
Abstract
Introduction
The prognostic impact of the number of examined lymph nodes (ELNs) in different histological subtypes of cervical cancer remains unclear. We aimed to assess the impact of the number of ELNs in stage IA2–IIA cervical cancer with different histological subtypes.
Methods
Data of patients with stage IA2–IIA squamous cell carcinoma (SCC) and adenocarcinoma (AC) of the uterine cervix between 1988 and 2013 were retrieved from the Surveillance, Epidemiology, and End Results program. Univariate and multivariate Cox regression analyses were performed to analyze the effect of number of ELNs on cause-specific survival (CSS) and overall survival (OS).
Results
The final data set identified 11,830 patients including 7,920 (66.9%) women with SCC and 3,910 (33.1%) with AC. The median number of ELNs was 19. The multivariate analysis indicated that the number of ELNs was an independent prognostic factor influencing CSS and OS, both as a continuous or a categorical variable. Patients with a higher number of ELNs had better survival outcomes. In SCC subtype, the number of ELNs was also the independent prognostic factor of CSS and OS in node-positive patients, but not in patients with node-negative disease. In AC patients, ELN count was not an independent predictor of CSS and OS regardless of lymph node status.
Conclusion
The number of ELNs is an independent prognostic factor in patients with stage IA2–IIB cervical cancer. A higher number of ELNs is associated with better survival outcomes, especially in the node-positive SCC subtype.
Introduction
Cervical cancer is one of the most common malignancies in women and has become an important disease that threatens women’s health.Citation1,Citation2 Radical hysterectomy is the main local treatment of early stage cervical cancer, and pelvic lymphadenectomy is an important surgical procedure during radical hysterectomy. Several studies have found that the number of examined lymph nodes (ELNs) could predict precise lymph node staging in lung, gastric, rectal, and ovarian cancer, and patients with a higher number of ELNs show better survival.Citation3–Citation6 However, for patients with cervical cancer, extensive lymphadenectomy may lead to more postoperative complications and damage the patient’s immune system.Citation7,Citation8
The status of lymph node is not considered in the current International Federation of Gynecology and Obstetrics (FIGO) staging system. However, more studies have found that a higher number of positive lymph nodes (PLNs) was associated with worse prognosis.Citation9,Citation10 Theoretically, a higher number of ELNs could accurately assess lymph node status, which may reduce the risk of occult lymph node metastases. Previous studies have found that a higher number of ELNs was associated with better survival in patients with node-positive disease.Citation11,Citation12 However, several studies have shown that extensive lymphadenectomy did not improve survival.Citation13–Citation15 In addition, a population-based study found that a higher number of ELNs was associated with better survival outcomes in patients with node-negative cervical cancer.Citation16 Therefore, the clinical value of ELN count in cervical cancer remains controversial.
Squamous cell carcinoma (SCC) and adenocarcinoma (AC) are the most common histological subtypes of cervical cancer, which show differences in epidemiology, etiology, molecular characterization, and prognosis.Citation17–Citation19 To the best of our knowledge, there are no studies investigating the prognostic impact of the number of ELNs in different histological subtypes of cervical cancer. In this study, we aimed to investigate the prognostic value of the number of ELNs in cervical cancer using the Surveillance, Epidemiology, and End Results (SEER) database and further analyzed whether the results were affected by histological subtypes.
Materials and methods
Patients
We included patients diagnosed with FIGO stage IA2–IIA SCC and AC of the uterine cervix after hysterectomy and lymphadenectomy between 1988 and 2013 based on the SEER program.Citation20 Patients with unknown ELN count and PLN count were excluded. We obtained the permission to access the SEER research data files with the reference number 14239-Nov2015. The Clinical Research Ethics Committee of the First Affiliated Hospital of Xiamen University approved this study. This study did not include any interactions with human subjects or use personally identifiable information, therefore, the ethics committee did not require that written informed consent be obtained.
Demographic and clinicopathological factors
The demographic and clinicopathological factors including age, year of diagnosis, ethnicity, FIGO stage, grade, histological subtypes, number of PLNs and ELNs, and radiotherapy were collected from the SEER database. The FIGO stage IA2–IIA category included stages IA2, IB not otherwise specified (NOS), IB1, IB2, and IIA in the SEER database. The number of PLNs was classified as 0, 1, 2, 3, and >4. The number of ELNs was classified according to previous studies as follows: 1–10, 11–20, 21–30, and >30.Citation13,Citation16 The primary endpoints of this study were cause-specific survival (CSS) and overall survival (OS).
Statistical analysis
All statistical analyses were completed using the SPSS package (version 21.0; IBM Corporation, Armonk, NY, USA). The Pearson’s χ2 test was used to compare the frequency distributions between categorical variables. Analysis of variance was used to compare the continuous variables in patients. Survival rates were determined by using Kaplan–Meier method and log-rank test. Univariate and multivariate Cox proportional hazard analyses were performed to identify the prognostic factors of CSS and OS. The impact of ELNs in the multivariate Cox proportional hazard model was evaluated by using continuous variables or categorical variables in two models. All the prognostic variables that were found to be significant in the univariate analysis were included in the multivariate analysis. A p-value of <0.05 was considered significant in all the analyses.
Results
The demographic and clinicopathological characteristics are summarized in . A total of 11,830 patients were included in this study, and 8,825 (74.6%) patients were diagnosed after 2000. The median age was 43 years (range, 9–90 years). Among them, 66.9% (7,920) and 33.1% (3,910) of patients were diagnosed with SCC and AC, respectively. Regarding the FIGO stage, 1,573 (13.3%), 9,528 (80.5%), and 729 (6.2%) patients were in stage IA2, IB, and IIA, respectively.
Table 1 Patients’ demographic and clinicopathological characteristics
The median number of ELNs was 19. A total of 2,374 (20.1%), 4,418 (37.3%), 3,034 (25.6%), and 2,004 (16.9%) patients were categorized as having 1–10, 11–20, 21–30, and >30 ELNs, respectively. A total of 1,812 (15.3%) patients were with node-positive disease, and the median number of PLNs was two (range, 1–43) in patients with node-positive disease.
Patients who were younger, diagnosed after 2000, white ethnicity, IB NOS stage, received radiotherapy, and married had a higher number of ELNs. The probability of a higher number of PLNs was higher in patients with more ELNs. The clinicopathological data among the four groups were not significantly different for histological subtypes and grade ().
The median time of follow-up was 86 months (range, 1–311 months). The 5- and 10-year CSS were 91.6% and 89.1%, respectively, and the 5- and 10-year OS were 89.3% and 83.9%, respectively.
The univariate analysis showed that ELN as a continuous variable or as a categorical variable was the significant prognostic factor in CSS and OS (). The results of multivariate analysis showed that ELN was an independent prognostic factor for both CSS and OS as a continuous or a categorical variable (). Patients with a higher number of ELNs had a better survival. In the subgroup analysis of patients with node-positive disease, the number of ELNs was also an independent prognostic factor for survival. However, the number of ELNs was not associated with survival outcomes in node-negative patients (). Age, year of diagnosis, ethnicity, FIGO stage, grade, histological subtypes, number of PLNs, and radiotherapy were also independent prognostic factors for survival in the multivariate analysis.
Table 2 Univariate analysis on prognostic factors of survival
Table 3 Multivariate analyses of impact of examined lymph node count on survival according to different lymph node status
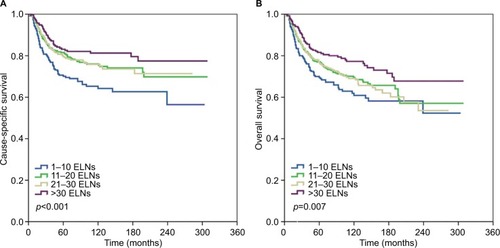
The prognostic value of the number of ELNs in patients with SCC and AC was further analyzed. The ELN count was not significantly different between SCC and AC (p=0.760). However, more patients had a higher number of PLNs in SCC subtype, whereas AC patients were more likely to have node-negative disease (p<0.001). In SCC subtype, the results of multivariate analysis showed that the number of ELNs as a continuous or a categorical variable was also an independent prognostic factor for CSS and OS in the entire cohort and in the node-positive subset, but not in the node-negative patients (; ). However, ELN count was not an independent predictor of CSS and OS regardless of lymph node status ().
Figure 1 Impact of examined lymph node (ELN) count on cause-specific survival (A) and overall survival (B) in node-positive cervical squamous cell carcinoma.
Discussion
In this study, we investigated the prognostic impact of ELN count of early stage cervical cancer patients in a population-based study. Our results indicated that ELN count was an independent prognostic factor for survival outcomes, especially in patients with a node-positive disease. The subgroup analysis showed similar results in patients with SCC subtype, while ELN count had no prognostic value in AC patients.
Currently, the therapeutic value of extensive lymphadenectomy in patients with cervical cancers remains controversial. A study by Lim et al found that a more extensive lymphadenectomy (>40 ELNs) improved survival in patients with tumors sized >4 cm.Citation21 However, other studies found that the ELN count had no effect on survival.Citation13–Citation15 In this study, we found that a higher number of ELNs was associated with better survival in patients with early stage cervical cancer.
Although the lymph node status has not been included in the FIGO staging system, several studies have suggested that a higher number of PLNs was an unfavorable prognostic factor for survival.Citation9,Citation10 Our study also found that patients with a higher number of PLNs had worse prognosis and that the risk of lymph node involvement (>4) was significantly increased in patients with >30 ELNs. Therefore, a higher number of ELNs may reduce the risk of occult lymph node metastases.
The effect of number of ELNs on survival of patients with cervical cancer according to different lymph node status remains controversial. A previous SEER study suggested that more extensive lymphadenectomy improved survival in node-negative patients and had no prognostic value in node-positive patients (from 1988 to 2005).Citation16 In our study, subgroup analyses found that ELN count was the independent prognostic factor in node-positive patients but not in patients with node-negative disease. Our results were contrary to the findings of Shah et al,Citation16 which may be due to the difference in sample size (11,830 vs 5,222, respectively). In addition, 48.0% of patients in the Shah et alCitation16 study were diagnosed after 2000, and 76.4% of patients in our study were diagnosed after 2000, which differences in the use of adjuvant therapy may exist according to the year of diagnosis. Although there were contrary findings between the two SEER studies, our results were similar to previous studies.Citation11,Citation12 Mao et al also found that there was no prognostic effect of ELN count in node-negative patients.Citation22
The epidemiology, etiology, clinicopathological and molecular characteristics, treatment response, and prognosis of SCC are significantly different compared to AC of the uterine cervix.Citation17–Citation19 However, the incidence of AC has increased in recent decades. In our study, 33.1% of patients were diagnosed with cervical AC, which was higher than a previous SEER study (20%).Citation23 Several studies have shown that radiotherapy was the main local treatment in cervical SCC, while more cervical AC patients received primary surgery.Citation24,Citation25 Therefore, the higher incidence of AC in our study was related to difference in the study population. Previous studies indicated that there was no significant difference in lymph node status between SCC and AC.Citation26,Citation27 In this study, the ELN count was not significantly different between SCC and AC. However, more patients had a higher number of PLNs in SCC subtype, whereas AC patients were more likely to have node-negative disease. However, the SCC subtype had a higher number of PLNs compared with AC group.
The effect of ELN count on the survival of patients with SCC and AC is not well determined. Our subgroup analysis found that ELN count was the independent prognostic factor in node-positive SCC subtype. In addition, the ELN count had no prognostic value in AC patients regardless of nodal status. To the best of our knowledge, our study was the first to identify the prognostic value of ELN count in cervical cancer with different histological subtypes.
The extent of lymphadenectomy may be individualized based on accurate assessment of lymph node status. Previous studies have found that advanced FIGO stage, large tumor size, deep stromal invasion, involvement of the parametrium, and lymphovascular invasion could predict lymph node metastasis in cervical cancer.Citation28,Citation29 In addition, positron emission tomography/computer tomography (PET/CT) and magnetic resonance imaging (MRI) have higher sensitivity and specificity in predicting lymph node metastasis.Citation30,Citation31 However, the accuracy of PET/CT decreases for nodal size <5 mm and micrometastasis.Citation30,Citation31 PET/MRI-diffusion weighted imaging may be a valuable imaging technique for nodal staging in patients with cervical and endometrial cancer, but further studies are required to investigate its potential clinical utility.Citation32
An increasing number of studies have found that sentinel lymph node (SLN) biopsy is an important indicator evaluating pelvic nodal status in cervical cancer, with excellent detection rates and high sensitivity.Citation33,Citation34 SLN biopsy without pelvic lymphadenectomy is considered safe in cervical cancer patients with negative SLNs.Citation35,Citation36 Several studies have found that indocyanine green SLN mapping in cervical cancer provided higher overall and bilateral detection rates compared with current standard of careCitation37–Citation39 and removed up to three SLNs which may be enough to accurately assess the lymph node staging in cervical cancer patients.Citation40 The current National Comprehensive Cancer Network guidelines recommended the SLN technique for early stage cervical cancer with tumor size <2 cm.Citation41 Our study found that the number of ELNs has no effect on survival in node-negative cervical cancer. Therefore, combined with the current SLN biopsy technology, pelvic lymphadenectomy may be avoided in node-negative cervical cancer.
Our study has several limitations that need to be acknowledged. First, inherent bias could not be avoided in retrospective studies. Second, the SEER program lacks data concerning several pathological factors including lymphovascular invasion, stromal invasion, and postoperative complications among the ELNs groups, which may cause bias to analysis. In addition, the extents of lymphadenectomy (pelvic, inguinal, or para-aortic) were not clearly defined because there is no detailed record in the SEER database. Third, there was no information regarding whether or not chemotherapy has been given. Fourth, the period of this study spanned about 25 years, and the adjuvant treatment of early stage cervical cancer has changed in recent decades,Citation42 which may have potentially impacted the survival outcomes.
Conclusion
In patients with stage IA2–IIB cervical cancer, the number of ELNs is an independent prognostic factor of survival. A higher number of ELNs is associated with better survival outcomes, especially in the node-positive SCC subtype. Further studies are required to determine the optimal extent of lymphadenectomy in cervical cancer with different histological subtypes.
Acknowledgments
This work was supported by grants from the Natural Science Foundation of Fujian Province (numbers 2015J01550 and 2013D001), the Foundation Medical Innovation Foundation of Fujian Province (number 2015-CXB-34), and the Foundation for Young Scholar of Fujian Provincial Health Department (number 2014-ZQN-ZD-31). The authenticity of this article has been validated by uploading the key raw data onto the Research Data Deposit (RDD) public platform (www.researchdata.org.cn), with the approval RDD number as RDDA201700184.
Disclosure
The authors report no conflicts of interest in this work.
References
- SiegelRLMillerKDJemalACancer statistics, 2016CA Cancer J Clin201666173026742998
- ChenWZhengRBaadePDCancer statistics in China, 2015CA Cancer J Clin201666211513226808342
- LiangWHeJShenYImpact of examined lymph node count on precise staging and long-term survival of resected non-small-cell lung cancer: a population study of the US SEER database and a Chinese multi-institutional registryJ Clin Oncol201735111162117028029318
- WooYGoldnerBItuartePLymphadenectomy with optimum of 29 lymph nodes retrieved associated with improved survival in advanced gastric cancer: a 25,000 patient international database studyJ Am Coll Surg2017224454655528017807
- HallMDSchultheissTESmithDDImpact of total lymph node count on staging and survival after neoadjuvant chemoradiation therapy for rectal cancerAnn Surg Oncol201522Suppl 3S580S58725956577
- KleppeMvan der AaMAVan GorpTSlangenBFKruitwagenRFThe impact of lymph node dissection and adjuvant chemotherapy on survival: a nation wide cohort study of patients with clinical early-stage ovarian cancerEur J Cancer201666839027536891
- ChenGDLinLYWangPHLeeHSUrinary tract dysfunction after radical hysterectomy for cervical cancerGynecol Oncol200285229229711972390
- ZulloMAManciNAngioliRMuziiLPaniciPBVesical dysfunctions after radical hysterectomy for cervical cancer: a critical reviewCrit Rev Oncol Hematol200348328729314693341
- KasuyaGOgawaKIrahaSPostoperative radiotherapy for uterine cervical cancer: impact of lymph node and histological type on survivalAnticancer Res20133352199220423645776
- HornLCHentschelBGalleDBilekKExtracapsular extension of pelvic lymph node metastases is of prognostic value in carcinoma of the cervix uteriGynecol Oncol20081081636717920109
- KimHSKimJHChungHHSignificance of numbers of metastatic and removed lymph nodes in FIGO stage IB1 to IIA cervical cancer: primary surgical treatment versus neoadjuvant chemotherapy before surgeryGynecol Oncol2011121355155721334733
- PieterseQDKenterGGGaarenstroomKNThe number of pelvic lymph nodes in the quality control and prognosis of radical hysterectomy for the treatment of cervical cancerEur J Surg Oncol200733221622117097845
- SuprasertPCharoenkwanKKhunamornpongSPelvic node removal and disease-free survival in cervical cancer patients treated with radical hysterectomy and pelvic lymphadenectomyInt J Gynaecol Obstet20121161434621978816
- DittoAMartinelliFLo VulloSThe role of lymphadenectomy in cervical cancer patients: the significance of the number and the status of lymph nodes removed in 526 cases treated in a single institutionAnn Surg Oncol201320123948395423812772
- XieXZSongKCuiBClinical and pathological factors related to the prognosis of chinese patients with stage Ib to IIb cervical cancerAsian Pac J Cancer Prev201213115505551023317208
- ShahMLewinSNDeutschITherapeutic role of lymphadenectomy for cervical cancerCancer2011117231031720862747
- FujiwaraKMonkBDevouassoux-ShisheboranMAdenocarcinoma of the uterine cervix: why is it different?Curr Oncol Rep2014161241625325935
- GienLTBeaucheminMCThomasGAdenocarcinoma: a unique cervical cancerGynecol Oncol2010116114014619880165
- ZhouJWuSGSunJYComparison of clinical outcomes of squamous cell carcinoma, adenocarcinoma, and adenosquamous carcinoma of the uterine cervix after definitive radiotherapy: a population-based analysisJ Cancer Res Clin Oncol2017143111512227646608
- Surveillance, Epidemiology, and End Results (SEER) Program (www.seer.cancer.gov) SEER#x0002A;Stat Database: Incidence - SEER 18 Regs Research Data + Hurricane Katrina Impacted Louisiana Cases, Nov 2015 Sub (1973-2013 varying) - Linked To County Attributes - Total U.S., 1969-2014 CountiesNational Cancer Institute, DCCPS, Surveillance Research Program released April 2016, based on the November 2015 submission. Available from: https://seer.cancer.gov/dataAccessed January 25, 2017
- LimSChoKLeeSEffect of number of retrieved lymph nodes on prognosis in FIGO stage IB-IIA cervical cancer patients treated with primary radical surgeryJ Obstet Gynaecol Res201743121121927862677
- MaoSDongJLiSWangYWuPPrognostic significance of number of nodes removed in patients with node-negative early cervical cancerJ Obstet Gynaecol Res201642101317132527435888
- AdegokeOKulasingamSVirnigBCervical cancer trends in the United States: a 35-year population-based analysisJ Womens Health (Larchmt)201221101031103722816437
- Vinh-HungVBourgainCVlastosGPrognostic value of histopathology and trends in cervical cancer: a SEER population studyBMC Cancer2007716417718897
- ZhouJWuSGSunJYThe effect of local treatment modalities in patients with early-stage adenocarcinoma of the uterine cervix: a population-based analysisInt J Surg201741162228302450
- WinerIAlvarado-CabreroIHassanOThe prognostic significance of histologic type in early stage cervical cancer – a multi-institutional studyGynecol Oncol2015137347447825677061
- NohJMParkWKimYSComparison of clinical outcomes of adenocarcinoma and adenosquamous carcinoma in uterine cervical cancer patients receiving surgical resection followed by radiotherapy: a multicenter retrospective study (KROG 13–10)Gynecol Oncol2014132361862324486605
- SakuragiNUp-to-date management of lymph node metastasis and the role of tailored lymphadenectomy in cervical cancerInt J Clin Oncol200712316517517566838
- ZhouJRanJHeZYTailoring pelvic lymphadenectomy for patients with stage IA2, IB1, and IIA1 uterine cervical cancerJ Cancer20156437738125767608
- ChoiHJJuWMyungSKKimYDiagnostic performance of computer tomography, magnetic resonance imaging, and positron emission tomography or positron emission tomography/computer tomography for detection of metastatic lymph nodes in patients with cervical cancer: meta-analysisCancer Sci201010161471147920298252
- MayoralMParedesPDomènechB18F-Fdg PET/CT and sentinel lymph node biopsy in the staging of patients with cervical and endometrial cancer. Role of dual-time-point imagingRev Esp Med Nucl Imagen Mol20173612026 Spanish, with English abstract27667001
- SteccoABuemiFCassaràAComparison of retrospective PET and MRI-DWI (PET/MRI-DWI) image fusion with PET/CT and MRI-DWI in detection of cervical and endometrial cancer lymph node metastasesRadiol Med2016121753754527033474
- DiabYSentinel lymph nodes mapping in cervical cancer a comprehensive reviewInt J Gynecol Cancer201727115415827792042
- LécuruFMathevetPQuerleuDBilateral negative sentinel nodes accurately predict absence of lymph node metastasis in early cervical cancer: results of the SENTICOL studyJ Clin Oncol2011291686169121444878
- LennoxGKCovensACan sentinel lymph node biopsy replace pelvic lymphadenectomy for early cervical cancer?Gynecol Oncol20171441162027742472
- NiikuraHOkamotoSOtsukiTProspective study of sentinel lymph node biopsy without further pelvic lymphadenectomy in patients with sentinel lymph node-negative cervical cancerInt J Gynecol Cancer20122271244125022864335
- BudaAPapadiaAZapardielIFrom Conventional Radiotracer Tc-99(m) with blue dye to indocyanine green fluorescence: a comparison of methods towards optimization of sentinel lymph node mapping in early stage cervical cancer for a laparoscopic approachAnn Surg Oncol20162392959296527126631
- ImbodenSPapadiaANauwerkMA comparison of radio colloid and indocyanine green fluorescence imaging, sentinel lymph node mapping in patients with cervical cancer undergoing laparoscopic surgeryAnn Surg Oncol201522134198420326122376
- RuscitoIGasparriMLBraicuEISentinel node mapping in cervical and endometrial cancer: indocyanine green versus other conventional dyes – a meta-analysisAnn Surg Oncol201623113749375627160526
- PapadiaAImbodenSGasparriMLSiegenthalerFFinkAMuellerMDEndometrial and cervical cancer patients with multiple sentinel lymph nodes at laparoscopic ICG mapping: how many are enough?J Cancer Res Clin Oncol20161421831183627318493
- National Comprehensive Cancer NetworkNCCN Clinical Practice Guidelines in Oncology. Cervical Cancer. Version 1.2017 [updated October 10, 2016] Available from: https://www.nccn.org/professionals/physician_gls/pdf/cervical.pdfAccessed May 28, 2017
- PetersWA3rdLiuPYBarrettRJ2ndConcurrent chemotherapy and pelvic radiation therapy compared with pelvic radiation therapy alone as adjuvant therapy after radical surgery in high-risk early-stage cancer of the cervixJ Clin Oncol20001881606161310764420