs therapeutic intervention. However, for patients who are candidates for systemic therapy, an anti-CD20 monoclonal antibody alone or in combination with chemotherapy remains at the forefront of the therapeutic landscape.
It is well recognized that rituximab will remain as the cornerstone of therapy in the treatment of patients with FL. The loss of exclusivity of composition-of-matter patents of biologics in recent and coming years, and the lack of access to rituximab in some countries are of particular concern for patients and physicians. Thus, it is relevant, appropriate, and necessary to develop a biosimilar to rituximab with the potential to generate cost savings and efficiencies for health care systems and to increase access to patients worldwide, which can help augment resources for other important aspects of health care.
It will be crucial to engage clinicians on the importance of biosimilars, and moreover, to increase understanding of data that underpin the development of biosimilars and how these data may translate into clinical practice. At present, several potential rituximab biosimilars are in development. As a result of extensive studies, the availability of safe and effective rituximab biosimilars is eagerly anticipated, potentially offering a greater range of therapeutic options and improved clinical benefits to patients with FL.
Acknowledgments
Medical writing support was provided by Neel Misra, MSc, of Engage Scientific Solutions, and funded by Pfizer Inc.
Author contributions
All the authors made substantial contributions to conception and design, execution, or analysis and interpretation of data; drafted the article or revised it critically; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
This review was supported by Pfizer Inc. JS has served on advisory boards for Pfizer, Boehringer Ingelheim, and Bristol-Myers Squibb, and on speakers bureaus for Celgene, Boehringer Ingelheim, and Eli Lilly. BD was a full-time employee of Pfizer at the time this manuscript was initiated. IJ is a full-time employee of Pfizer. JC has no conflicts of interests to declare in this work.
References
- Cancer ResearchUKNon-Hodgkin lymphoma incidence statisticsLondonCancer Research UK2011 Available from: http://www.cancerresearchuk.org/cancer-info/cancerstats/types/nhl/incidence/uk-nonhodgkin-lymphoma-incidence-statistics#worldAccessed August 5, 2016
- FerlayJSoerjomataramIErvikMGLOBOCAN 2012 v1.0, Cancer incidence and mortality worldwide: IARC CancerBase No. 11LyonInternational Agency for Research on Cancer2013 [updated October 9, 2014]. Available from: http://globocan.iarc.frAccessed August 5, 2016
- Union for International Cancer ControlFollicular lymphoma Union for International Cancer Control, 2014 review of cancer medicines on the WHO list of essential medicines Executive summaryGenevaWorld Health Organization2014 Available from: http://www.who.int/selection_medicines/committees/expert/20/applications/FollicularLymphoma.pdfAccessed August 5, 2016
- Solal-CélignyPRoyPColombatPFollicular lymphoma international prognostic indexBlood200410451258126515126323
- StashenkoPNadlerLMHardyRSchlossmanSFCharacterization of a human B lymphocyte-specific antigenJ Immunol19801254167816856157744
- Genentech IncRituxan (rituximab) injection prescribing informationSouth San Francisco, CAGenentech Inc1997 [updated April 2016]. Available from: http://www.gene.com/download/pdf/rituxan_prescribing.pdfAccessed August 5, 2016
- RocheMabThera 100 mg and 500 mg concentrate for solution for infusion. eMC+2014 [updated May 26, 2016]. Available from: http://www.medicines.org.uk/emc/medicine/2570/SPC/Mabthera+100mg+and+500mg+concentrate+for+solution+for+infusionAccessed August 5, 2016
- National Comprehensive Cancer NetworkNCCN clinical practice guidelines in oncology. B-cell Lymphomas. Version 12017Fort Washington, PANCCN2017 [updated 2017]. Available from: https://www.nccn.org/professionals/physician_gls/pdf/b-cell.pdfAccessed February 9, 2017
- DreylingMGhielminiMMarcusRSallesGVitoloULadettoMESMO Guidelines Working GroupNewly diagnosed and relapsed follicular lymphoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-upAnn Oncol201425Suppl 3iii76iii8225122695
- CzuczmanMSGregorySAThe future of CD20 monoclonal antibody therapy in B-cell malignanciesLeuk Lymphoma201051698399420367564
- Mac ManusMPHoppeRTIs radiotherapy curative for stage I and II low-grade follicular lymphoma? Results of a long-term follow-up study of patients treated at Stanford UniversityJ Clin Oncol1996144128212908648385
- WilderRBJonesDTuckerSLLong-term results with radiotherapy for Stage I–II follicular lymphomasInt J Radiat Oncol Biol Phys20015151219122711728680
- PughTJBallonoffANewmanFRabinovitchRImproved survival in patients with early stage low-grade follicular lymphoma treated with radiation: a Surveillance, Epidemiology, and End Results database analysisCancer2010116163843385120564102
- ArdeshnaKMSmithPNortonABritish National Lymphoma InvestigationLong-term effect of a watch and wait policy versus immediate systemic treatment for asymptomatic advanced-stage non-Hodgkin lymphoma: a randomised controlled trialLancet2003362938351652212932382
- ArdeshnaKMQianWSmithPRituximab versus a watch-and-wait approach in patients with advanced-stage, asymptomatic, non-bulky follicular lymphoma: an open-label randomised phase 3 trialLancet Oncol201415442443524602760
- BricePBastionYLepageEComparison in low-tumor-burden follicular lymphomas between an initial no-treatment policy, prednimustine, or interferon alfa: a randomized study from the Groupe d’Etude des Lymphomes Folliculaires. Groupe d’Etude des Lymphomes de l’AdulteJ Clin Oncol1997153111011179060552
- FlinnIWvan der JagtRKahlBSRandomized trial of bendamustine-rituximab or R-CHOP/R-CVP in first-line treatment of indolent NHL or MCL: the BRIGHT studyBlood2014123192944295224591201
- RummelMJNiederleNMaschmeyerGStudy group indolent Lymphomas (StiL)Bendamustine plus rituximab versus CHOP plus rituximab as first-line treatment for patients with indolent and mantle-cell lymphomas: an open-label, multicentre, randomised, phase 3 non-inferiority trialLancet201338198731203121023433739
- SallesGSeymourJFOffnerFRituximab maintenance for 2 years in patients with high tumour burden follicular lymphoma responding to rituximab plus chemotherapy (PRIMA): a phase 3, randomised controlled trialLancet20113779759425121176949
- KahlBSHongFWilliamsMERituximab extended schedule or re-treatment trial for low-tumor burden follicular lymphoma: Eastern Cooperative Oncology Group Protocol e4402J Clin Oncol201432283096310225154829
- Janssen Biotech, IncImbruvica prescribing informationHorsham, PAJanssen Biotech, Inc2016 [updated June 2016]. Available from: http://www.accessdata.fda.gov/drugsatfda_docs/label/2016/205552Orig1s012lbl.pdfAccessed December 5, 2016
- National Cancer InstituteFDA approval for ibrutinib (Imbruvica): approved for chronic lymphocytic leukemia after previous treatmentBethesda, MDUS Department of Health and Human Services2013 [updated April 8, 2015]. Available from: http://www.cancer.gov/about-cancer/treatment/drugs/fda-ibrutinibAccessed August 5, 2016
- Janssen-Cilag International NVIMBRUVICA 140 mg hard capsules. eMC+2014 [updated October 21, 2014]. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/003791/WC500177775.pdfAccessed December 5, 2016
- FoodUSAdministrationDrugFDA approves Zydelig for three types of blood cancers [FDA news release]Silver Spring, MDUS Department of Health and Human Services2014 [updated July 23, 2014]. Available from: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm406387.htmAccessed August 5, 2016
- Genentech IncGazyva prescribing informationSouth San Francisco, CAGenentech Inc2016 [updated February 2016]. Available from: https://www.gene.com/download/pdf/gazyva_prescribing.pdfAccessed December 5, 2016
- SehnLHChuaNMayerJObinutuzumab plus bendamustine versus bendamustine monotherapy in patients with rituximab-refractory indolent non-Hodgkin lymphoma (GADOLIN): a randomised, controlled, open-label, multicentre, phase 3 trialLancet Oncol20161781081109327345636
- RadfordJDaviesACartronGObinutuzumab (GA101) plus CHOP or FC in relapsed/refractory follicular lymphoma: results of the GAUDI study (BO21000)Blood201312271137114323843495
- MarcusREDaviesAJAndoKObinutuzumab-based induction and maintenance prolongs progression-free survival (PFS) in patients with previously untreated follicular lymphoma: primary results of the randomized phase 3 GALLIUM studyPoster presented at: American Society of Hematology (ASH)December 3–6, 2016Washington, DC
- SehnLHAssoulineSEStewartDAA phase 1 study of obinutuzumab induction followed by 2 years of maintenance in patients with relapsed CD20-positive B-cell malignanciesBlood2012119225118512522438256
- SallesGMorschhauserFLamyTPhase 1 study results of the type II glycoengineered humanized anti-CD20 monoclonal anti-body obinutuzumab (GA101) in B-cell lymphoma patientsBlood2012119225126513222431570
- CelgeneRevlimid prescribing informationSummit, NJCelgene2015 [updated February 2015]. Available from: http://www.accessdata.fda.gov/drugsatfda_docs/label/2015/021880s041lbl.pdfAccessed December 5, 2016
- FowlerNHDavisRERawalSSafety and activity of lenalidomide and rituximab in untreated indolent lymphoma: an open-label, phase 2 trialLancet Oncol201415121311131825439689
- VitalEMKayJEmeryPRituximab biosimilarsExpert Opin Biol Ther20131371049106223600760
- BaerWHMainiAJacobsIBarriers to the access and use of rituximab in patients with non-Hodgkin’s lymphoma and chronic lymphocytic leukemia: a physician surveyPharmaceuticals (Basel)20147553054424810947
- LiESubramanianJAndersonSThomasDMcKinleyJJacobsIADevelopment of biosimilars in an era of oncologic drug shortagesDrug Des Devel Ther2015932473255
- GogineniKShumanKLEmanuelEJSurvey of oncologists about shortages of cancer drugsN Engl J Med2013369252463246424350971
- WeiseMBielskyMCDe SmetKBiosimilars: what clinicians should knowBlood2012120265111511723093622
- FoodUSAdministrationDrugScientific considerations in demonstrating biosimilarity to a reference product: guidance for industrySilver Spring, MDU.S. Department of Health and Human Services, Center for Drug Evaluation and Research (CDER), Center for Biologics Evaluation and Research (CBER)2015 [updated April 2015]. Available from: http://www.fda.gov/downloads/DrugsGuidanceComplianceRegulatoryInformation/Guidances/UCM291128.pdfAccessed August 5, 2016
- European Medicines AgencyGuideline on similar biological medicinal products containing biotechnology-derived proteins as active substance: non-clinical and clinical issuesLondonEuropean Medicines Agency2015 [updated December 18, 2014]. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2015/01/WC500180219.pdfAccessed August 5, 2016
- European Medicines AgencyEuropean public assessment reports (EPAR) for human medicines: biosimilarsLondonEuropean Medicines Agency2016 Available from: http://www.ema.europa.eu/ema/index.jsp?curl=pages/medicines/landing/epar_search.jsp&mid=WC0b01ac058001d125Accessed June 21, 2016
- Sandoz, IncZarxio (filgrastim-sndz) injection prescribing informationPrinceton, NJSandoz, Inc2015 [updated March 20, 2015]. Available from: http://www.accessdata.fda.gov/drugsatfda_docs/label/2015/125553lbl.pdfAccessed August 5, 2016
- US Food and Drug AdministrationFilgrastim-sndzSilver Spring, MDUS Department of Health and Human Services, US Food and Drug Administration2015 [updated March 6, 2015]. Available from: http://www.fda.gov/Drugs/InformationOnDrugs/ApprovedDrugs/ucm436953.htmAccessed August 5, 2016
- Expert Committee on Biological StandardizationGuidelines on evaluation of similar biotherapeutic products (SBPs)GenevaWorld Health Organization2009 [updated October 19–21, 2009]. Available from: http://www.who.int/biologicals/areas/biological_therapeutics/BIOTHERAPEUTICS_FOR_WEB_22APRIL2010.pdfAccessed August 5, 2016
- Generics and Biosimilars Initiative (GaBI)Biosimilar rituximab approved in South Korea. GaBI online2016 [updated December 2, 2016]. Available from: http://gabionline.net/Biosimilars/News/Biosimilar-rituximab-approved-in-South-KoreaAccessed December 5, 2016
- CoiffierBSanchoJMJurczakWPharmacokinetic and safety of CT-P10, a biosimilar candidate to the rituximab reference product, in patients with newly diagnosed advanced stage follicular lymphoma (AFL)Poster presented at: American Society of Hematology (ASH)December 3–6, 2016Washington, DC
- YooDHSuhCHShimSCA multicentre randomised controlled trial to compare the pharmacokinetics, efficacy and safety of CT-P10 and innovator rituximab in patients with rheumatoid arthritisAnn Rheum Dis201776356657027624791
- JurczakWIlidiaMGovindbabuKSA phase III efficacy and safety study of the proposed rituximab biosimilar GP2013 versus rituximab in patients with previously untreated advanced follicular lymphomaPoster presented at: American Society of Hematology (ASH)December 3–6, 2016Washington, DC
- KarnikSThompsonMSDeGruttolaHCharacterization and comparison of PF-05280586—a proposed rituximab biosimilar to the licensed productPoster presented at: American Association of Pharmaceutical Scientists-National Biotechnology Conference (AAPS-NBC 2013)May 20–22, 2013San Diego, CA
- BeckerJCMeliaLAGumbinerBThomasDSpencer-GreenGMengXA phase I trial comparing PF-05280586 (a potential biosimilar) and rituximab in subjects with active rheumatoid arthritisPoster presented at: 2014 American College of Rheumatology/Association of Rheumatology Health Professionals (ACR/ARHP) Annual Scientific MeetingNovember 15–19, 2014Boston, MA
- GhielminiMSchmitzSFCogliattiSBProlonged treatment with rituximab in patients with follicular lymphoma significantly increases event-free survival and response duration compared with the standard weekly × 4 scheduleBlood2004103124416442314976046
- van OersMHVan GlabbekeMGiurgeaLRituximab maintenance treatment of relapsed/resistant follicular non-Hodgkin’s lymphoma: long-term outcome of the EORTC 20981 phase III randomized intergroup studyJ Clin Oncol201028172853285820439641
- ForstpointnerRUnterhaltMDreylingMGerman Low Grade Lymphoma Study Group (GLSG)Maintenance therapy with rituximab leads to a significant prolongation of response duration after salvage therapy with a combination of rituximab, fludarabine, cyclophosphamide, and mitoxantrone (R-FCM) in patients with recurring and refractory follicular and mantle cell lymphomas: results of a prospective randomized study of the German Low Grade Lymphoma Study Group (GLSG)Blood2006108134003400816946304
- CzuczmanMSWeaverRAlkuzwenyBBerlfeinJGrillo-LópezAJProlonged clinical and molecular remission in patients with low-grade or follicular non-Hodgkin’s lymphoma treated with rituximab plus CHOP chemotherapy: 9-year follow-upJ Clin Oncol200422234711471615483015
- HiddemannWKnebaMDreylingMFrontline therapy with rituximab added to the combination of cyclophosphamide, doxorubicin, vincristine, and prednisone (CHOP) significantly improves the out-come for patients with advanced-stage follicular lymphoma compared with therapy with CHOP alone: results of a prospective randomized study of the German Low-Grade Lymphoma Study GroupBlood2005106123725373216123223
- McLaughlinPGrillo-LópezAJLinkBKRituximab chimeric anti-CD20 monoclonal antibody therapy for relapsed indolent lymphoma: half of patients respond to a four-dose treatment programJ Clin Oncol1998168282528339704735
- MarcusRImrieKSolal-CelignyPPhase III study of R-CVP compared with cyclophosphamide, vincristine, and prednisone alone in patients with previously untreated advanced follicular lymphomaJ Clin Oncol200826284579458618662969
- MorschhauserFRadfordJVan HoofAPhase III trial of consolidation therapy with yttrium-90-ibritumomab tiuxetan compared with no additional therapy after first remission in advanced follicular lymphomaJ Clin Oncol200826325156516418854568
- MorschhauserFRadfordJVan HoofA90Yttrium-ibritumomab tiuxetan consolidation of first remission in advanced-stage follicular non-Hodgkin lymphoma: updated results after a median follow-up of 7.3 years from the International, Randomized, Phase III First-Line Indolent trialJ Clin Oncol201331161977198323547079
- HagenbeckARadfordJVan HoofA90Y-Ibritumomab tiuxetan (Zevalin®) consolidation of first remission in advanced-stage follicular non-Hodgkin’s lymphoma: updated results after a median follow-up of 66.2 months from the International, Randomized, Phase III First-Line Indolent Trial (FIT) in 414 patientsBlood2010116 Suppl abstr 594
- LeonardJJungSHJohnsonJLCALGB 50401: a randomized trial of lenalidomide alone versus lenalidomide plus rituximab in patients with recurrent follicular lymphomaJ Clin Oncol201230Suppl abstr 8000
- WitzigTEFlinnIWGordonLITreatment with ibritumomab tiuxetan radioimmunotherapy in patients with rituximab-refractory follicular non-Hodgkin’s lymphomaJ Clin Oncol200220153262326912149300
- HainsworthJDLitchySBurrisHA3rdRituximab as first-line and maintenance therapy for patients with indolent non-Hodgkin’s lymphomaJ Clin Oncol200220204261426712377971
- ColombatPSallesGBrousseNRituximab (anti-CD20 mono-clonal antibody) as single first-line therapy for patients with follicular lymphoma with a low tumor burden: clinical and molecular evaluationBlood200197110110611133748
- MartinelliGSchmitzSFUtigerULong-term follow-up of patients with follicular lymphoma receiving single-agent rituximab at two different schedules in trial SAKK 35/98J Clin Oncol201028294480448420697092
- GopalAKKahlBSde VosSPI3Kδ inhibition by idelalisib in patients with relapsed indolent lymphomaN Engl J Med2014370111008101824450858
- MartinPJungSHJohnsonJLCALGB 50803 (Alliance): a phase II trial of lenalidomide plus rituximab in patients with previously untreated follicular lymphomaJ Clin Oncol201432Suppl 5 abstr 8521
- CzuczmanMSKoryznaAMohrARituximab in combination with fludarabine chemotherapy in low-grade or follicular lymphomaJ Clin Oncol200523469470415681517
- McLaughlinPHagemeisterFBRodriguezMASafety of fludarabine, mitoxantrone, and dexamethasone combined with rituximab in the treatment of stage IV indolent lymphomaSemin Oncol2000276 Suppl 123741
- FeuerleinKZuccaEGhielminiMFirst-line treatment of follicular lymphoma: a patient-oriented algorithmLeuk Lymphoma200950332533419229730