
Abstract
Triple-negative breast cancer (TNBC) remains the poorest-prognosis breast cancer (BC) subtype. Gene expression profiling has identified at least six different triple-negative subtypes with different biology and sensitivity to therapies. The heterogeneous nature of TN tumors may justify the difficulty in treating this BC subtype. Several targeted agents have been investigated in clinical trials without demonstrating a clear survival benefit. Therefore, systemic chemotherapy remains the cornerstone of current clinical practice. Improving the knowledge of tumor biology is mandatory for patient management. In stages II and III, neoadjuvant systemic treatment is an effective option of care. The achievement of a pathological complete response represents an optimal surrogate for survival outcome as well as a test for tumor drug sensitivity. In this review, we provide a brief description of the main predictive biomarkers for tumor response to systemic treatment. Moreover, we review the treatment strategies investigated for TNBCs in neoadjuvant settings focusing on experimental drugs such as immunotherapy and poly [ADP-ribose] polymerase inhibitors that hold promise in the treatment of this aggressive disease. Therefore, the management of TNBC represents an urgent, current, unmet need in daily clinical practice. A key recommendation is to design biology-driven clinical trials wherein TNBC patients may be treated on the basis of tumor molecular profile.
Introduction
Currently, the treatment of patients with triple-negative breast cancer (TNBC) is the biggest challenge in the breast cancer (BC) scenario. TNBCs are defined by the absence of both hormone (estrogen and progesterone) receptors and HER2 overexpression.Citation1 TNBCs represent a heterogeneous group of BCs with different treatment sensitivity and prognosis. Preclinical studies have identified at least six different molecular subtypes: two basal-like (BL1 and BL2), an immunomodulatory (IM), a mesenchymal (M), a mesenchymal stem-like (MSL), and a luminal androgen receptor (LAR).Citation2
In the early stages, the use of neoadjuvant systemic treatment (NST) is the standard of care in TNBCs. Patients who achieve a pathological complete response (pCR) with primary therapy have improved survival outcomes.Citation3,Citation4 Standard neoadjuvant regimens include anthracyclines, taxanes, and cyclophosphamide.Citation5,Citation6 Platinum-based chemotherapy has been proposed but is not yet recommended by available guidelines. Different systemic treatment options have been investigated besides the use of chemotherapy.Citation7–Citation12 However, there are no approved targeted therapies for TNBC in the neoadjuvant setting, although many different drugs have been studied and still others are currently being tested.
Clearly, there is a major need to better understand the characteristics and the clinical behavior of TNBCs with an aim to develop effective treatments for this BC subtype. The identification of molecular targets is essential for the design of clinical trials that investigate new treatment strategies. In this article, we review the literature on the use of NST in TNBCs. We focus on the molecular markers able to predict response/resistance to therapies. Moreover, we review the recent data on experimental drugs tested, and discuss findings concerning immunologic checkpoint inhibitors in this population. The main, ongoing clinical trials conducted in this field are reported as well.
Predictive factors of response/resistance to neoadjuvant treatment
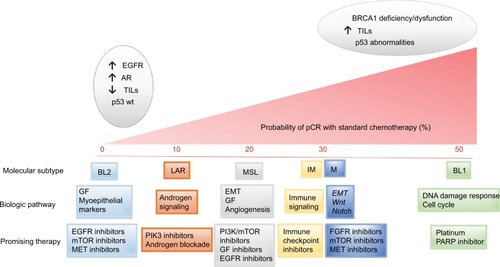
The known, investigated, predictive factors of response/resistance to NST in patients with TNBC are shown in and listed further.
Figure 1 Triple negative breast cancer (TNBC) molecular subtypes classified according to gene expression and the main involved pathways. Each of these subclasses show varying pathological complete response (pCR) rates following standard neoadjuvant chemotherapy. Promising therapies for every molecular subtype have been suggested.
Breast-related cancer antigen 1
TNBCs are likely to be breast-related cancer antigen 1 (BRCA1) mutation carriers or to have gene expression profiles similar to BRCA1-deficient tumors.Citation13 BRCA genes play an important role in DNA double-strand break repair, contributing to the maintenance of DNA stability.Citation14 Approximately 20% of all TNBCs show loss or inactivation of BRCA genes, resulting in an inefficient repair mechanism.Citation15,Citation16 Besides a mutation in BRCA1/BRCA2, hypermethylation of both – the BRCA1 promoter and Fanconi anemia gene (FANCF) – result in a BRCA-like phenotype (also called the “BRCAness” tumors). The BRCA status is considered a predictive factor of response to chemotherapy and poly [ADP-ribose] polymerase (PARP) inhibitory agents. With regard to chemotherapy, tumor cell lines lacking functional BRCA1 or 2 have increased sensitivity to DNA cross-linking agents such as platinum and to DNA-damaging chemotherapy agents such as anthracycline ().Citation17 In two clinical studies conducted in TNBC patients treated with neoadjuvant single-agent cisplatin, pCR rates in BRCA-mutated women were 100% and 83%, respectively.Citation15,Citation18 Moreover, a significant difference in pCR rates has been found between BRCA1-mutated and BRCA1-wild-type women treated with anthracycline and taxane regimens (57.1% vs 29%; p < 0.001).Citation16 On the other hand, preclinical evidence has shown a negative correlation between the BRCA1 mutation and taxane sensitivity due to the loss of a pro-apoptotic pathway activated in response to taxane-induced DNA damage.Citation19 Furthermore, the increased sensitivity to DNA double-strand break agents has been confirmed in BRCA-like tumors that have a homologous recombination deficiency (HRD) similar to BRCA-mutated ones. A pooled analysis of six phase II trials conducted in TNBC patients treated with platinum demonstrated that patients with a high HRD score had an increased pCR rate compared to HR-non-deficient patients (53% vs 18%) regardless of the BRCA mutation status.Citation20
Table 1 pCR rate reported in published clinical trials in TNBC BRCA-mutated (BRCA mt) patients
Molecular subtypes
Lehmann et al analyzed gene expression profiles in 587 TNBCs and identified six different subtypes: BL1, BL2, IM, M, MSL, and LAR.Citation21 BL tumors are characterized by a high frequency of chromosomal rearrangements, genomic instability, and BRCA1 or BRCA2 mutations. In particular, BL1 tumors are usually enriched in cell-cycle and DNA-damage-response genes that justify their high sensitivity to DNA-damaging agents such as platinum. In contrast, BL2 cancers frequently overexpress growth factor receptors, such as epidermal growth factor receptor (EGFR), IGF1R, and myoepithelial markers with low probability of tumor response to chemotherapy.Citation21 More recent data, presented at the San Antonio Breast Cancer Symposium (SABCS) 2016, confirmed how BL1 tumors were likely to achieve a higher pCR rate compared to other TNBC subtypes (38% vs 20%, p = 0.015).Citation22 Both M and MSL are enriched in pathways associated with EMT (epithelial–mesenchymal transition) and cell motility. This BC subtype frequently presents PI3KCA-activating mutations. According to genomic expression, mesenchymal tumor cells have displayed responses to dasatinib (abl/src inhibitor) and a PI3K/mTOR inhibitor. The LAR subtype cells express androgen receptors with sensitivity to an AR antagonist such as bicalutamide. Finally, IM tumors are enriched in genes involved in immune cell processes and may be considered the more promising subtypes for immunotherapies.Citation21 This molecular classification seems to have not only a predictive value but also a prognostic one. A significant difference in relapse-free survival (RFS) has been found among molecular subtypes. In particular, LAR tumors show a decreased RFS compared with the BL1, IM, and MSL subtypes (HR = 2.9, 3.2, and 10.5, respectively; p < 0.05). There were no reported significant differences in terms of distant-metastasis-free survival (DMFS).Citation21
Epidermal growth factor receptor
The EGFR is a transmembrane tyrosine kinase receptor localized on the cell surface that induces cell proliferation, angiogenesis, and apoptosis inhibition.Citation23–Citation25 EGFR abnormalities are reported in 27%–57% of TNBCs.Citation26 Clinical data suggested a possible predictive and prognostic value of the EGFR. A retrospective analysis of 117 patients, 28 of whom had a TNBC, showed that EGFR expression was related to a worse response to anthracycline-based NST and poor overall prognosis (p = 0.03).Citation27 Moreover, in a multivariate analysis of a retrospective study conducted in 287 women with TNBCs, EGFR overexpression was a significant independent prognostic factor for relapse (31% in EGFR-positive vs 16.2% in EGFR-negative patients).Citation28 Preclinical data showed how the use of anti-EGFR antibodies can decrease antitumor activity by downregulation of EGFR (endocytosis and degradation) and limit cell migration.Citation29 Based on this evidence, a multi-center, prospective, single-arm phase II study was conducted among 60 women with stages II and IIIa TNBC, with an aim to investigate the rule of panitumumab (anti-EGFR antibody) in addition to NST (fluorouracil+epirubicin + cyclophosphamide [FEC] followed by docetaxel).Citation12 The pCR rates were 46.8% in breast and nodes, and 55.3% in the breast only. EGFR expression was confirmed as a predictive factor for response to chemotherapy plus panitumumab. A positive trend for pCR was shown in EGFR overexpressed BC (58% vs 28%, p = 0.079), suggesting a potential benefit of anti-EGFR therapy plus chemotherapy in this subgroup of patients.Citation12
Tumor-infiltrating lymphocytes
Since the last decade onward, the immune system has been under investigation as a possible target in the management of different cancer subtypes. Tumor-infiltrated lymphocytes (TILs) have been identified in both tumor and stromal tissues. Intratumoral TILs (It-TILs) are lymphocytes that have a direct interaction with cancer cells, whereas stromal TILs (Str-TILs) are lymphocytes localized in the peripheral stromal area. Considering BC subtypes, TNBCs have the highest tumor TIL expression (~20%) compared to other BC subtypes.Citation30,Citation31 In particular, the IM subtype of TNBC is characterized by high presence of immune cells, antigen presentation, and activation of immune pathways.Citation21 Clinical data suggested a predictive role of TILs in terms of pCR in patients treated with NST, mainly with platinum regimens.Citation32–Citation34 A prospective evaluation of TILs in the GeparSixto trial found that lymphocyte-predominant (LP) BC, defined as tumors with lymphocytic infiltrate greater than 50%, were more likely to achieve pCR as compared to non-LP BCs (59.9% vs 33.8%; p < 0.001).Citation35 The addition of carboplatin to anthracycline and taxane in LPBCs further increased the pCR rate up to 75% (p = 0.002).Citation35 The predictive role of TILs primarily suggested by some small retrospective dataCitation36–Citation39 was confirmed by the large meta-analysis present at the SABCS 2016, where a total of 3,771 tumors from the clinical Gepar studies (Gepar-Duo, GeparTrio, GeparQuattro, GeparQuinto, GeparSixto, and GeparSepto) were evaluated for the presence of TIL.Citation40 These results suggest TILs are a strong predictive marker for response to NST in all BC subtypes.Citation40 This predictive value was translated into a survival benefit in the TNBCs group. The presence of TILs in residual tumor disease after primary chemotherapy seems to be related to more favorable long-term outcomes as well.Citation40 Another retrospective cohort of 278 patients with TNBCs correlated TIL presence with a risk reduction of metastasis and death. The major prognostic relevance of TILs was found in patients with residual tumor >2 cm and/or node metastasis.Citation33 These authors hypothesized a possible use of TILs for selecting patients with high risk of relapse after NST. A comparison between TIL expression in the BC tissue before and after chemotherapy administration was also undertaken, showing that chemotherapy switches low-TIL tumors into high-TIL tumors.Citation33 Cytotoxic drugs are able to modify the tumor microenvironment, thus inducing cross-presentation of new peptide antigens, dendritic cell activation, and specific cytotoxic T cells.Citation41–Citation46 This evidence supports the idea that the efficacy of immunotherapy may be amplified by chemotherapy.Citation33 Based on these data, several neoadjuvant trials studying the addition of immunotherapy to chemotherapy in TNBC patients are ongoing.
Focusing on the subsets of TILs, there are two different functional components: cytotoxic CD8+ T cells and regulatory FOXP3+ T cells. CD8+ TILs lead to tumor cell death through linking foreign antigens on tumor cells.Citation47–Citation49 In contrast, FOXP3+ TILs, have a critical role in suppressing antitumor immunity. Miyashita et al published a retrospective multicenter study which evaluated CD8+ TIL, FOXP3+ TIL, and CD8/FOXP3 ratios before and after NST in TNBC tissue.Citation50,Citation51 The results showed that patients with high CD8+ TILs had a smaller residual tumor (≤2 cm) than patients with low-TILs (p = 0.005).Citation52 No association between residual tumor size and FOXP3+ TILs or the CD8/FOXP3 ratio was found. Both high CD8+ levels and higher CD8/FOXP3 ratio were associated with improved recurrence-free survival and breast-cancer-specific survival (p < 0.0001).Citation52 These data have been confirmed in a large meta-analysis, where the absence of both CD8+ TILs and FOXP3+ TILs were associated with worse disease-free survival (DFS) and overall survival (OS).Citation53
PD-1/PD-L1
The programmed cell death protein 1 (PD-1) is expressed on the surface of T cells, and is an immune checkpoint that inhibits T-cell effector function within tissues. PD-1 has two ligands known as PD-L1 and PD-L2; in particular, PD-L1 expression is present in several tumor types. The ligand between PD-L1 and PD-1 on the surface of a lymphocyte blocks the immune response against cancer cells.Citation54 The presence of PD-L1 in the tumor microenvironment seems to indicate an adaptive immune resistance to endogenous antitumor activity.Citation55 With regard to BC, PD-L1 expression has been found in 50% of all BC subtypes. Its expression was mainly associated with high histological grade and negative hormone receptors.Citation56 The first study to investigate PD-L1 expression (defined as cell-surface membrane staining >5%) conducted in BC found a higher PD-L1 expression in TNBCs as compared to non-TNBCs (p < 0.001).Citation57 In a large study, PD-L1 expression was found to be positive in 64% of the cell membrane, 80% of cytoplasm, and in 93% of tumor stroma in TNBCs. In these cases, PD-L1 expression was related to better survival outcomes.Citation58 Despite this evidence, it is well known that PD-L1 is a dynamic marker that changes rapidly over time. The tumor microenvironment, as well as systemic cytotoxic treatment and radiation, influence the immune system thereby determining PD-L1 expression changes. Therefore, a biopsy at one time point may not accurately reflect the real tumor microenvironment. For this reason, tumor PD-L1 expression can be considered to only reflect an immune-active microenvironment with activated T cells in an immunocompetent host, and is not an appropriate predictive biomarker to select patients for immunotherapeutic treatment.Citation59 Clinical data on the use of anti-PD-1 or anti-PD-L1 antibodies in different cancer subtypes showed how response is possible even in patients with low PD1/PD-L1 expression.Citation60–Citation64
Androgen receptor
The LAR TNBC is characterized by high androgen receptor (AR) and luminal cytokeratin expression.Citation21 Overall, ARs are expressed in 12%–36% of TNBCs.Citation65–Citation68 LAR BCs are usually associated with low grade and tumor size, mainly present in postmenopausal women.Citation69 Significantly better DFS, RFS, and OS have been reported on comparing LAR to non-LAR TNBCs.Citation21,Citation70,Citation71 AR expression seems to be a predictive biomarker for tumor resistance to chemotherapy. When considering neoadjuvant anthracycline/taxane-based chemotherapy, LAR tumors have the lowest pCR rate (0%–10%) as compared to other TNBCs.Citation21,Citation70,Citation71 On the other hand, AR expression could be considered a predictive marker for tumor response to antiandrogen therapies. Several preclinical studies demonstrated the sensitivity of the LAR cell line to antiandrogen medication.Citation21 Xenograft studies with the use of bicalutamide or enzalutamide support the hypothesis that anti-androgen therapy may be useful for such tumors.Citation21,Citation72 In the metastatic setting, clinical evidence suggested the efficacy of these two drugs in terms of clinical benefit rate and progression-free survival (PFS) in patients with AR-positive BC.Citation10,Citation11 A phase IIB study (NCT02689427) conducted in AR-positive TNBCs treated with enzalutamide plus placlitaxel in the neoadjuvant setting is currently ongoing.Citation73
Tumor suppressor gene p53
In the subgroups of TNBCs, BL tumors often overexpress genes that codify for proteins involved in cell-cycle and DNA-damage response. p53 is a tumor suppressor protein which plays a key role in apoptosis in response to DNA damage. The complex p53–p63 inhibits the activity of Rab7 – a protein involved in the degradation of EGFR which induces cell proliferation, angiogenesis, and inhibits apoptosis.Citation74 Available evidence suggests a possible relationship between p53 and BRCA1, with an increased frequency of p53 mutations in BRCA-related tumors.Citation3 p53-mutated tumors are characterized by aggressive tumor biology with poor differentiation, high tumor grade, and invasiveness.Citation75,Citation76 p53 overexpression seems to be associated with a worse prognosis in terms of OS and DFS, but with higher chemotherapy sensitivity.Citation75,Citation77–Citation80 With regard to TNBC, many studies have demonstrated that p53 is mutated in the majority (60%–88%) of these tumors.Citation81 The most frequent p53 mutations in TNBC are missense mutations with single-amino-acid substitution.Citation82 Bidard et al showed that a p53+/TNBC tumor treated with anthracyclines/alkylating agents had a higher probability of achieving pCR compared to other p53+/BC subtypes (p < 0.001).Citation83
Chemotherapy agents in the neoadjuvant setting
Cytotoxic chemotherapy is the backbone of TNBC treatment. In a large study evaluating the neoadjuvant setting, Liedtke et al evaluated the response to different neoadjuvant chemotherapy regimens in 1,118 patients with early-stage BC treated with different drugs.Citation84 In the subgroup of TNBC, the pCR rate was higher as compared to that among non-TNBC patients (22% vs 11%; p = 0.034), independent of chemotherapy regimens.Citation84 Actually, the standard of care in the neoadjuvant setting for TNBC is sequential anthracycline–taxane-based chemotherapy.Citation5 The pCR rate of these regimens ranges from 28% to 36%.Citation84–Citation86 To increase the rate of response, different chemotherapeutic strategies have been tested ().
Table 2 pCR rate due to different chemotherapy regimens reported in published clinical trials in TNBC patients
Weekly nanoparticle-albumin-bound paclitaxel (nab-paclitaxel) instead of weekly paclitaxel
Available evidence suggests a possible clinical benefit in terms of tumor response due to the introduction of nab-paclitaxel instead of weekly paclitaxel. In the phase III GeparSepto study, pCR was reached in 48% of TNBC patients treated with weekly nab-paclitaxel 150 mg/m2 versus 26% of patients treated with weekly paclitaxel 80 mg/m2 (p = 0.00027).Citation87 Of note, the dose of nab-paclitaxel was reduced from 150 to 125 mg/m2 due to the higher incidence of severe sensory neuropathy, without affecting the treatment efficacy.Citation87 A phase III trial (ETNA study) first presented at the the American Society of Clinical Oncology (ASCO) 2016 showed a higher rate of response in the nab-paclitaxel arm compared to the paclitaxel one (41.3% vs 35.5%; p-value not statistically significant).Citation88 Similar pCR rates have been reported by Kuwayama et al in a subgroup of TNBC patients treated with four cycles of weekly nab-paclitaxel 100 mg/m2.Citation89 Moreover, early results from the WSG-ADAPT trial showed a possible advantage in terms of pCR by adding nab-paclitaxel, rather than gemcitabine, to carboplatin (44.5 vs 28.4, p = 0.004).Citation22 Several clinical trials are currently further investigating the role of nab-paclitaxel in this setting.
Addition of platinum agents
The hypothesis of an increased efficacy of platinum agents in TNBC is based on the fact that these tumors often show functional BRCA1 alterations that increase the sensitivity to cross-linking agents.Citation90 Clinical evidence suggests that the addition of platinum to standard chemotherapy increases the rate of tumor response, but this clinical advantage has not been clearly translated into a survival benefit. Platinum-based chemotherapy has been investigated in several studies, but the best platinum agent, the ideal combination, or the best sequence with other chemotherapy agents remains unknown.Citation91–Citation93 In particular, a retrospective study that compared docetaxel with cisplatin or carboplatin showed the superiority of cisplatin in terms of OS (hazard ratio [HR] 0.49, p = 0.007) and PFS (HR 0.40, p = 0.018) with a quite good tolerability profile.Citation92 This difference between the two platinum agents was not confirmed in another large pooled analysis.Citation94 More consistent are the data on the increased response rate due to the addition of platinum to standard chemotherapy, mainly in anthracycline-free regimens.Citation95–Citation98 The subgroup analysis of five clinical trials, conducted in TNBC patients treated with neoadjuvant platinum-containing therapies combined with taxanes, showed a pCR rate ranging from 33% to 67%.Citation95–Citation99 These data are in accordance with the results from the GeparSixto study, where the addition of carboplatin to anthracycline or taxane-based therapy improved the pCR from 36.9% to 53.2%.Citation100 A large meta-analysis (included six randomized controlled trials and 22 retrospective or prospective studies) strongly confirmed the advantage due to platinum addition in both the objective response rate (86.7%) and the pCR rate (48.4%).Citation94 Data presented at the ASCO 2017 further underline the advantage in tumor response in patients treated with carboplatin/docetaxel compared to taxane–anthracycline-based regimen.Citation101 Data from the WSG-ADAPT TN trial suggested that immune marker gene expression (CD8, PD1, and PFDL1) and high-proliferation markers (proliferation score, Prosigna Breast Cancer Prognostic Gene Signature Assay [PAM-50] risk-of-recurrence [ROR] score, MKI67, CDC20, NUF2, KIF2C, CENPF, EMP3, and TYMS) were positively associated with pCR in carbo-containing chemotherapy regimens.Citation22 In all of these reported studies, the addition of carboplatin increased hematological and non-hematological toxicity, with consequent frequent dose reduction. Nowadays, the increased toxicity and the lack of clear demonstrated long-term survival benefit due to platinum addition constitute reasons why platinum agents are not included in the standard of care for TNBC in the neoadjuvant setting. Despite this, the evidence that the pCR is strongly associated with OS in TNBC is an argument often used by the physicians to justify the addition of carboplatin to NST in clinical practice. Several phase III trials are ongoing and may provide more information on this topic.
Eribulin in addition to carboplatin
Eribulin is a non-taxane microtubule inhibitor that causes irreversible cell-cycle blockade at the G2–M phase. Eribulin is approved in the management of metastatic BC after at least two treatment regimens with an anthracycline and a taxane, but its role in other settings is currently under investigation. A phase II clinical trial conducted in 30 TN early-stage BC patients investigated the response rate to 3-weekly carboplatin AUC 6 plus eribulin 1.4 mg/m2 (days 1 and 8 every 21 days).Citation102 In total, 80% of enrolled patients had a clinical complete or partial response, and 43% achieved pCR.Citation102 Moreover, another phase II international trial (NCT01372579) is ongoing with the aim to investigate the efficacy of a preoperative eribulin mesylate and carboplatin combination in stages I–III TNBCs.Citation103
Dose-dense chemotherapy
Dose-dense (DD) chemotherapy aims to achieve maximum tumor death by delivering therapeutic drugs over a shorter duration. The efficacy of DD systemic treatment was mainly investigated in the adjuvant setting. A recent meta-analysis including a total of eight phase III trials (17,188 randomized women) showed that patients treated with DD chemotherapy had better OS and DFS than those on the conventional schedule. In particular, statistically significant OS benefit was observed in patients with hormone-receptor-negative tumors (HR 0.8, p = 0.002).Citation104 Data from the DD schedule in the neoadjuvant setting are less consistent.Citation105 Published clinical trials included women treated with outdated regimens and/or schedules; there are no data regarding the benefit of DD anthracycline–taxane-based primary chemotherapy. Conven-tionally, in clinical practice, results from DD adjuvant chemotherapy studies are applied in the neoadjuvant setting too.
Targeted agents tested in neoadjuvant setting
summarizes the main clinical trials where targeted agents have been evaluated in addition to NST.
Table 3 pCR rate TNBC patients treated with chemotherapy plus targeted agents
PARP-1 inhibitors
PARP-1 is an enzyme known to be involved in the base-excision repair pathway, which plays a key role in the repair of single-stranded DNA breaks.Citation106,Citation107 During the last decade, drugs able to interfere with the DNA-damage-repair systems and to induce a synthetic lethality, named PARP inhibitors (such as iniparib, olaparib, and veliparib), have been developed. The main evidence is in the metastatic setting, where PARP inhibitors have been tested as single agents and in combination with chemotherapy.Citation9,Citation108 The best results in terms of efficacy emerged from combination with cisplatin or carboplatin, as well as with topotecan and temozolamide, with response rates in BRCA-related BC of up to 73%.Citation109–Citation112 Considering the use of PARP inhibitors in the neoadjuvant setting, a single-arm phase II study showed efficacy in terms of pCR of gemcitabine combined with carboplatin and iniparib in TNBC.Citation113 In this study, the presence of HRD was associated with higher response rates, regardless of BRCA 1/2 mutational status.Citation113 Results from the veliparib and carboplatin arm in the I-SPY-2 trial, a multicenter, adaptively randomized trial, reported 51% pCR in the experimental arm versus 26% in the standard regimen. Considering adverse events, hematological side effects were higher in the veliparib–carboplatin group than in the control arm.Citation114 No difference in the pCR rate due to the addition of velaparib to carboplatin–paclitaxel, followed by doxorubicin plus cyclophosphamide, has been reported in a phase III study presented by the German Breast Group at the ASCO 2017.Citation115 A phase II study of neoadjuvant talazoparib monotherapy in BRCA-associated BC is ongoing at the MD Anderson Cancer Center.Citation116 Considering these preliminary controversial results, PARP inhibitors are still under investigation.
Anti-angiogenic agents
Bevacizumab is a humanized monoclonal antibody that targets the main isoforms of circulating vascular endothelial growth factor (VEGF), resulting in the inhibition of angiogenesis, cell tumor growth, and cell survival.Citation117 Bevacizumab use has been investigated in both advanced and early-stage BC treatments, showing an increased response rate – mainly, in TNBC patients.Citation84,Citation100,Citation118–Citation120 When added to chemotherapy in preoperative treatment, the pCR rate ranges from 40% to 59% independent of the chemotherapy regimen administered. The phase III GeparQuinto trial included 663 TNBC patients treated with epirubicin and cyclophosphamide followed by docetaxel with or without bevacizumab, and showed a pCR rate of 39.3% in the bevacizumab arm versus 27.9% in the control arm (p = 0.021).Citation7 The advantage in response rate due to the addition of bevacizumab has been demonstrated in two other large trials. The first one is the multicenter British phase III study (ARTemis), where 781 patients were randomized to receive bevacizumab or placebo plus docetaxel followed by cyclophosphamide, 5-fluorouracil, and epirubicine.Citation121 In the TNBC subgroup, bevacizumab provided an advantage in terms of pCR from 34% to 49%.Citation121 The second one – the CALGB 40603/Alliance trial, conducted in 443 patients with stages II and III TNBC – confirmed the increase of tumor response in the bevacizumab group, independent of the chemotherapy regimen administered.Citation122,Citation123 Similar response rates have been found in two phase II trials: the Ca.Pa.Be study, where 44 TNBC women were treated with a combination of paclitaxel, carboplatin, and bevacizumab, and the KCSG BR-0905 trial, where 45 women were treated with bevacizumab, docetaxel, and carboplatin.Citation124,Citation125 The addition of bevacizumab to nab-paclitaxel was investigated in two phase II trials, showing an increase of response rate compared to bevacizumab plus paclitaxel or docetaxel.Citation126,Citation127 In the first one, the SWOG S0800 trial, the combination of bevacizumab plus nab-paclitaxel, followed by DD doxorubicin and cyclophosphamide, increased the pCR rate up to 59% (p = 0.014).Citation126 In the second one, 50% of TNBC patients treated with bevacizumab plus nab-paclitaxel and carboplatin achieved pCR.Citation127 With regard to safety profile, patients treated with bevacizumab experienced an increased number of immediate and delayed postoperative complications as well as neutropenia and hypertension.Citation121,Citation122 Nowadays, the use of bevacizumab in the neoadjuvant setting is still controversial and not recommended, mainly due to the lack of survival-benefit evidence.
Immunotherapy
The evidence that stimulating the immune cells might, therefore, be an option to increase response rates is the rationale for designing clinical trials with the addition of immunotherapy in the neoadjuvant setting. Preliminary results from the KEYNOTE-173 presented at the ASCO 2017 (nab-paclitaxel ± carboplatin plus pembrolizumab, followed by cyclophosphamide and doxorubicin) suggested promising antitumor activity of pembrolizumab when combined with NST.Citation128
The objective response rate before surgery was 100% in the pembrolizumab and carboplatin group versus 80% in the other experimental group (nab-paclitaxel + pembrolizumab); the pCR rate (yT0/Tis yN0) was 90% versus 60%, respectively.Citation128 Similar results have been reported in the subgroup of patients treated with pembrolizumab in the I-SPY-2 trial.Citation129 Data presented at the ASCO 2017 were based on results observed in patients at high risk of relapse using upfront tumor profiling (including mammaPrint 70-gene signature test). Patients were treated with weekly paclitaxel for 12 weeks ± pembrolizumab, followed by anthracyclines.Citation129 In the TNBC women, an absolute increase in the estimated pCR rate of 40% was observed in the pembrolizumab arm (based on the estimated pCR rate of 60% with pembrolizumab plus standard therapy compared to 20% with standard NST alone).Citation129 Currently, two different strategies are under investigation to evaluate the real benefit of immunotherapy in early-stage TNBC: the addition of PD1/PD-L1 inhibitors to different NST regimens and the administration of PD1/PD-L1 inhibitors in the adjuvant setting in patients with residual BC disease after NST. In the first case, four studies are currently recruiting patients: the phase III NeoTRIPaPDL1 trial, a multicenter randomized study with patients treated with nab-paclitaxel plus carboplatin ± atezolizumab;Citation130 the GeparNuevo trial, a phase II study of nab-paclitaxel ± durvalumab followed by epirubicin plus cyclophosphamide; and two other studies with nab-paclitaxel plus atezolizumab or durvalumab.Citation131–Citation133 With regard to the second strategy, two big clinical trials are now ongoing, both conducted in high-risk TNBC patients with residual disease after NST, randomized to receive 1 year of adjuvant pembrolizumab or avelumab versus observation.Citation134,Citation135 The results of all these studies are awaited with high interest.
Conclusion
According to current international guidelines, in early-stage TNBC, the timing of treatment (pre- vs postoperative) has no effect on long-term outcomes. All chemotherapy strategies used in adjuvant treatment may also be used preoperatively. If a primary chemotherapy treatment is used, it is recommended to deliver all planned treatment without unnecessary breaks, irrespective of the magnitude of tumor response.Citation136,Citation137
In our opinion, NST should be the first option in the case of operable TNBC, especially in locally advanced cases (when mastectomy is required due to tumor size), as well as in high-grade and high-proliferation-rate tumors. Despite the progress in our understanding of TNBC, anthracycline–taxane-based chemotherapy remains the standard of care for NST in all TNBC subtypes. Platinum agents, as well as PARP-inhibitor agents, provide pCR advantage in different clinical trials, mainly in BRCA-defense tumors, without demonstrating an improvement in survival benefit. At present, there are no clear predictive biomarkers useful in clinical practice. The classification of TNBC using molecular profile showed how TNBCs are a heterogeneous group which explains the lack of survival benefit of experimental drugs tested in several clinical trials. All of the available evidence suggests the necessity of design biology-driven clinical trials wherein TNBC patients may be treated on the basis of tumor molecular profile.
Acknowledgments
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
- EstellerMEpigenetics in cancerN Engl J Med2008358111148115918337604
- KennedyRDQuinnJEJohnstonPGHarkinDPBRCA1: mechanisms of inactivation and implications for management of patientsLancet200236093381007101412383682
- BirgisdottirVStefanssonOABodvarsdottirSKHilmarsdottirHJonassonJGEyfjordJEEpigenetic silencing and deletion of the BRCA1 gene in sporadic breast cancerBreast Cancer Res200684R3816846527
- BalmañaJDíezORubioITCardosoFESMO Guidelines Working GroupBRCA in breast cancer: ESMO clinical practice guidelinesAnn Oncol201122Suppl 6vi31vi3421908500
- SenkusEKyriakidesSOhnoSESMO Guidelines CommitteePrimary breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-upAnn Oncol201526Suppl 5v8v3026314782
- HuoberJvon MinckwitzGDenkertCEffect of neoadjuvant anthracycline-taxane-based chemotherapy in different biological breast cancer phenotypes: overall results from the GeparTrio studyBreast Cancer Res Treat2010124113314020697801
- GerberBLoiblSEidtmannHGerman Breast Group InvestigatorsNeoadjuvant bevacizumab and anthracycline-taxane-based chemotherapy in 678 triple-negative primary breast cancers; results from the geparquinto study (GBG 44)Ann Oncol201324122978298424136883
- YardleyDAShipleyDLPeacockNWPhase I/II trial of neo-adjuvant sunitinib administered with weekly paclitaxel/carboplatin in patients with locally advanced triple-negative breast cancerBreast Cancer Res Treat2015152355756726155975
- TuttARobsonMGarberJEOral poly(ADP-ribose) polymerase inhibitor olaparib in patients with BRCA1 or BRCA2 mutations and advanced breast cancer: a proof-of-concept trialLancet2010376973723524420609467
- GucalpATolaneySIsakoffSJTranslational Breast Cancer Research Consortium (TBCRC 011)Phase II Trial of bicalutamide in patients with androgen receptor-positive, estrogen receptor-negative metastatic breast cancerClin Cancer Res201319195505551223965901
- TrainaTAMillerKYardleyDAResults from a phase 2 study of enzalutamide (ENZA), an androgen receptor (AR) inhibitor, in advanced AR+ triple-negative breast cancer (TNBC)J Clin Oncol201533Suppl 15 abstract 1003
- NabholtzJMAbrialCMouret-ReynierMAMulticentric neoadjuvant phase II study of panitumumab combined with an anthracycline/taxane-based chemotherapy in operable triple-negative breast cancer: identification of biologically defined signatures predicting treatment impactAnn Oncol20142581570157724827135
- HafftyBGYangQReissMLocoregional relapse and distant metastasis in conservatively managed triple negative early-stage breast cancerJ Clin Oncol200624365652565717116942
- D’AndreaADGrompeMThe Fanconi anaemia/BRCA pathwayNat Rev Cancer200331233412509764
- ByrskiTHuzarskiTDentRPathologic complete response to neoadjuvant cisplatin in BRCA1-positive breast cancer patientsBreast Cancer Res Treat2014147240140525129345
- WangCZhangJWangYPrevalence of BRCA1 mutations and responses to neoadjuvant chemotherapy among BRCA1 carriers and non-carriers with triple-negative breast cancerAnn Oncol201526352352825480878
- FarmerHMcCabeNLordCJTargeting the DNA repair defect in BRCA mutant cells as a therapeutic strategyNature2005434703591792115829967
- SilverDPRichardsonALEklundACEfficacy of neoadjuvant Cisplatin in triple-negative breast cancerJ Clin Oncol20102871145115320100965
- ChabalierCLamareCRaccaCPrivatMValetteALarminatFBRCA1 downregulation leads to premature inactivation of spindle checkpoint and confers paclitaxel resistanceCell Cycle2006591001100716639080
- TelliMLTimmsKMReidJHomologous recombination deficiency (HRD) as a predictive biomarkers of response to neoadjuvant platinum-based therapy in patients with triple negative breast cancerCancer Res2016764 Suppl P3-07-12
- LehmannBDBauerJAChenXIdentification of human triple-negative breast cancer subtypes and preclinical models for selection of targeted therapiesJ Clin Invest201112172750276721633166
- GluzONitzULiedtkeCComparison of 12 weeks neoadjuvant Nab-paclitaxel combined with carboplatinum vs. gemcitabine in triple-negative breast cancer: WSG-ADAPT TN randomized phase II trialCancer Res2016764 Suppl Abstract nr S6-07
- HerbstRSReview of epidermal growth factor receptor biologyInt J Radiat Oncol Biol Phys2004592 Suppl2126
- ZhangHBerezovAWangQErbB receptors: from oncogenes to targeted cancer therapiesJ Clin Invest200711782051205817671639
- SiziopikouKPCobleighMThe basal subtype of breast carcinomas may represent the group of breast tumors that could benefit from EGFR-targeted therapiesBreast200716110410717097880
- BidardFCConfortiRBouletTMichielsSDelalogeSAndréFDoes triple-negative phenotype accurately identify basal-like tumour? An immunohistochemical analysis based on 143 ‘triple-negative’ breast cancersAnn Oncol20071871285128617675400
- NogiHKobayashiTSuzukiMEGFR as paradoxical predictor of chemosensitivity and outcome among triple-negative breast cancerOncol Rep200921241341719148516
- LiuDHeJYuanZEGFR expression correlates with decreased disease-free survival in triple negative breast cancer: a retrospective analysis based on a tissue microarrayMed Oncol201229240140521264531
- FerraroDAGaboritNMaronRInhibition of triple-negative breast cancer models by combinations of antibodies to EGFRProc Natl Acad Sci U S A201311051815182023319610
- DisisMLStantonSETriple-negative breast cancer: immune modulation as the new treatment paradigmAm Soc Clin Oncol Educ Book2015e25e3025993181
- García-TeijidoPCabalMLFernándezIPPérezYFTumor-infiltrating lymphocytes in triple negative breast cancer: the future of immune targetingClin Med Insights Oncol201610Suppl 1313927081325
- DenkertCLoiblSNoskeATumor-associated lymphocytes as an independent predictor of response to neoadjuvant chemotherapy in breast cancerJ Clin Oncol201028110511319917869
- DieciMVCriscitielloCGoubarAPrognostic value of tumor-infiltrating lymphocytes on residual disease after primary chemotherapy for triple-negative breast cancer: a retrospective multicenter studyAnn Oncol201425361161824401929
- VinayakSGrayRJAdamsSAssociation of increased tumor-infiltrating lymphocytes (TILs) with immunomodulatory (IM) triple-negative breast cancer (TNBC) subtype and response to neoadjuvant platinum-based therapy in PrECOG0105J Clin Oncol201432Suppl 15 abstract 1000
- SalgadoRDenkertCDemariaSInternational TILs Working Group 2014The evaluation of tumor-infiltrating lymphocytes (TILS) in breast cancer: Recommendations by an International TILS Working Group 2014Ann Oncol201526225927125214542
- PruneriGVingianiABagnardiVClinical validity of tumor-infiltrating lymphocytes analysis in patients with triple-negative breast cancerAnn Oncol201627224925626598540
- LoiSMichielsSSalgadoRTumor infiltrating lymphocytes are prognostic in triple negative breast cancer and predictive for trastuzumab benefit in early breast cancer: results from the FinHER trialAnn Oncol20142581544155024608200
- AdamsSGrayRJDemariaSPrognostic value of tumor-infiltrating lymphocytes in triple-negative breast cancers from two phase III randomized adjuvant breast cancer trials: ECOG 2197 and ECOG 1199J Clin Oncol201432272959296625071121
- Cimino-MathewsAFooteJBEmensLAImmune targeting in breast cancerOncology (Williston Park)201529537538525979549
- DenkertCvon MinckwitzGDarb-EsfahaniSEvaluation of tumor-infiltrating lymphocytes (TILs) as predictive and prognostic biomarker in different subtypes of breast cancer treated with neoadjuvant therapy – a metaanalysis of 3771 patientsCancer Res2017774 Suppl Abstract nr S1-09
- ZitvogelLApetohLGhiringhelliFAndréFTesniereAKroemerGThe anticancer immune response: indispensable for therapeutic success?J Clin Invest200811861991200118523649
- RoselliMCeredaVdi BariMGEffects of conventional therapeutic interventions on the number and function of regulatory T cellsOncoimmunology2013210e2702524353914
- JägerDJägerEKnuthAImmune responses to tumour antigens: implications for antigen specific immunotherapy of cancerJ Clin Pathol200154966967411533070
- SchreiberRDOldLJSmythMJCancer immunoediting: integrating immunity’s roles in cancer suppression and promotionScience201133160241565157021436444
- ApetohLGhiringhelliFTesniereAToll-like receptor 4-dependent contribution of the immune system to anticancer chemotherapy and radiotherapyNat Med20071391050105917704786
- AndreFDieciMVDubskyPMolecular pathways: involvement of immune pathways in the therapeutic response and outcome in breast cancerClin Cancer Res2013191283323258741
- BerkeGThe binding and lysis of target cells by cytotoxic lymphocytes: molecular and cellular aspectsAnnu Rev Immunol1994127357738011296
- SegalNHParsonsDWPeggsKSEpitope landscape in breast and colorectal cancerCancer Res200868388989218245491
- ZitvogelLKeppOKroemerGImmune parameters affecting the efficacy of chemotherapeutic regimensNat Rev Clin Oncol20118315116021364688
- LiyanageUKMooreTTJooHGPrevalence of regulatory T cells is increased in peripheral blood and tumor microenvironment of patients with pancreas or breast adenocarcinomaJ Immunol200216952756276112193750
- ViguierMLemaîtreFVerolaOFoxp3 expressing CD4+CD25(high) regulatory T cells are overrepresented in human metastatic melanoma lymph nodes and inhibit the function of infiltrating T cellsJ Immunol200417321444145315240741
- MiyashitaMSasanoHTamakiKPrognostic significance of tumor-infiltrating CD8+ and FOXP3+ lymphocytes in residual tumors and alterations in these parameters after neoadjuvant chemotherapy in triple-negative breast cancer: a retrospective multicenter studyBreast Cancer Res20151712426341640
- IbrahimEMAl-FoheidiMEAl-MansourMMKazkazGAThe prognostic value of tumor-infiltrating lymphocytes in triple-negative breast cancer: a meta-analysisBreast Cancer Res Treat2014148346747625361613
- PardollDMThe blockade of immune checkpoints in cancer immunotherapyNat Rev Cancer201212425226422437870
- WimberlyHBrownJRSchalperKPD-L1 expression correlates with tumor-infiltrating lymphocytes and response to neoadjuvant chemotherapy in breast cancerCancer Immunol Res20153432633225527356
- GhebehHMohammedSAl-OmairAThe B7-H1 (PD-L1) T lymphocyte-inhibitory molecule is expressed in breast cancer patients with infiltrating ductal carcinoma: correlation with important high-risk prognostic factorsNeoplasia20068319019816611412
- MittendorfEAPhilipsAVMeric-BernstamFPD-L1 expression in triple-negative breast cancerCancer Immunol Res20142436137024764583
- BeckersRKSelingerCIVilainRProgrammed death ligand 1 expression in triple-negative breast cancer is associated with tumour-infiltrating lymphocytes and improved outcomeHistopathology2016691253426588661
- MengXHuangZTengFXingLYuJPredictive biomarkers in PD-1/PD-L1 checkpoint blockade immunotherapyCancer Treat Rev2015411086887626589760
- RobertCLongGVBradyBNivolumab in previously untreated melanoma without BRAF mutationN Engl J Med2015372432033025399552
- BrahmerJReckampKLBaasPNivolumab versus docetaxel in advanced squamous-cell non-small-cell lung cancerN Engl J Med2015373212313526028407
- BorghaeiHPaz-AresLHornLNivolumab versus docetaxel in advanced nonsquamous non-small-cell lung cancerN Engl J Med2015373171627163926412456
- MotzerRJEscudierBMcDermottDFCheckMate 025 InvestigatorsNivolumab versus everolimus in advanced renal-cell carcinomaN Engl J Med2015373191803181326406148
- FerrisRLBlumenscheinGJrFayetteJNivolumab for recurrent squamous-cell carcinoma of the head and neckN Engl J Med2016375191856186727718784
- CollinsLCColeKsMarottiJDHuRSchnittSJTamimiRMAndrogen receptor expression in breast cancer in relation to molecular phenotype: results from the Nurses’ Health StudyMod Pathol201124792493121552212
- MrklićIPogorelićZCapkunVTomićSExpression of androgen receptors in triple negative breast carcinomasActa Histochem2013115434434823031358
- ThikeAAYong-Zheng ChongLCheokPYLoss of androgen receptor expression predicts early recurrence in triple-negative and basal-like breast cancerMod Pathol201427335236023929266
- SafarpourDPakneshanSTavassoliFAAndrogen receptor (AR) expression in 400 breast carcinomas: is routine AR assessment justified?Am J Cancer Res201444353368 eCollection 201425057438
- AgoffSNSwansonPELindenHHawesSELawtonTJAndrogen receptor expression in estrogen receptor–negative breast cancer. Immunohistochemical, clinical, and prognostic associationsAm J Clin Pathol2003120572573114608899
- ParkSKooJParkHSExpression of androgen receptors in primary breast cancerAnn Oncol201021348849219887463
- MasudaHBaggerlyKAWangYDifferential response to neoadjuvant chemotherapy among 7 triple-negative breast cancer molecular subtypesClin Cancer Res201319195533554023948975
- CochraneDRBernalesSJacobsenBMRole of the androgen receptor in breast cancer and preclinical analysis of enzalutamideBreast Cancer Res2014161R724451109
- M.D. Anderson Cancer CenterPhase IIB neoadjuvant enzalutamide (ZT) plus taxol for androgen receptor (AR)-positive triple-negative breast cancer (AR+ TNBC) Available from: https://clinicaltrials.gov/ct2/show/NCT02689427. NLM identifier: NCT02689427Accessed December 8, 2017
- CeresaBPBahrSJrab7 activity affects epidermal growth factor: epidermal growth factor receptor degradation by regulating endocytic trafficking from the late endosomeJ Biol Chem200628121099110616282324
- GuarneriVBarbieriEPiacentiniFPredictive and prognostic role of p53 according to tumor phenotype in breast cancer patients treated with preoperative chemotherapy: a single-institution analysisInt J Biol Markers201025210411120544688
- YadavBSChananaPJhambSBiomarkers in triple negative breast cancer: a reviewWorld J Clin Oncol20156625226326677438
- HanJSCaoDMolbergKHHormone receptor status rather than HER2 status is significantly associated with increased Ki-67 and p53 expression in triple-negative breast carcinomas, and high expression of Ki-67 but not p53 is significantly associated with axillary nodal metastasis in triple-negative and high-grade non-triple-negative breast carcinomasAm J Clin Pathol2011135223023721228363
- LangerødAZhaoHBorganØTP53 mutation status and gene expression profiles are powerful prognostic markers of breast cancerBreast Cancer Res200793R3017504517
- MillerLDSmedsJGeorgeJAn expression signature for p53 status in human breast cancer predicts mutation status, transcriptional effects, and patient survivalProc Natl Acad Sci U S A200510238135501355516141321
- BiganzoliECoradiniDAmbrogiFp53 status identifies two subgroups of triple-negative breast cancers with distinct biological featuresJpn J Clin Oncol201141217217921199790
- TurnerNMorettiESiclariOTargeting triple negative breast cancer: is p53 the answer?Cancer Treat Rev201339554155023321033
- WalerychDNapoliMCollavinLDel SalGThe rebel angel: mutant p53 as the driving oncogene in breast cancerCarcinogenesis201233112007201722822097
- BidardFCMatthieuMCCholletPp53 status and efficacy of primary anthracyclines/alkylating agent-based regimen according to breast cancer molecular classesAnn Oncol20081971261126518325917
- LiedtkeCMazouniCHessKRResponse to neoadjuvant therapy and long-term survival in patients with triple-negative breast cancerJ Clin Oncol20082681275128118250347
- von MinckwitzGUntchMNüeschEImpact of treatment characteristics on response of different breast cancer phenotypes: pooled analysis of the German neo-adjuvant chemotherapy trialsBreast Cancer Res Treat2011125114515621042932
- von MinckwitzGUntchMBlohmerJUDefinition and impact of pathologic complete response on prognosis after neoadjuvant chemotherapy in various intrinsic breast cancer subtypesJ Clin Oncol201230151796180422508812
- UntchMJackischCSchneeweissAGerman Breast Group (GBG); Arbeitsgemeinschaft Gynäkologische Onkologie—Breast (AGO-B) InvestigatorsNab-paclitaxel versus solvent-based paclitaxel in neoadjuvant chemotherapy for early breast cancer (GeparSepto-GBG 69): a randomised, phase 3 trialLancet Oncol201617334535626869049
- GianniLMansuttiMAntonAETNA (evaluating treatment with neoadjuvant abraxane) randomized phase III study comparing neoadjuvant nab-paclitaxel (nab-P) versus paclitaxel (P) both followed by anthracycline regimens in women with HER2-negative high-risk breast cancer: a MICHELANGO studyJ Clin Oncol201634Suppl 15 abstract 502
- KuwayamaTYamauchiHTakanoTPrimary analysis of a randomized phase II, multicenter trial: neoadjuvant weekly nab-paclitaxel 100 mg/m2 followed by FE100C compared with docetaxel 75 mg/m2 followed by FE100C for early breast cancer in JapanJ Clin Oncol201533Suppl 28 abstract 136
- StefanssonOAVillanuevaAVidalAMartíLEstellerMBRCA1 epigenetic inactivation predicts sensitivity to platinum-based chemotherapy in breast and ovarian cancerEpigenetics20127111225122923069641
- ChenXSYuanYGarfieldDHWuJYHuangOShenKWBoth carboplatin and bevacizumab improve pathological complete remission rate in neoadjuvant treatment of triple negative breast cancer: a meta-analysisPLoS One201499e10840525247558
- HurleyJReisIMRodgersSEThe use of neoadjuvant platinum-based chemotherapy in locally advanced breast cancer that is triple negative: retrospective analysis of 144 patientsBreast Cancer Res Treat2013138378379423542956
- von MinckwitzGMartinMNeoadjuvant treatments for triple-negative breast cancer (TNBC)Ann Oncol201223Suppl 6vi35vi3923012300
- PetrelliFCoinuABorgonovoKThe value of platinum agents as neoadjuvant chemotherapy in triple-negative breast cancers: a systematic review and meta-analysisBreast Cancer Res Treat2014144222323224557340
- SikovWMDizonDSStrengerRFrequent pathologic complete responses in aggressive stages II to III breast cancers with every-4-week carboplatin and weekly paclitaxel with or without trastuzumab: a Brown University Oncology Group StudyJ Clin Oncol200927284693470019720916
- ChenXSNieXQChenCMWeekly paclitaxel plus carboplatin is an effective nonanthracycline-containing regimen as neoadjuvant chemotherapy for breast cancerAnn Oncol201021596196720211870
- RoyVPockajBAAllredJBA Phase II trial of docetaxel and carboplatin administered every 2 weeks as preoperative therapy for stage II or III breast cancer: NCCTG study N0338Am J Clin Oncol201336654054422868240
- ChangHRGlaspyJAllisonMADifferential response of triple-negative breast cancer to a docetaxel and carboplatin-based neoadjuvant treatmentCancer2010116184227423720549829
- Campos GomezSCampos GomezKAGarcia GarcesMMorelosGHernandez AlvarezJNeoadjuvant carboplatin and docetaxel in locally advanced triple negative breast cancer: a Hispanic trialJ Clin Oncol201634Suppl 15 abstract e12554
- von MinckwitzGSchneeweissALoiblSNeoadjuvant carboplatin in patients with triple-negative and HER2-positive early breast cancer (GeparSixto; GBG 66): a randomised phase 2 trialLancet Oncol201415774775624794243
- EnriquezDPoma NietoNFuentesHAGuerraHRuiz MendozaREGomezHLImproving pathological response in locally advanced triple negative breast cancer: comparison between CbD and AC-T regimensJ Clin Oncol201735Suppl 15 abstract 585
- KaklamaniVGJerussJSHughesEPhase II neoadjuvant clinical trial of carboplatin and eribulin in women with triple negative early-stage breast cancer (NCT01372579)Breast Cancer Res Treat2015151362963826006067
- Northwestern UniversityCarboplatin and eribulin mesylate in triple negative breast cancer patients Avalaible from: https://clinicaltrials.gov/ct2/show/NCT01372579. NLM identifier: NCT01372579Accessed June 1, 2011
- PetrelliFCabidduMCoinuAAdjuvant dose-dense chemotherapy in breast cancer: a systematic review and meta-analysis of randomized trialsBreast Cancer Res Treat2015151225125925917869
- ReinischMAtasevenBKümmelSNeoadjuvant dose-dense and dose-intensified chemotherapy in breast cancer – review of the literatureBreast Care (Basel)2016111132027051390
- HastakKAlliEFordJMSynergistic chemosensitivity of triple-negative breast cancer cell lines to poly(ADP-Ribose) polymerase inhibition, gemcitabine and cisplatinCancer Res201070207970798020798217
- AlliESharmaVBSunderesakumarPFordJMDefective repair of oxidative dna damage in triple-negative breast cancer confers sensitivity to inhibition of Poly(ADP-ribose) polymeraseCancer Res20096983589359619351835
- GelmonKATischkowitzMMackayHOlaparib in patients with recurrent high-grade serous or poorly differentiated ovarian carcinoma or triple-negative breast cancer: a phase 2, multicentre, open-label, non-randomised studyLancet Oncol201112985286121862407
- BalmañaJTungNMIsakoffSJPhase I trial of olaparib in combi-nation with cisplatin for the treatment of patients with advanced breast, ovarian and other solid tumorsAnn Oncol20142581656166324827126
- SomloGFrankelPHLuuTHEfficacy of the combination of ABT-888 (veliparib) and carboplatin in patients with BRCA-associated breast cancerJ Clin Oncol201331Suppl 15 abstract 1024
- PahujaSBeumerJHApplemanLJA phase I study of veliparib (ABT-888) in combination with weekly carboplatin and paclitaxel in advanced solid malignancies and enriched for triple-negative breast cancer (TNBC)J Clin Oncol201533Suppl 15 abstract 1015
- KummarSChenAJiJPhase I study of PARP inhibitor ABT-888 in combination with topotecan in adults with refractory solid tumors and lymphomasCancer Res201171175626563421795476
- TelliMLJensenKCVinayakSPhase II study of gemcitabine, carboplatin, and iniparib as neoadjuvant therapy for triple-negative and BRCA1/2 mutation-associated breast cancer with assessment of a tumor-based measure of genomic instability: PrECOG 0105J Clin Oncol201533171895190125847929
- RugoHSOlapadeODeMicheleAVeliparib/carboplatin plus standard neoadjuvant therapy for high-risk breast cancer: first efficacy results from the I-SPY 2 TRIALCancer Res20137324 Suppl Abstract nr S5-02
- GeyerCEO’ShaughnessyJUntchMPhase 3 study evaluating efficacy and safety of veliparib (V) plus carboplatin (Cb) or Cb in combination with standard neoadjuvant chemotherapy (NAC) in patients (pts) with early stage triple-negative breast cancer (TNBC)J Clin Oncol201735Suppl 15 abstract 520
- M.D. Anderson Cancer CenterNeoadjuvant talazoparib for patients with a BRCA deleterious mutation Available from: https://clinical-trials.gov/ct2/show/NCT02282345. NLM Identifier: NCT02282345Accessed October 30, 2014
- GreenbergSRugoHSTriple-negative breast cancer: role of antiangiogenic agentsCancer J2010161333820164688
- von MinckwitzGEidtmannHRezaiMGerman Breast Group; Arbeitsgemeinschaft Gynäkologische Onkologie–Breast Study GroupsNeoadjuvant chemotherapy and bevacizumab for HER2-negative breast cancerN Engl J Med2012366429930922276820
- ThomssenCPiergaJYPritchardKIFirst-line bevacizumab-containing therapy for triple-negative breast cancer: analysis of 585 patients treated in the ATHENA studyOncology201282421822722508241
- O’ShaughnessyJRomieuGDiérasVByrtekMDuenneA-AMilesDMeta-analysis of patients with triple-negative breast cancer (TNBC) from three randomized trials of first-line bevacizumab (BV) and chemotherapy treatment for metastatic breast cancer (MBC)Cancer Res20107024 Suppl P6-12-03
- EarlHMHillerLDunnJAARTemis InvestigatorsEfficacy of neoadjuvant bevacizumab added to docetaxel followed by fluorouracil, epirubicin, and cyclophosphamide, for women with HER2-negative early breast cancer (ARTemis): an open-label, randomised, phase 3 trialLancet Oncol201516665666625975632
- SikovWMBerryDAPerouCMImpact of the addition of carboplatin and/or bevacizumab to neoadjuvant once-per-week paclitaxel followed by dose-dense doxorubicin and cyclophosphamide on pathologic complete response rates in stage II to III triple-negative breast cancer: CALGB 40603 (Alliance)J Clin Oncol2015331132125092775
- GolshanMCirrincioneCTCareyLAImpact of neoadjuvant therapy on breast conservation rates in triple-negative and HER2-positive breast cancer: combined results of CALGB 40603 and 40601 (Alliance)J Clin Oncol201533Suppl 15abstract 1007
- GuarneriVDieciMVBisagniGPreoperative carboplatin-paclitaxel-bevacizumab in triple-negative breast cancer: final results of the phase II Ca.Pa.Be studyAnn Surg Oncol20152292881288725572687
- KimHRJungKHImSAMulticentre phase II trial of bevacizumab combined with docetaxel-carboplatin for the neoadjuvant treatment of triple-negative breast cancer (KCSG BR-0905)Ann Oncol20132461485149023380385
- NahlehZABarlowWEHayesDFSWOG S0800 (NCI CDR0000636131): addition of bevacizumab to neoadjuvant nab-paclitaxel with dose-dense doxorubicin and cyclophosphamide improves pathologic complete response (pCR) rates in inflammatory or locally advanced breast cancerBreast Cancer Res Treat2016158348549527393622
- MrózekELaymanRRamaswamyBPhase II trial of neo-adjuvant weekly nanoparticle albumin-bound paclitaxel, carboplatin, and biweekly bevacizumab therapy in women with clinical stage II or III HER2-negative breast cancerClin Breast Cancer201414422823424703985
- SchmidPParkYHMuñoz-CouseloEPembrolizumab (pembro) + chemotherapy (chemo) as neoadjuvant treatment for triple negative breast cancer (TNBC): preliminary results from KEYNOTE-173J Clin Oncol201735Suppl 15 abstract 556
- NandaRLiuMCYauCPembrolizumab plus standard neoadjuvant therapy for high-risk breast cancer (BC): results from I-SPY 2J Clin Oncol201735Suppl 15 abstract 506
- Fondazione MichelangeloNeoadjuvant therapy in TRIPle negative breast cancer with antiPDL1 (NeoTRIPaPDL1) Available from: https://clinicaltrials.gov/ct2/show/NCT02620280. NLM Identifier: NCT02620280Accessed November 3, 2015
- M.D. Anderson Cancer CenterTriple-negative first-line study: neoadjuvant trial of nab-paclitaxel and MPDL3280A, a Pdl-1 inhibitor in patients with triple negative breast cancer Avalaible from: https://clinicaltrials.gov/ct2/show/NCT02530489. NLM Identifier: NCT02530489Accessed August 19, 2015
- Yale UniversityNeoadjuvant MEDI4736 concomitant with weekly nab-paclitaxel and dose-dense AC for stage I–III triple negative breast cancer Available from: https://clinicaltrials.gov/ct2/show/NCT02489448 NLM Identifier: NCT02489448Accessed July 1, 2015
- Merck Sharp & Dohme CorpSafety and efficacy study of pembrolizumab (MK-3475) in combination with chemotherapy as neoadjuvant treatment for participants with triple negative breast cancer (TNBC) (MK-3475-173/KEYNOTE 173) Available from: https://clinicaltrials.gov/show/NCT02622074. NLM Identifier: NCT02622074Accessed December 2, 2015
- National Cancer Institute (NCI)Pembrolizumab in treating patients with triple-negative breast cancer Available from: https://clinicaltrials.gov/ct2/show/NCT02954874. NLM Identifier: NCT02954874Accessed November 3, 2016
- Pierfranco ConteIstitutoOncologico VenetoIRCCSAdjuvant treatment for high-risk triple negative breast cancer patients with the anti-PD-l1 antibody avelumab (A-Brave) Available from: https://clinicaltrials.gov/ct2/show/NCT02926196. NLM Identifier: NCT02926196Accessed October 5, 2016
- SenkusEKyriakidesSOhnoSESMO Guidelines CommitteePrimary breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-upAnn Oncol201526Suppl 5v8v3026314782
- DenduluriNSomerfieldMREisenASelection of optimal adjuvant chemotherapy regimens for human epidermal growth factor receptor 2 (HER2) – negative and adjuvant targeted therapy for HER2-positive breast cancers: an American Society of Clinical Oncology Guideline Adaptation of the Cancer Care Ontario Clinical Practice GuidelineJ Clin Oncol201634202416242727091714